
Abstract
Background:
Femoroacetabular impingement syndrome (FAIS) is a common hip disorder that can lead to joint degeneration and osteoarthritis. Posterolateral (PL) cam lesions, characterised by an α angle >60° on anteroposterior (AP) pelvis and Dunn views, present significant surgical challenges due to their anatomical location and proximity to critical vascular structures. Effective surgical intervention relies on achieving optimal postoperative resection, yet clear radiographic thresholds for surgical success remain undefined.
Objective:
This study aimed to investigate the relationship between postoperative α angle measurements on pelvis AP radiographs and clinical outcomes in patients undergoing hip arthroscopy for PL cam lesions. Additionally, it seeks to determine an optimal postoperative α angle threshold that correlates with improved patient-reported outcomes at 2 years.
Methods:
A retrospective analysis was performed on a cohort of 117 patients (121 hips) who underwent hip arthroscopy for femoroacetabular impingement syndrome (FAIS) between the years 2013 and 2022, with a minimum follow-up period of 2 years. Preoperative and postoperative α angles were measured on the pelvis AP and Dunn views. Clinical outcomes were assessed using the Hip Outcome Score–Activities of Daily Living (HOS-ADL), the modified Harris Hip Score (mHHS), and the Non-Arthritic Hip Score (NAHS). Receiver operating characteristic (ROC) curve analysis was used to establish an α angle cutoff associated with better functional recovery.
Results:
Patients with a postoperative α angle below 55° demonstrated significantly better functional outcomes across all scoring systems. ROC analysis confirmed that α < 55° was a strong predictor of achieving a patient-acceptable symptomatic state (PASS), with an area under the curve (AUC) of 0.849 for mHHS, 0.741 for NAHS, and 0.721 for HOS-ADL (p < 0.001). Sensitivity and specificity values varied across scoring systems, with PASS-NAHS showing a sensitivity of 88.0% and specificity of 52.6%, PASS-HOS-ADL demonstrating a sensitivity of 88.0% and specificity of 52.6%, and PASS-mHHS revealing a sensitivity of 87.6% and specificity of 75%. Multivariate logistic regression further confirmed that a postoperative α angle below 55° was independently associated with improved hip function, reinforcing its significance as a key threshold for surgical success.
Conclusion:
A postoperative pelvis AP α angle of less than 55° appears to be a key threshold for optimal recovery in patients with PL cam lesions. These findings highlight the importance of adequate resection during hip arthroscopy to enhance functional outcomes. Further research with larger patient cohorts and advanced imaging techniques may help refine postoperative evaluation criteria.
Keywords
Introduction
Femoroacetabular impingement syndrome (FAIS) is a prevalent hip condition that can result in substantial joint damage, potentially leading to degeneration and osteoarthritis. 1 FAI is a 3D deformity where the specific movements causing the most significant impingement depend on the anatomical position of the lesion. 2 It arises from 2 main hip morphology disorders: (1) cam morphology, due to a loss of concavity at the anterior head-neck junction of the femur; and (2) pincer morphology, which results from an overgrowth of the acetabular margin that excessively covers the femoral head or a combination of both.3,4 For cam impingement, the alpha (α) angle is the most common radiographic sign used for diagnosis, characterised radiologically by a decreased femoral head-neck offset ratio and α > 60°.5–7 Hip arthroscopy has become an essential tool for addressing cam lesions. Residual posterolateral cam lesions, most often located at the posterosuperior/lateral head-neck junction, are the leading cause of revision hip arthroscopy. Complete resection in this region is technically demanding, and insufficient removal frequently results in the need for a secondary procedure.8–11 Optimal correction of the cam lesion at anteroposterior (AP) radiographs (posterolateral lesion) by arthroscopy still may not be associated with the experience of the surgeon or usage of intraoperative navigation;12,13 some may offer open treatment of these lesions instead of arthroscopy.14–16
Posterolateral (PL) lesions, characterised by α > 60° on both AP pelvis and Dunn views of the hip, represent a more challenging deformity given the risk of iatrogenic injury to nearby anatomic structures. 14 Specifically, the retinacular vessels of the ascending branch of the medial circumflex femoral artery that supply the femoral head are located in the lateral synovial fold. Compared to anterior cam lesions, PL lesions are associated with an increased frequency of cartilage lesions. 17 Some surgeons consequently propose that patients with PL cam lesions should be treated with open surgical dislocation rather than hip arthroscopy.12,13 However, it has been argued that the open approach does not offer advantages in terms of visualisation or resection since the resection is in the same area, and the vascular anatomy similarly limits any distal resection. Arthroscopy may additionally eliminate the risk of trochanteric nonunion and postoperative hardware removal.14–16,18
Surgeons need a clearly defined cut-off value for the α angle on postoperative pelvis x-rays to accurately evaluate the adequacy of resection and optimise patient outcomes. A recent systematic review suggested that reducing the α angle below 55° improves outcomes, although this conclusion was based on heterogeneous imaging modalities, including x-ray, magnetic resonance imaging (MRI), and 3D computed tomography (CT). 19 Patient-acceptable symptomatic state (PASS) is 1 of the metrics developed to assess the clinical importance of patient-reported outcomes (PROs). 20 This study aims to determine the connection between the Pelvis AP postoperative α angle measurements and clinical outcomes in patients treated surgically with PL cam lesions. Additionally, it seeks to establish a cut-off value for postoperative pelvis AP radiographs indicating an angle below which patients will achieve higher rates of PASS in the second year postoperatively regarding PL cam assessment. The hypothesis is that there is a correlation between the postoperative α angle of PL cam lesions and functional hip scores.
Materials and methods
This study included 117 patients (121 hips) who underwent hip arthroscopy for femoroacetabular impingement (FAI) with a minimum follow-up of 2 years. Data were collected prospectively, and all patients were analysed retrospectively. Local ethics committee approval was obtained for the study. The diagnosis of FAI was based on clinical symptoms and radiographic findings. An α angle >55° in images obtained at 45° Dunn’s position for cam deformity and a lateral centre-edge angle (LCEA) >40° for pincer deformity were considered.21–25 Only hips with posterolateral cam morphology were included, defined as an increased α angle > 60° on both the AP pelvis and 45° Dunn views, consistent with lateral or posterosuperior extension. Patients who demonstrated isolated anterior cam morphology, characterised by an elevated Dunn α but a normal AP α, were excluded. Patients with avascular necrosis, advanced hip osteoarthritis (Tönnis Grade >1), 26 previous ipsilateral hip surgery, revision hip arthroscopy, incomplete radiographic data, or hip dysplasia (LCEA <25°) 25 were excluded. Surgery was indicated for patients with persistent hip pain affecting daily activities and unresponsive to conservative treatment for at least 3 months.
Surgical technique
The patient was positioned supine on a traction table designed for hip arthroscopy, with appropriate hip distraction achieved and supported by a perineal post. All procedures were performed by a single senior surgeon with >10 years of experience in hip arthroscopy. To enhance access and visualisation of the central compartment, a horizontal interportal capsulotomy was performed. Acetabuloplasty was conducted using a 4.5-mm arthroscopic burr. Irreparable degenerative labral tears or multiple cleavage planes were identified, and unstable flaps were meticulously debrided. Tears involving chondrolabral disruptions and the labral base were repaired using 1–3 suture anchors. Following this, traction was released, and the procedure proceeded to the peripheral compartment, where cam deformity decompression was performed. This step was confirmed through intraoperative fluoroscopy and arthroscopic dynamic examination. At the end of the procedure, the capsule remained open.
Rehabilitation
During postoperative bed rest, the patients were fitted with a derotation boot. They were also instructed to use crutches to limit weight-bearing for 2 weeks. On the first postoperative day, they started daily passive range-of-motion exercises. At week 3, they began active range-of-motion and complete weight-bearing exercises. After 6 weeks, they started strengthening and walking on a light treadmill. For the first 4 weeks, they were administered daily oral anti-inflammatory medication.
Preoperative data collection and radiographic assessment
Preoperative data were collected on continuous and categorical demographic and clinical variables, including age, sex, body mass index (BMI), and symptom duration. Radiographic evaluations were performed for all patients using anteroposterior (AP) supine pelvis radiographs and 45° Dunn views. The LCEA was measured on pelvis radiographs following the method described by Wiberg. 25 The α angle was determined from preoperative and postoperative day 1.
Pelvis AP radiographs
A positioning boot was applied before obtaining the x-ray to achieve a consistent and reliable radiological assessment. The α angle is defined as the angle between a line extending from the midpoint of the femoral neck to the center of the femoral head and a line drawn from the centre of the femoral head to the point where the bone first deviates from the normal sphericity of the head (Figure 1).6,27 All radiographic assessments were performed by 2 orthopaedic specialists.
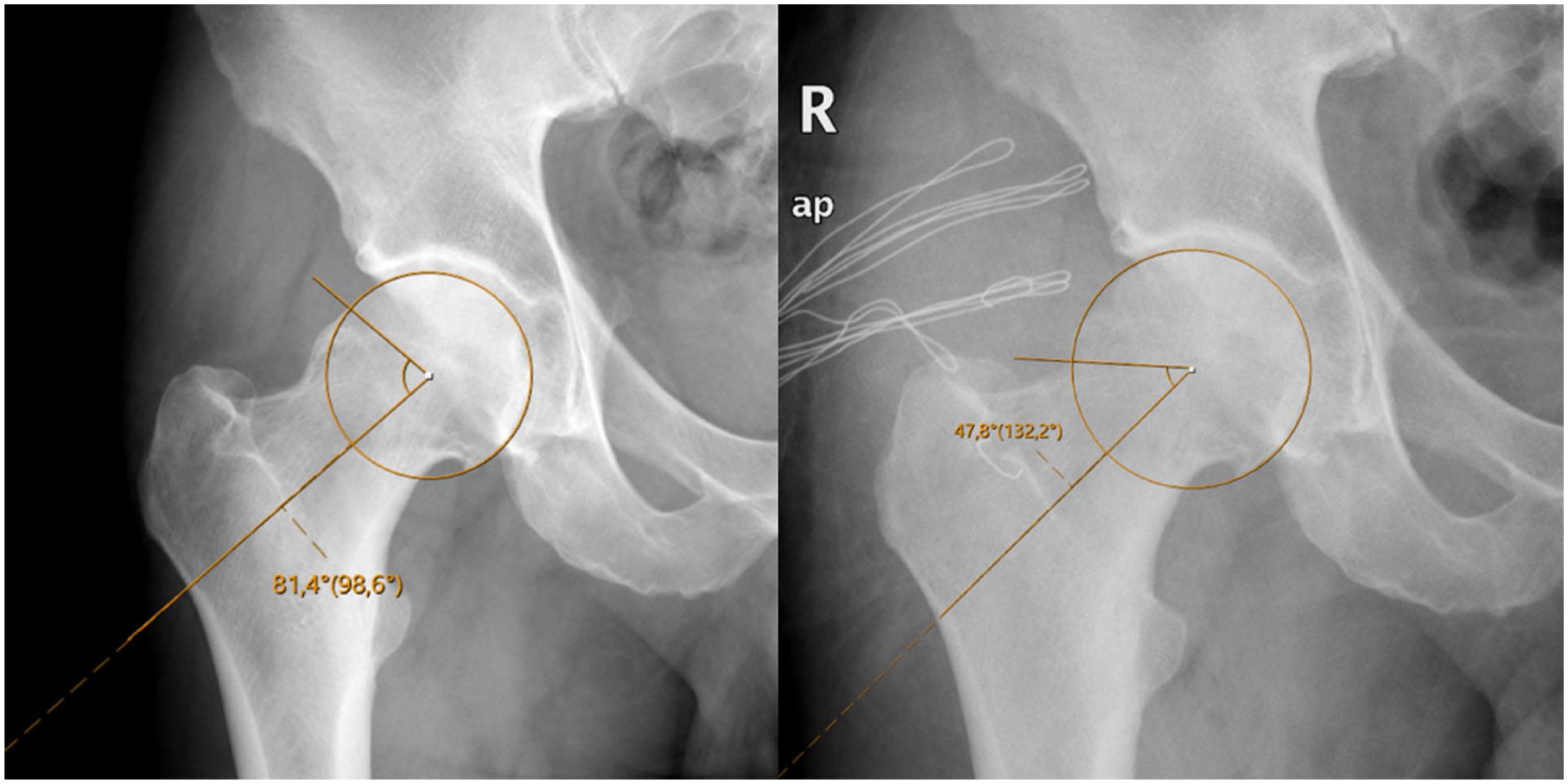
Preoperative and postoperative measurements of α angle from pelvis AP x-ray.
Patient-reported outcomes and PASS thresholds
Patient-reported outcomes (PROs), including the Hip Outcome Score–Activities of Daily Living (HOS-ADL), the modified Harris Hip Score (mHHS), and the Non-Arthritic Hip Score (NAHS) 28 were collected through direct contact with the patients. PRO questionnaires were administered at a recent postoperative clinic visit for each patient, with a minimum follow-up of 24 months.
For femoroacetabular impingement (FAI), the patient-acceptable symptomatic state (PASS) thresholds within 5 years (i.e., 2–5 years) after hip arthroscopy have been reported as 83.3 for the mHHS, 85.6 for NAHS and 86 for the HOS-ADL.28–30 Because patients were evaluated at different time points, the minimal clinically important difference (MCID) was not used. Instead, outcomes were divided into categories based on these validated PASS thresholds.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY). Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR), while categorical variables were presented as frequencies and percentages. The normality of continuous variables was assessed using the Shapiro-Wilk test. For normally distributed data, group comparisons were conducted using the independent samples t-test (Student’s t-test). In contrast, the Mann-Whitney U-test was applied for non-normally distributed variables. Categorical data were analysed using the chi-square (χ²) test, and Fisher’s exact test was used when expected cell counts were <5.
To evaluate the relationship between postoperative pelvis AP α angles and clinical outcomes, receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cutoff value, with the area under the curve (AUC) calculated accordingly. The Youden Index and Kolmogorov-Smirnov (K-S) statistic were used to identify the optimal threshold and sensitivity, and specificity values were reported. A multivariate logistic regression analysis assessed independent predictors of improved functional outcomes. Variables included in the regression model were selected using a stepwise approach, and statistical significance was set at p < 0.05 for all analyses.
Results
The study included 117 patients, 77 males (65.8%) and 40 females (34.1%). The mean age of the patients was 34.94 ± 10.97 years (range 17–61 years). The mean follow-up duration was 59.3 ± 27.5 months (range 24–127 months). The mean duration of symptoms before intervention was 18.83 ± 16.10 months (range 2–120 months). The average body mass index (BMI) was 26.11 ± 3.51 kg/m² (range 17.36–39.83 kg/m²).
To assess interobserver reliability between the 2 surgeons, intraclass correlation coefficients (ICC) were calculated. The ICC for postoperative pelvis AP α was 0.648 (95% confidence interval [CI], 0.356–0.791), indicating moderate reliability, while the ICC for preoperative pelvis AP α was 0.770 (95% CI, 0.515–0.873), demonstrating good reliability. 31
Receiver operating characteristic (ROC) analysis was conducted to assess the predictive power of pelvis AP postoperative α measurements for PL cam lesions concerning functional outcomes using NAHS, HOS-ADL, and mHHS score systems. The area under the curve (AUC) values demonstrated that the postoperative α value is a significant predictor of clinical success, particularly when pelvis AP α < 55°, across all scoring systems (Table 1).
ROC Analysis for pelvis AP α < 55° as a predictor of functional outcomes with different PASS scores.
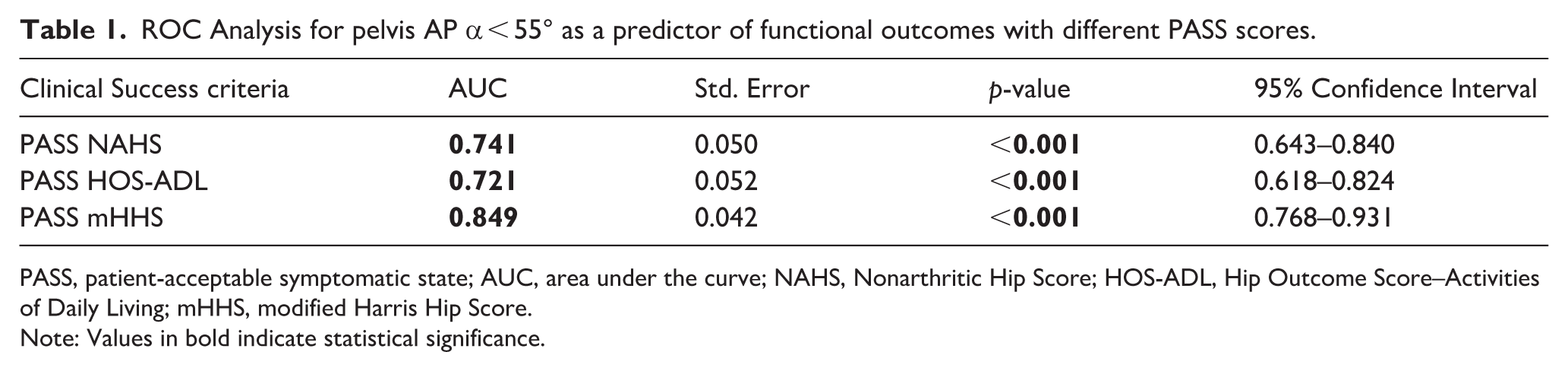
PASS, patient-acceptable symptomatic state; AUC, area under the curve; NAHS, Nonarthritic Hip Score; HOS-ADL, Hip Outcome Score–Activities of Daily Living; mHHS, modified Harris Hip Score.
Note: Values in bold indicate statistical significance.
The AUC values for achieving PASS values for NAHS, HOS-ADL, and mHHS were 0.741 (95% CI, 0.643–0.840; p < 0.001), 0.721 (95% CI, 0.618–0.824; p < 0.001), and 0.849 (95% CI, 0.768–0.931; p < 0.001), respectively. These findings indicate that the AP α < 55° measurement has moderate predictive power for NAHS and HOS-ADL while demonstrating excellent predictive capability for the mHHS scoring system (Figure 2).
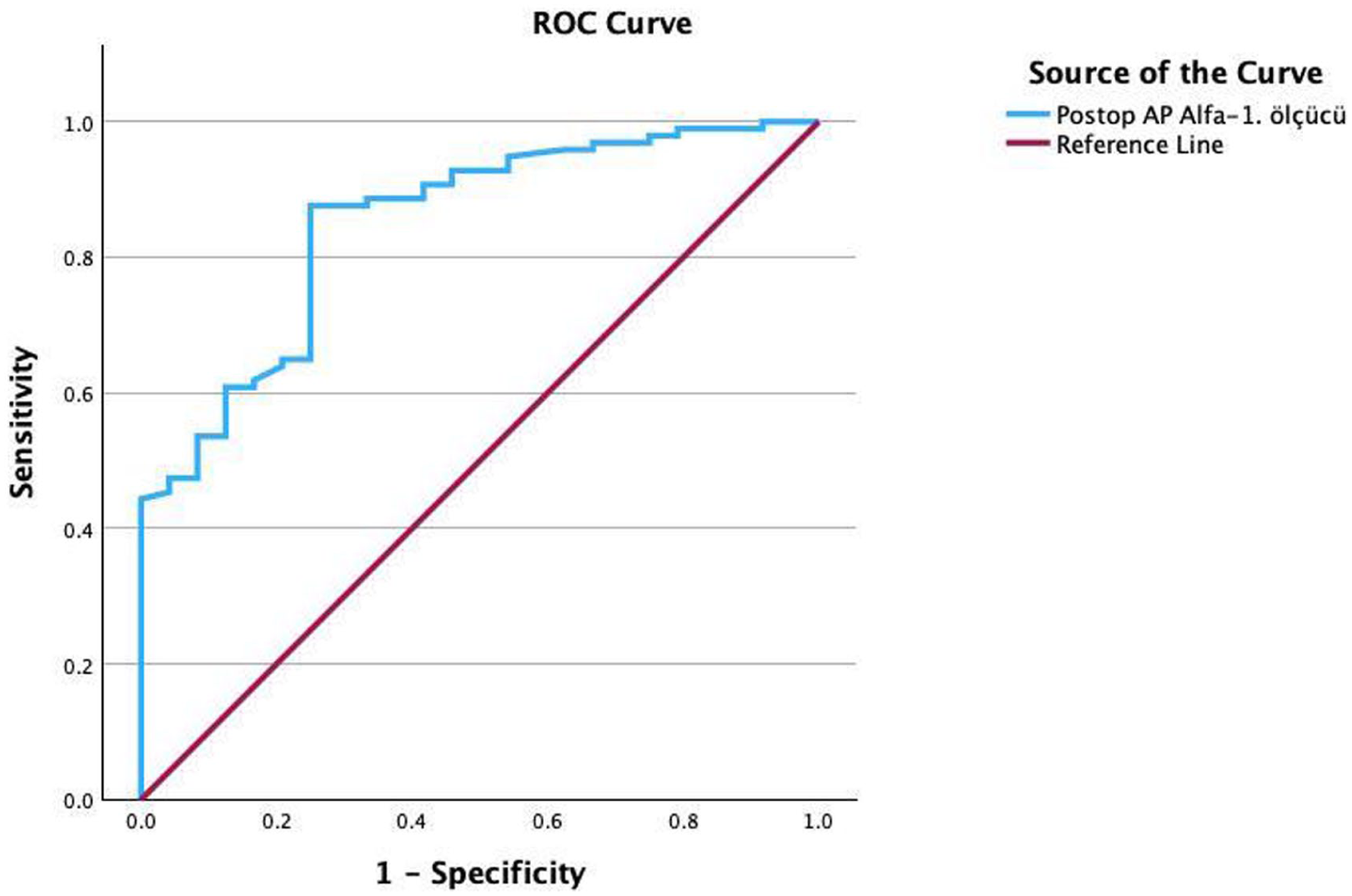
The ROC curve for the postoperative pelvis AP α angle in the mHHS scoring system shows an AUC of 0.849, demonstrating excellent predictive power for the mHHS.
The optimal cutoff value for the pelvis AP α angle was determined as 55°, which yielded the highest Youden Index (J = 0.406) and Kolmogorov-Smirnov (K-S) statistic (0.406). At the specified cutoff value where pelvis AP α < 55°, the sensitivity and specificity metrics for each scoring system were as follows: the PASS NAHS yielded a sensitivity of 88.0% and a specificity of 52.6%; similarly, the PASS HOS-ADL demonstrated a sensitivity of 88% and a specificity of 52.6%. Furthermore, the PASS mHHS reported a sensitivity of 87.6% and a specificity of 75%. These results suggest that AP α < 55° is associated with better functional recovery across all systems, particularly demonstrating excellent predictive power in mHHS.
The demographic and clinical characteristics of the patients stratified by postoperative pelvis AP α angle are summarised in Table 2. The mean age of patients in the α < 55° group was 34.23 ± 10.81 years, while in the α ⩾ 55° group, it was 37.10 ± 11.36 years (p = 0.226). No significant differences were observed between the groups in terms of BMI (p = 0.496), symptom duration (p = 0.415), and preoperative AP α angle (p = 0.806).
Demographic and clinical characteristics by postoperative pelvis AP α measurement IQR: interquartile range.
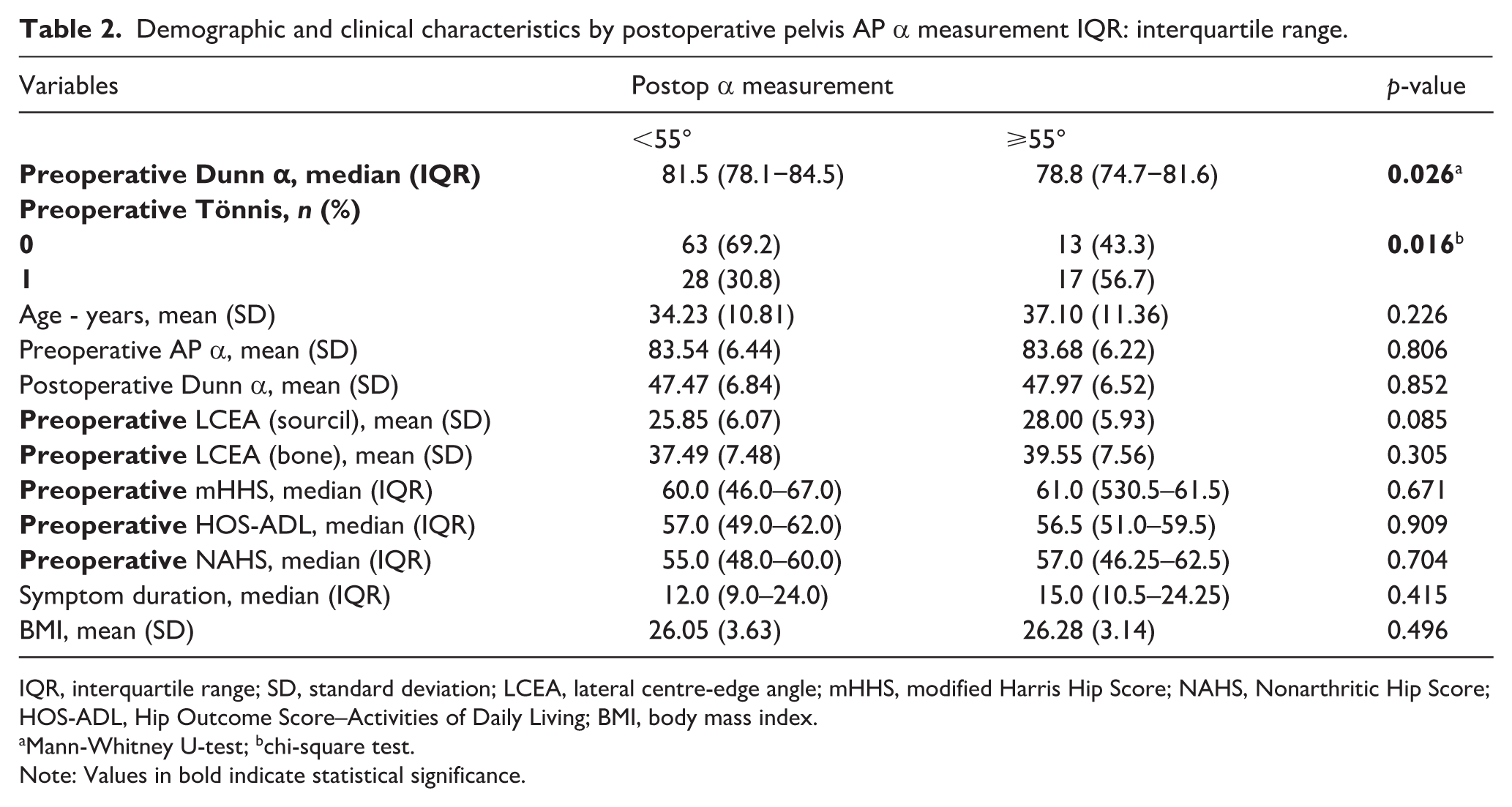
IQR, interquartile range; SD, standard deviation; LCEA, lateral centre-edge angle; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; HOS-ADL, Hip Outcome Score–Activities of Daily Living; BMI, body mass index.
Mann-Whitney U-test; bchi-square test.
Note: Values in bold indicate statistical significance.
Among functional scores, preoperative Dunn α angle values were significantly lower in the α ⩾ 55° group compared to the α < 55° group (78.8 vs. 81.5, p = 0.026). Similarly, the distribution of preoperative Tönnis scores showed a significant difference between the groups (p = 0.016), with a higher proportion of preoperative Tönnis scores of 1, patients in the α ⩾ 55° group (56.7% vs. 30.8%). This suggested that preoperative Dunn α and preoperative Tönnis scores may be important indicators of postoperative functional outcomes in patients with postoperative pelvis AP α ⩾ 55°. Other functional outcome measures, including preoperative mHHS, HOS-ADL, and NAHS, did not show statistically significant differences between the 2 groups (p > 0.05).
Multivariate logistic regression analysis further confirmed the predictive significance of postoperative pelvis AP α < 55°. The results demonstrated that postoperative pelvis AP α < 55° was independently associated with improved functional outcomes. The stepwise regression analysis further confirmed that preoperative Tönnis score and preoperative Dunn α were not statistically significant in predicting outcomes, emphasising the dominant role of achieving the postoperative pelvis AP α < 55° for postoperative success.
Discussion
The primary objective of this study was to determine the optimal postoperative α angle threshold in PL cam lesions that correlates with improved functional outcomes. Residual cam lesions, especially those with an α angle >55° on lateral Dunn radiographs, are known to negatively affect clinical outcomes. 8 However, the current literature lacks a defined cut-off value for the α angle, nor does it clarify how much the pelvis AP α angle must be decreased to attain improved functional outcomes for PL cam lesions.
Posterolateral cam lesions are among the most challenging to resect due to their anatomical location and proximity to critical vascular structures. Traditionally, these lesions have been considered more global or severe than isolated anterior cam lesions, as they are often visible on AP radiographs and lateral Dunn view.9–11
Recent studies have proposed various cut-off values for postoperative α angles to predict functional recovery and cartilage damage risk. For instance, it has been suggested that α ⩾ 70° on AP and ⩾56° on lateral views predicts advanced chondral lesions. 32 In comparison, a threshold of α ⩾ 60° has been widely accepted as a benchmark for cam pathology classification. 17 Rogers et al. 33 further reported that an increased AP α angle above 55° was independently associated with more severe cartilage damage, while Tang et al. 32 found that a 7.1° increase in AP α angle and a 5.2° increase in Lauenstein α angle (analogous to Dunn) resulted in a 1-grade increase in acetabular chondral injury, with AP α ⩾ 70° and Lauenstein α ⩾ 57° serving as predictive thresholds.
The study by Larson et al. 34 further supports these findings by comparing patients with lateral impingement (α angle > 60° on both Dunn and AP views) and those without lateral impingement (α angle > 60° on Dunn but not on AP view). Their study found that while lateral impingement patients had larger preoperative α angles and greater acetabular and femoral cartilage damage, postoperative α angles, PROs and survivorship were similar to those without lateral impingement. This suggests that even more severe and laterally located cam deformities can be adequately resected arthroscopically, yielding comparable long-term outcomes.
Our findings align with these prior studies and contribute further evidence supporting a functional α angle threshold. We observed that reducing the postoperative pelvis AP α angle to <55° significantly predicted improved functional scores. This is consistent with recent literature investigating cut-off values for favourable clinical outcomes. Gürsan et al. 35 reported that a postoperative Dunn α ⩽ 48.3° was strongly associated with higher PASS rates for anterior cam lesions, with a sensitivity of 0.75 and specificity of 0.69. Similarly, Monahan et al. 36 found that a postoperative α angle ⩽46° correlated with a higher return-to-sports rate. Based on our results, we propose that achieving a postoperative pelvis AP α < 55° should be considered a key surgical goal in treating PL cam lesions. This threshold was associated with better functional recovery and improved PROs, reinforcing the importance of thorough resection in these cases.
Despite the possible technical difficulties in accessing and completely resecting superolateral/posterior cam deformities, some studies still advocate open surgical treatment.14–16 Our study also identifies surgical goals and aligns with the findings by Larson et al., 34 emphasising that the optimal amount of resection is crucial for guiding arthroscopic techniques for these challenging lesions. By establishing a postoperative pelvis AP α threshold, our study provides valuable insights that can help optimise arthroscopic management and improve functional outcomes in patients with PL cam morphology without the need for potential open surgery.
Future multicentre studies with larger cohorts are needed to refine postoperative α angle thresholds. Integrating advanced imaging techniques, like 3D CT analysis, may enhance preoperative planning and postoperative assessment for more precise surgery corrections.
There are some limitations. This study’s retrospective nature is limited, and a prospective study would provide stronger evidence. Radiographic assessments relied on AP and Dunn view X-rays, which may not fully capture 3D cam morphology – 3D CT or MRI could improve accuracy. Interobserver variability in α angle measurements remains a concern, though 2 orthopaedic specialists conducted evaluations. Other factors, including the severity of cartilage damage, labral condition, femoral version, and surgeon-related technical variation, may also have an effect on postoperative results. These aspects were not set as exclusion criteria and could not be fully controlled within this cohort and should therefore be kept in mind when interpreting the findings. Despite these limitations, this study provides valuable insights into optimal postoperative α angles for PL cam lesions and supports arthroscopic treatment efficacy.
Conclusion
A postoperative pelvis AP α angle of less than 55° appears to be a key threshold for optimal recovery in patients with PL cam lesions. These findings highlight the importance of adequate resection during hip arthroscopy to enhance functional outcomes. Further research with larger patient cohorts and advanced imaging techniques may help refine postoperative evaluation criteria.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.