
Abstract
Objectives:
Total hip arthroplasty (THA) and resurfacing hip arthroplasty (RHA) offer promising therapeutic solutions to physically active patients with hip osteoarthritis (OA). The impact of physical activity on long-term implant integrity in this population remains unknown. This systematic review compares the impact of physical activity and sports participation on implant integrity in THA versus RHA.
Methods:
A comprehensive search of Medline, Embase (both via Ovid), Scopus, and CINAHL was conducted from inception to May 2023 following the Cochrane Handbook for Systematic Reviews of Interventions. Data were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The quality of included studies was assessed using the Newcastle-Ottawa Scale. Implant integrity was measured either radiographically, via serum metal ion levels or revision rates.
Results:
A total of 16 studies with 4676 patients (THA: 3146; RHA: 1530) met the inclusion criteria. The median age at surgery was 60 years (range 49 to 86) in THA and 54 (range 49–61) years in RHA. At a median follow-up of 7.1 (range 4.8–13.1) years in THA and 10 (range 2.8–11.7) years in RHA, 3 studies out of 12, including 65.7% of the patients who underwent THA, and 2 studies out of 5, including 30.1% of the patients who underwent RHA, demonstrated that increased physical activity was associated with poor implant survivorship.
Conclusions:
Patients undergoing THA or RHA should be counselled to participate in moderate physical activity and may benefit from avoiding sports that exert an excessive load on their implants. On average, the quality of the studies was moderate. The outcome measures used to quantify physical activity and implant integrity are heterogenous.
Introduction
Returning to sports and recreational activities are among the priorities for patients undergoing hip arthroplasty, especially in young and active patients. Both total hip arthroplasty (THA) and resurfacing hip arthroplasty (RHA) are viable surgical options for active individuals with hip osteoarthritis (OA). 1 Patient expectations after hip arthroplasty, including symptom relief and restoration of physical function, have increased over the last few decades. 2 Hip arthroplasty has become a surgical solution for a broader demographic, including younger and more active patients with longer life expectancy. 3
The revision rate in THA and RHA varies according to follow-up period. At 8 years, the overall revision rate in THA was reported to be 4.0% compared to 5.3% for RHA. 4 Prosthetic wear, aseptic loosening, and revision rate are viable parameters that have been studied to determine the longevity of hip arthroplasty bearings. 5 Radiographically, periprosthetic osteolysis and linear wear rate are valuable indicators of implant integrity because they are presymptomatic markers of aseptic loosening. Serum metal ion levels are also important to consider in the context of long-term prosthetic wear because of the adverse local tissue reactions that may ensue. Nonetheless, the use of metal-on-metal bearings has declined over the years because of concerns regarding the potential toxicity of cobalt chromium ions. 6 In athletes and physically active individuals, metal ion debris complications may be of greater concern due to the increased friction between bearings in this population. 7 .
According to the current guidelines, patients can return to preoperative levels of low- to moderate-level impact sports between seven to twelve months following THA, 8 whereas patients who undergo RHA are permitted to return to low-intensity sporting activities 3 months after the procedure and high-impact sports at 6 months postoperatively. 9 Banerjee et al. 10 found that while physical activity is possible after RHA, there is a shift towards low-impact sports. Although moderate sporting activity seems to be acceptable in RHA, only a few studies with small sample sizes have evaluated its consequences on wear and aseptic loosening. Additionally, most studies have only evaluated the short-term impact of physical activity and sports participation on implant integrity.11,12 There remains controversy surrounding the long-term consequences and nature of sports (i.e., low versus high impact) on the survivorship of RHA and THA implants. Many patients are determined to remain physically active following RHA or THA, thus necessitating a clear understanding of the impact of physical activity on implant integrity. To address this question, we performed a systematic review of the literature to evaluate the long-term impact of physical activity and sports participation on implant integrity in THA and RHA.
Methods
This systematic review was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).13,14
The search strategy was registered in PROSPERO a priori 2022 (CRD42022380226).
Search strategy
We performed a queried search of Medline, Embase (both via Ovid), Scopus, and CINAHL from inception to May 2023. The search was piloted in Medline using Medical Subject Headings (MeSH) and free-text (title, abstract, or keyword) searching to retrieve articles related to THA, RHA, physical activity, and implant integrity. We adapted the search to use subject headings (when applicable) and syntax specific to the other databases. The search was conducted by a health sciences librarian. The search strategy can be found in Supplemental material Table S1.
Screening
Screening of studies was conducted using Covidence version 2 (Veritas Health Innovation, Melbourne, Australia). After duplicate articles were removed, 2 authors (JJL and AA) screened the articles by title and abstract independently and in duplicate (i.e., primary screening). Following primary screening, the same 2 authors screened articles by full-text independently and in duplicate to determine the final inclusion (i.e., secondary screening). Conflicts were resolved through discussion or were arbitrated with additional reviewers (AT and SR). A Cohen kappa coefficient was computed to determine inter-rater reliability at primary screening.
Eligibility criteria
The population of included studies consisted of adult patients aged 18 years or older who underwent THA or RHA for hip OA (>50% of study population). Studies were included if they had a physical activity or sports participation component. We included studies with a minimum follow-up of 5 years with primary outcomes including a measure of physical activity and sports participation (e.g., self-reported questionnaires, accelerometer, pedometer) and implant-related outcomes (e.g., revision rate, implant survivorship, radiological outcomes).
The study designs consisted of prospective or retrospective cohort, case-control, cross-sectional, or randomised controlled trials. The following studies were excluded: (1) postoperative exercise programs that did not measure physical activity; (2) phantom, simulation, cadaveric or non-human studies; (3) studies that analysed only muscle morphology or architecture as outcomes; (4) non-exercise modalities (e.g., manual therapy, osteopathy, electrical stimulation, water-based therapy); (5) studies not evaluating functional outcomes; (6) systematic reviews, literature reviews and meta-analyses; (7) published in a language other than French or English; (8) abstracts, editorials, conference proceedings, and clinical trial registrations without results.
Quality assessment
2 authors (JJL and AT) independently assessed the quality of the included studies using the Newcastle-Ottawa Scale. 15 This scale consists of eight items within three domains for a maximum of 9 points. The cohort studies were rated based on selection (max 4 points), comparability (max 2 points), and outcome (max 3 points); whereas the case-control studies were rated based on selection (max 4 points), comparability (max 2 points), and exposure (max 3 points). Studies were rated as low (1–3 points total), moderate (4–6 points total), or high quality (7–9 points total).
Data extraction
Baseline data for each study was extracted, including the title, lead author, year of publication, country, study design, and statistical analysis. Data extraction was performed by a single author (JJL). Corresponding authors were contacted if insufficient information was presented to determine inclusion eligibility and were excluded if no response was received (n = 6). We extracted data pertaining to the study population such as number of patients, number of hips operated, age at surgery, sex, follow-up duration, and the percentage of patients with a diagnosis of OA. Implant details, including the manufacturer and composition, were extracted along with the exercise prescription details (i.e., volume, duration, effort or exertion, load, progression), physical activity/sports participation outcomes measures, implant integrity and failure outcome measures, and main study findings.
Results
Our initial search yielded a total of 4037 studies. After duplicates were removed, 2496 articles underwent primary screening, of which 89 were evaluated by full text. A total of 16 studies with 4676 patients (THA: 3146; RHA: 1530) met all the inclusion criteria.5,16 –30 A Cohen kappa of 0.82 was obtained, demonstrating excellent agreement between both reviewers. A detailed flowchart of the screening process is illustrated in Figure 1. After appraising the included articles using the Newcastle-Ottawa Scale, 6 studies were deemed of high quality,19,22,23,25,28,30 9 studies were of moderate quality,5,16 –18,21,24,26,27,29 and 1 study was of poor quality. 20 The Newcastle-Ottawa Scale study quality assessment can be found in Supplemental material Table S2.
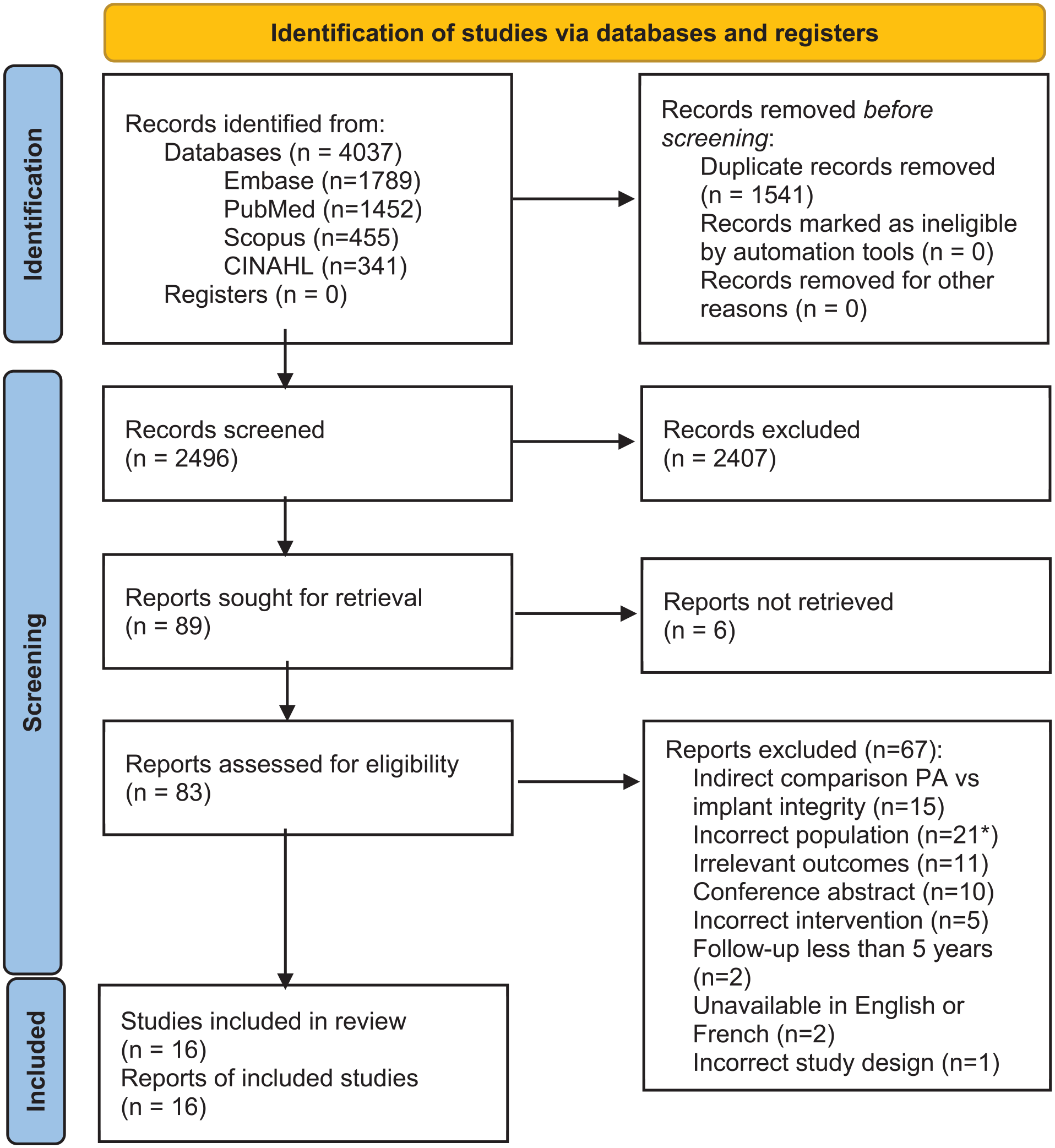
PRISMA preferred reporting flow diagram for conducting systematic reviews and meta-analyses. *For studies that did not specify the primary diagnosis requiring THA/RHA, the corresponding author was contacted. After no response, the article was excluded (n = 6).
Demographic features
The included studies comprised 3146 patients who underwent THA and 1530 patients who underwent RHA for a total of 3524 and 1851 operated hips, respectively. The median age at time of surgery was 60 years (range 49–86 years) for patients undergoing THA and 54 years (range 49–61 years) for patients undergoing RHA. The patient population was 47.1% female. The median follow-up was 7.1 years (range 4.8–13.1 years) in THA and 10 years (range 2.8–11.7 years) in RHA. The primary diagnosis was OA for 85.1% of patients. Baseline patient characteristics are outlined in Table 1.
Baseline patient characteristics of the included studies.

THA, total hip arthroplasty; RHA, resurfacing hip arthroplasty; OA, osteoarthritis.
Physical activity measurement
Some studies specified the exercise prescription details, while others simply reported measurements of physical activity. The University of California at Los Angeles (UCLA) Activity Scale was used in 9 (56.3%) studies.16,17,19 –21,25,28 –30 3 (18.8%) studies used an accelerometer to measure physical activity.18,26,27 3 (18.8%) studies used a subjective patient questionnaire to report the exercise prescription details.5,19,22 An Impact Score (IS) and Hip Cycle Score (HCS) were used in 2 (12.5%) studies.17,24
Wear and failure metrics in THA
Of the 3524 included THA, 2223 (63.1%) femoral stems were cemented and 1301 (36.9%) were cementless. Among the 12 studies reporting on the outcomes of THA, 8 measured implant integrity via radiographic assessment. 3 studies measured serum metal ions (cobalt and/or chromium) in patients postoperatively. Revision rates were presented in 6 studies.
In 9 studies,5,16,19,20,26 –30 including 1078 (34.3%) participants who underwent THA, physical activity was not associated with poor implant outcomes, as measured either radiographically, using serum metal ions levels, or via revision rates. 1 study found that linear polyethylene wear was highest within the non-active group (19 out of 60 total participants). 5
However, in 3 studies including 2068 (65.7%) participants, 22,23,25 increased physical activity was associated with lower rates of implant integrity at an average follow-up of 6.3 years. The first study by Flugsrud et al. 22 found that men with a high level of physical activity, measured via a self-reported questionnaire, were at increased risk of revision (relative risk [RR] 4.8; 95% CI, 1.3–18). Gschwend et al. 23 identified an increased average linear wear rate in the physically active group compared to the minimally active group (2.1 versus 1.5 mm, respectively, p < 0.05). Lübekke et al. 25 found that the adjusted odds ratio for femoral osteolysis comparing high (UCLA 8–10) versus moderate (UCLA 5–7) activity was 3.6 (95% CI, 1.6–8.3) and revision for aseptic loosening was greatest in the high activity group (p = 0.023).
Wear and failure metrics in RHA
Of the 1851 included RHA, 1326 (71.6%) had cemented femoral components and 525 (28.4%) were cementless. Among the 5 studies reporting on the outcomes of RHA, postoperative radiographic assessment of the hip implant was performed in 3 studies. Serum metal ion levels (cobalt and/or chromium) were measured in 2 studies and revision rates were computed in 2 of the RHA studies.
2 studies,17,18 including 461 (30.1%) patients who underwent RHA, reported an association between increased physical activity and poor implant integrity, which was measured via serum metal ion levels (p < 0.001) and revision rate. In a study by Le Duff et al. 17 , a 10-point increase in IS corresponded to a 37% increase in risk of revision (hazard ratio [HR], 1.37; 95% CI, 1.18–1.59), while a 10-point increase in the HCS increased the risk of revision by 22% (HR, 1.22; 95% CI, 1.06–1.41). Furthermore, a smaller study by Jelsma et al. 18 reported that patients performing higher intensity physical activity were found to have higher cobalt ion concentrations.17,18 The other RHA studies (n = 4, 1069 participants) did not demonstrate a significant association between increased physical activity and implant failure.21,24,27,28 A summary of the included studies can be found in Table 2.
Characteristics of the included studies in the systematic review.
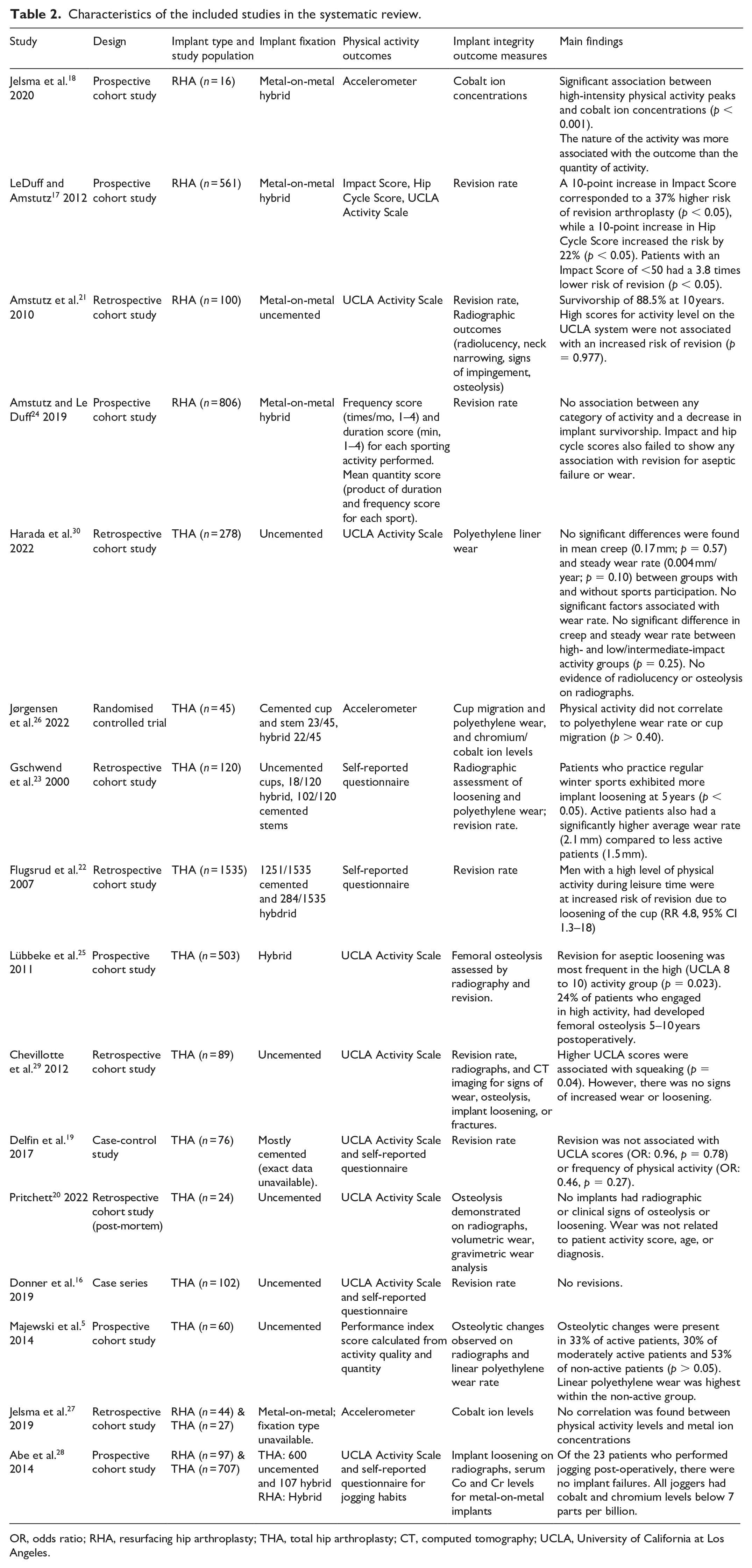
OR, odds ratio; RHA, resurfacing hip arthroplasty; THA, total hip arthroplasty; CT, computed tomography; UCLA, University of California at Los Angeles.
Studies directly comparing THA to RHA
2 studies directly compared THA to RHA. Both studies did not suggest that increased physical activity was associated with decreased implant survivorship. The first study compared joggers to non-joggers (total of 97 RHA hips and 707 THA hips) and found no significant difference in radiographic signs of implant migration or wear at a mean follow-up of 5 years. 28 The second study was a retrospective cohort study of patients with metal-on-metal hip arthroplasty; 27 there was no correlation between physical activity levels and metal ion concentrations in both THA (27 hips) and RHA (44 hips) patients.
Discussion
Herein, we present the first systematic review exploring the long-term impact of physical activity and sports participation on implant integrity in THA versus RHA. Overall, 16 studies met all the inclusion criteria, resulting in 3146 patients who underwent THA and 1530 patients who underwent RHA. Several notable findings have been reported, including the following: (1) 3 studies out of 12, including 65.7% of the patients who underwent THA, and 2 studies out of 5, including 30.1% of the patients who underwent RHA, demonstrated that increased physical activity was associated with decreased implant survivorship; (2) the most common method to assess implant integrity was radiographic analysis (11 studies), followed by revision rate (8 studies) and serum metal ion levels (5 studies); (3) methods used to measure physical activity participation and implant integrity are heterogeneous across studies.
THA versus RHA
Although studies have shown comparable results regarding revision rates and metal ion counts between both interventions,31,32 patient characteristics are an important consideration when identifying surgical candidates for RHA. In a prospective, multicentre study with a 10-year follow-up, the authors found that the 10-year survival from all-cause revision was 92.9% in males aged less than 65 years at the time of implantation of a Birmingham metal-on-metal RHA. 33 As RHA preserves more bone than THA, it seems to be a viable alternative for young and active individuals. Considering that no femoral stem is inserted into the femur in RHA, high-impact sports such as competitive running, should be well tolerated because the load is evenly distributed throughout the femur. 34 In addition, patients undergoing RHA are typically younger and in better physical condition than those undergoing THA, which could contribute to the long-term survival of RHA.
Bearing materials
Although ceramic-on-ceramic hip bearings appear more promising in the younger population undergoing hip arthroplasty, the intrinsic properties of ceramic are more brittle and thus more likely to fracture. 35 Majewski et al. 5 used a polyethylene bearing with a ceramic femoral head and found that osteolytic changes were present in 33% of active patients, 30% of moderately active patients, and 53% of non-active patients (p > 0.05). Nonetheless, linear polyethylene wear was highest in the non-active group. Pritchett et al. 20 also demonstrated that polyethylene wear was not related to patient activity scores, age or preoperative diagnosis when using polyethylene bearing and ceramic-coated metal heads.
Types of physical activity associated with decreased implant survivorship
It has been documented that low- to moderate-level impact sports are well tolerated after THA. 8 However, participation in high-impact sports, such as singles tennis and competitive running should be counselled to decrease potential postoperative complications such as aseptic loosening and periprosthetic fractures due to excess load exerted on the joint. 8 Nonetheless, Majewski et al. 5 found that the linear polyethylene wear rate was the highest in the non-active group. Therefore, patients should aim for a middle ground by engaging in low to moderate physical activity levels.
The studies included in this review measured physical activity using either the UCLA activity-level scale, an accelerometer, a subjective patient questionnaire or an IS/HCS. The UCLA activity-level scale is commonly used in patients with osteoarthritis to evaluate their physical function and exhibits a strong relationship with the Harris Hip Score and the Short Form-12, 2 other frequently used metrics in this population. 36 However, the subjective nature of the questionnaire may affect its validity. 37 Accelerometers entail a certain degree of uncertainty depending on patient compliance with the device. Nonetheless, utilising objective measures of physical activity prevents observation biases and enhances the internal validity of studies that consider the impact of physical activity on implant survivorship.
Clinical recommendations
Our review outlines that strenuous physical activity may reduce implant longevity in both THA and RHA patients. The moderate- to high-quality findings support encouraging patients to participate in physical activity following hip arthroplasty. However, contact sports or physical activity that exerts excess load on the joint should be avoided. Discussing the risks of participating in these activities is essential as low to moderate physical activity could potentially promote long-term joint health. Moreover, monitoring implant longevity using serial radiographic or clinical parameters, particularly in active individuals, is important to assess long-term outcomes. It is also crucial to tailor physical activity recommendations to individual factors such age, baseline fitness, habitus, and surgical approach used.
Limitations
This review presents several limitations. First, there was significant heterogeneity in the physical activity measures and implant integrity outcomes. Therefore, a meta-analysis was not deemed suitable. A significant number of included studies were retrospective cohorts that relied on participants’ memory of physical activity, potentially introducing recall biases. In addition, multiple studies included a high proportion of patients undergoing hybrid cemented THA, which may limit the generalisability of the results given the recent popularity of uncemented implants. Few studies included in this review directly compared THA to RHA using objective measurements and validated scales of physical activity and implant integrity. Finally, the study by Flugsrud et al. 22 accounted for 48.8% of the patients in our systematic review who underwent THA, potentially indicating over-representation of this study.
Conclusion
This review summarizes the current literature on the long-term impact of physical activity after THA and RHA. While patients should be encouraged to participate in physical activity following hip arthroplasty, they should also be counselled on the long-term impact of contact sports and activities that place an excess load on the joint. Better understanding the mechanisms by which excess physical activity, as well as specific types of movements, induce implant wear could allow physicians to more effectively counsel their patients following THA or RHA. Future studies should use standardised physical activity and implant integrity outcome metrics to compare the effect of physical activity and sports participation on the long-term implant integrity of patients who have undergone THA versus RHA.
Supplemental Material
sj-pdf-1-hpi-10.1177_11207000251315941 – Supplemental material for Long-term impact of physical activity and sports participation on implant integrity in resurfacing hip arthroplasty versus total hip arthroplasty: a systematic review
Supplemental material, sj-pdf-1-hpi-10.1177_11207000251315941 for Long-term impact of physical activity and sports participation on implant integrity in resurfacing hip arthroplasty versus total hip arthroplasty: a systematic review by Jordan J Levett, Abdulrhman Alnasser, Anthony Teoli, Simon Martel, Shawn Robbins, Olga L Huk, David J Zukor and John Antoniou in HIP International
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Jill Boruff, MLIS, AHIP for her assistance in piloting the bibliographic search.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.