
Abstract
Introduction:
Ultrasound-guided venipuncture and tip location by intracavitary electrocardiogram have many advantages during the insertion of peripherally inserted central catheters, both in terms of safety and cost-effectiveness. Recently, a new tip-conductive peripherally inserted central catheters and new Doppler ultrasound device integrated with intracavitary electrocardiogram have been introduced into clinical practice in China. A randomized multicenter study (clinical trial no. NCT03230357) was performed to verify the feasibility and accuracy of intracavitary electrocardiogram, as performed with this new peripherally inserted central catheters and device.
Methods:
Our study enrolled a total of 2250 adult patients in 10 different Chinese hospitals. The patients were randomly assigned to either the study group (intracavitary electrocardiogram) or the control group (anatomical landmark guidance) in a 2:1 allocation. Ultrasound was used in both groups for venipuncture and tip navigation. All patients underwent chest X-ray after the procedure to verify the position of the catheter tip.
Results:
No insertion-related complications were reported in either group. In the study group, first-attempt successful tip location was 91.7% (95% confidence interval: 90.3%–93.1%), significantly higher than 78.9% (95% confidence interval: 76.0%–81.9%) observed in the control group (p < 0.001). As evaluated by post-procedural chest X-ray, tip location in the study group had a sensitivity of 99.3% (95% confidence interval: 98.8%–99.7%), significantly higher than 86.8% (95% confidence interval: 84.4%–89.2%) observed in the anatomical landmark group (p < 0.001).
Conclusion:
These results indicated that during peripherally inserted central catheters insertion in adult patients, tip location with intracavitary electrocardiogram guidance, as carried out by a new tip-conductive peripherally inserted central catheters and intracavitary electrocardiogram integrated ultrasound device, was more effective and more accurate than tip location using anatomical landmarks.
Keywords
Introduction
Peripherally inserted central catheters (PICCs) play a critical role in patient care and provide a reliable, medium-, or long-term venous access for a variety of clinical indications, including the safe administration of chemotherapeutic agents, parenteral nutrition, and intravenous fluids.1–3 In the United States, the Intravenous Nurse Society (INS) recommends that the tip of a central venous access device should be preferably placed either in the lower third of the superior vena cava (SVC) or at the transition between the SVC and right atrium (RA; i.e. the cavoatrial junction (CAJ)). 4 Inaccurate tip positioning can increase the incidence of catheter-related complications, such as thrombosis, malfunction, or arrhythmias. Recent findings have indicated that the first-attempt success rate of tip location estimated by chest X-ray was approximately 80% when only relying on the conventional anatomical landmark method, which may not be regarded as a satisfactory outcome.5–7 The intracavitary electrocardiogram (IC-ECG) method has been used for the tip location of central venous access devices since the 1960s in European countries. 8 It is proved to be safe, accurate, and highly cost effective, because it saves the expenses related to post-procedural X-ray confirmation and possible repositioning of malpositioned catheters. In the past studies, IC-ECG was performed to guide the positioning of the PICC tip while using a column of saline contained in the catheter as an intracavitary (endovascular) electrode. Recently, a tip-conductive PICC was designed and fabricated by adding some functional materials to the silicone to make the catheter tip conductive. The conductive tip and guide wire together act as the intracavitary electrode, so saline flushing is no more required. Besides, a new Doppler ultrasound device including the function of ECG-EDUG (an abbreviation of ECG and Doppler Ultrasound Guidance devices; Branden Medical Scientific, Inc.) has recently become commercially available (Figure 1). In this study, we performed a new Chinese randomized multicenter study on the accuracy of IC-ECG, taking advantage of the tip-conductive PICC and EDUG device.
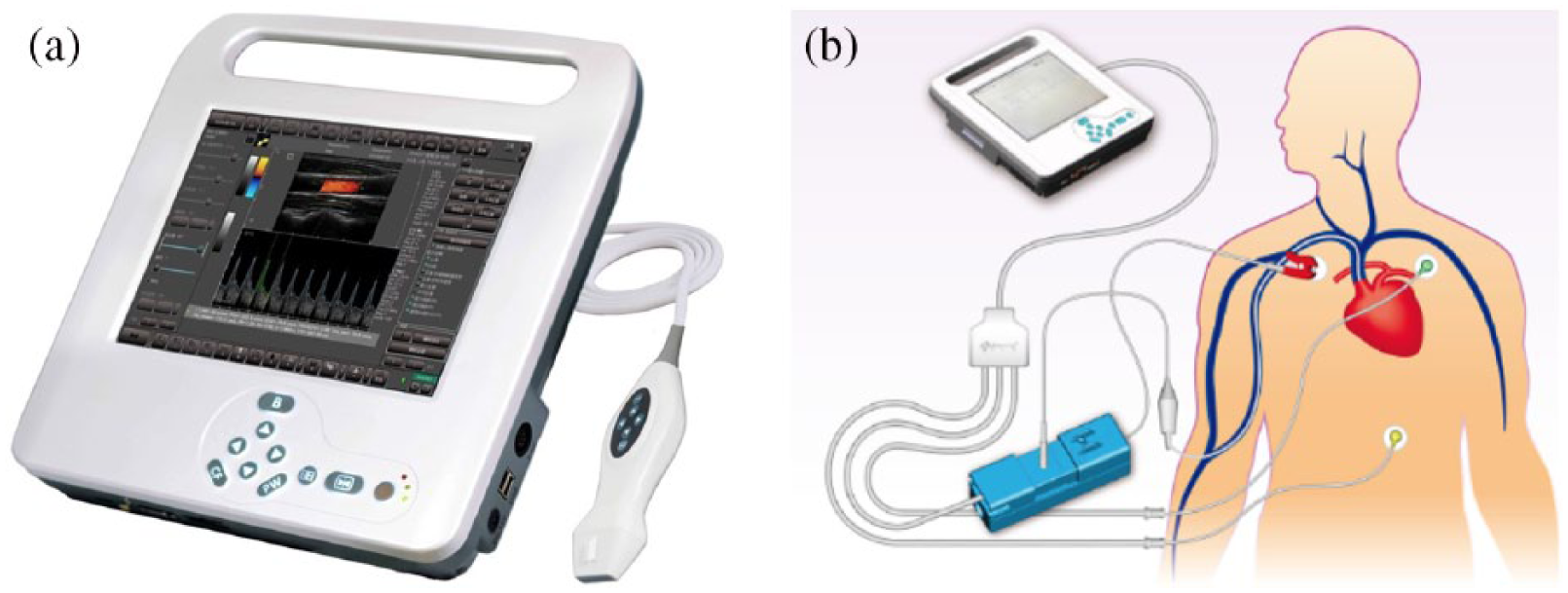
(a) The EDUG machine shows the depth of vein and blood flow speed through the ultrasound guidance. (b) The EDUG machine shows the changes in P-wave through the ECG guidance.
Materials and methods
Study design and patients
We designed a multicenter, open-label, randomized, prospective study, based on the CONSORT 2010 Statement, 9 comparing the accuracy of tip location by IC-ECG (performed with the new tip-conductived PICC and EDUG device) versus that of the traditional anatomical landmarks method, in Chinese patients requiring PICC placement. Inclusion criteria were as follows: (a) clinical indication to PICC insertion, (b) age between 18 and 80 years, and (c) normal P-wave appearance on the surface ECG recordings. The main exclusion criteria were pregnancy, previous history of central line insertion, cardiovascular conditions such as valve heart disease, atrial fibrillation, supraventricular tachycardia, pulmonary heart disease, pacemaker implantation, and history of cardiac surgery, which may affect P-waves. Patients were randomly assigned to either the study group or to the control group in a 2:1 allocation. A site-stratified block randomization with randomly varying block sizes of 4 and 6 was performed. Random assignment was performed by a statistician from Fudan University, and random envelopes were assigned to each site. Sequences were concealed from patients and clinical staff until assignment. Baseline parameters such as sex, age, and disease were collected by a specially designed App. The study protocol was centrally approved by the Independent Medical Ethics Committee (IEC) of Qilu Hospital, Medical School of Shandong University on 10 May 2017 and registered with ClinicalTrials.gov (number identifier: NCT03230357). All participating patients provided informed consent.
Methods
In the control group, the ultrasound technology provided by the EDUG device was used to identify a suitable vein for catheter insertion and perform ultrasound-guided venipuncture. The traditional anatomical landmarks method was used to estimate the catheter length.
In the study group, ultrasound guidance and traditional anatomical landmarks methods were performed the same as in the control group. Tip-conductive PICC was advanced gently until 5 cm was remaining, after which IC-ECG was performed according to the standard technique. As the catheter was slowly advanced into the SVC, the P-wave gradually increased, reaching a maximal peak at the CAJ. As the catheter entered the RA, a diphasic P-wave appeared and the catheter was retracted slowly to return to the position of maximal peak P-wave, with no negative components.
In both groups, during the procedure, the jugular vein was assessed by ultrasound to verify the presence of gross malposition. When the tip of PICC was visualized in the vein, the tip location maneuver was repeated. A post-procedural chest X-ray was obtained and interpreted by independent radiologists. The position of the tip close to the CAJ (approximately 3 cm below the tracheal carina) was considered optimal. If the catheter tip was located in the axillary vein, subclavian vein, jugular vein, or in the right ventricle, the tip was considered to be malpositioned. If the tip of the catheter was located in the RA or inferior vena cava, it was considered to be too “low.” If located in the high or middle one-third of the SVC, the position of the tip was considered to be too “high.”
Statistical analysis
All randomly assigned patients were included and missing data were excluded in the final analysis. The Chi-square test and t-test were used to analyze the differences between groups. Two-sided p values of less than 0.05 were considered statistically significant. All statistical analyses were performed using SPSS software, version 21.0 (IBM, Armonk, NY, USA). In the study group, sensitivity and specificity were calculated as follows: sensitivity referred to the occurrence of the peak of the P-wave as the catheter tip was at the CAJ (i.e. the ability of the technique to identify correctly placed catheters, with no false negatives); specificity was the rate at which characteristic P-wave changes might be associated with a tip not located at the CAJ (no false positive). 10
Results
Patient characteristics
Between May and December 2017, 2688 patients were screened for entering our study. Of those, we excluded 221 patients with clinical conditions where the IC-ECG might not be applicable (abnormal surface ECG) and182 patients with other exclusion criteria (age and previous history of central venous access device). In addition, 35 patients refused to participate in the study. Thus, a total of 2250 patients were randomly assigned to either the study group (n = 1500) or the control group (n = 750), according to a 2:1 allocation. All patients underwent chest X-ray confirmation of catheter tip positioning (Figure 2). No other protocol deviations occurred during the entire procedure. Patient baseline and PICC characteristics were similar between the two study groups (Table 1). Most PICCs were inserted via the basilic vein. No insertion-related complications were reported in either group.
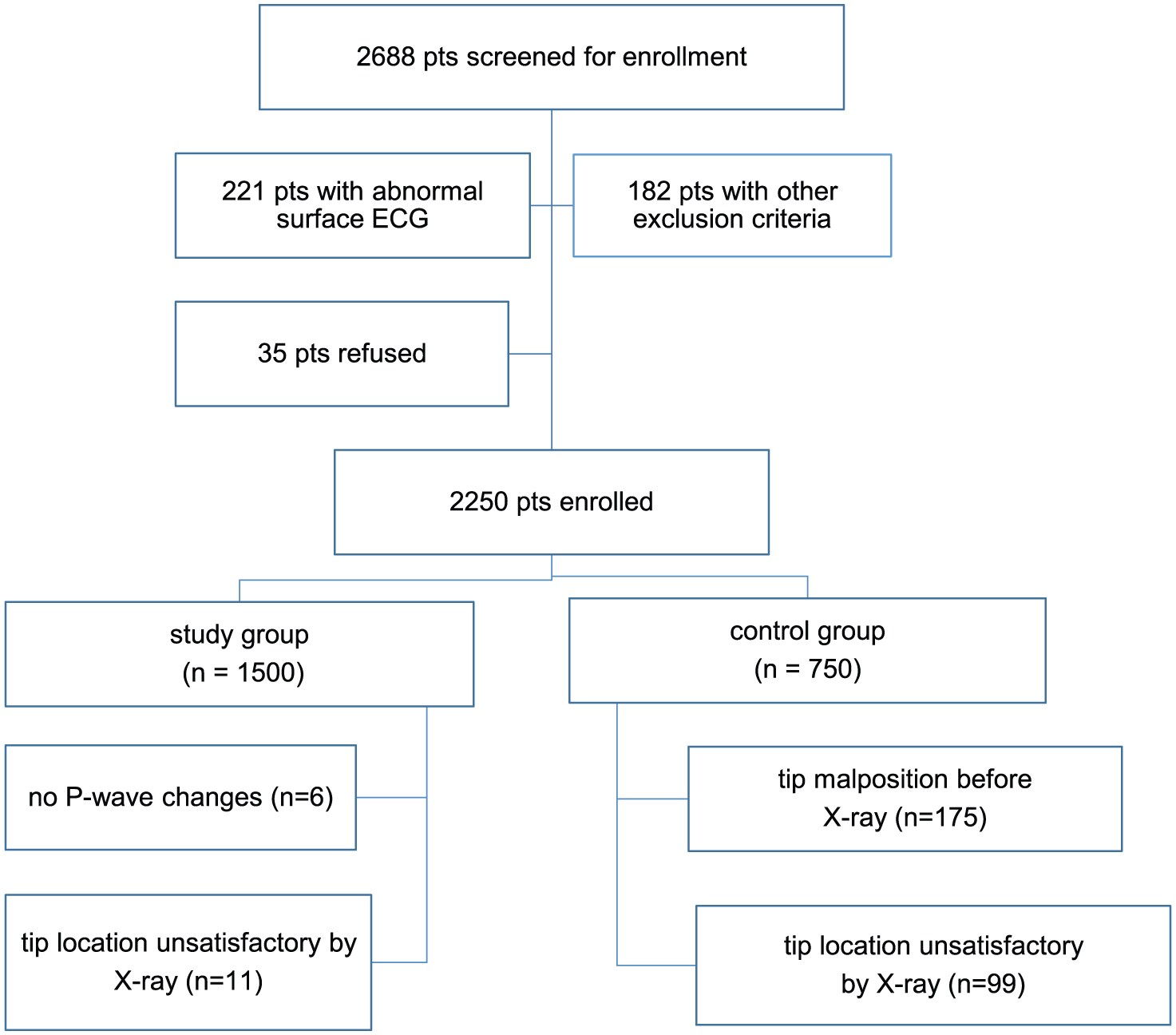
Patient enrollment.
Patients’ characteristics (n = 2250).
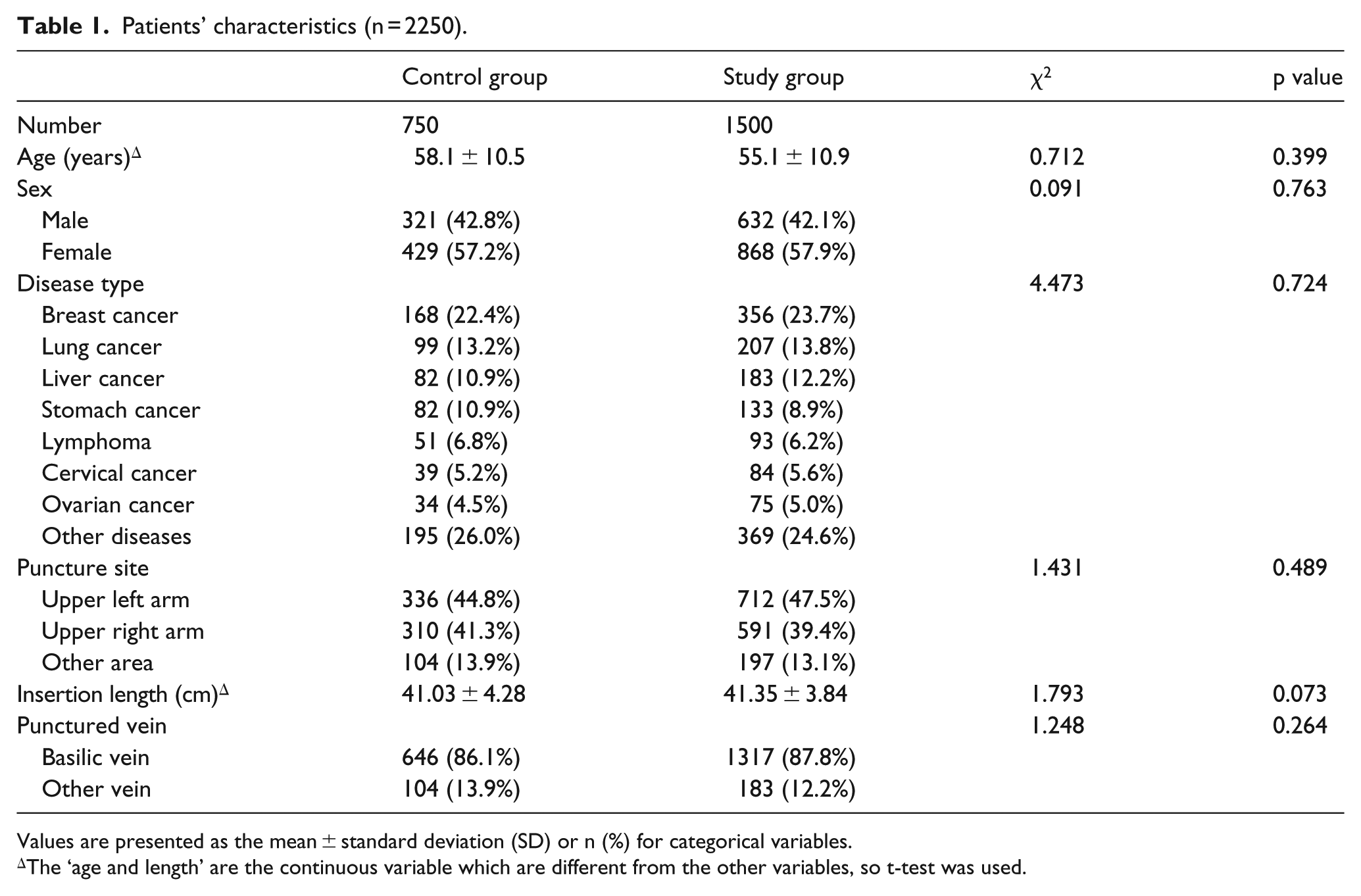
Values are presented as the mean ± standard deviation (SD) or n (%) for categorical variables.
The ‘age and length’ are the continuous variable which are different from the other variables, so t-test was used.
Efficacy of IC-ECG compared with the landmark technique
In the control group (750 patients), there were 178 cases of malpositioned tip (detected by ultrasound), which were adjusted intra-procedurally before chest X-ray. Of the 1500 patients in the study group, 124 cases did not show the typical P-wave changes during the procedure and 118 had malpositioned tips upon ultrasound examination. In all 118 cases, the typical P-wave changes appeared after reposition. In six cases, the characteristic P-wave changes did not appear, though the catheter tip was found to be at the CAJ at the post-procedural X-ray (false negatives).
Malposition rate was detected by chest X-ray in the control group, and there were 99 cases (13.2%) of unsatisfactory tip location. In 42 cases (5.6%), the position of catheter tip was too “high”; in 53 cases (7.1%) too “low”; and in 4 cases (0.5%), there was an overt malposition. In the study group, there were 11 cases (0.7%) of unsatisfactory tip location. Sensitivity was 99.3% (11 false negatives) and specificity was 100% (no false positive). All unsatisfactory placements (8 “high” catheters and 3 “low” catheters) occurred during the first period of the study, suggesting a learning curve. Interestingly, no case of overt malposition was observed in the study group (Table 2).
Comparison of tip location between the groups.
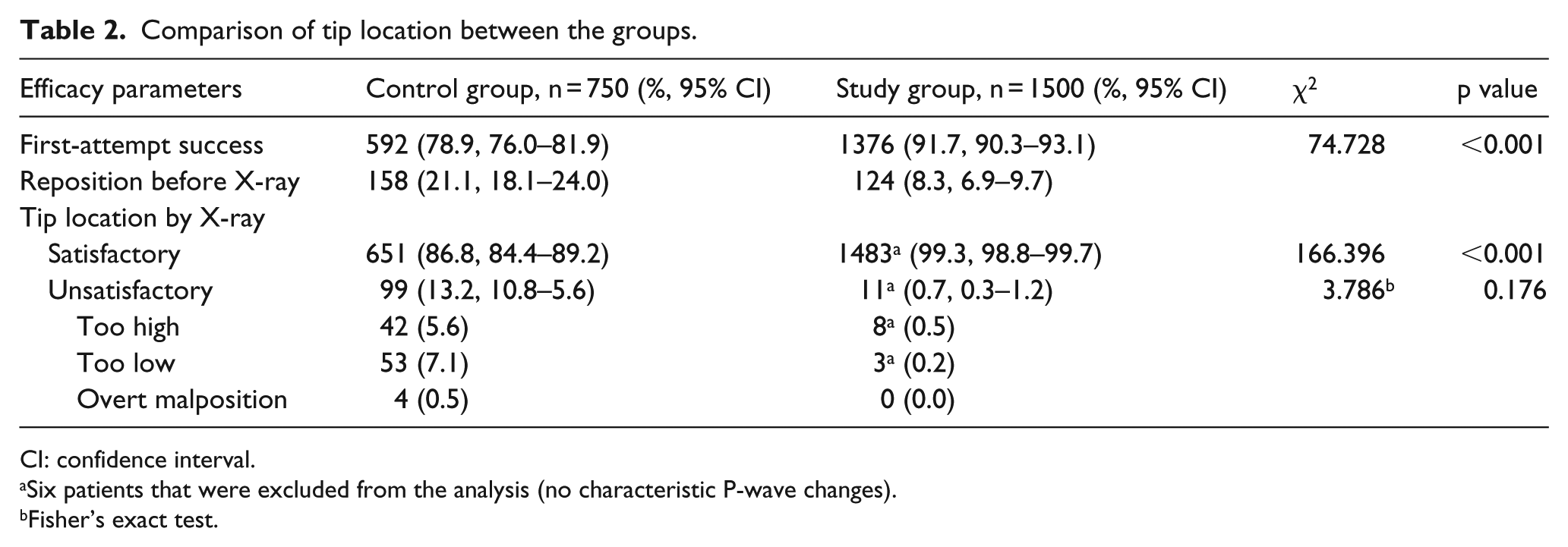
CI: confidence interval.
Six patients that were excluded from the analysis (no characteristic P-wave changes).
Fisher’s exact test.
Discussion
PICCs have several advantages compared with other venous access devices; namely, long-term use, safety, efficiency, compatibility with hyperosmolar, and irritant drugs as well as negligible complications. 11 The PICCs have been used in China since the late 1990s and popularized rapidly in recent 10 years. The ultrasound technology has been well applied for the clinical benefits of vein assessment, venipuncture, and ruling-out gross malpositions, reducing the PICC-associated complications such as pain, bleeding, infections, and thrombosis. Moreover, the proper location of the PICC tip is essential. If the tip of the catheter is placed too high (in the middle or upper third of the SVC, or in the brachiocephalic, or in the internal jugular, or in the subclavian vein), there is an increased risk of malfunction and/or venous thrombosis. If the tip is positioned too low (RA, right ventricle, or inferior vena cava), there is a risk of arrhythmia, heart cavity lesions, tricuspid valve dysfunction or lesions, or atrial thrombosis. 12 Chest X-ray is still regarded as the gold standard for confirming the tip position. However, the accuracy of chest X-ray is not 100%, as many factors such as artifacts and errors of perspective and technical difficulties may alter interpretation of the radiologic image, leading to a significant incidence of false positives and false negatives. IC-ECG is currently used in many countries as a safe and accurate method to locate the PICC tip by interpreting P-wave morphology. In a recent comparative randomized Chinese study by Yuan et al., 4 significant benefits of IC-ECG guidance versus traditional anatomical landmark guidance were reported. In the IC-ECG-guided group, the first-attempt success rate was 89.2%, which was significantly higher than 77.4% observed in the landmark group (p < 0.0001). Our study confirms that tip location by IC-ECG is more accurate than the landmark technique. The tip-conductive PICC acting in concert with EDUG can promote the convenience of IC-ECG imaging, without the need for saline infusion. A perfect match between tip location by IC-ECG and tip location by chest X-ray was found in 99.3% of patients. However, the match between tip location by the landmarks method and X-ray was only 86.8%. Confirming previous reports 13 from theliterature, 14 we did not detect any adverse events or complications directly or indirectly related to the IC-ECG method.
Malposition of PICCs occurs frequently, but the exact rate can vary greatly due to the operator and patient. Several studies have reported that anatomical landmark guidance may be associated with a malposition rate of 10%–40%.15–17 Our study showed that the first-attempt target rate of the landmarks technique was 76.3%, consistent with the findings in other studies. However, with the help of ultrasonography, malposition was identified and timely adjusted during the procedure.
According to the literature, approximately 7% of patients with no clear and evident P-wave recognized on the baseline ECG may have to resort to other tip location methods. 12 In this study, where we had strict inclusion and exclusion criteria, in 6 out of 1500 patients, although the P-wave was apparently normal at baseline ECG, the intracavitary ECG did not show any significant P-wave, while the chest X-ray showed no evidence of malposition. The reason for such false negative results is unclear yet; inappropriate placement of the electrodes may be a possible explanation. The overall rate of false negative in the study group was nonetheless extremely low (11 cases, 0.7%). In addition, no false-positive results of the IC-ECG method were observed in this study.
Our study has some obvious limitations. First, we assumed that the post-procedural chest X-ray was the gold standard for tip location, which is not completely correct, since previous reports showed that radiology may be somehow less accurate than other tip location methods (such as transesophageal echocardiography or IC-ECG itself). However, tip location by chest X-ray remains the gold standard in China, so that our study design was adequate. Also, even if our randomized multicenter study demonstrated the superiority of the IC-ECG technique in preventing tip malposition, we did not provide data regarding long-term complications. Finally, we successfully adopted the new tip-conductive PICC and EDUG device for IC-ECG, but we have no data on the comparison of conventional IC-ECG and this new method. A randomized clinical study may be designed to compare the convenience, cost time, and tip accuracy.
In conclusion, our study demonstrated that the IC-ECG method, as performed using the tip-conductive PICC and EDUG device, is safer and more accurate than the traditional landmark methods for achieving a rapid and satisfactory tip location during PICC placement in adult patients.
Footnotes
Acknowledgements
Hai-Jun Zhang holds intellectual property rights on the technology licensed to Branden Medical Scientific, Inc., who manufactured the PICCs and EDUG described in this article. Yu-Xia Yin and Wei Gao contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovation and Achievement Transformation Fund of Shandong Province (No. 2013ZHZX2A0401).