
Abstract
Background:
Septic arthritis is a debilitating condition with prolonged treatment and adverse outcomes. A gram stain is often performed from the joint aspirate sample, followed by a definitive culture. In our study, we assessed the accuracy of gram staining for suspected septic arthritis and explored factors associated with positive culture growth and false negatives in the gram stain.
Methods:
We retrospectively reviewed joint aspirates performed from 2015-2021 at a major trauma centre. Aspirates not cultured for septic arthritis were excluded. Data collected included aspirate site, gram stain and culture result delay, patient demographics, orthopaedic/rheumatological history, and comorbidities. Outcomes measured were gram stain sensitivity and specificity. Factors influencing positive cultures and false negative gram stain results were analysed using logistic regression.
Results:
Of 408 joint aspirates meeting the criteria, 37 did not undergo initial gram staining. Gram stain sensitivity was 30.4%, specificity was 97.6%. The delay from aspirate to definitive gram stain and culture results was 1.1 and 5.4 days, respectively Logistic regression identified that prosthetic joint(p = 0.007), past joint infections(p = 0.006), arthritis(p < 0.001), hypertension(p = 0.007), diabetes(p = 0.019) were positively associated with positive cultures. Past joint infections(p = 0.004) were positively associated with false negative gram stain results. Patients on antibiotics during the aspirate had a higher risk of false negative gram stain results (OR = 5.538, 95%CI, 2.802–10.948; p < 0.001).
Conclusions:
In conclusion, the initial gram stain has limited sensitivity and caution should be exercised when interpreting negative results. Vigilance is crucial when the highlighted comorbidities or antibiotic use are present, to assess patients with potential joint infections.
Introduction
Septic arthritis is a medical emergency and can have very serious implications for patients. The incidence is between 4–29 cases per 100,000. 1 The patient typically presents with a hot and inflamed joint, most commonly lower limb, or systemic symptoms of illness like fever and tachycardia. 2 This presentation is shared by several other conditions and so further testing is necessary to confirm or rule out a diagnosis of septic arthritis. Missing this diagnosis can have severe consequences, given a 10% mortality rate of the disease and the risk of morbidity and disability.3 –5 Thus, rapid and accurate testing and treatment are required to confirm the diagnosis and treat the infection, typically through antibiotics and drainage to prevent dangerous complications.2,6
Current diagnostic testing typically involves aspirating the affected joint and then testing for organisms through a variety of methods, including gram staining,1,2 gram cultures,2,7 and white blood cell counts.2,8 Standard blood tests for infections, such as C-reactive protein (CRP), white blood cell (WBC) count or blood cultures, may also be done. 2 Newman’s criteria stated for septic arthritis to be diagnosed either: an organism should be identified from either the joint or bloodstream; or histological/ radiological evidence of infection and turbid fluid from the joint. 9
The risk of septic arthritis has been reported as significantly higher for those with risk factors (rheumatoid arthritis and immune-compromised). These reports compare the sensitivity and specificity of gram stains and cultures. 10 However, there has yet to be an up-to-date, robust report on predisposing factors for positive cultures and false negative gram stains from a large cohort of septic arthritis patients.
In this study, we sought to answer the following: (1) what is the specificity and sensitivity of gram staining; (2) What factors predispose patients to septic arthritis; (3) What factors predispose patients to have false negative gram stains?
Methods
Ethical approval was granted by the local ethics committee of our institution. This study received the project number 10244 on 27 December 2021. Informed consent was not required given the large, anonymised retrospective cohort nature of the study.
All aspiration procedures performed between January 2015 and January 2021 were included for review. A list of all individual theatre aspiration procedures was retrieved. Exclusion criteria included aspirates performed for reasons other than suspected septic arthritis, such as for therapeutic purposes or injecting medications into the joint.
We only included aspirations performed in theatres due to the homogenous nature and standardisation of the procedure in this setting. Aspirations performed in clinics or the emergency department were excluded as the technique is user dependent and can introduce various contaminants into the samples that obscure the comparability of the data set. 11
After retrieving the sample, gram staining was performed in the first instance, with a culture performed over the following days assessing for a range of organisms and sensitivities.
In our study, the last reported culture is taken as the gold standard for microorganism detection and septic arthritis diagnosis.
For each patient undergoing aspiration, the site of aspiration, Body mass index (BMI), smoking status, and broad-spectrum antibiotic usage status at the time of aspiration were collected. A wide range of comorbidities were also collected for analysis, including: vascular; cardiac; respiratory; neurological; immunological; rheumatological; renal; hepatic; haematological; endocrine; hypertension; and diabetes. Joint-specific problems were also collected, including a prosthesis of the affected joint, past joint infections, and arthritis of the specific joint.
From the patients who received an aspirate for septic arthritis, only patients where this was subsequently cultured were included. All associated clinical, demographic and comorbidity factors were then used to determine factors associated with positive culture septic arthritis cases. True negatives and positives, and false negatives and positives were calculated from the gram stain results. These were used to compute the sensitivity and specificity values for the gram stain.
SPSS IBM v28.0.1.0 was used for all data analysis. Multivariate binary logistic regression was used to assess predictors and associated factors for positive and false negative gram stain cultures. This was done because it is useful for clinicians to risk stratify patients and exercise hypervigilance with patients who specifically have a higher risk of positive culture septic arthritis, as well as exercise caution when facing certain cases of gram stain negative cases.
The individual odds ratios (OR) were calculated for each comorbidity and demographic class on either false negative gram stain or positive cultures.
A cutoff of p < 0.2 was used for inclusion in the multivariate modelling. Multicollinearity was assessed between the remaining variables, with a variance inflation factor of 5 used as a cut-off for exclusion, with the highest being excluded first, with an iterative process being used until all were under the threshold.
Results
The initial database search yielded 449 theatre performed joint aspirations. After applying the exclusion criteria, 41 aspirates were excluded, and 408 aspirations were included, performed on 352 unique patients. Of these, 371 procedures received gram staining. The exclusion process is documented in Figure 1.
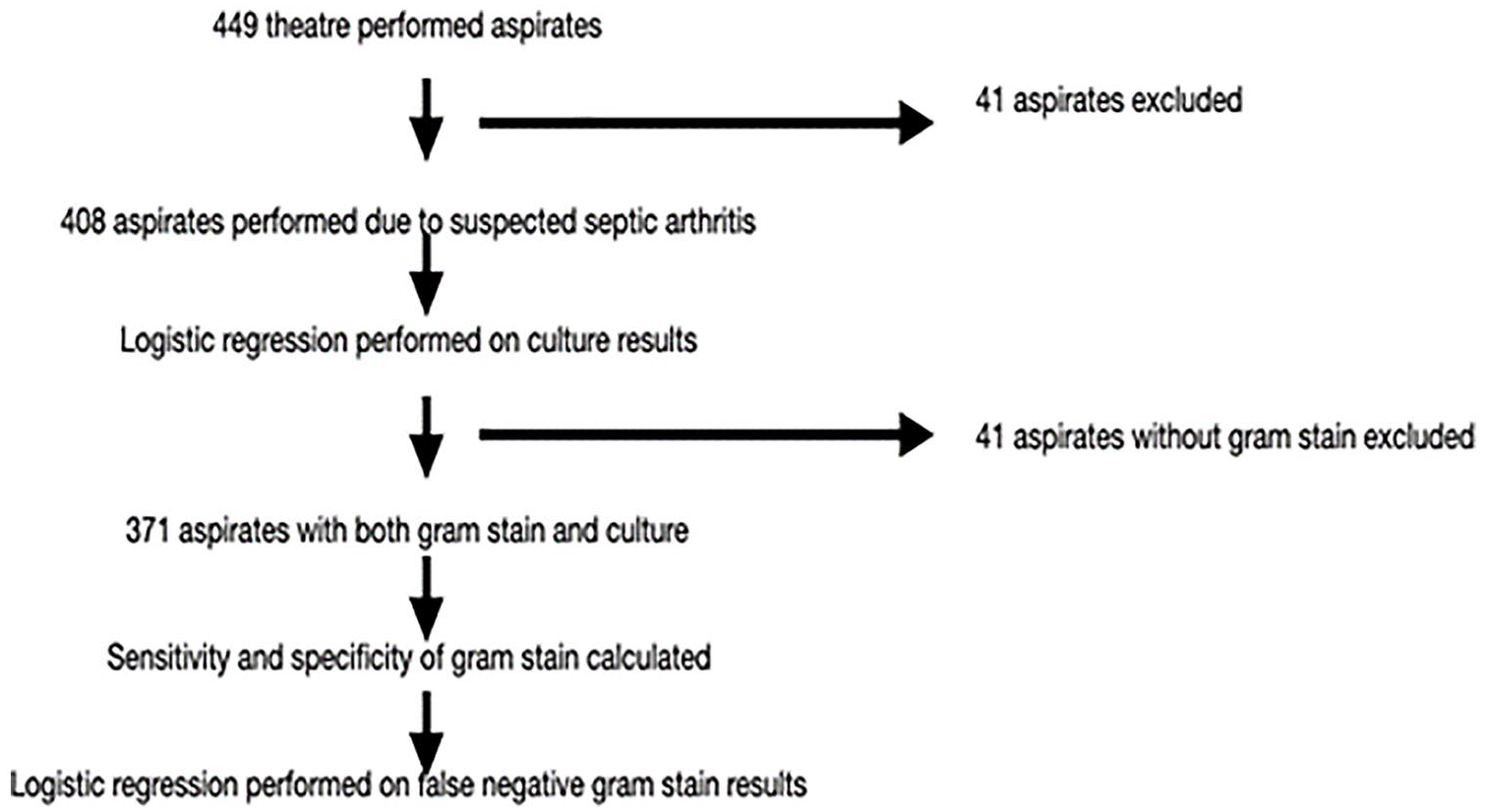
The application of the inclusion/exclusion criteria in various calculations in our study.
The cohort demographics are detailed in Table 1. The average patient was 66.9 years old with a BMI of 28.6 kg/m2, and 49.5% of patients were male. 7.8% smoked, 53.6% never smoked and 38.5% ex-smokers. Of the 371 aspirates performed, the majority were hip (245) or knee (153), with only 10 being performed on other joints. These joints were: 3 shoulder, 2 ankle, 2 elbow, 2 wrist, and 1 pelvis. The univariate analysis of each demographic and comorbidity factor on positive culture and false negative gram staining are reported in Table 2 and 3 respectively.
Demographic breakdown of the cohort.
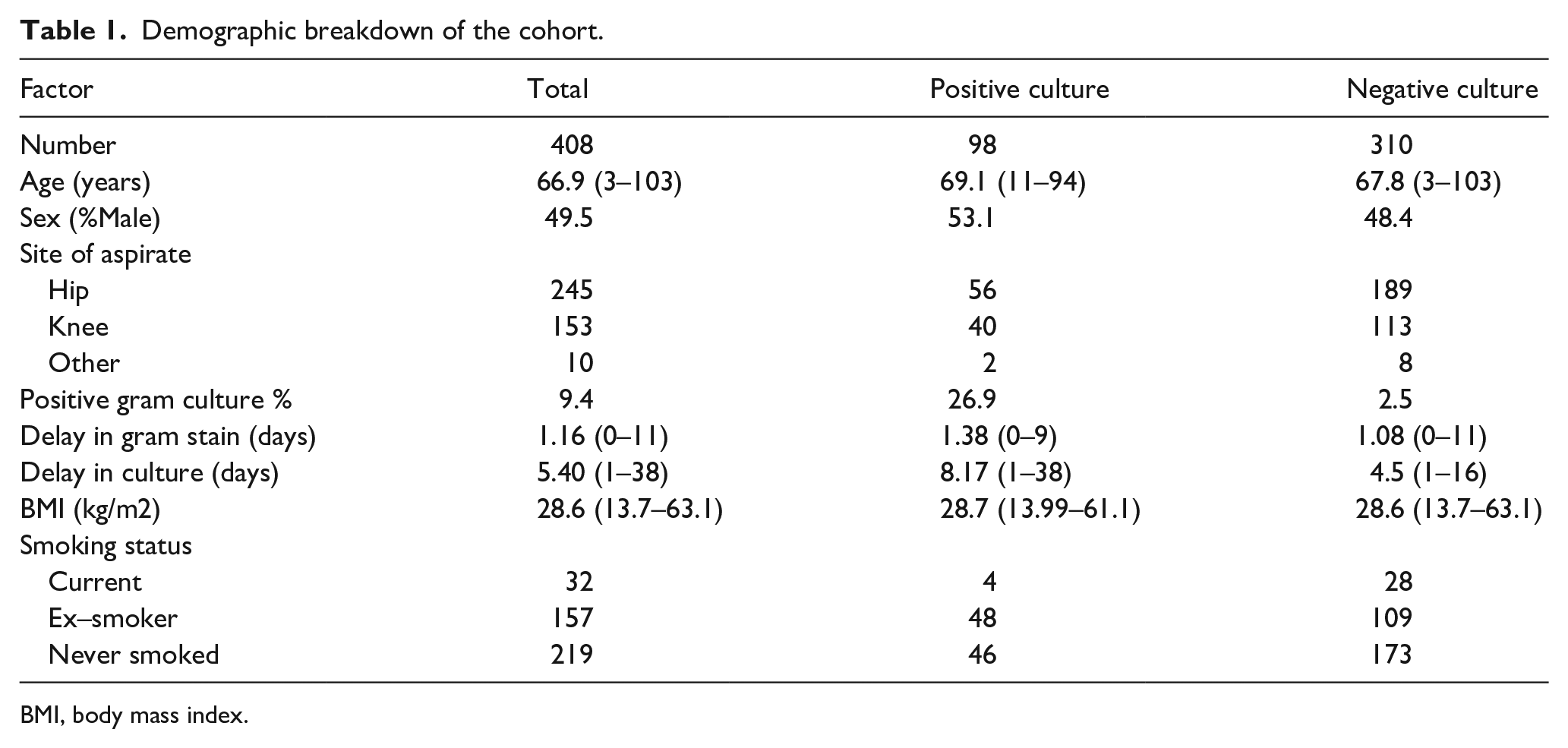
BMI, body mass index.
Univariate analysis of each demographic and comorbidity factor on having a positive culture aspirate.
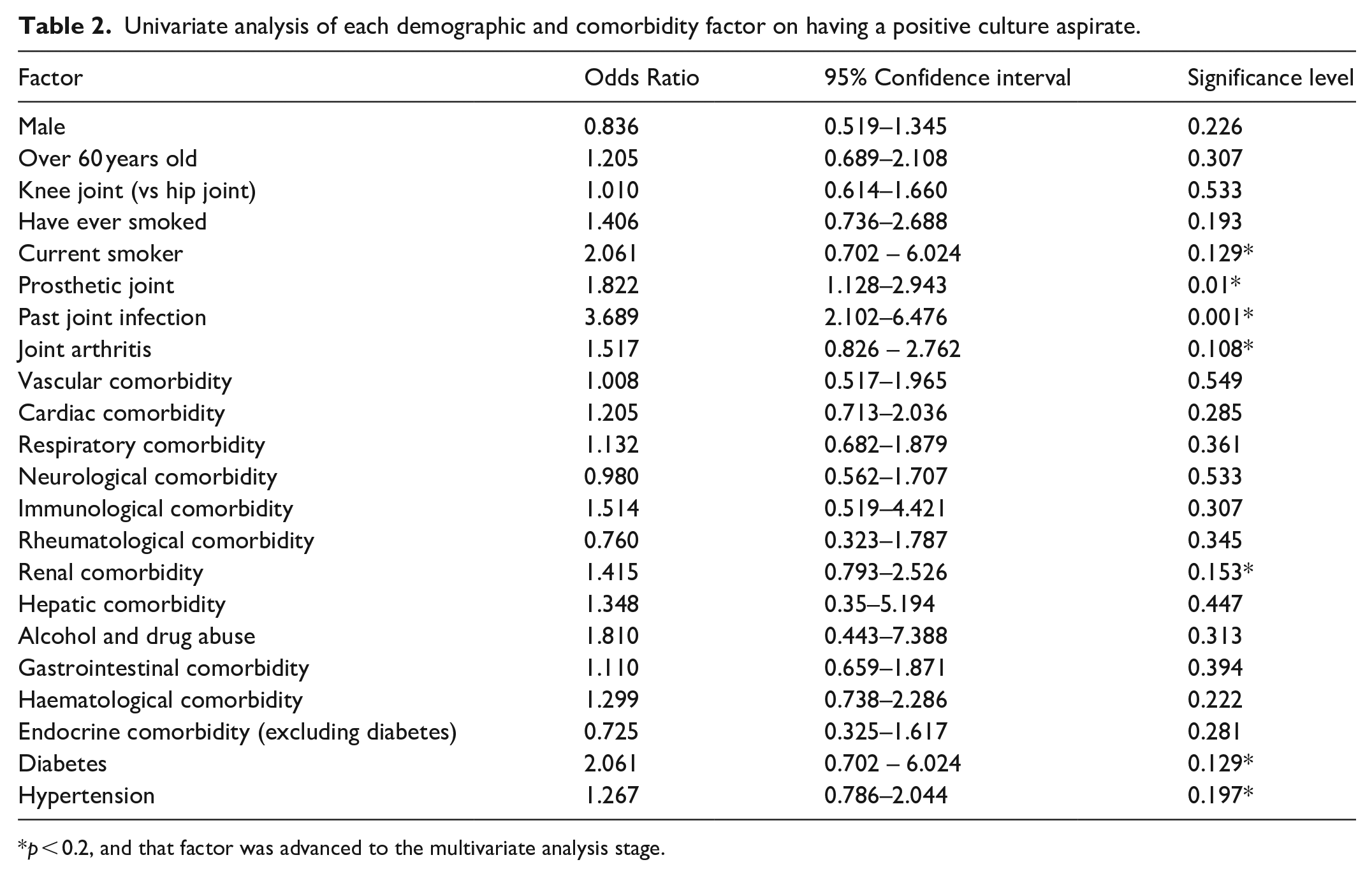
p < 0.2, and that factor was advanced to the multivariate analysis stage.
Univariate analysis of each demographic and comorbidity factor on having a false negative gram stain aspirate.
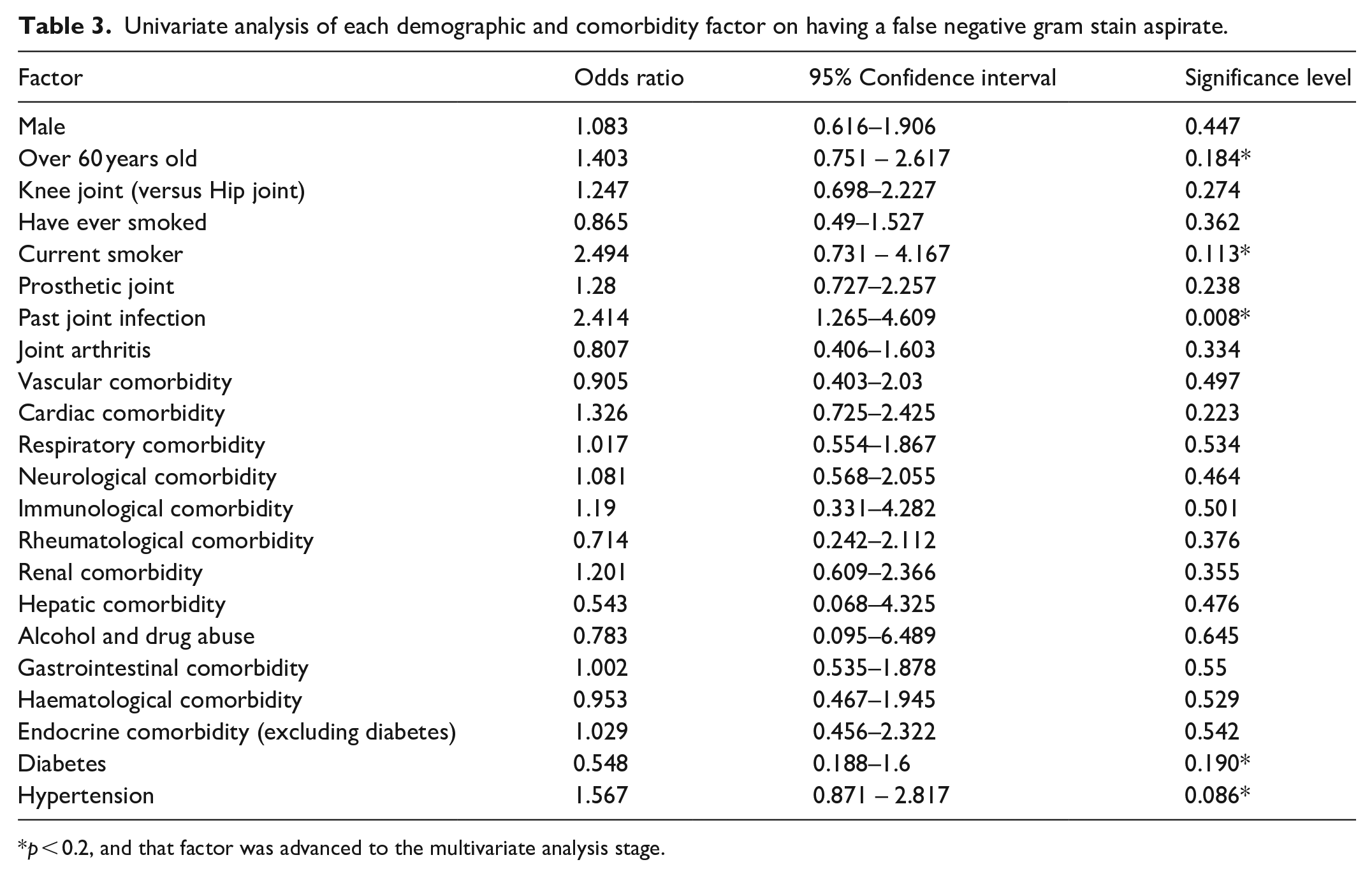
p < 0.2, and that factor was advanced to the multivariate analysis stage.
The time from aspirate to definitive gram stain and culture results were 1.1 and 5.4 days, respectively. Comparing the cultures and gram stains, showed there were 282 true negatives (TN), 25 true positives (TP), 7 false positives (FP) and 57 false negatives (FN) gram stains. The sensitivity and specificity of gram staining were 30.5% (95% confidence interval [CI] 20.5–40.4%) and 97.6% (95% CI, 95.8–99.4%). The positive and negative predictive values were 78.1% and 83.2%.
A threshold of p < 0.2 was chosen for inclusion in multivariable modelling.
The multicollinearity of the factors meeting the threshold was calculated, with a variance inflation factor of 5 chosen as the threshold for exclusion. No variables on either model had this degree of multicollinearity with other included variables.
The multivariable modelling on binary logistic regression of positive culture results is reported in Table 4
Binary logistic regression on positive culture result from joint aspirate.
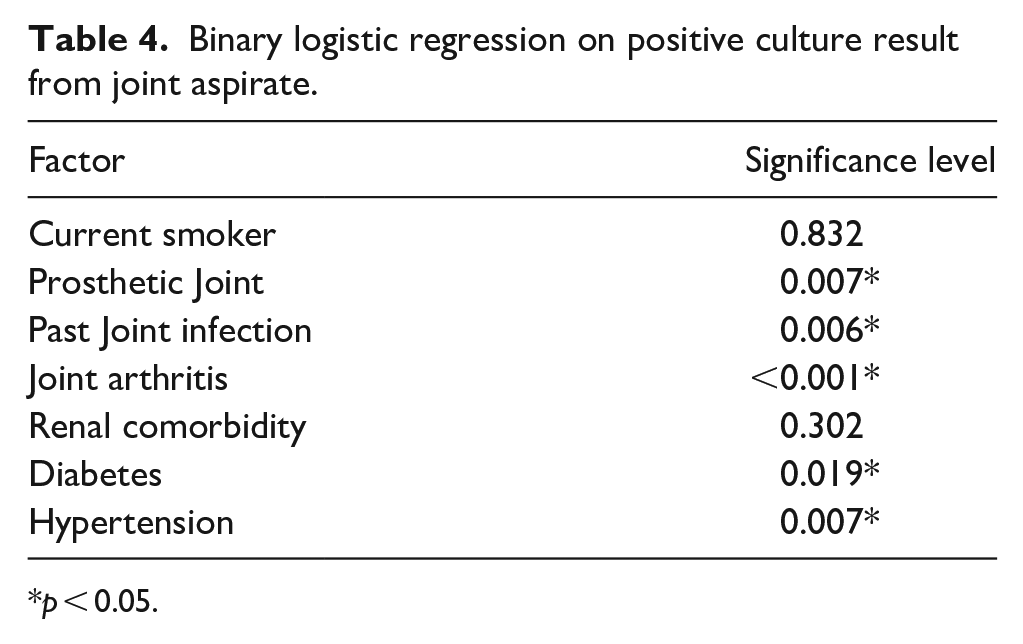
p < 0.05.
Similarly, the binary logistic regression for false negatives is detailed in Table 5.
Binary logistic regression on false negative gram stain result from joint aspirate.
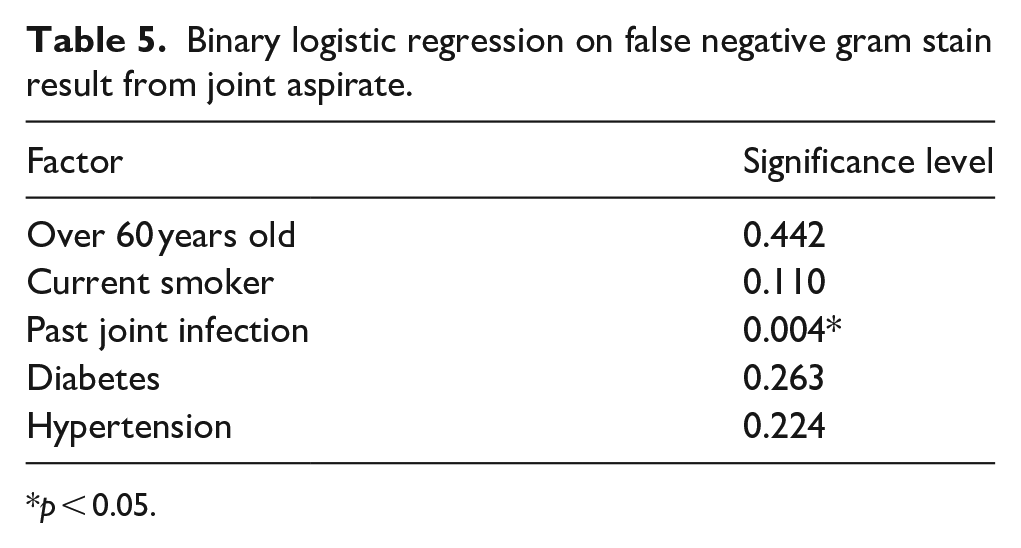
p < 0.05.
On multivariate modelling, the factors that had significance of p < 0.05 were highlighted.
Table 4 shows patients with prosthetic joints (p = 0.007), past joint infections (p = 0.006), arthritis (p < 0.001), diabetes (p = 0.019) and hypertension (p = 0.007) were at a statistically significantly higher risk of having positive cultures.
Table 5 shows patients with past joint infections (p = 0.004) were at a significantly greater risk of having a false negative gram stain.
Patients on antibiotics at the time of aspirate were also at higher risk of false negative gram stain results, which was statistically significant (OR = 5.538; 95% CI, 2.802–10.948; p < 0.001).
Discussion
Presentation, diagnosis and treatment of septic arthritis
The most common presentation of septic arthritis is pain, warmth and swelling of the hip or knee joint with a reduced range of motion.2,7,8 The patient, particularly if paediatric, may also present with systemic systems, including fever, chills and tachycardia.1,2,8,12 Blood tests may show a raised CRP, erythrocyte sedimentation rate (ESR), WBC count or procalcitonin.1,2,13
Imaging can be used though this has limitations. X-rays can help exclude other diagnoses though is not used in isolation due to a lack of sensitivity or specificity. 13 Ultrasound can be used to see joint effusions but has limited effectiveness if used within the first 24 hours. 13 Magnetic resonance imaging (MRI) scans are both specific and sensitive and show changes in the bone marrow and soft tissue in addition to effusions. 14 However, there are issues with access to this.
A large part of the diagnosis of septic arthritis is clinical suspicion based on the patient’s presentation. 7 On suspicion of septic arthritis, a joint aspirate is often done. This can be tested through a variety of methods, including a positive gram stain or culture of a joint aspirate; elevated WBCs in the aspirate. 1 On confirmation of the diagnosis, septic arthritis is typically treated by joint drainage in combination with intravenous (IV) antimicrobials.1,2
The duration of the treatment and specific drug used is determined by the pathogen, which can be identified through the gram culture.
If the treatment is delayed or unsuccessful, this can cause subchondral bone loss, permanent joint dysfunction or death.1,12
Diagnostic accuracy of gram stain
Gram staining is frequently used in the management of septic arthritis. Our results show that whilst it is specific, it is not sensitive. This aligns with existing research, which shows a high specificity of 97–100%. Values for sensitivity are lower though greatly vary from 22–81%. Our results, in addition to the existing literature, suggest that whilst it can be useful to confirm the disease, it is poor at ruling out patients who do not have septic arthritis. Therefore, using this test in isolation is very dangerous as the diagnosis of septic arthritis may be missed. As patients who have a positive gram stain will need a culture anyway to determine which organism is present and who to treat it and those who are negative will still need a culture to rule out septic arthritis due to the low sensitivity, the test has limited use. Table 6 shows the existing literature on the accuracy of joint aspirates from different settings.
The existing literature on the accuracy of joint aspirate gram staining in suspected septic arthritis.
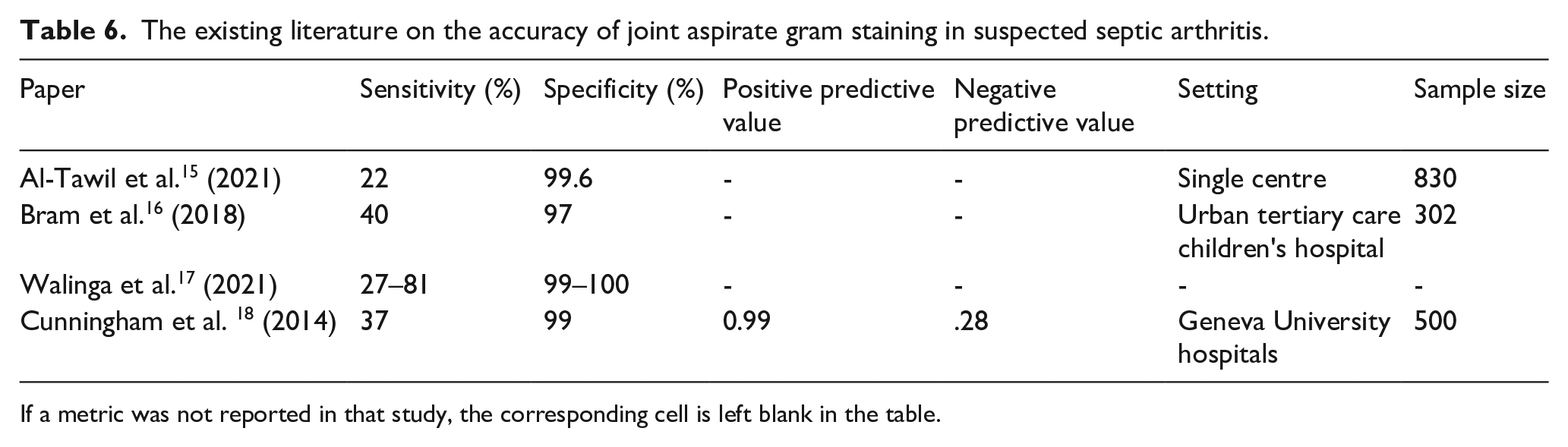
If a metric was not reported in that study, the corresponding cell is left blank in the table.
Risk factors for septic arthritis
Our analysis revealed that prosthetic joints, previous joint infections, arthritis, hypertension and diabetes were all associated with an increased risk of culture-positive septic arthritis.
Past medical history of diabetes leads to an increased risk of infections in general due to the dampening effect of hyperglycaemia on the immune system and an increased risk of skin infections due to diabetic neuropathy.1,7,19,20 Skin infections are independently associated with an increased risk.1,19,21,22
Past medical history impacting the joints has been linked to an increased risk of septic arthritis. These include arthritis,1,19,21,22 prostheses,1,7,19,22 and joint surgery.1,19,2,22 Prostheses and joint surgery are both linked to the development of septic arthritis due to the changes to the physiology of the joint, causing increased risk of haematogenous spread from other sources or during the surgery.1,19,20,22,23 Both rheumatoid arthritis (RA) and osteoarthritis are reported as risk factors for septic arthritis.1,19,21,22,24 RA causes significant joint damage, which is likely to increase the risk of infection. Collagen-induced arthritis, the most common type of RA, has been shown to increase the risk of septic arthritis in mice due to an excessive release of cytokines and eicosanoids. 25 It is also thought that using DMARDs and steroids in rheumatoid arthritis will decrease the immune response, which predisposes to most types of infections. 21 This is supported by other papers which show that the use of corticosteroids or a reduced immune response from chemotherapy or immunosuppression increases the risk of septic arthritis.1,7,20,22 OA is reported as a risk factor less frequently than RA in the literature and the increased risk is attributed to the associated joint damage. However, an experiment by Volkze and Müller-Hilke. 26 did not show that OA was linked to an increased risk of septic arthritis but was associated with factors, old age and prosthetic joints, which do.
Age is associated with many conditions that predispose to septic arthritis, such as joint prostheses, chronic diseases where immunosuppression is used or arthritis. It is therefore associated in many studies as a risk factor,1,19 –22,24 although was not associated with increased risk in our data set. Although this may be due to a higher threshold of over 80 being used in other studies. 24 Social factors, including drug or alcohol abuse,1,7,20 renal disease and liver disease have also been associated with increased risk.20,21
Risk factors for false negative gram stains in septic arthritis
Only past joint infections were associated with false negative results. We could not find any existing literature which examined this.
Limitations
A limitation of our study was its retrospective nature. Additionally, we assumed that gram culture is the gold standard. However, it has a false negative rate of 5–25%, meaning it is possible patients with septic arthritis were not included in the study. 27 Additionally, only samples done in theatre were included, which could make the sample size less reflective of everyday clinical practice. We did this to reduce the risk of contamination and less user and case dependent variability. However, it is still possible that the cultures were contaminated on collection or in the lab.
Conclusion
Our study investigates outcomes of gram staining and culture of large cohort of patients undergoing aspiration for suspected septic arthritis. The initial gram stain is relatively fast and specific for culture positive septic arthritis, however it has poor sensitivity, and so can create false reassurance for clinicians in the management of this clinical presentation. Given the severity of the long-term rehabilitation prospects of septic arthritis, we recommend a high level of caution to any negative gram stain results in these clinical presentations, especially for patients with the highlighted current and past comorbidities investigated as risk factors in our statistical modelling.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.