
Abstract
Objective:
Arteriovenous fistulas for hemodialysis vascular access are a burden for the cardiovascular system. After successful kidney transplantation, prophylactic arteriovenous fistula ligation may improve cardiac outcomes; however, evidence is scarce. This survey investigates physicians’ preference for management of arteriovenous fistulas and identifies the factors associated with preference for either arteriovenous fistula ligation or maintenance.
Materials and methods:
A survey was sent to members of eight national and international Nephrology and Vascular Surgery societies. The survey comprised eight case vignettes of asymptomatic patients with a functioning arteriovenous fistula after kidney transplantation. Characteristics possibly associated with treatment preferences were arteriovenous fistula flow, left ventricular ejection fraction, and patient age. Respondents were asked to state preference to maintain or ligate the arteriovenous fistula. Linear mixed-effects models were used to investigate the association of treatment preference with case characteristics.
Results:
A total of 585 surveys were returned. A reduced left ventricular ejection fraction of 30% (beta 0.60, 95% confidence interval 0.55; 0.65) and a high flow of 2500 mL/min (beta 0.46, 95% confidence interval 0.41; 0.51) were associated with a higher preference for arteriovenous fistula ligation. Disagreement among respondents was considerable, as in four out of eight cases less than 70% of respondents agreed on the arteriovenous fistula management strategy.
Conclusion:
Although respondents recognize a reduced left ventricular ejection fraction and a high flow as the risk factors, the high disagreement on management preferences suggests that evidence is inconclusive to recommend arteriovenous fistula ligation or maintenance after kidney transplantation. More research is needed to determine optimal arteriovenous fistula management after successful kidney transplantation.
Introduction
Nephrologists and surgeons often face patients with a functioning arteriovenous fistula (AVF) after kidney transplantation. Although the AVF is the preferred vascular access (VA) for patients on maintenance hemodialysis (HD), it burdens the cardiovascular system by increasing cardiac output, left ventricular mass, and pulmonary arterial pressure.1,2 This process of “AVF cardiotoxicity” may result in symptoms of heart failure or may remain asymptomatic. 3 A higher left ventricular mass is associated with cardiovascular events and death in asymptomatic HD patients. 4 While on HD, the benefits of an adequately functioning AVF usually outweigh these detrimental cardiac effects of AVFs. This balance of pros and cons of AVFs might change for individual patients after successful kidney transplantation, as the cardiovascular burden persists while patients no longer benefit from the advantages of AVFs. The main disadvantages of routine ligation are the need for the construction of a new AVF in case HD needs to be reinitiated, the burden of the ligation surgery, and the loss of a VA site for blood sample collections, as some AVFs are used for this purpose in case no suitable veins are accessible for conventional venepuncture.
Small observational studies suggest that left ventricular mass could improve after AVF ligation in kidney transplantation recipients.5,6 However, neither large observational studies, nor intervention trials have been performed to evaluate whether preservation or ligation of AVFs should be recommended in kidney transplantation recipients. Although AVF ligation may improve cardiac function, studies on the effect of a functional AVF on kidney function revealed conflicting results, suggesting that kidney allograft function may deteriorate after ligation.7,8
Data on the current practice of VA management after kidney transplantation and recommendations in guidelines on this topic are scarce. The United Kingdom Renal Association and United States National Kidney Foundation guidelines on VA do not include any advice on VA management after kidney transplantation.9,10 The European Best Practice Guideline on Vascular Access mentions possible improvement of cardiac function after AVF ligation, but does not recommend routine ligation after kidney transplantation. 11 Thus far, no studies on physicians’ attitudes toward VA management after kidney transplantation have been published. Therefore, the aim of this study was to investigate physicians’ preferences for AVF preservation or ligation in asymptomatic patients after successful kidney transplantation. We also aimed to identify the factors influencing these preferences and to assess differences in treatment preferences across specialties and other physician subgroups.
Methods
Participants
Eligible participants were physicians associated with the Journal of Vascular Access of the Vascular Access Society, the American Society of Diagnostic and Interventional Nephrology, the Vascular Access Society of Britain and Ireland, the Italian Society of Nephrology, the Australian and New Zealand Society of Nephrology, the European Society for Vascular Surgery, the Dutch Federation of Nephrology, and the Dutch Society for Vascular Surgery. An online survey was sent out in the societies’ newsletters or as a separate e-mail.
Questionnaire
Interviews were performed with a focus group of vascular surgeons and nephrologists in one academic and one affiliated hospital. Factors influencing physicians’ decisions to maintain or ligate a VA after kidney transplantation were identified. From these, a questionnaire was compiled. The complete questionnaire is available in the Supplementary materials. Respondents were asked to state their characteristics, including specialty, seniority, number of VA-related decisions per year, affiliation, and country. They were then asked if routine VA surveillance was performed in kidney transplantation patients in their hospital. Eight case vignettes were presented of patients with a good kidney transplantation prognosis, a functioning brachiocephalic AVF without local symptoms and with options for future AVF creation (Table 1). Case vignettes were presented with all possible combinations of age, AVF flow, and left ventricular ejection fraction (LVEF). Respondents were asked to state their preference for maintaining or ligating the AVF on a four-point Likert scale. We decided against a neutral midpoint option, as no clear preference to ligate the AVF in practice means that the AVF is maintained. By presenting a four-point Likert scale, we forced the respondents to decide on either maintenance or ligation. 12
Example case vignette. Age, cardiac status, and AVF flow were varied for the eight clinical case vignettes.
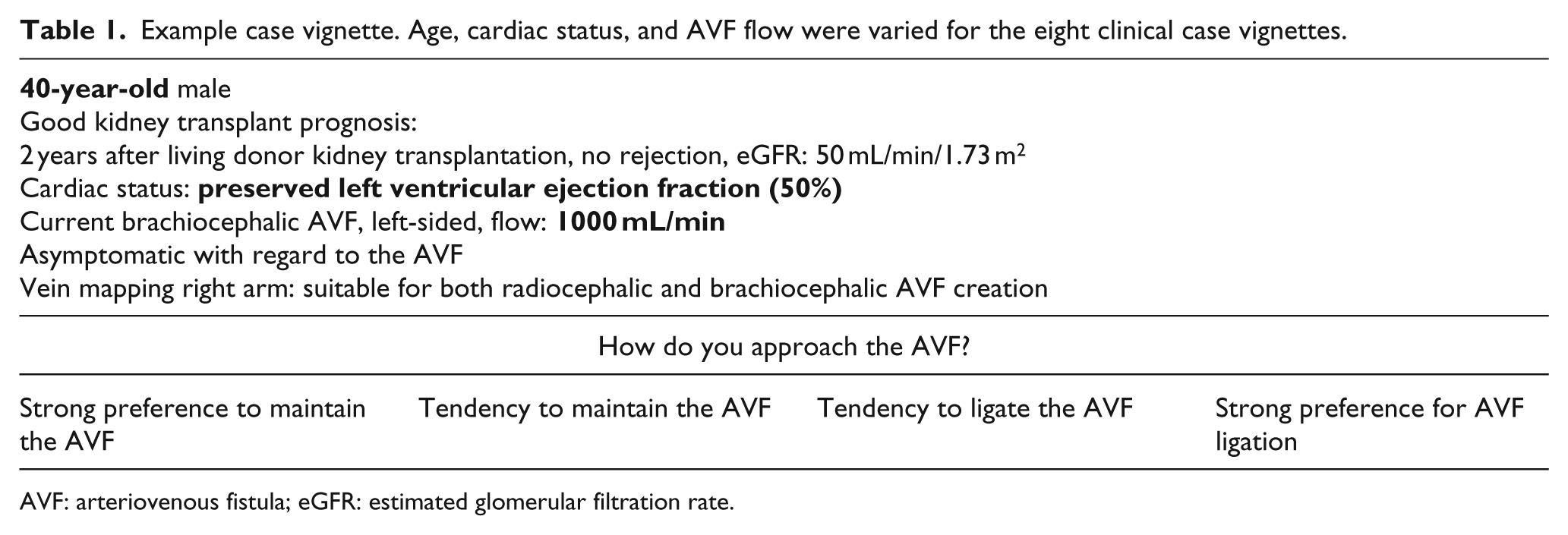
AVF: arteriovenous fistula; eGFR: estimated glomerular filtration rate.
We crafted the case vignettes in a way that decisions would focus on long-term outcomes, rather than being forced toward either ligating or maintaining the AVF. We assumed a poor transplant prognosis or no contralateral AVF options to result in a “maintain AVF” response by nearly all respondents, and symptoms of cardiac failure or complaints about the AVF itself to result in AVF ligation by nearly all respondents. Based on these assumptions, we did not vary these variables in the clinical cases.
The case vignettes were presented in a random order. A response to each Likert scale was required to continue to the next case. Partially filled-in questionnaires were included in the analysis. After the randomized case vignettes, respondents were presented with one case vignette of a patient with the characteristics shown in Table 1, but without a given AVF flow. Respondents were asked if they would never ligate the AVF, always ligate the AVF, or base their decision on the AVF flow. In the latter case, they were asked to specify at which minimum flow they would ligate the AVF. Finally, respondents could freely comment on which criteria are important to them in deciding on AVF management after kidney transplantation.
Statistical analysis
Descriptive statistics were used to describe respondents’ characteristics. Preferences were coded on a four-point scale, with 1 representing a strong preference to maintain the AVF and 4 representing a strong preference to ligate the AVF. Analyses were performed for all respondents and separately for surgeons and nephrologists, academic and affiliated hospital physicians, and those who make less or more than the median number of 80 VA-related decisions per year. Mean scores for maintenance or ligation of AVFs were calculated per case vignette. If for a case vignette less than 70% of respondents prefer to ligate an AVF while more than 30% of respondents prefer to maintain the AVF, or vice versa, we considered disagreement to be considerable.
The factors influencing clinicians’ preferences were assessed using linear mixed-effects models. Linear mixed-effects models can be used to estimate the preference of ligation across respondents, while accounting for the dependency of observations within respondents. The patients’ age (40 or 65 years), AVF flow (1000 or 2500 mL/min), and cardiac status (LVEF 30% or 50%) were entered as separate independent variables in the fixed-effects model and the individual respondents as the random effect. The case vignettes were entered as repeated measurements. In the model building phase, the model with the best fitting covariance matrix was selected based on the Akaike’s information criterion (AIC; whereby a lower AIC indicated a better model fit). The AIC is based on the value of the maximum likelihood and on the number of parameters in the model and can be used to compare the fit between models. 13 The final model with unstructured covariance fit best (lowest AIC) and was then fit by restricted maximum likelihood to estimate the preference for ligation. The model outcomes were beta values, indicating by how many points the 1–4 Likert scale is affected in the presence of each independent variable. The values each beta could theoretically take range from −3 to +3. Lower beta scores systematically indicated stronger preference to maintain the AVF. Reference categories were defined as an age of 40 years, a flow of 1000 mL/min, and an LVEF of 50%. Analyses were performed in SPSS version 22 (SPSS, IBM Corporation).
Results
Participants
A total of 585 responses were received. Most respondents were surgeons (54.5%) or nephrologists (37.6%) with a median of 13 years of clinical experience and 80 VA-related treatment decisions in the past year. The characteristics of respondents are shown in Table 2. Nine (1.5%) respondents stated that they had not made any VA-related decisions in the past year. Routine VA surveillance after kidney transplantation was performed by 29% of respondents.
Characteristics of respondents (n = 585). Experience years and number of treatment decisions are median and interquartile ranges.
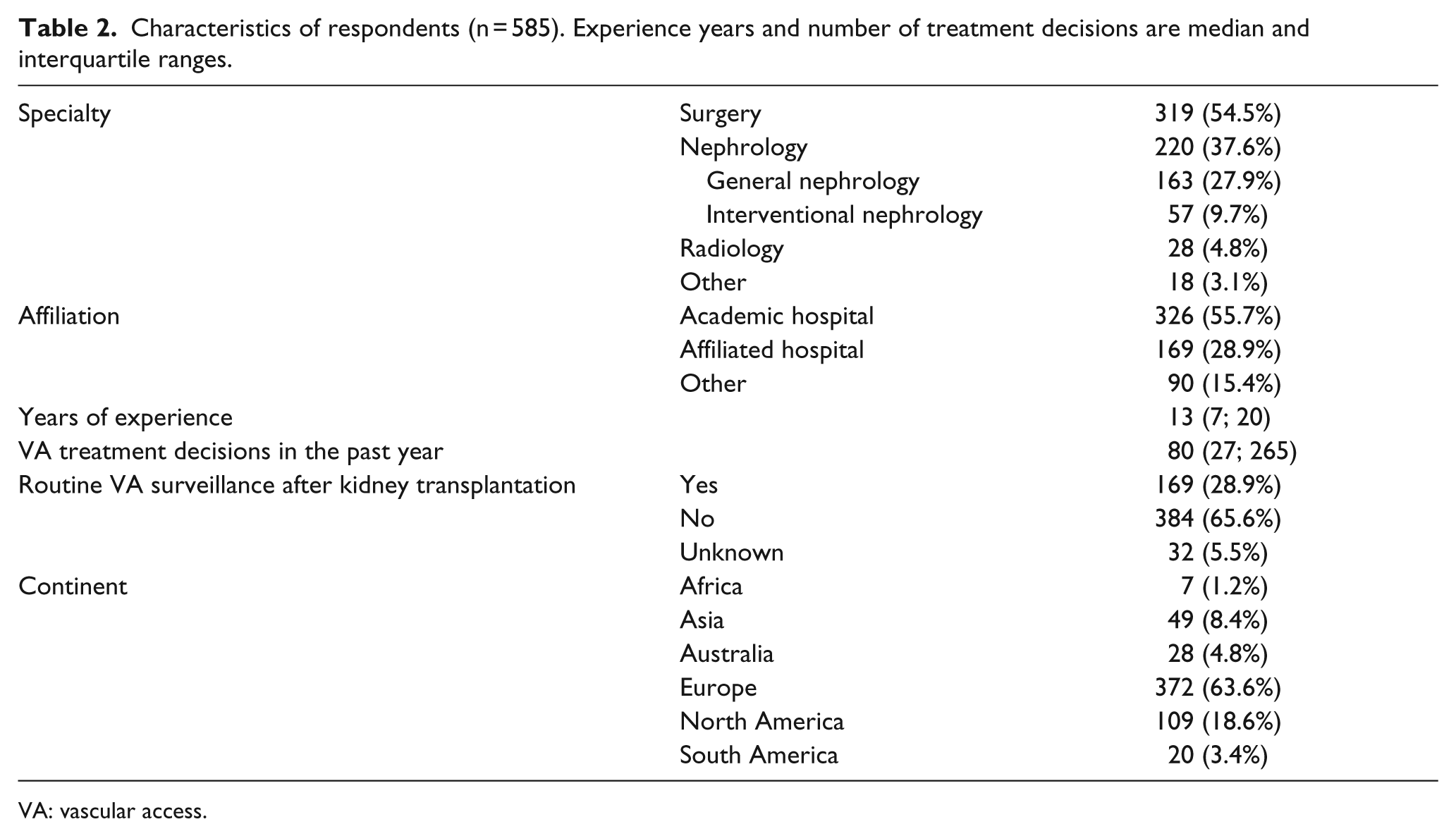
VA: vascular access.
Treatment preferences
For four out of eight cases, disagreement was considerable with less than 70% of respondents preferring either AVF maintenance or ligation (Figure 1). The tendency to ligate the AVF was the highest in clinical cases with a high AVF flow of 2500 mL/min and a reduced LVEF of 30%, in which 55.3% (patient age 40 years) and 59.6% (patient age 65 years) of the respondents strongly preferred AVF ligation. On the other hand, 20.0% and 19.2% of respondents preferred to maintain the AVF in these cases, respectively. Only eight respondents (1.4%) strongly preferred maintenance of the AVF in all clinical cases, whereas 28 respondents (4.8%) always strongly preferred AVF ligation.
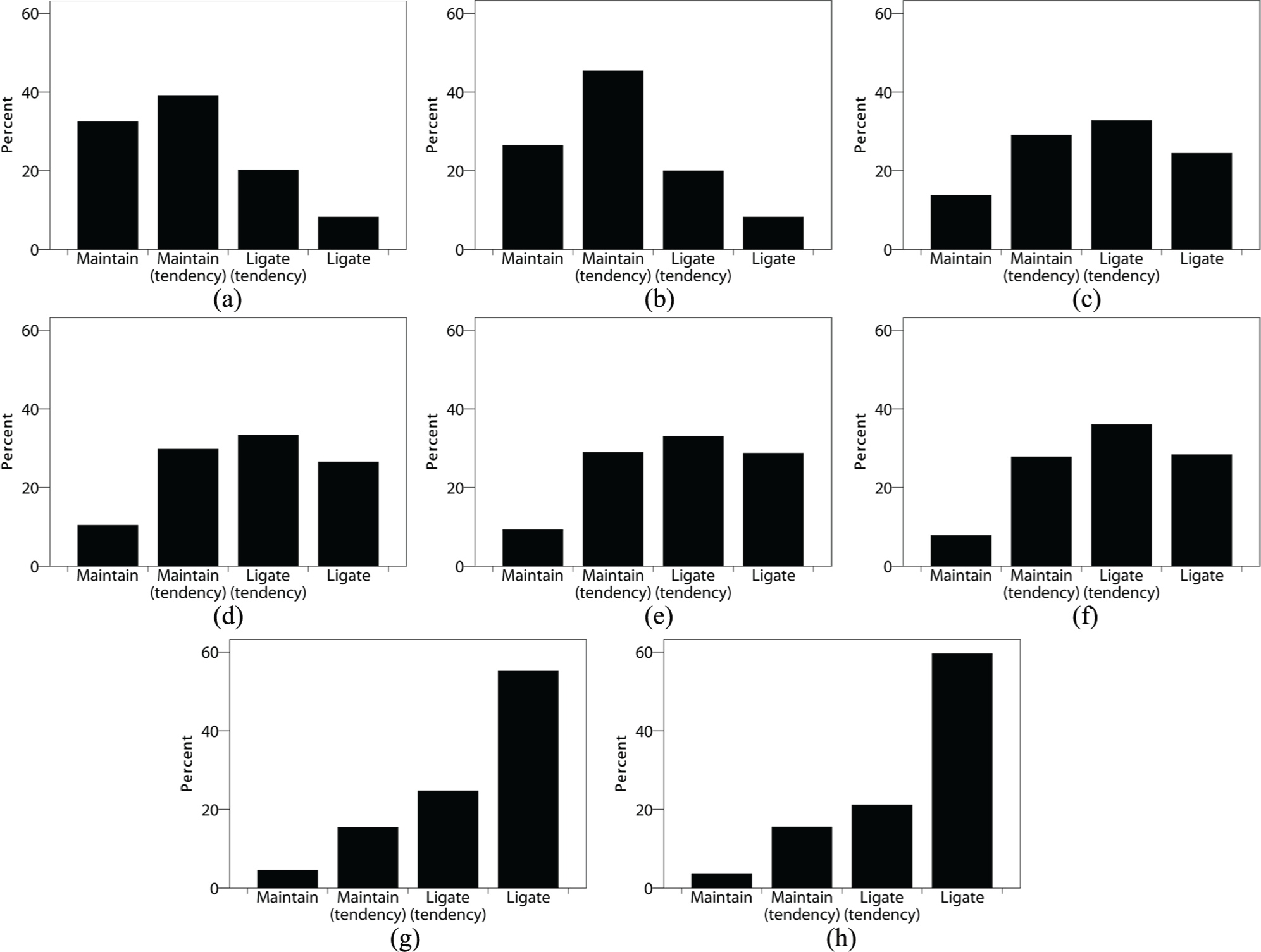
Distribution of preferences per case vignette: (a) 40 years, flow 1000 mL/min, LVEF 50%; (b) 65 years, flow 1000 mL/min, LVEF 50%; (c) 40 years, flow 2500 mL/min, LVEF 50%; (d) 65 years, flow 2500 mL/min, LVEF 50%; (e) 40 years, flow 1000 mL/min, LVEF 30%; (f) 65 years, flow 1000 mL/min, LVEF 30%; (g) 40 years, flow 2500 mL/min, LVEF 30%; and (h) 65 years, flow 2500 mL/min, LVEF 30%.
Impact of patient characteristics on VA treatment preference
A high AVF flow of 2500 mL/min (beta 0.46, 95% confidence interval 0.41; 0.51) and a reduced LVEF of 30% (beta 0.60, 95% confidence interval 0.55; 0.65) were independently associated with an increased preference to ligate the AVF (Figure 2) and cases with these combinations scored highest on the mean tendency to ligate (Table 3). Age was not significantly associated with treatment preferences. In the subgroup analyses, the same pattern was observed for surgeons and nephrologists, physicians in academic and affiliated hospitals, physicians who made less than the median number of 80 versus 80 or more VA treatment decisions in the past year, and physicians who do versus do not perform routine AVF surveillance (Supplementary, Table 1). No clinically relevant interactions were observed between patient age, AVF flow, and LVEF (Supplementary, Table 2).
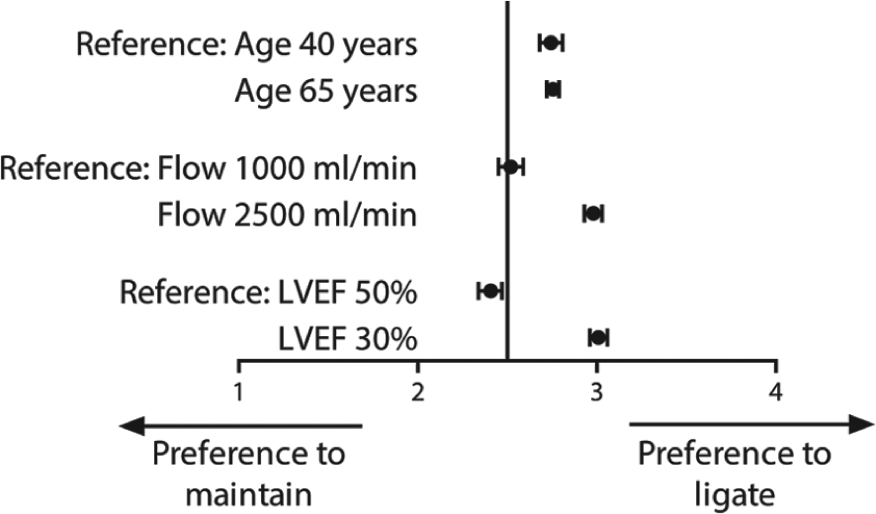
Associations of patient factors on the tendency to maintain or ligate AVFs. Age of 40 years, a flow of 1000 mL/min, and a preserved LVEF of 50% were set as reference categories.
Mean scores (±standard deviation) for case vignettes, nephrologists, and surgeons. Values range from 1 (strong preference to maintain AVF) to 4 (strong preference to ligate AVF).
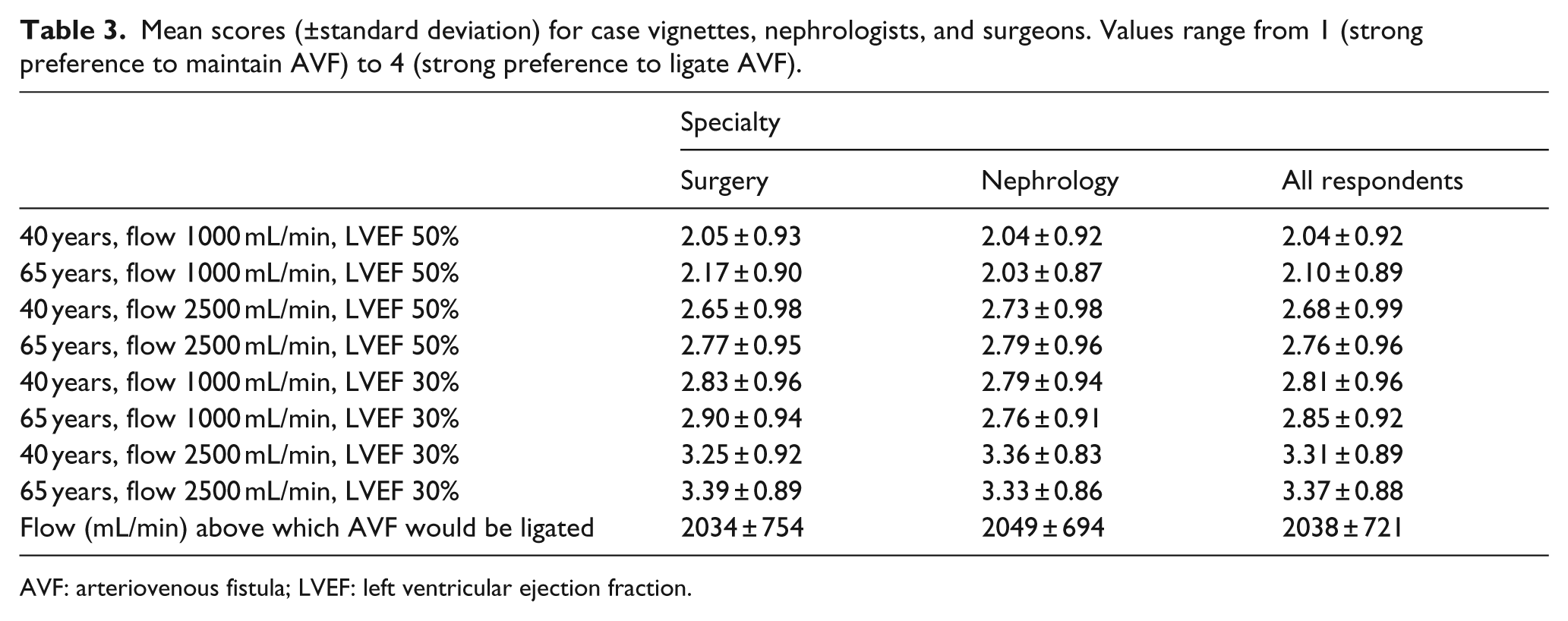
AVF: arteriovenous fistula; LVEF: left ventricular ejection fraction.
Influence of VA flow on the tendency to ligate
In the case of a 40-year-old patient with a preserved LVEF, 120 (24.9%) respondents would never ligate the AVF, 63 (13.1%) would always ligate the AVF, and 299 (62.0%) base their decision on the AVF flow. For both nephrologists and surgeons, the mean cut-off value above which AVF ligation was preferred was at 2038 mL/min (Table 3 and Figure 3).
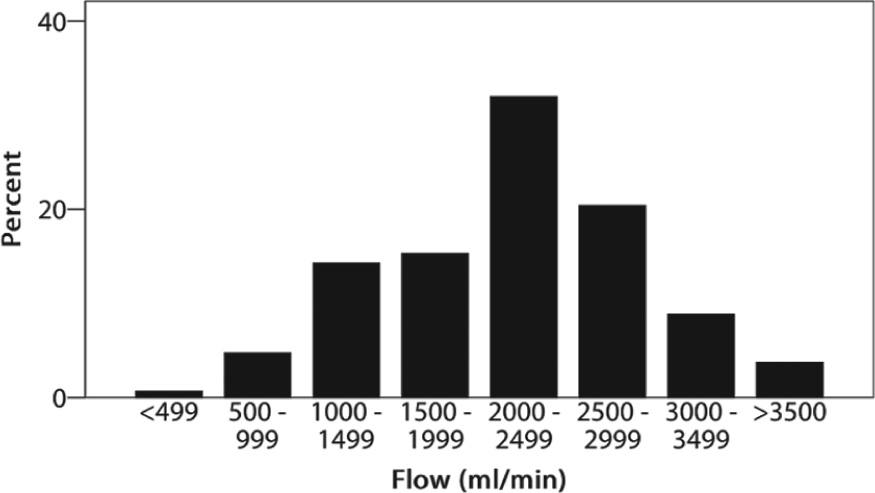
Cut-off value of flow (mL/min) above which AVF ligation is preferred by respondents who base their decision on AVF flow.
Other factors relevant for decision making
The respondents could comment optionally on which factors are important in their decision-making process. The most frequently encountered answers were on cardiac comorbidity and symptoms (n = 87), AVF flow (n = 61), expected kidney allograft survival (n = 52), local symptoms (n = 28), prospect to create another AVF (n = 27), and patient preference (n = 15). Flow reduction strategies including a Miller banding procedure or a revision using distal inflow were suggested by 43 respondents.
Discussion
No consensus exists on whether routine ligation should be performed in kidney transplantation recipients who are asymptomatic with regard to their VA, even though small studies suggest a beneficial effect of VA ligation on cardiac parameters including left ventricular mass. With this survey, we aimed to investigate physicians’ attitudes toward treatment of VAs after kidney transplantation and to measure the influence of patient characteristics on this preference.
As the mean preference score was higher than 2.5 in six out of eight cases, we observed a preference for AVF ligation in the presented asymptomatic cases with a good renal allograft function. The management preferences did not differ between nephrologists and surgeons or other subgroups. A reduced LVEF and a high AVF flow were associated with a higher preference for AVF ligation.
Disagreement among respondents
In general, there was considerable disagreement among respondents with regard to the preferred treatment strategy for the case vignettes. While the majority of respondents prefer to ligate a VA in the patients with a high AVF flow and reduced LVEF, 20% of respondents prefer to maintain the VA in these patients. In patients with less pronounced risk factors, the variability in preferences was even greater. This demonstrates that the best treatment for these patients is unknown and there is no consensus among physicians on AVF management. Several factors should be taken into account when considering the optimal VA management after kidney transplantation.
Return to HD and resumed use of the AVF
Routine AVF ligation may harm patients who return to HD and might otherwise have resumed the use of their AVF. Whether this should be taken into account in patients with a stable kidney function depends on two aspects: (1) the likelihood that patients outlive their renal allograft and return to HD and (2) the chance that the AVF could still be used at that time.
Local differences of the prognosis of renal allografts may be an important explanation of the observed disagreement in physicians’ preference. In a recent publication from the European ERA-EDTA registry, the 5-year death-censored allograft survival in recipients of a living donor kidney transplant approaches 90% and an increasing proportion of patients will die with a functioning kidney graft and never return to HD. 14 For deceased donors, the 5-year graft survival was 77% for all patients, while it was worse for elderly patients at 62%. In the United States, the 5-year graft survival of patients transplanted in 2010 was similar at 73% for deceased donors and 85% for living donors. 15 Other factors such as expanded donor criteria and choice of immunosuppressive regimens may contribute to regional differences in transplantation outcomes. 16 Of note, kidney allograft failure is not the same as return to HD, as patients may also be retransplanted preemptively or opt for peritoneal dialysis or conservative treatment.
The question arises what percentage of patients could use their VA for HD at time of renal allograft failure if the VA is not routinely ligated. In a retrospective study by Manca and coworkers 17 in which 542 transplanted patients with a functional AVF were included, 207 AVFs closed either spontaneously (156 patients) or surgically because of local symptoms (49 patients). During follow-up, 89 patients returned to HD, while only 49 of them reused the AVF they had at the time of transplantation. Immediate routine ligation would therefore only harm 49/542 (9%) of patients and expose 156 of them (29%) to an unnecessary procedure.
Aitken and Kingsmore 18 observed similar outcomes in a cohort of 398 patients with a patent AVF at the time of kidney transplantation. In this cohort, 78 AVFs (19.6%) failed within 1 year or were ligated for symptoms or cosmetic reasons. In 98 patients, graft loss occurred and in 69 cases of graft loss (70%) the AVF was still patent or could be used after minor procedures. Routine ligation of all AVFs in this cohort would have harmed these 69 (17.3%) patients.
Why age does not seem to matter in physician’s preferences?
In elderly patients, the major cause for kidney allograft loss is death with a functioning allograft. 19 This would favor AVF ligation in elderly patients. Inversely, if AVF ligation improves long-term cardiovascular outcomes, young patients could benefit more from timely ligation. On the contrary, younger patients are also more likely to return to HD in their lifetime. Based on our results, we could not determine how age was being weighted as a contributing factor to the preference of the physicians in the presented cases.
Banding as an intermediate option in VA management after kidney transplantation
Several respondents suggested a banding procedure rather than ligation for high-flow AVFs. Obviously, banding could be a sensible option, although it remains challenging to permanently reduce AVF flow, as recurrent high flow has been reported in up to 50% of patients. 20 A banding procedure may therefore not be the optimal strategy to improve long-term cardiovascular outcomes for all patients, but may be considered in patients who will likely return to HD.
Patients’ preferences
Whether or not to ligate an AVF after kidney transplantation should be a process of shared decision making by the patient and the physician. To properly counsel patients on this topic, physicians should have an understanding of the pathophysiology of AVF cardiotoxicity and the risks and benefits of ligation. Patients may prefer to maintain their AVF if the cosmetic consequences of future contralateral AVF creation are not acceptable or if the AVF remains in use for blood collection.
Study limitations
We did not vary the transplant prognosis and did not include cardiac or local AVF symptoms in the case vignettes. Therefore, the survey only provides information on preferences for prophylactic AVF ligation to improve long-term cardiovascular outcomes and does not reflect physicians’ preferences for AVF management to treat current heart failure or local symptoms. In addition, it is important to emphasize that the survey responses solely reflect physicians’ preferences, which may not match with clinical practice. As the majority of respondents do not perform routine VA surveillance after kidney transplantation, it is likely that AVF ligation is not as frequently performed in asymptomatic patients as suggested by the reported preferences of the physicians who participated in the survey.
Conclusion and future directions
The significant variability in preferences demonstrates that the current evidence is not convincing to recommend routine preservation or ligation of AVFs in kidney transplantation recipients. We hope that this research stimulates the discussion about optimal care for VAs after kidney transplantation and results in future studies on this underexposed part of VA management. It could be of great value to gain more insight into the protocols for surveillance that are currently being used all over the world and to propose a consensus-based guideline.
We aim to explore patients’ attitudes toward their AVF in an upcoming survey, as the feasibility of an intervention trial on AVF ligation after kidney transplantation strongly depends on patients’ attitude regarding AVF ligation and preservation. Ultimately, we aim to perform a randomized clinical trial investigating the effect of prophylactic AVF ligation on renal allograft function, cardiac parameters, cardiac and all-cause mortality as well as VA complications in patients who restart HD.
Supplementary Material
Supplementary Material, Supplementary_Material_-_Survey – No consensus on physicians’ preferences on vascular access management after kidney transplantation: Results of a multi-national survey
Supplementary Material, Supplementary_Material_-_Survey for No consensus on physicians’ preferences on vascular access management after kidney transplantation: Results of a multi-national survey by Bram M Voorzaat, Cynthia J Janmaat, Esther D Wilschut, Koen EA Van Der Bogt, Friedo W Dekker and Joris I Rotmans in The Journal of Vascular Access
Footnotes
Acknowledgements
We thank the board and members of the Journal of Vascular Access of the Vascular Access Society, the American Society of Diagnostic and Interventional Nephrology, the Vascular Access Society of Britain and Ireland, the Italian Society of Nephrology, the Australian and New Zealand Society of Nephrology, the European Society for Vascular Surgery, the Dutch Federation of Nephrology and the Dutch Society for Vascular Surgery for participating in this survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.