
Abstract
Background:
The objective of this study was to determine the effect of bone marrow aspirate concentrate (BMAC) on long-term patient outcomes when used as an adjuvant to acetabular repair of the labrum.
Methods:
A systematic review and meta-analysis were completed following PRISMA 2020 guidelines. Included in the analysis were controlled studies which assessed functional outcomes via the International Hip Outcome Tool-33 (iHOT-33) 12 or 24 months after acetabular repair with BMAC adjunct. 4 studies totaling 315 participants were analysed.
Results:
Pooled effect sizes for iHOT-33 scores were not significantly different between control and treatment groups at 12 (p = 0.14, Cohen’s D ≏ 0.79) or 24 months (p = 0.30, Cohen’s D ≏ 0.56).
Conclusions:
Non-significant trends in favour of BMAC augmentation were found in this study. However, the trends reported are promising and warrant further investigation with further randomised controlled trials.
Introduction
The acetabular labrum is the fibrocartilaginous soft tissue that encapsulates the acetabulum. Acetabular labral tears are reported as the cause of 22–55% of groin or hip pain, which hinders range of motion and negatively impacts patient quality of life.1 –4 Femoroacetabular impingement (FAI) syndrome is 1 of the primary predispositions to labral tear. Other causes include osteoarthritis and traumatic injury.5 –7
Regenerative medicine shows promise in bridging the treatment gap between anti-inflammatory management and surgery. Bone marrow aspirate concentrate (BMAC) therapy holds appeal as a potential adjuvant to surgical repair of the fibrocartilaginous acetabular labral tear due to its success in other areas of healing, such as articular cartilage repairs. 8
The regenerative stem cells found in the bone marrow are theorised to augment the body’s healing response and tissue growth. Enhanced growth factor, cytokine, and chemokine response due to mesenchymal stem cells present in BMAC may catalyse the effects on healing. 9 BMAC has been used in osteoarthritic joints, tendon healing, bone fractures, and cartilage injuries.10 –12 While BMAC has shown positive corollaries in these uses, there is limited literature on its effect as an adjuvant to hip labral repair. The purpose of this systematic review and meta-analysis is to determine the efficacy of BMAC as an adjunct to arthroscopic labral repair in improving patient outcomes.
Methods
A systematic review and meta-analysis of International Hip Outcome Tool-33 (iHOT-33) scores were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines. 13
Search procedure
5 medical databases (PubMed, Embase, Scopus, WebOfScience, and Cochrane Library) were searched using MeSH key terms for articles examining BMAC augmentation for acetabular labrum repair published prior to 20 April 2023. This comprehensive search yielded 455 studies whose titles and abstracts were exported to the Rayyan.ai online software for duplicate removal and screening. 2 reviewers (BJG and SS) manually sorted through the retrieved articles. Following the removal of 234 total duplicates, the titles and abstracts of 221 studies were assessed for inclusion and exclusion criteria (Figure 1).
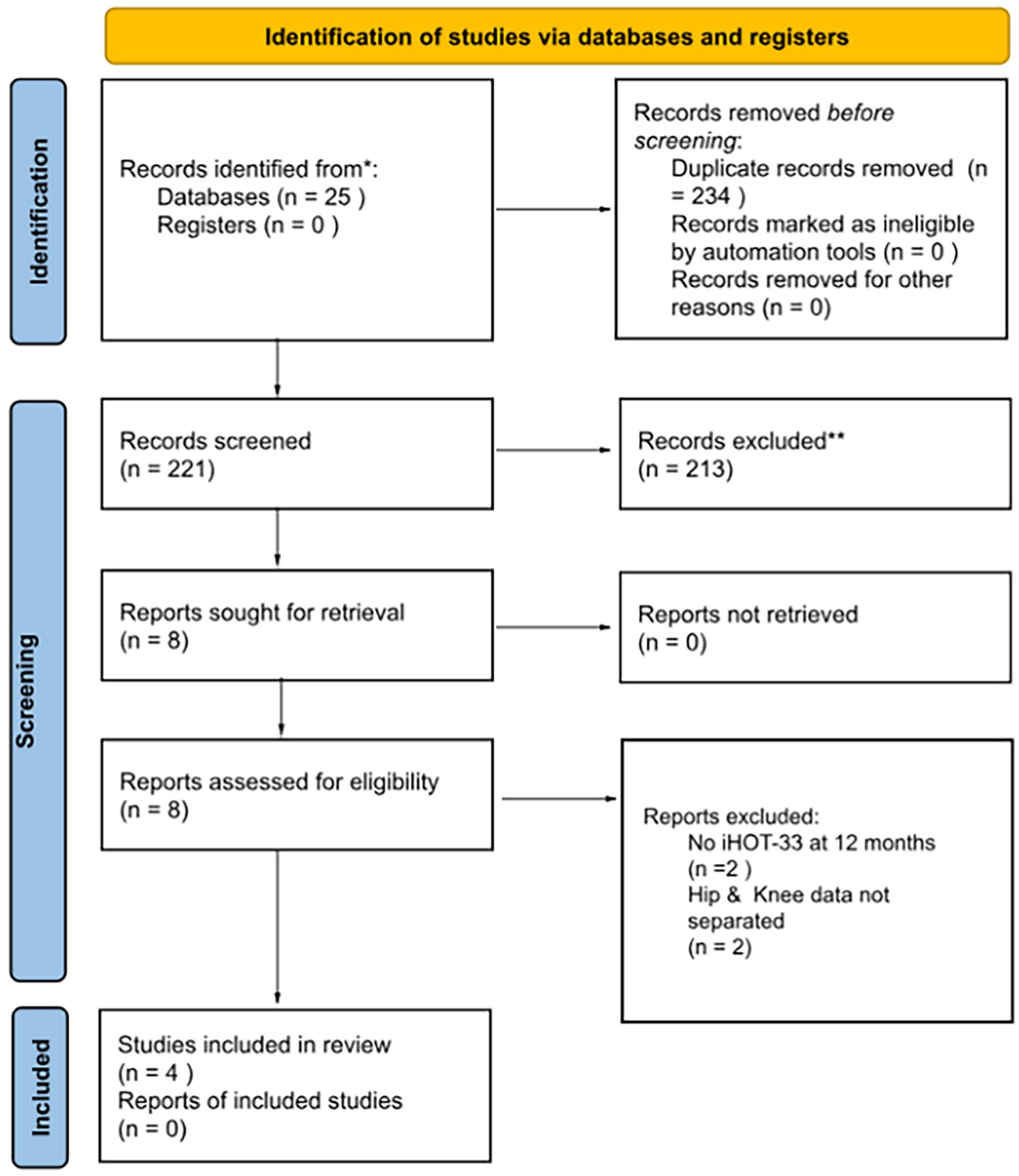
PRISMA flowchart detailing study selection via databases and registers.
Inclusion and exclusion criteria
Titles and abstracts were screened by 2 authors (BJG and SS) and disagreements were resolved by a third author (SBP). The remaining 8 studies underwent full-text appraisal. Included studies assessed iHOT-33 scores before hip arthroscopy with BMAC augmentation and at 12 or 24 months follow-up. 14 Cohort studies, prospective studies, retrospective reviews, and randomised control trials published at any time were eligible for inclusion. Studies were excluded if multiple joints were evaluated but results were not stratified by joint to determine outcomes (n = 2) and if they did not assess functional outcomes via iHOT33 scores at 12 or 24 months (n = 2). Studies which did not reassess scores at 12 or 24 months follow-up were eliminated for the purpose of homogeneity. Studies which reported data only at 12 or 24 months follow-up were included and the data were pooled separately. Articles were not excluded based on language of publication or nation of origin. 4 studies (n = 168 in the control groups and n = 187 patients in the treatment group) were determined to be eligible for data analysis.
Data collection and analysis
Full-text appraisal was completed for four studies, with 315 total participants. Initial critical appraisal was performed, followed by data extraction for the acetabular repair without BMAC group (control) and the acetabular repair with BMAC group (treatment). Treatment efficacy of individual studies was reported using descriptive statistics of pooled mean iHOT-33 scores and standard deviations for baseline and follow-up time points (Table 1).
Descriptive statistics including pooled average, standard deviation, average difference, effect size, and statistical significance of subgroup homogeneity.
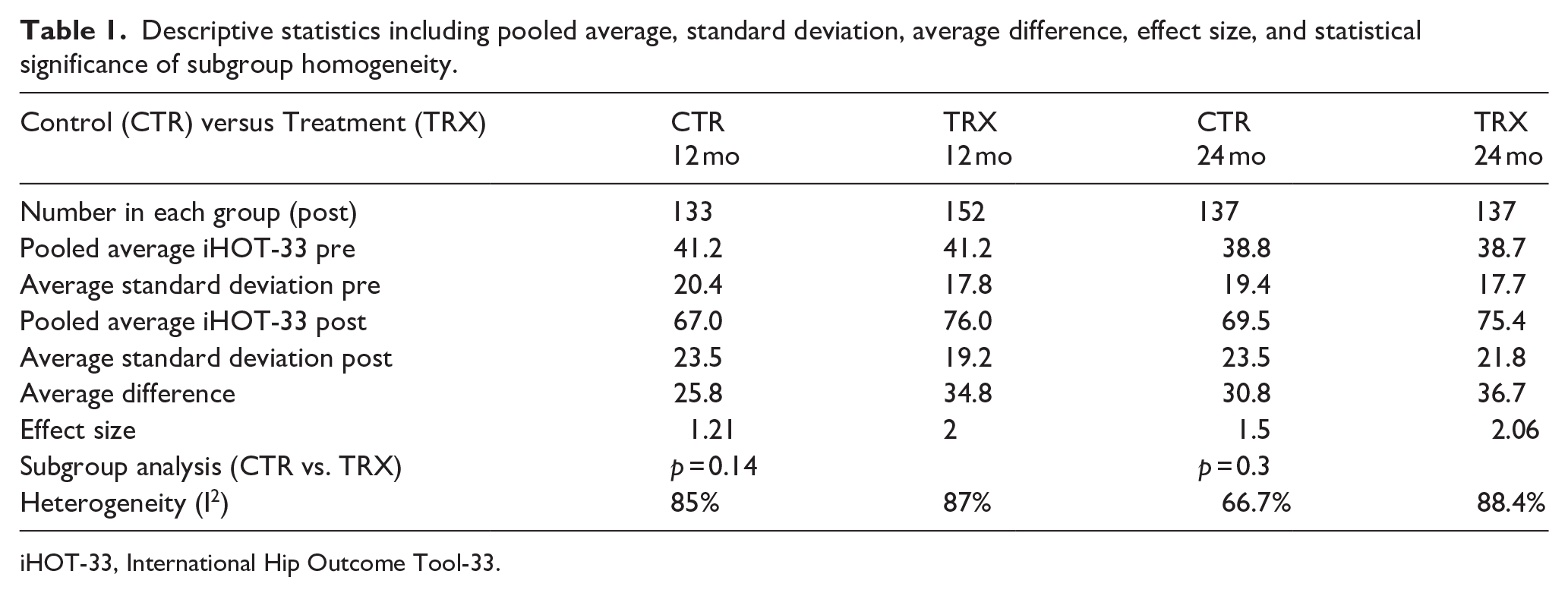
iHOT-33, International Hip Outcome Tool-33.
A random effect meta-analysis was performed to determine differences in iHOT-33 scores within and between groups at follow-up time points. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 29. Results were reported via pooled effect size (Cohen’s d = Mean, 95% CI [LL, UL]) and statistical significance (p < 0.05) for each subgroup for each time point is shown on the forest plot (Figures 2 and 3). The pooled effect size represents the change in iHOT-33 scores between baseline and follow up which represents functional outcomes. The estimation of overall variance between studies was assessed with Tau 2 (τ2). H2 was used to represent the standard deviation of the estimated overall effect size in the random-effects meta-analysis relative to a fixed-effect meta-analysis. I2 represents the total heterogeneity between the studies beyond what would be expected by chance alone, where a lower number represents greater agreement between study results. Measures of subgroup homogeneity are also reported using chi-squared (q), degrees of freedom (df), and statistical significance (p < 0.10). Significance in this test represents a meaningful difference between subgroups. Following analysis, studies were then subjected to critique of design.
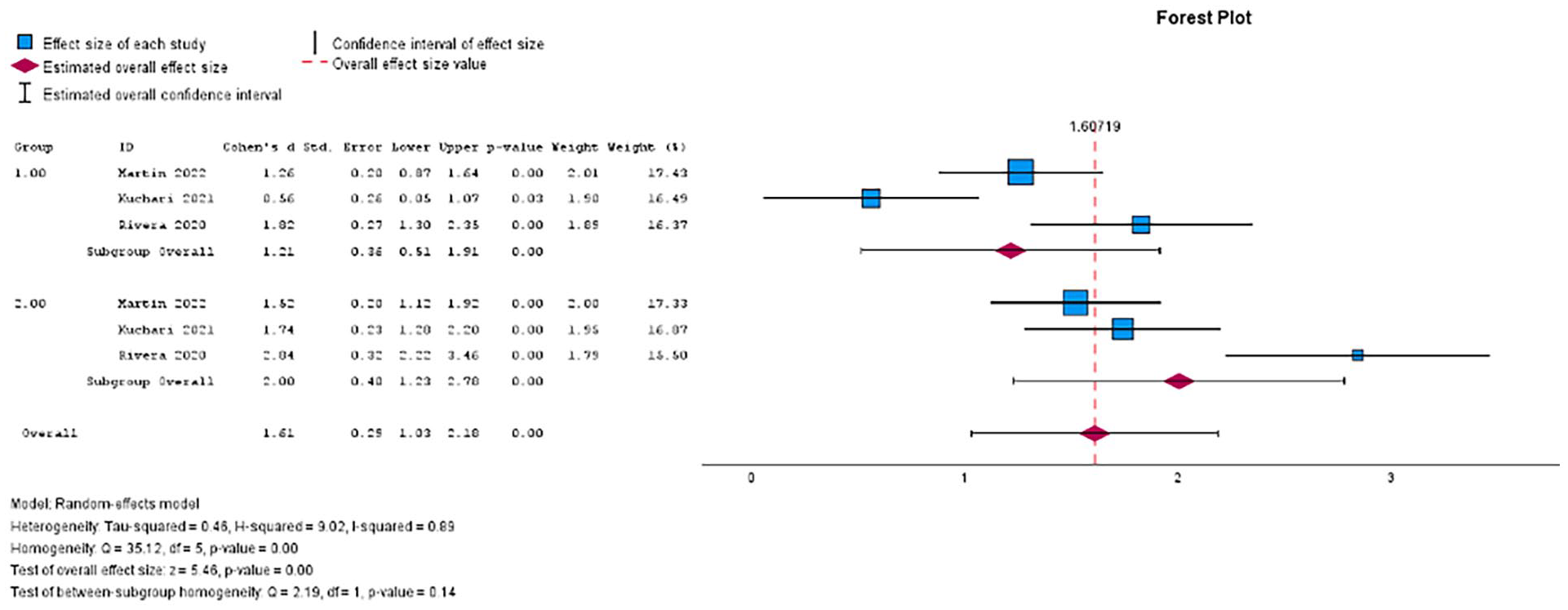
A forest plot of the meta-analysis showing the individual pooled effect size for the control (1) and treatment (2) groups at 12 months.
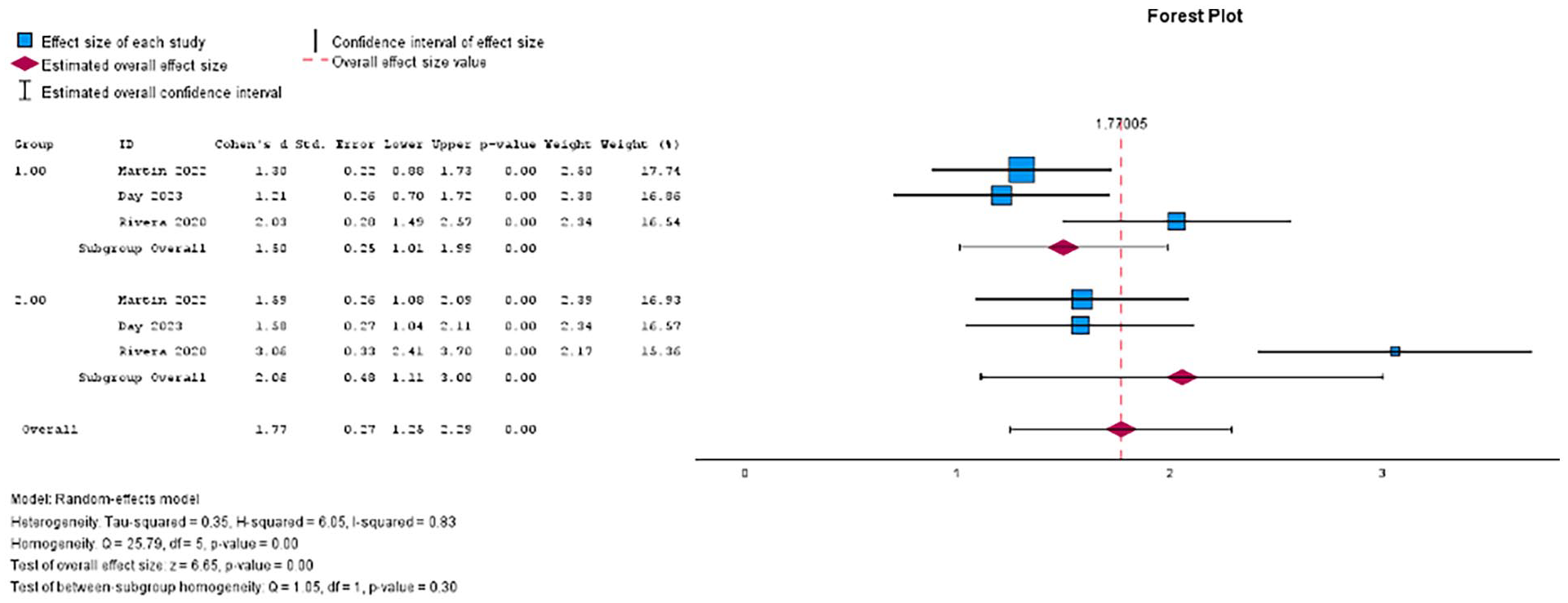
A forest plot of the meta-analysis showing the individual pooled effect size for the control (1) and treatment (2) groups at 24 months.
Certainty of evidence and risk of bias assessment
Included articles were subjected to scoring for certainty of evidence using Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria independently by 2 authors (NA and AG) (Table 3). 15 Bias in each article was also assessed based on their respective study design independently by 2 authors (NA and AG). Single-arm observational studies were subjected to evaluation with ROBINS-I. 16 Risk of bias and data was reported by stoplight plot and summary plot created using the robvis tool (Figures 4 and 5). 17
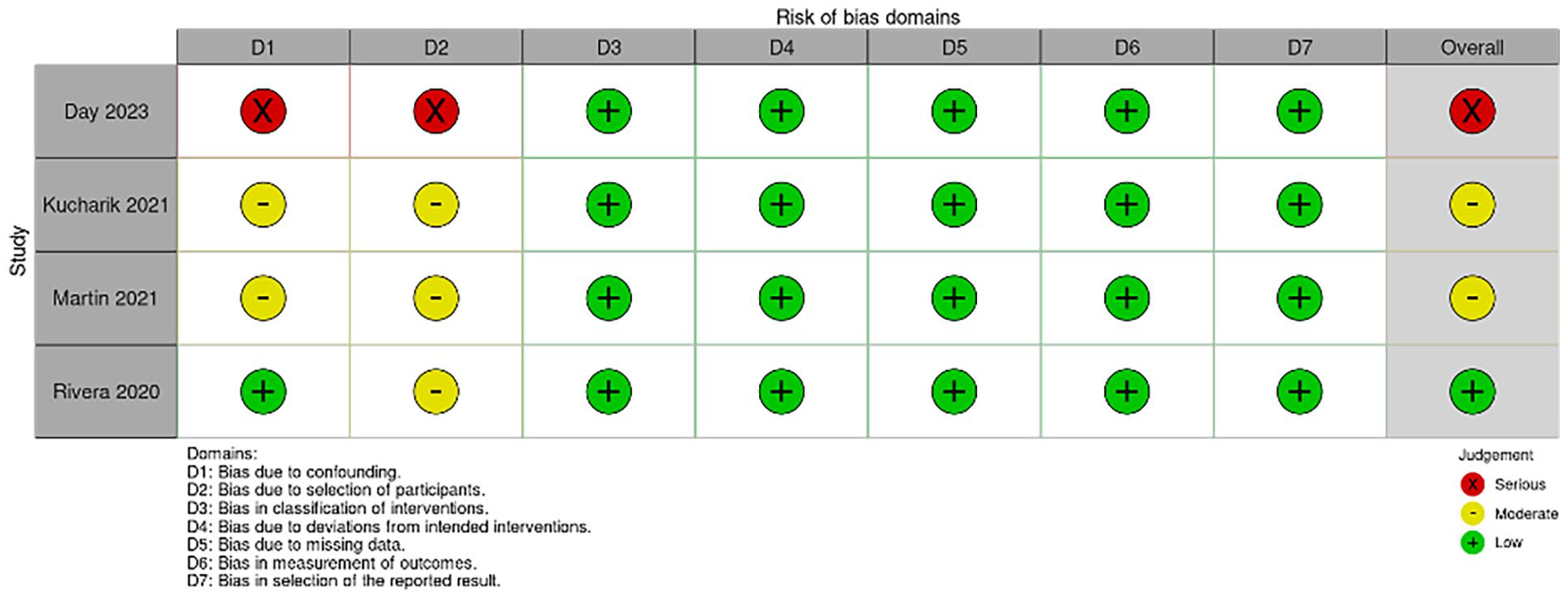
ROBINS-1 Risk of Bias traffic light plot.
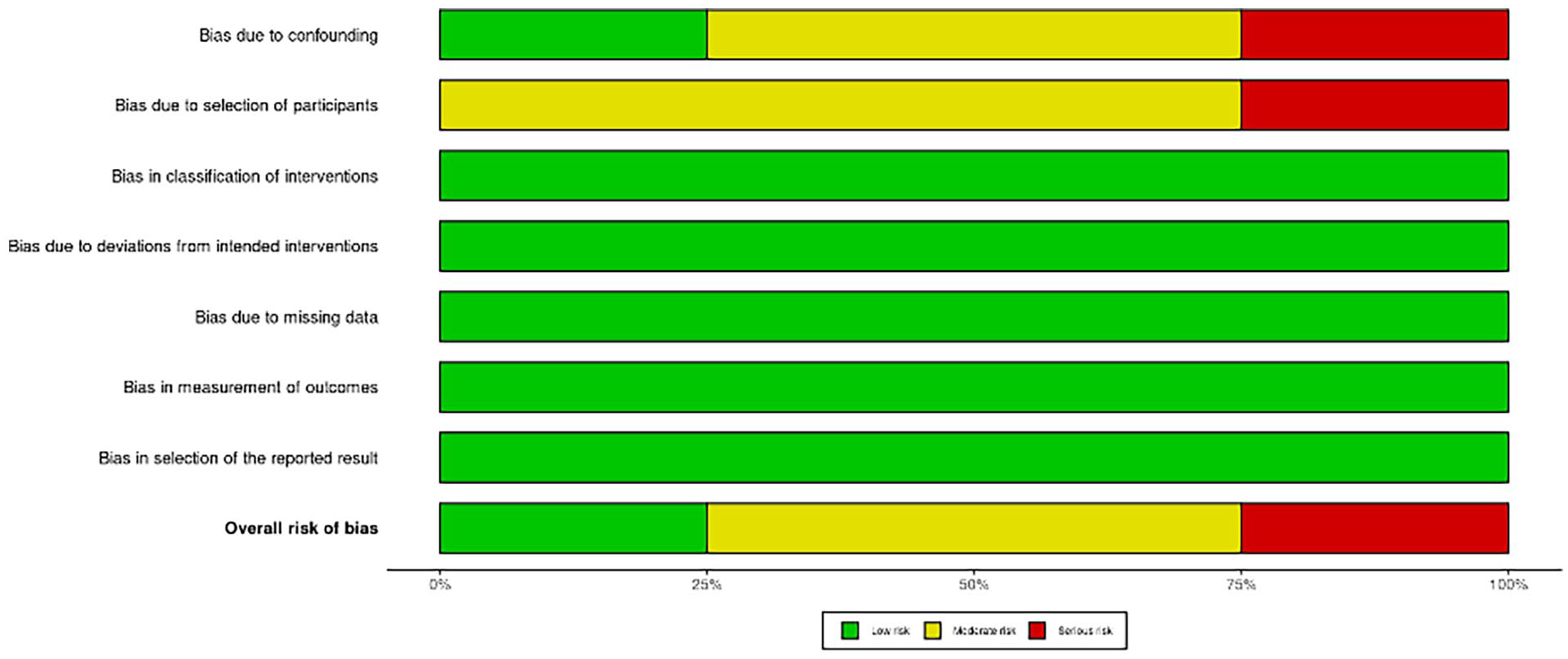
ROBINS-1 Risk of Bias summary plot.
Results
Effect of intervention
In each of the included studies, the control and treatment groups saw significant improvement in iHOT-33 scores between baseline and both follow-up time points (p < 0.001) (Figures 2 and 3). In the control group, the pooled mean iHOT-33 scores were 41.2 ± 20.4 at baseline, 67.0 ± 23.5 at 12 months, and 69.5 ± 23.5 at 24 months (Table 1). The arthroscopic labral repair with the adjunctive BMAC group had pooled mean iHOT-33 scores of 41.2 ± 17.8 at baseline, 76.0 ± 19.2 at 12 months, and 75.4 ± 21.8 at 24 months (Table 1). The average improvement in iHOT-33 scores at 12 months was 25.8 in the control group and 30.8 in the BMAC group. At 24 months, the average difference from baseline was 34.8 for the control and 36.7 for the BMAC groups (Table 1).
The pooled effect size of the control group indicates statistically significant differences between baseline and 12 months follow-up (p < 0.01, Cohen’s D = 1.21, 95% CI [0.51, 1.91]), as did the treatment group (p < 0.01, Cohen’s D = 2.00, 95% CI [1.23, 2.78]) (Figure 2).
At 24 months follow-up, the control group maintained a significant difference from baseline (p < 0.01, Cohen’s D = 1.50, 95% CI [1.01,1.99]) as did the treatment group (p < 0.01, Cohen’s D = 2.06, 95% CI [1.11, 3.00]) (Figure 3).
Analysis of subgroup differences revealed no difference at 12 months (Q = 2.19, df = 1, p = 0.14) or 24 months (Q = 1.05, df,1, p = 0.30) (Figures 2 and 3). Interventions, populations, and qualitative data can be found in Table 2.
Summary of included studies.
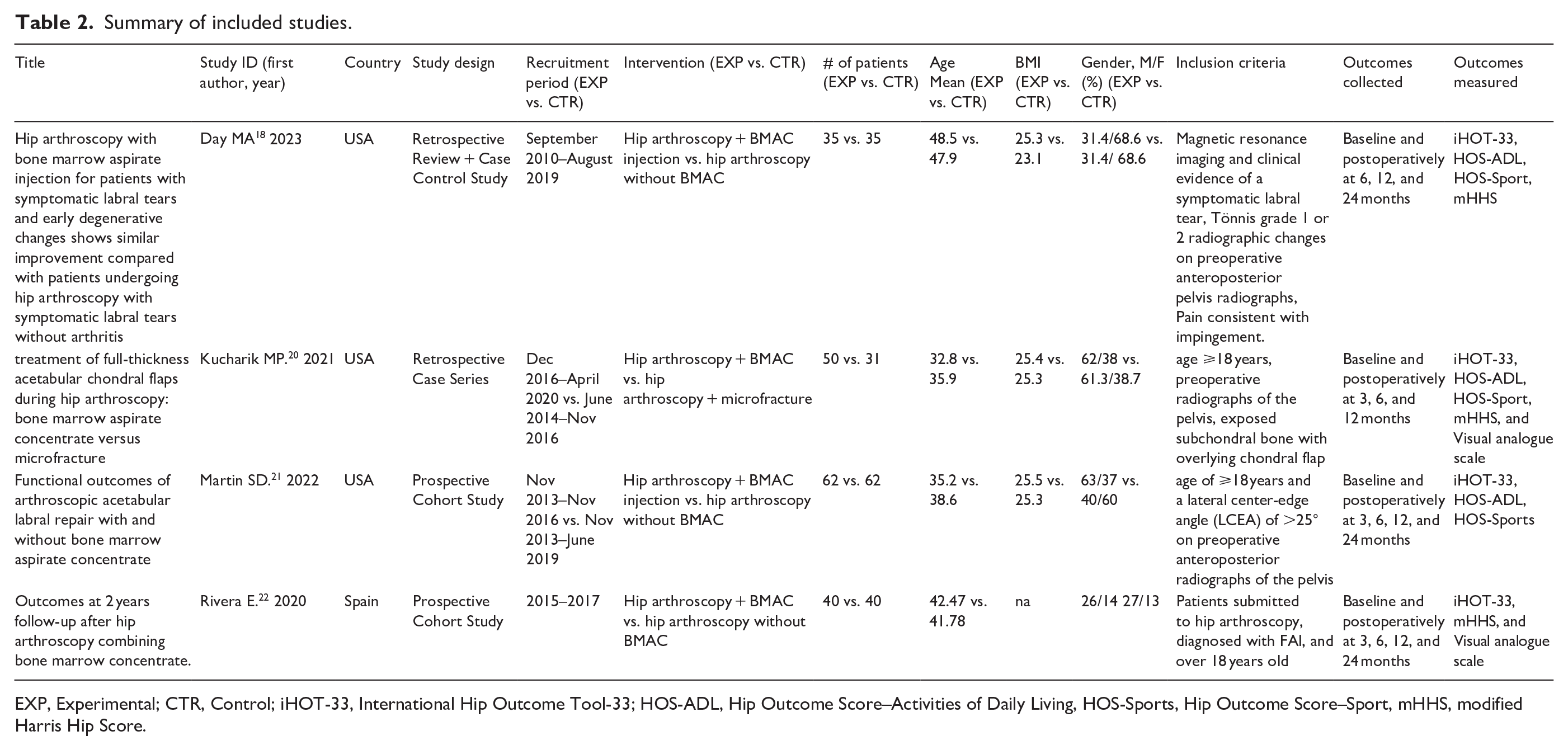
EXP, Experimental; CTR, Control; iHOT-33, International Hip Outcome Tool-33; HOS-ADL, Hip Outcome Score–Activities of Daily Living, HOS-Sports, Hip Outcome Score–Sport, mHHS, modified Harris Hip Score.
Heterogeneity
Heterogeneity of the 12-month analysis for the control group was found to be τ2 = 0.32, H2 = 6.66, and I2 = 85.0%. The treatment group showed τ2 = 0.41, H2 = 7.67, and I2 = 87.0%. Within the 24-month analysis, the control group heterogeneity measures were τ2 = 0.125, H2 = 3.01, and I2 = 66.7%, while the treatment group heterogeneity measures were τ2 = 0.62, H2 = 8.63, and I2 = 88.4%.
Certainty of evidence and risk of bias assessment
The studies included were determined to be of moderate quality (Table 3). Risk of bias analysis revealed one study with low risk, 2 with moderate risk, and 1 with severe risk of bias (Figures 4 and 5). Overall GRADE analysis revealed a low certainty of evidence, which was determined using the lowest evidence included (Table 3).
GRADE analysis of the included studies.
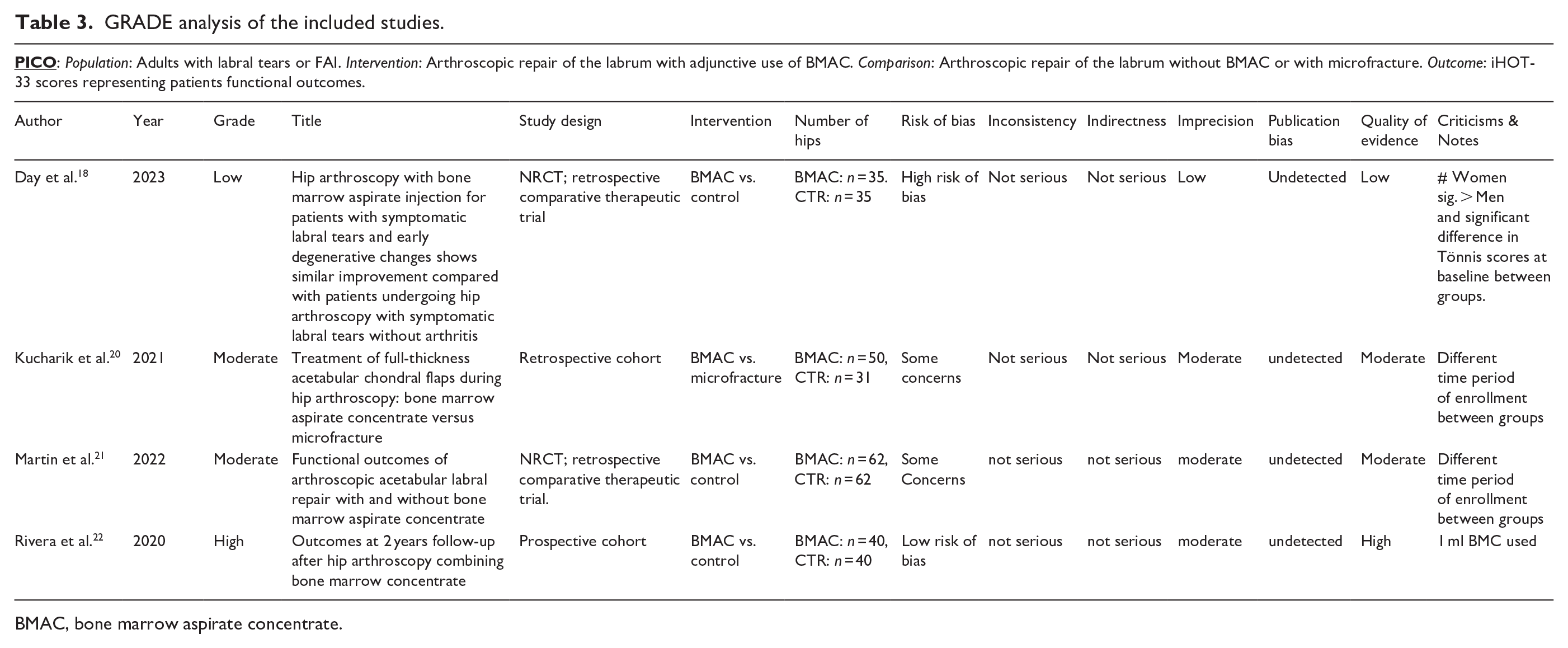
BMAC, bone marrow aspirate concentrate.
Discussion
This systematic review and meta-analysis sought to determine the efficacy of BMAC as an adjunct to acetabular repair of the labrum. Despite the trends favouring BMAC augmentation, the 4 studies included in the analysis of iHOT-33 scores revealed no statistically significant differences between the control and treatment groups at 12 or 24 months follow-up. Moderate differences in effect size with p-values nearing significance were found concomitantly with high levels of heterogeneity in both groups at both time points. This suggests that the trends favouring the use of BMAC may become statistically significant if there was less variance between study results. The varying quality and risk of bias determined using the GRADE and ROBINS-I assessments further highlight the need for careful interpretation of the findings. This nuanced understanding is critical in interpreting the results of this study. More high-quality research is needed before clinical recommendations may be made.
Further examination of the presented studies is also warranted. Day et al. 18 compared a group with hip OA, Tönnis scale grade 1 and grade 2 hips, to a control group without osteoarthritis. While both groups had labral injury and received labrum-preserving arthroscopic surgery of the hip, only the OA group received adjunctive BMAC. The improvements in iHOT-33 scores were comparable, but the presence of OA in the BMAC group is a confounding variable, which is detailed in the GRADE analysis (Table 3). When OA presents concomitantly with labral injury, it is unknown how much each pathology contributes to the baseline symptomatology. Therefore, when iHOT-33 scores improve in the comorbid group, it cannot be determined if this is from adjunctive BMAC enhancing labral tear recovery or from relief of pain and improving function secondary to cartilage degeneration. Additionally, the groups experienced different rates of intraoperative labral debridement compared to labral repair. Labral debridement was chosen over labral repair 54.3% of the time by the surgeon in the BMAC group but only 14.3% of the time in the control group. This may also affect the rate of improvement within the study and should be standardised or controlled in future research. Due to the differences in OA, the rate of progression to hip revision arthroscopy or total hip arthroplasty is not comparable. 19 It is noteworthy that BMAC harvesting did not result in any complications. Although several confounding variables were present in this study, the results are not outliers and likely do not substantially affect the overall results.
In a paper by Kucharik et al., 20 both groups had full-thickness chondral flaps, underwent arthroscopic acetabular labral repair, and were reassessed at 12 months. The 2 groups were homogenous at baseline and underwent the same procedures. Over 50% of each group had Tönnis grade 1 hip. For either treatment case, it cannot be determined how much labrum or cartilaginous healing contributed to overall improvements in iHOT-33 scores. Importantly, the treatment group received adjunctive BMAC while the control group underwent microfracture, which is theorised to also introduce stem cells into the joint space. The BMAC group reported significantly better outcomes at 12 months compared to the control group. This adds a confounding factor to the pooled analysis of the control group in the current study. Since it was the study with the least amount of improvement at follow-up, the use of microfracture as a control may have diminished the mean efficacy of the control group. This study also displays the importance of another potential confounding factor in the assessment of the efficacy of BMAC: the type of femoral acetabular impingement (FAI) present. There was no statistically significant difference (p = 0.173). However, future studies should consider potential differences in outcomes reported between cam, pincer, and combined type lesions.
Martin et al. 21 also presented data on procedure type, lesion type, and presence of degenerative joint changes. In this study, all patients received labral repair, but both control and treatment groups experienced equivalent confounding levels of mild to severe OA. An equal majority of each group received acetabuloplasty and about half of each group also underwent femoroplasty. Between the 2 groups, the BMAC group showed no statistical difference at any time point, except for when 75% of the sample with moderate arthritis was selectively assessed. In this case, superior outcomes at both time points were seen in the BMAC group. This suggests that BMAC may selectively improve iHOT-33 scores specifically in the presence of moderate joint degeneration, thus providing context to the previously mentioned issues regarding comorbidity and symptom improvement. No details on the BMAC concentrations used were provided, but it was reported that no adverse events were noted in the collection of BMAC.
Lastly, Rivera et al. 22 compared a BMAC adjunct group to a labral repair control group with no significant procedural or baseline data. This paper reported cell doses used in bone marrow concentrate and enrolled a large majority of hips with cam-type FAI, but did not report if any adverse events occurred because of the procedure. The participants in this paper also had OA. Thus, the current systematic review specifically represents the efficacy of BMAC in treating labral tears in the context of osteoarthritis. The data from the groups in this retrospective study were collected during different time periods but are overall a quality representation of the research question posited. Of note, the results presented in this paper at both time points were superior to the others and likely increased the pooled average.
The pooled mean iHOT-33 scores indicate a large improvement among control and treatment groups at both follow-up time points. This improvement reflects the overall efficacy of the surgical repair of the labrum. While the trends observed in the improvement of iHOT-33 scores with BMAC adjunct were not statistically significant, they suggest a potential clinical relevance that merits further investigation. Specifically, in our study, the pooled mean iHOT-33 scores of the treatment group improved by 9 points more than the control at 12 months and 4.9 points at 24 months follow-up (Table 1). This exceeds, or is very close to, the minimum clinically important difference (MCID) for iHOT-33 scores reported in the literature. The point improvements required for MCID range from 6.1 points in the original iHOT-33 design and validation study by Mohtadi et al., 14 to 10 points used conservatively for systematic review by Casartelli et al., 23 to 12.8 points in a paper by Nwachukwu et al. following hip revision arthroscopy. 24 This is presented to add clinical context to the differences seen between each group. Clinicians should weigh the cost and benefit of BMAC for patients who may not respond to conventional treatments or who have specific conditions that might benefit from regenerative therapies.
Limitations
This study is not without limitations. The sample size of the included papers was somewhat small, consisting of only 4 studies with a total of 315 individuals between both groups with 3 papers being pooled at each time point. Furthermore, this study exclusively examined functional outcomes and did not assess radiographic findings, safety outcomes, revision rates, or cost analysis, all of which play a role in clinical implementation. Of the included studies, only one was truly measuring if BMAC improves labral tear repair without a significant confounding variable. This prompts the substantial need for future prospective research where FAI type is case-controlled, osteoarthritis is not present, and BMAC injection values are quantified before clinical recommendations can be made on the topic. Lastly, the follow-up timeframe available for analysis was limited to 12 months and 24 months, which cannot be extrapolated to shorter or longer outcome periods.
Future directions
Future research in this field should include larger high-quality studies to directly assess the efficacy of BMAC as an adjunct to arthroscopic repair for hip labral tears, especially in the context of long-term outcomes with patient stratification based on individual characteristics. Specifically, these future studies should report detailed information on mesenchymal stem cells, other cell quantity, other substrates present in the BMAC, dosage, and clinically relevant confounding variables such the type of femoroacetabular impingement or severity grade of the lesion. Cost-effectiveness analyses, standardisation of BMAC processing, and pure patient-reported outcomes should also be explored.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.