
Abstract
Introduction:
This study aimed to compare preoperative education level, income level, and geographical birthplace between patients undergoing metal-on-metal hip resurfacing (MoM-HR) and those receiving a conventional uncemented total hip arthroplasty (THA).
Methods:
All patients with osteoarthritis who underwent a MoM-HR or an uncemented THA registered in the Swedish Arthroplasty Register 1999–2014 were included (n = 15,871). National databases provided additional information on household income and the highest achieved education. 1481 MoM-HR patients were matched to 1481 uncemented THA patients based on age, sex, and Charlson comorbidity index. Odds ratios (OR) of MoM-HR surgery depending on socioeconomic variables were calculated using logistic regression analysis.
Results:
The OR of having MoM-HR surgery was lower among patients with lower education level compared to those with a university degree. Also, 37% of the MoM-HR patients had an income in the 2 highest quintiles compared to 32% of uncemented THA patients. There was no difference in accessibility of MoM-HR surgery between patients born in or outside Sweden.
Conclusions:
In Sweden, within a universal healthcare coverage system, lower socioeconomic status in terms of education level was associated with decreased accessibility to innovative hip surgery, i.e., MoM-HR.
Keywords
Introduction
Recent studies have highlighted socioeconomic disparities in joint arthroplasty.1–3 The statutory right to equal quality of healthcare is considered a cornerstone of healthcare in Sweden but despite a universal healthcare coverage system, inequalities in health associated with socioeconomic status (SES) persists in Sweden as in many other European countries. 4
Patients with lower SES do not only have a higher risk of unhealthy behaviour but also of morbidity and mortality. 5 Decreased access and slower uptake of innovative healthcare technologies such as new surgical methods, e.g. robot-assisted prostatectomy, have been described in patients with lower income and other SES variables. 6
Given the steady increase of osteoarthritis (OA), 1 of the main causes of global disability, it is reasonable to anticipate a corresponding rise in the demand for total hip arthroplasty (THA).7,8 This raises the concern of health equity both at the individual and at the group level. Despite 2 decades having passed since the Institute of Medicine’s appeal to confront inequality, uneven access to joint arthroplasty has not been sufficiently confronted.9,10 Moreover, patients of immigrant background seemed to have up to 60% increased risk of preoperative problems before THA compared to patients born in Sweden. 11 Reports on the relationship between SES and THA are sparse, mostly focusing on postoperative outcomes. 12 However, it is equally important to study how SES relates to the choice of THA implant and to accessibility to new innovative surgeries which could have implications for healthcare policy and practice. 13
The third-generation of metal-on-metal hip resurfacing (MoM-HR) was introduced into clinical practice in the early 90s as an innovative hip implant constituting all-metal articulation. 14 MoM-HR was heavily marketed by manufacturers and quickly gained popularity and market uptake in the first decade of the 21st century as an alternative for a more active population due to its expected durable surface, and “anatomic” hip restoration. 15 The first third-generation MoM-HR surgery performed in Sweden was in 1999. 16 MoM-HR in Sweden peaked around 2007 and accounted for about 2% of all hip replacements, compared to 9% in the UK.17,18 Its use has decreased worldwide due to, among other factors, a higher risk of reoperation and market recalls of specific designs.19,20 The method has been more or less abandoned in Sweden since 2014; however, it is still used in several European countries. 16 Regardless, the healthcare systems in many countries have a considerable burden of surveillance on previously implanted MoM-HR. New hip resurfacing concepts are currently under evaluation. These include ceramic-on-ceramic systems and the recently introduced metal-on-polyethylene articulation. Moreover, innovations such as the reverse hip replacement systems suggest continued assessment and interest in new innovative joint resurfacing options. 21 Therefore, it is clinically important to study SES influence on the utilisation of innovative surgery, such as MoM-HR.
We hypothesised that patient SES influences utilisation of innovative hip arthroplasty. We have not found any previous study on access to innovative hip implants related to patient SES. In this study, we aimed to compare patients operated on with a conventional THA with patients operated on with the third-generation MoM-HR focusing on differences in preoperative SES.
Patients and methods
Study design and setting
This is a nationwide register-based case-control study of THA patients operated on in Sweden between 1999 and 2014. The data were collected from the Swedish Arthroplasty Register (SAR), the National Patient Register (NPR), and the Longitudinal Integration Database for Health Insurance and Labor Market Studies (LISA), Statistics Sweden.
SAR is a nationwide register with practically complete coverage of all patients receiving a hip arthroplasty in Sweden. It registers implant model used, type of fixation, BMI, and the year of surgery. The NPR is a database from the Swedish Board of Health and Welfare and covers all inpatient visits since 1987, with nationwide coverage and high validity. 22 Each record in the NPR corresponds to a single hospital episode. It also contains patient age, sex, dates of admission and discharge, Charlson comorbidity index, birthplace, all diagnoses, and surgical codes that are of relevance to hospital admission. LISA is an integration database run by Statistics Sweden that includes all persons 16 years of age or older. It integrates data from different registers on the labour market, such as the National Education Register, registers obtained by the National Social Insurance Board on transactions from different income security programs as well as from Taxation Registers to obtain information on individual and household disposable income. 23 The 12-digit personal identification number assigned to all Swedish residents at birth or immigration allows linkage between the registries.
All patients operated on with a THA 1998–2020 due to primary osteoarthritis coded according to the International Classification of Disease (ICD-10) were retrieved from the SAR. The SAR data wwere linked to NPR data using coded anonymous identifiers. Only patients registered in both registers were used for further analysis. Finally, education and income data were retrieved from LISA.
The study was approved by the regional ethics committee and the Swedish ethical review authority; Dnr: 2013/581–31 (+ amendments: 2016/2251-32, 2018/177-32, 2018/1068-32, 2018/1832–32, 2020/04776, 2020/06182), Dnr: T855-17. According to the ethical approval there was no need for participant consent.
Participants
A total of 222,664 patients underwent a THA-classified surgical procedure between 1998 and 2020 in Sweden. We used only the first hip arthroplasty observation in cases of more than one observation during the study period. We excluded patients with THA after hip fracture diagnosis (ICD-10: S72.0-9, M80.0F, M84.0F, M84.1F, M84.2E, M84.2F, M84,3F, M84.4F), hip malignancy (ICD-10: C40.2, C41.4, C79.5, C90.0, D16.9, D21.2, D48.0), re-operation (ICD-10: T84.0-3F, T84.5-6F, T84.8F, T91.2 and T93.1) or any arthritis diagnosis other than primary osteoarthritis (ICD-10: M00.8, M00.9F, M02.9F, M05.8-9F, M06.9F, M07.3F, M08.0F, M12.2F, M13.8, M15.0, M16.2-7, M16.9, M21.0-1F, M24.4F, M24.6F, M25.5F, M32.9, M36.2, M45.9, M65.9F, M79.6F, M86.6F, M87.0-3F, and M91-M96). A total of 207,060 patients had been operated on with THA due to primary hip osteoarthritis (ICD-10: M16.0, and M16.1). As MoM-HR was reserved primarily for a younger and more active population in Sweden, and cemented THA was disproportionately used in older patients with higher comorbidity in Sweden, we only included patients with an uncemented THA, which during the study period was mostly used in this population, in the control group. 24 Thus, we excluded patients with cemented THA (both acetabulum and femur fixed with cement) (n = 146,334) and hybrid THA (1 of either femur or acetabulum fixed with cement) (n = 25,581). As clinical practice changed in 2014, after which MoM-HR was not performed in common practice in Sweden, we also excluded all patients operated on after 2014 (n = 18,269). We were left with 16,876 patients with either uncemented THA (no component fixed with cement) (n = 15,378) or a MoM-HR (n = 1498). We further excluded patients who were not registered in the NPR (n = 780) and 2 patients who were coded as uncemented hip resurfacing. As no patients were operated on with MoM-HR before 1999 we excluded 223 uncemented THA who were operated on in 1998. Accordingly, we were left with 14,390 uncemented THA and 1,481 MoM-HR for the final analysis (Figure 1). MoM-HR was performed at 29 different hospitals, both in university and regional hospitals, and in 15/21 regions in Sweden.
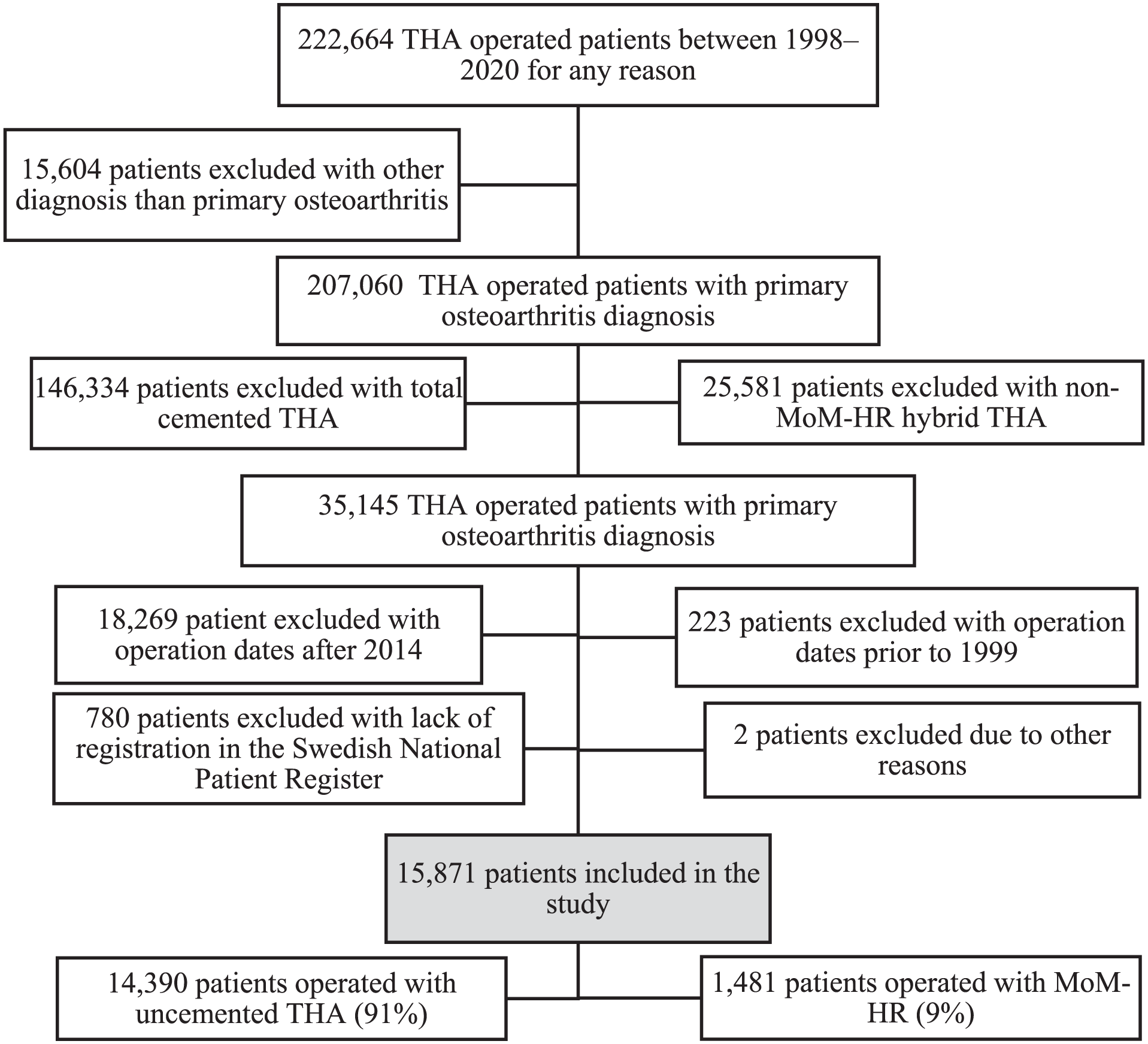
Flowchart of patient selection.
Exposure and outcome
Exposure was defined as the highest educational level prior to surgery, disposable income the calendar year prior to surgery, and country of birth. Education level was coded into 4 levels: primary and secondary school ⩽9 years, upper secondary school ⩽3 years, post-secondary education <3 years, and post-secondary education ⩾3 years. We used equivalence scales provided by Statistics Sweden to account for household differences in consumption needs. 23 These scales assign the weight of 1 for a single household and the weight 1.51 for a cohabiting couple. For additional members of the household 0.6 is assigned for adults, 0.52 for the first child, and 0.42 for each additional child. To obtain the disposable income per family consumption weight for each individual for each year we divided the family disposable income with the consumption weight in the family. The observations were later grouped into 5 income quintiles for the year of surgery. Each quintile consisted of 20% of the entire sample, i.e. 1st quintile included 20% of the sample with the lowest income, 2nd quintile included 20% of the sample with the second lowest income, and so forth. Country of birth was stratified into 2 groups: born in Sweden and born outside Sweden.
The outcome was the type of hip prosthesis (MoM-HR vs. uncemented THA) in 1999–2014.
Statistical analysis
Data are presented as median (interquartile range (IQR)), or percentage, as appropriate. Missing values were not imputed for statistical analysis. The level of statistical significance was set at p < 0.05. Comparisons between the 2 groups were assessed using the chi-square test (χ2) for nominal variables.
Propensity score index matching, based on age at surgery (categorised as <58 years or ⩾58 years), sex, and Charlson comorbidity index (1 year prior to the surgery), 25 was performed with a 1:1 matching (1 MoM-HR vs 1 uncemented THA). We were unable to find matches from the uncemented THA group based on the year of surgery for certain years due to the unequal distribution of patients across different years. While matching with 2 or more controls would yield larger study samples, it risked imbalance across specific surgical years. Subsequently, we were left with 1,481 MoM-HR patients and 1,481 uncemented THA patients. Due to missing data for 1 or more outcome variables, 41 uncemented THA patients and 17 MoM-HR cases were excluded from the logistic regression analysis.
Logistic regression analysis, incorporating key demographic variables, was employed to calculate the odds ratio (OR) of undergoing MoM-HR surgery. The ORs were adjusted for age, sex, Charlson comorbidity index, income, education, and whether patients were born in Sweden or abroad. ORs with a 95% confidence interval (95% CI) below 1 or both above 1 were considered statistically significant.
Statistical analyses were conducted using Stata 18.0 (Stata Corporation, College Station, TX, USA) and Statistical Analysis Systems (SAS) version 9.4 (SAS Campus Drive, Cary, NC, USA).
Results
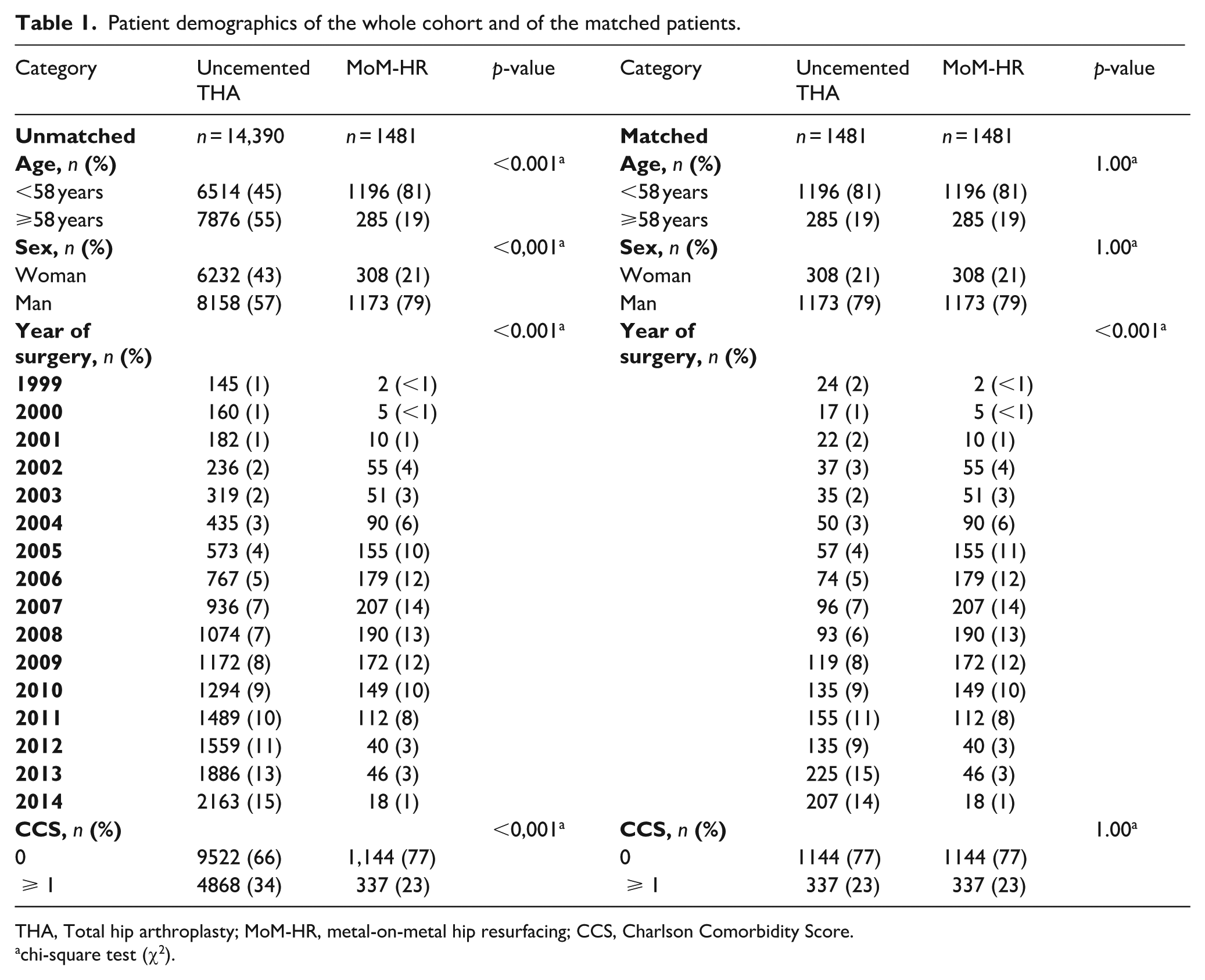
The final study population comprised 15,871 patients with a median age of 58 years (IQR 52–63 years). Of this population, 59% were men, and 67% had a Charlson score without any comorbidity. Prior to propensity score index matching, the uncemented THA group (n = 14,390) was significantly different from the MoM-HR group (n = 1481). The uncemented THA group comprised of older patients (55% were older than 58 years in the uncemented THA group vs. 19% in the MoM-HR group, p < 0.001), fewer men (57% vs 79%, p < 0.001), and had a higher Charlson comorbidity index score (p < 0.001). The propensity score index matching adjusted for these differences (Table 1).
Patient demographics of the whole cohort and of the matched patients.
THA, Total hip arthroplasty; MoM-HR, metal-on-metal hip resurfacing; CCS, Charlson Comorbidity Score.
chi-square test (χ2).
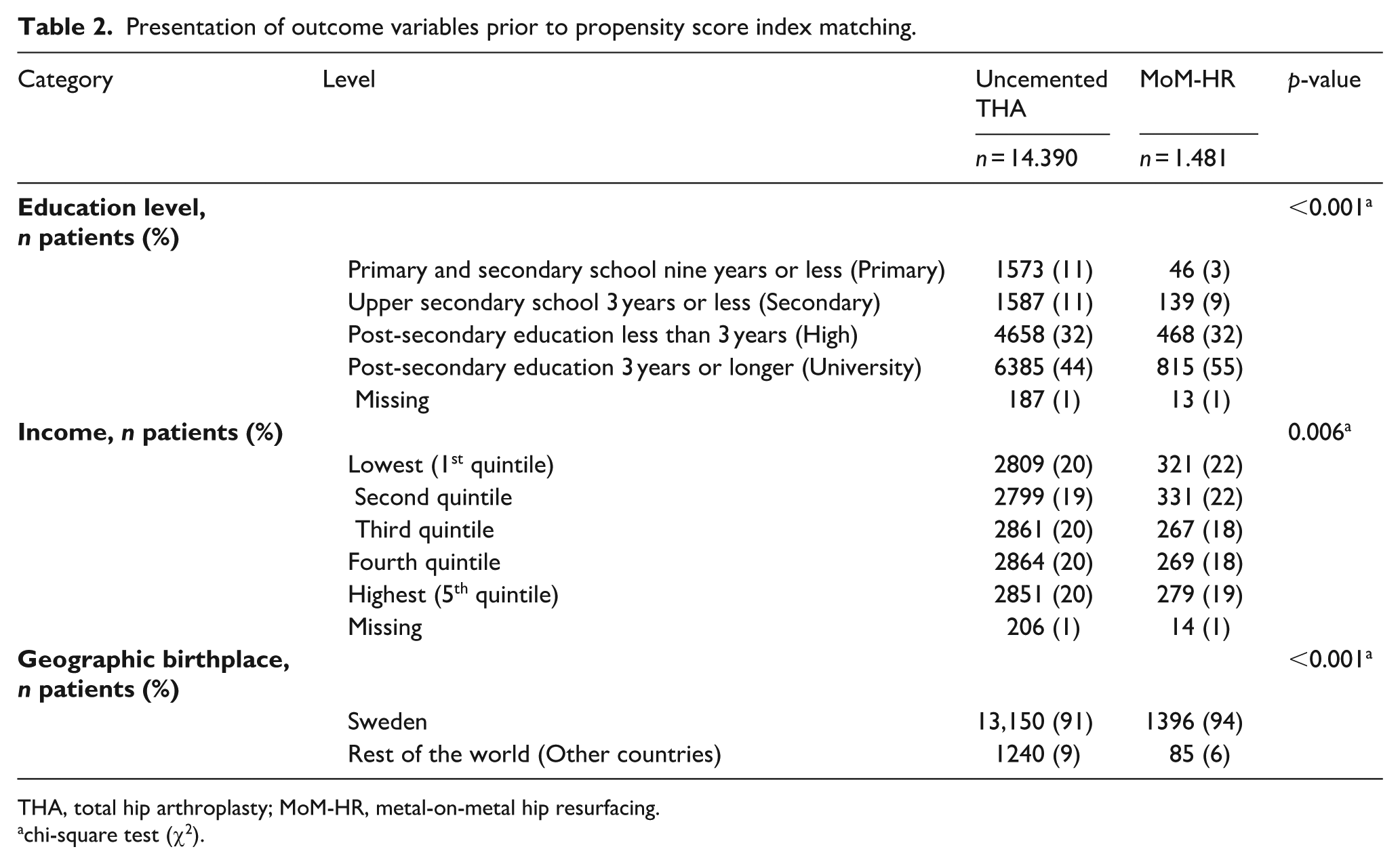
In the whole study population, 11% of the uncemented THA group did not attend upper secondary school or higher, and 44% had the highest education level, compared to 3% and 55% respectively in the MoM-HR group (Table 2). Additionally, 40% of patients in the uncemented THA group had an income in the two highest quintiles compared to 37% in the MoM-HR group. In total, 92% of all patients were born in Sweden (91% in the uncemented THA group vs. 94% in the MoM-HR group, p < 0.001).
Presentation of outcome variables prior to propensity score index matching.
THA, total hip arthroplasty; MoM-HR, metal-on-metal hip resurfacing.
chi-square test (χ2).
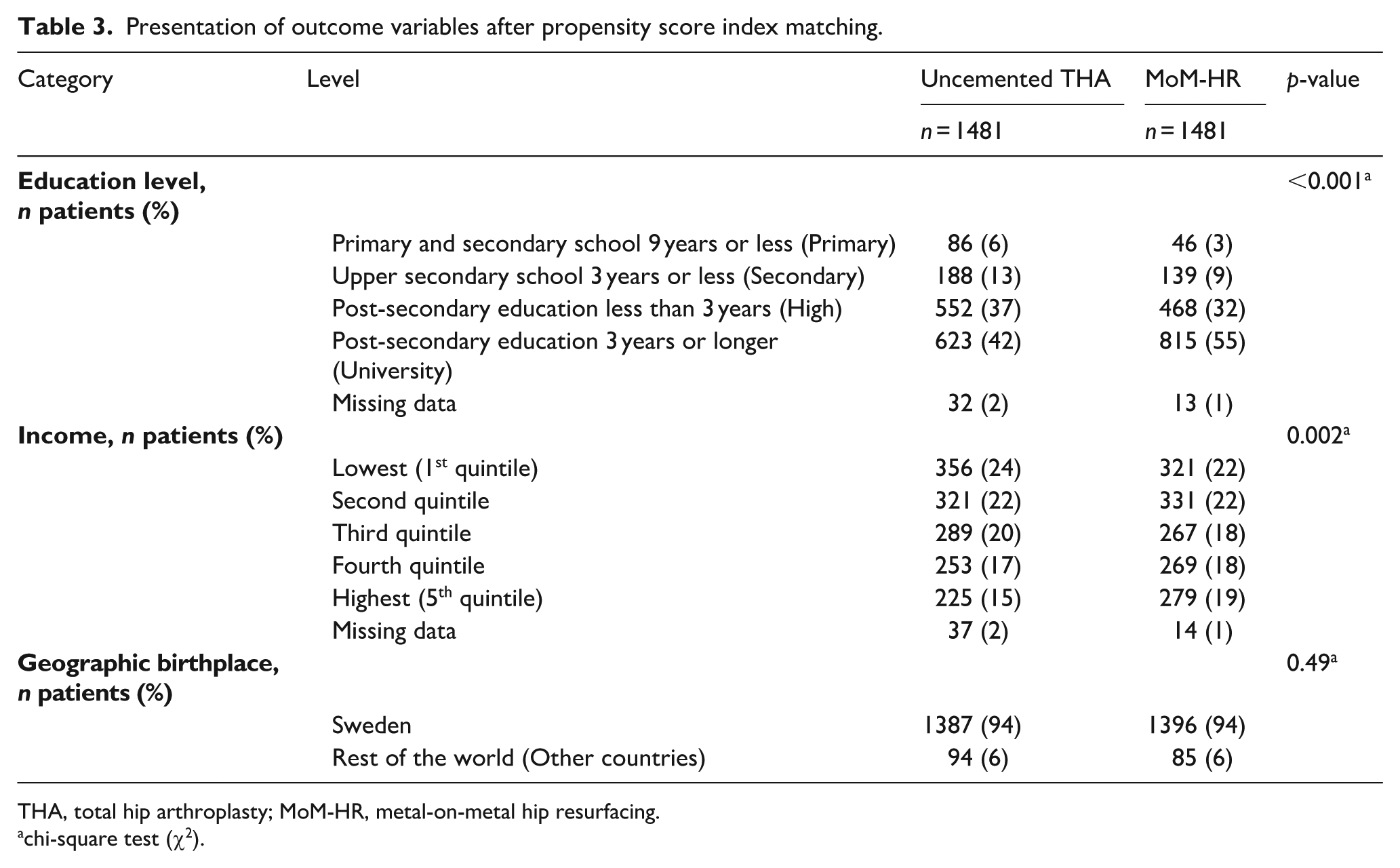
After propensity score index matching, the differences in the proportion of patients having the highest education level remained. The MoM-HR group had a statistically higher education- and income levels, compared to the uncemented THA group (Table 3). 93% of patients in the uncemented THA group and 94% in the MoM-HR group were born in Sweden (p = 0.49).
Presentation of outcome variables after propensity score index matching.
THA, total hip arthroplasty; MoM-HR, metal-on-metal hip resurfacing.
chi-square test (χ2).
In the logistic regression analysis primary education (OR 0.42; 95% CI, 0.29–0.62), upper secondary education (OR 0.57; 95% CI, 0.45–0.73), and post-secondary education less than 3 years (OR 0.66; 95% CI, 0.56–0.78) were associated with a lower probability of MoM-HR compared to patients with university education 3 years or more (Figure 2). There was no significant difference in the OR of MoM surgery when the highest income quintile group was compared with other income quintile groups. We found no association between patients born in Sweden or abroad and MoM-HR surgery (OR 1.09; 95% CI, 0.77–1.52).
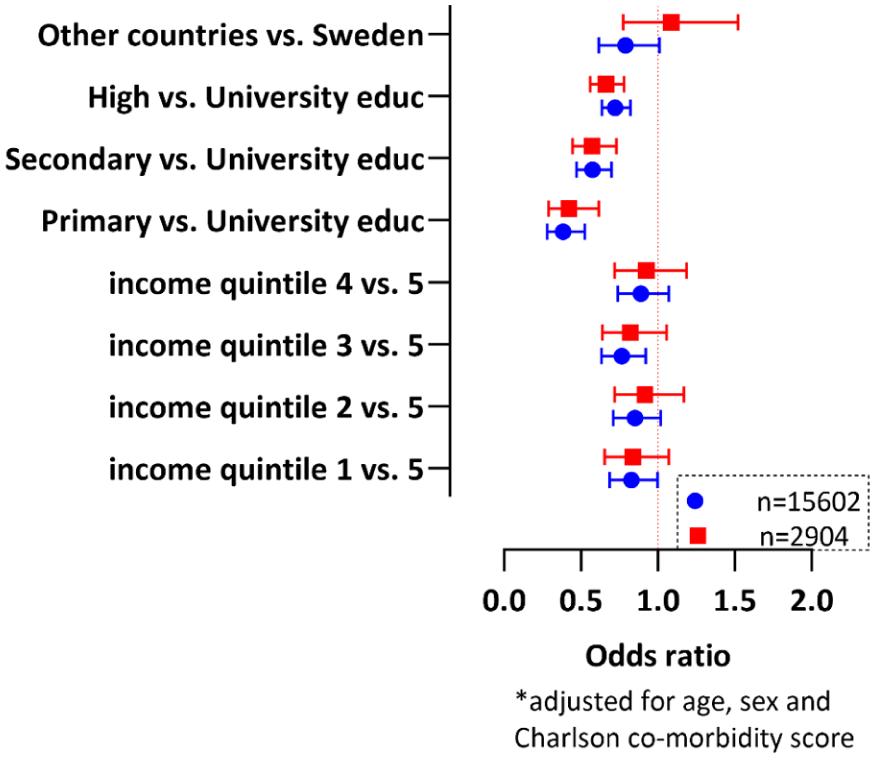
Graphic representation of socioeconomic variables after multinomial logistic regression analysis. Boxes and circles represent the odds ratios (ORs), and whiskers represent the 95% CI. The blue circles represent the ORs in the unmatched group and the red boxes represent patients after propensity score index matching. The ORs were considered statistically significant when the confidence interval was either lower than 1 or higher than 1. The reference populations were patients born in Sweden, patients with university education, and patients with an income in the highest (5th) quintile. The results were adjusted for every variable in the figure and also adjusted for age, sex, and Charlson comorbidity index. 269 (17 MoM-HR patients and 252 uncemented total hip arthroplasty patients) in the total cohort and 58 patients in the matched population (17 MoM-HR patients and 41 uncemented total hip arthroplasty patients) were excluded from the logistic regression analysis due to missing data for one or more outcome variables.]
A majority of the MoM-HR procedures (779 of 1481, 53%) were performed in regional hospitals. Additionally, 24 MoM-HR procedures (2%) were performed in private hospitals.
Discussion
This register-based case-control study found that high education level was associated with an increased probability of receiving a MoM-HR surgery. The MoM-HR group had higher education and income levels than the uncemented THA group. Our results highlight potential socioeconomic disparities in innovative orthopaedic surgery.
Wetterholm et al. 26 reported that the rate of hip arthroplasty increased with higher SES, i.e. it was most common in patients with high income, university education, and those with legislating occupations or senior officials. This aligns with our results, which shows that about 45% of our study population consisted of patients with a university degree of at least 3 years. In contrast, in the general Swedish population, only about 20% of residents from 25–64 years old had the highest educational degree during the study period. 27 Higher education is associated with a higher uptake of health-related technological progress. 28 Our study focused on potential predetermined SES factors for innovative hip arthroplasty. We found that 55% of MoM-HR patients compared to 44% of uncemented THA patients had the highest education level and that university education level was associated with a higher probability of MoM-HR surgery than lower education levels. This difference is in line with the previously described increased likelihood of cruciate ligament reconstruction (CLR) among patients with the highest level of education. 29 Language limitations and insufficient communication and information from health care providers could cause barriers in equity. 30 To the best of our knowledge, our study is the first to investigate the association between type of THA implant and level of education.
Our finding that lower income patients received an innovative hip prosthesis to a lesser extent correlates with studies in other medical fields. 31 Low-income patients are also under-represented in the utilisation of technology-assisted hip and knee arthroplasties that are used for improved surgical precision. 13 In line with the data from a nationwide insurance claims database, where low SES was associated with greater complication- and re-admission rates in THA, our findings indicate an association between patient SES and the likelihood of receiving innovative hip procedures even within universal healthcare coverage settings. 2 In Sweden and the rest of Europe, the death rate is higher among patients with low education. 4
A study from 2013 found no difference in reoperation rates 2 and 13 years after THA between immigrants and non-immigrants in Sweden. 32 However, continuous widespread inequality in access to hip replacement surgery in the UK, mainly affecting lower SES patients and groups of ethnic minorities has been found. 33 This is in concordance with reports of immigrant patients in Sweden being more dissatisfied and having more problems following THA compared to the non-immigrant population. 34 Even though we did not find any association between implant choice and geographic birthplace, it is of great importance that equity in THA is ensured so that no patient group is overlooked or underserved. 35
A recent systematic literature review on innovations in healthcare underlined the importance of co-creation between the caregivers, patients, governmental agencies, and market actors. 36 Notably, an innovative surgical implant does not always turn out to be favourable compared to a conventional implant, so the end result might be that patients receiving a newer implant become the disadvantaged ones. An example of this is described in a qualitative study of patient experiences living with the Articular Surface Replacement (ASR) implant, a MoM-HR arthroplasty known for its high complication rate and subsequent recall. 37 Patients reported that they were satisfied with the implant despite the recall as long as they stayed asymptomatic. This suggests that a model of care valuing patient engagement and information sharing might be especially critical in managing the expectations and experiences of patients from varying SES backgrounds who might have different levels of access to innovative healthcare technologies.
The introduction of new implants and medical technologies should follow a stepwise introduction algorithm based on strong data. 38 Therefore, we were surprised that most MoM-HR procedures were performed in regional hospitals, not university hospitals, since their assignments differ in Sweden. Regional hospitals are focused on established large-volume procedures such as routine primary joint arthroplasty. It has been argued that the introduction of the third-generation MoM-HR was not based on solid evidence. 39 Interestingly, prior to propensity score index matching we found that MoM-HR operated patients to a greater extent were men, younger, and had a lower comorbidity level compared to the uncemented THA group. The over-representation of men can partly be attributed to recommendations of only using the implants in patients with larger femoral heads (more common in men). 15 On the other hand, the difference in age and comorbidity between the groups is puzzling, as during the study period in Sweden, uncemented THA was also reserved for younger patients with fewer comorbidities. 24 Younger and healthier patients could have been over-represented as the implementation of the third-generation MoM-HR was not necessarily driven by the healthcare profession but by marketing and the influence of different patient communities. Even if the surgical technique is ultimately the surgeon’s choice, it appears that patients with higher education more actively sought innovative hip surgery, i.e., were able to make individual-informed health-related decisions. 40 It is not likely that surgeons choose different implants based on patient SES. Health literacy has been increasingly considered over the past decades. It refers to the individual’s ability to find, understand, and use health-related information and to the responsibility of organisations, such as healthcare providers, to ensure that all patients get equal possibilities to make “well-informed” health-related decisions.41,42
The primary strength of our study lies in the meticulous application of propensity score index matching, including the Charlson comorbidity index, effectively mitigating the risk of confounding in our 1:1 match. Additionally, the high validity and nationwide coverage of the used registers enhances the robustness of our findings.
Nonetheless, we acknowledge certain limitations. First, the exclusion of cemented THA and hybrid THA resulted in analyzing a relatively low number of uncemented THA surgeries which limited our ability to find more than one exact match for every MoM-HR case. This potential limitation may impact the strength of our results, as even younger and healthier patients could have been operated on with cemented or hybrid THA due to other reasons such as surgeons’ preference, bone quality, or hospital policy. Also, patients receiving a MoM-HR likely proactively sought out surgeons performing this procedure, while patients operated on with uncemented THA in most instances probably did not opt for a specific implant. The missing outcome data for 269 patients in the whole study population and 58 patients in our matched cohort could pose a risk for selection bias in our logistic regression analysis, although we do not believe that would change or results significantly.
Second, we were unable to match the groups based on the year of surgery due to the imbalance of distribution (Table 1). 71% of MoM-HR patients were operated on between 2005–2010, while 71% of uncemented THA patients were operated on between 2008–2014. This could affect the association between income and choice of implant, as the employment rate and overall national income levels vary with time. To handle this, we would have needed a larger patient sample, which was not possible.
Third, our study lacks information on body mass index (BMI) and smoking status, variables that could differ between the groups, given that MoM-HR is typically considered for more active patients. We lacked information on the smoking status of all patients and the BMI of about 50% of the patients. Matching based on Charlson comorbidity index scores was aimed at compensating for potential differences, but the absence of BMI and smoking data remains a notable limitation.
Fourth, we did not perform a distributional cost-effectiveness analysis (DCEA), i.e. an analysis to address the challenges of quantifying the health benefits and costs of a new technology across different subpopulations.43,44 With such analysis one can both study the net health benefit and the equity impact of a new innovation. It is, however, evident from our results that the population with high SES was adversely affected by the choice of MoM-HR surgery.
Lastly, while regional differences could potentially act as confounding factors, most patients were operated on in various regional hospitals across the country rather than centralised at university hospitals, so we do not believe this has impacted our results.
Conclusion
In our study, the adoption of the third-generation MoM-HR in Sweden was more prevalent among individuals with high educational levels and high incomes. It is crucial to acknowledge that socioeconomic disparities exist and that if left unaddressed, unwarranted variations in the adoption of innovative surgical techniques and implants may occur. It is imperative to recognise and address these inequalities before integrating new approaches into routine practice. Our findings contribute valuable insights into the dynamics of healthcare utilisation and will help guide strategies to ensure equitable access to cutting-edge orthopaedic interventions.
Footnotes
Acknowledgements
We thank the Swedish Arthroplasty Register, Swedish National Patient Register, the Longitudinal Integration Database for Health Insurance and Labor Market Studies, and Statistics Sweden for data provision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received from Region Stockholm. Dnr: RS2019-1054, RS2022-0674.