
Abstract
Background:
There are variations in the performance of individual prostheses used in hip replacements. Some of which have unexpectedly higher revision rates – outliers. The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) has established a standardised multi-stage approach for identifying these devices. This is done by comparing the revision rates of individual prostheses to all other prostheses in class, with the exception of large head metal-on-metal (LHMoM) prostheses. However, improvements in device design and performance over time have required a need to reconsider the comparator group. This study aimed to identify a more specific comparator to better reflect contemporary surgical practice.
Methods:
The time to first revision was estimated on the data of 413,417 primary total conventional hip replacements undertaken for osteoarthritis (OA) from 01 January 2003 to 31 December 2019. Survivorship analyses with stepwise exclusions were undertaken. The first exclusion was LHMoM, followed by other non-modern bearing surfaces (defined as all the bearing couples except metal or ceramic heads on cross-linked polyethylene and mixed ceramic-on-ceramic), and then devices with modular neck-stem design or used for specific purposes (incl. constrained, dual-mobility, and head size <28 mm). Lastly, all remaining prostheses previously identified as having a higher than anticipated rate of revision (HTARR) were also excluded.
Results:
These exclusions progressively reduced the cumulative percent revision (CPR) rate. The final comparator, which only includes satisfactory-performed prostheses of contemporary design and use, has a 10-year CPR of 4.30% (95% CI, 4.2–4.41) which is lower than 4.93% (95% CI, 4.84–5.02) for the current comparator used by the AOANJRR (all prostheses excluding LHMOM). Over the study period, 13 additional components were identified utilising the modified comparator.
Conclusions:
The calculation of the comparator revision rate should be re-evaluated to include only modern prosthesis constructs to ensure that poorly performing prostheses are identified early.
Introduction
Total hip replacement (THR) is the surgical treatment for end-stage hip osteoarthritis (OA).1,2 Even though joint replacement is an effective surgical procedure with high success rates, concerns continue to exist with respect to variation in prosthesis performance and, in particular, prostheses introduced to the market that are consequently shown to have a higher than anticipated revision rate (HTARR). Recent data show that the outcomes of THR have improved over time but suboptimal results due to less than satisfactory implant performance do still occur. 3 An important role for joint replacement registries is to monitor the comparative performance of implants to identify factors that are associated with higher rates of revision.
Registries record detailed information on procedures performed as well as patient outcomes.3 -7 They are also able to provide population-based data on the comparative outcome within a community. Outcome data on the revision rate of individual devices are necessary to enable an evidence-based approach to prosthesis selection. Analyses of registry data have found that the majority of the prostheses currently in use have satisfactory outcomes.8,9 However, a number of prostheses have been identified as having a rate of revision that is higher than other prostheses in the same class.
The AOANJRR has previously developed a standardised multi-stage approach for detecting outliers based on a comparison of the revision rate of an individual prosthesis (either femoral stem or acetabular cup) with the comparator group — defined as all other prostheses in the same procedure class with the exception of large head metal-on-metal (LHMoM) prostheses. 10 The entire class of LHMoM devices has been previously identified as having a significantly higher risk of revision and their inclusion in the comparator group would overestimate the revision rate. The purpose of this activity is to identify early those devices that are not performing at an acceptable level. The identification of outlier devices assists surgeon prosthesis selection, improves patient outcomes, and reduces healthcare costs. 11 The prostheses identified are listed in the Annual Report of the AOANJRR.
The current comparator group used by the AOANJRR has some limitations as non-routine procedures reflected by the use of complex prostheses are not excluded. Prostheses parts or bearing surfaces that are known to be associated with higher revision rates, other than LHMOM, are currently included. For example, high-risk prostheses such as modular-neck stems or prostheses used for specific purposes (including constrained, dual-mobility, and head size <28 mm) are considered in the current comparator.12 -14 In addition, improvements are continually being made in the design, manufacture and performance of many devices over time. The comparator group may not adequately reflect contemporary practices and is likely to overestimate the standard revision rate. 3
The aim of this study was to assess a number of different comparator group options to provide a more relevant standard revision rate for evaluating the comparative performance of new devices and identifying prostheses with a HTARR.
Materials and methods
The study period was from the first year that the AOANJRR collected THR data from all Australian hospitals (January 2003) to the closure of the dataset at the end of December 2019. The study population included all patients undergoing a primary total conventional hip replacement performed for primary osteoarthritis (OA). This selection initially included 413,417 procedures. A number of specific exclusions were then undertaken to assess the impact on the cumulative percent revision of the different comparator groups. The first exclusion was LHMoM, followed by other non-modern bearing surfaces (defined as all the bearing couples except metal or ceramic heads on cross-linked polyethylene and mixed ceramic-on-ceramic), and then devices with modular neck-stem design or used for specific purposes (including constrained, dual mobility, and head size <28 mm). Lastly, all remaining HTARR prostheses previously identified by the multi-stage standard approach were excluded (Figure 1). The AOANJRR standard methodology for identifying HTARRs was employed to determine the impact of modified comparator on the number of identified outliers.
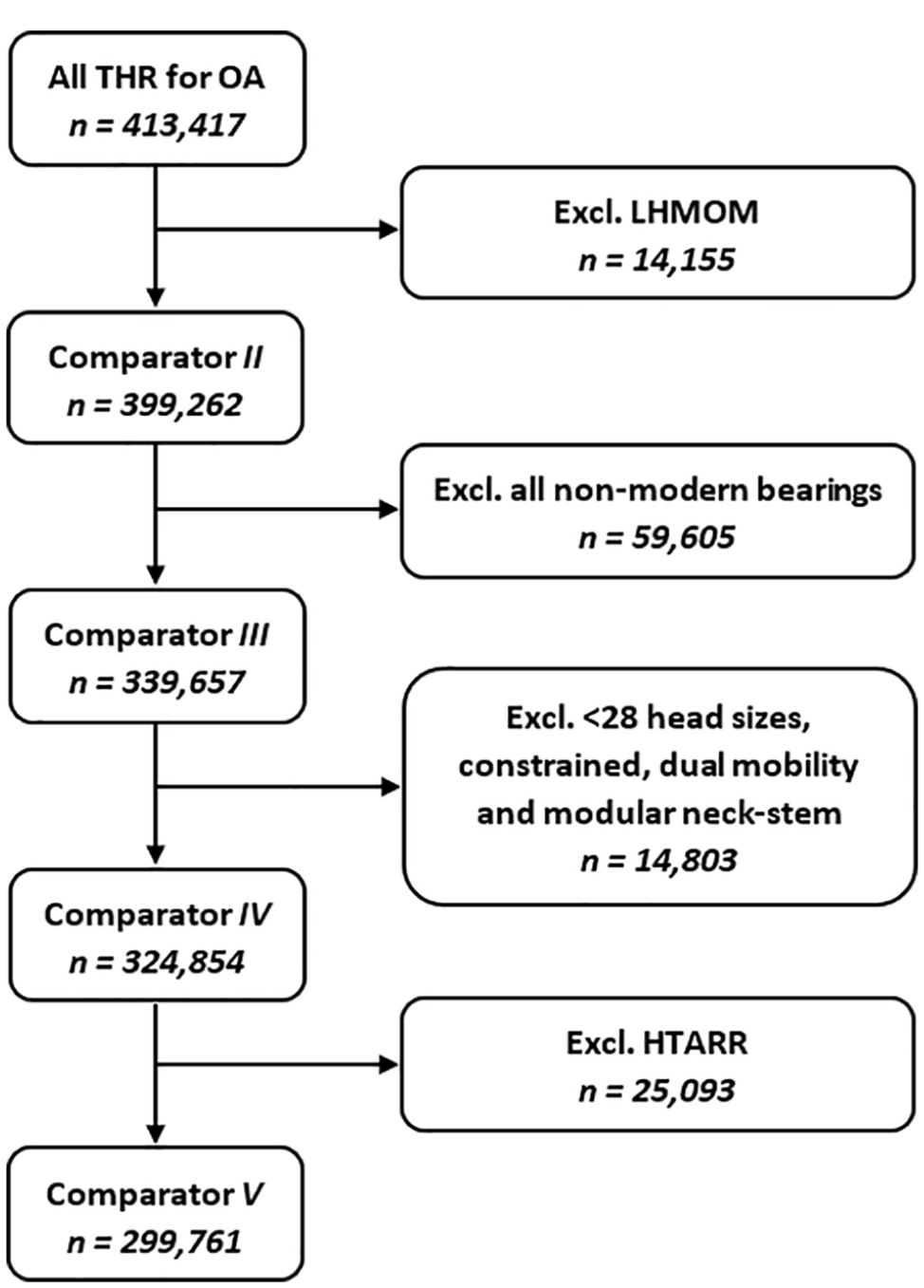
Flow chart showing stages of exclusion criteria and study populations.
We performed a stepwise exclusion of various prostheses and classes. The current comparator excluded all LHMOM. Next, all non-modern bearing surfaces were excluded because they are rarely used and accounted for <4% of primary THR procedures performed in 2019. 3 The next exclusions were devices with modular neck-stem design or used for specific purposes. Modular neck components can dissociate and break due to corrosion and wear at the modular junction and also as a class of devices have been shown to have higher rates of revision than the same fixed neck designs.13,14 Dual-mobility and constrained acetabular prostheses are used more frequently for patients with a higher risk of dislocation. 15 Head sizes ⩽28 mm have a higher revision rate for dislocation and are used uncommonly in standard modern total hip replacement.12,16 Finally, the remaining prostheses previously identified as having HTARRs by the AOANJRR were also excluded from the comparator. The research was conducted according to the ethical principles of the Helsinki Declaration II. The Southern Adelaide Clinical Human Research Ethics Committee has also provided ethics approval for this study (No. 485.13).
Statistical method
The primary outcome measure was time to first revision surgery, defined as reoperations of previous hip replacements where 1 or more of the prosthetic components are replaced, removed, or added. Death was treated as a censored case with survival time based on the time those cases exited the study sample. Patients with no revision or death had survival times based on the time elapsed between their initial implantation date and the end of the follow-up period. 5 comparator groups, the study populations (Figure 1), all in primary conventional THR performed for OA were studied using Kaplan-Meier (KM) survival analysis. 3 The unadjusted cumulative percentage revision (CPR) was calculated after the primary surgery, with an accompanying 95% confidence interval (CI) using unadjusted pointwise Greenwood estimates. Since each study population is defined as a subset after the exclusion, statistical comparisons of revision rates were not undertaken with Hazard Ratios (HRs). However, given the significant role of bearing surface on the survivorship of comparator, revision rates of the prostheses with non-modern against modern bearings were compared for the entire period using Cox proportional-hazards model when adjusting for age and sex. Finally, the effectiveness of the modified comparator was evaluated based on the ability to detect additional individual prostheses by performing the first 2 stages of the AOANJRR standard procedure for identifying outlier prostheses. This is done by comparing the revision rate of individual prostheses to twice the average revision rate of all other prostheses that belong to the same broad device class and reporting the results for femoral stems and acetabular cups separately. In addition, the impact of confounding factors is examined by calculating age- and gender-adjusted HRs to check if there is a significant difference compared to the combined HR of the comparator group. 10 The statistical analysis was performed using R software, 17 including the packages Survival version 3.2-11 and Survminer version 0.4.9.18,19
Results
Results shown in Figure 2 and Table 1 present the CPR among the comparator groups showing the proportion revised over the years. The CPR at 10 years for the current comparator was 4.93% (95% CI, 4.84–5.02), and the subsequent exclusions progressively reduced the CPR rate. Comparator V showed the lowest 10-year CPR of 4.30% (95% CI, 4.20–4.41). However, there was no significant difference in the 10-year CPR for Comparator V compared to Comparator IV 4.40% (95% CI, 4.30–4.50). The restriction to modern bearings (Comparator III) resulted in a large reduction in the CPR compared to the current comparator group (Comparator II) at 10 years.
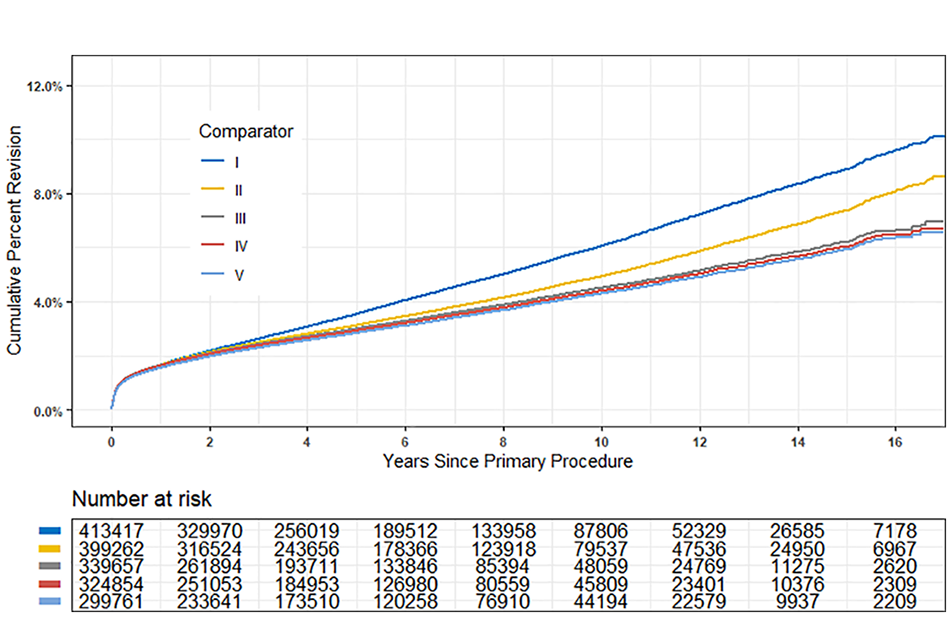
CPR of the study populations over the study period.
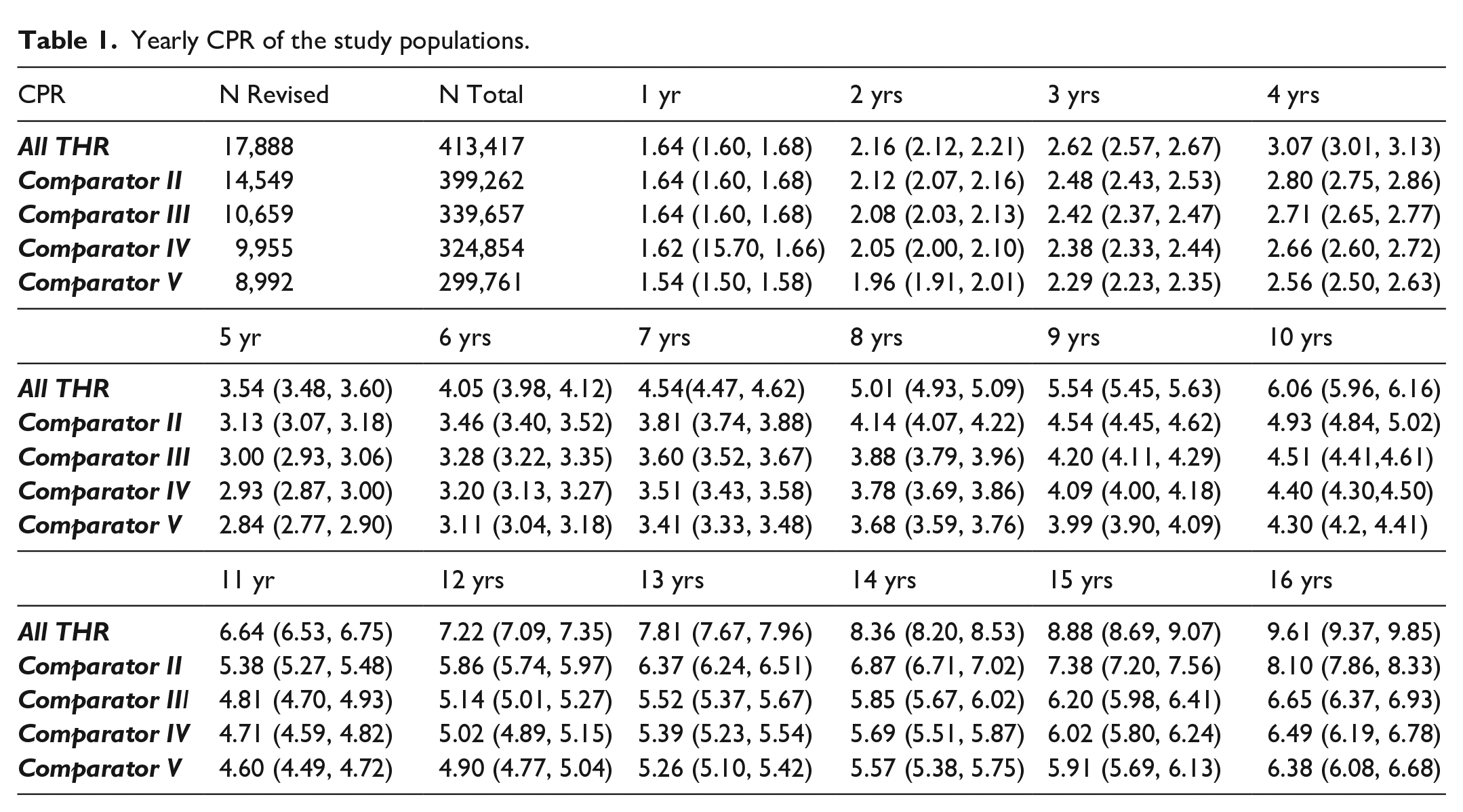
Yearly CPR of the study populations.
Given the substantial effect of excluding non-modern bearings (1st and 2nd exclusions) on the CPR of all primary THR, the risk of revision was compared by the type of bearing surfaces (non-modern vs. modern). This is done to enable more specific and valid comparisons of the risk of revision between two groups of devices over time. The pattern of variation in risk has significant consequences with respect to the underlying reasons for any difference. There was a significantly higher rate of revision for the non-modern compared to the modern bearing surfaces (hazard ratio [HR] 2.00; 95% CI, 1.94–2.06; p < 0.001) (Figure 3).
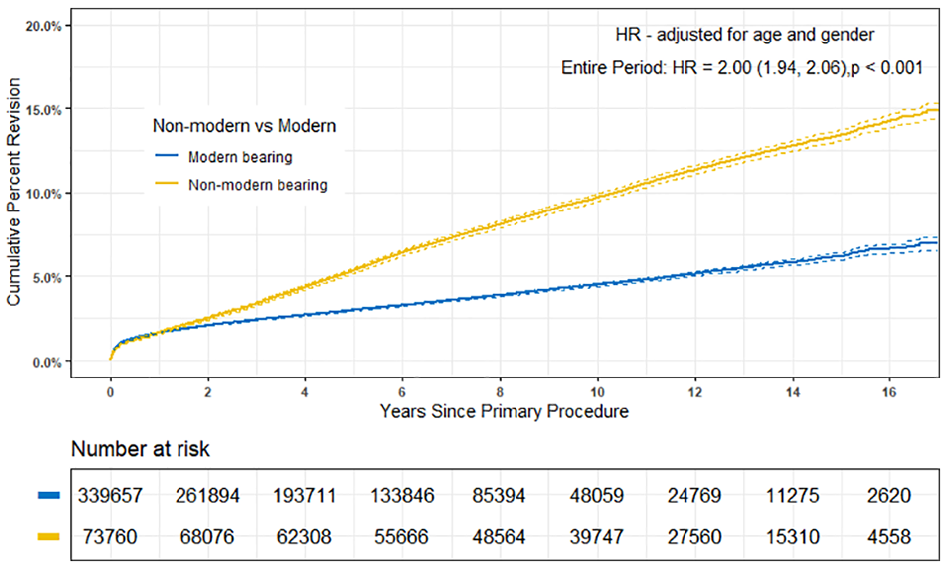
CPR of primary conventional THR by the type of bearing surface.
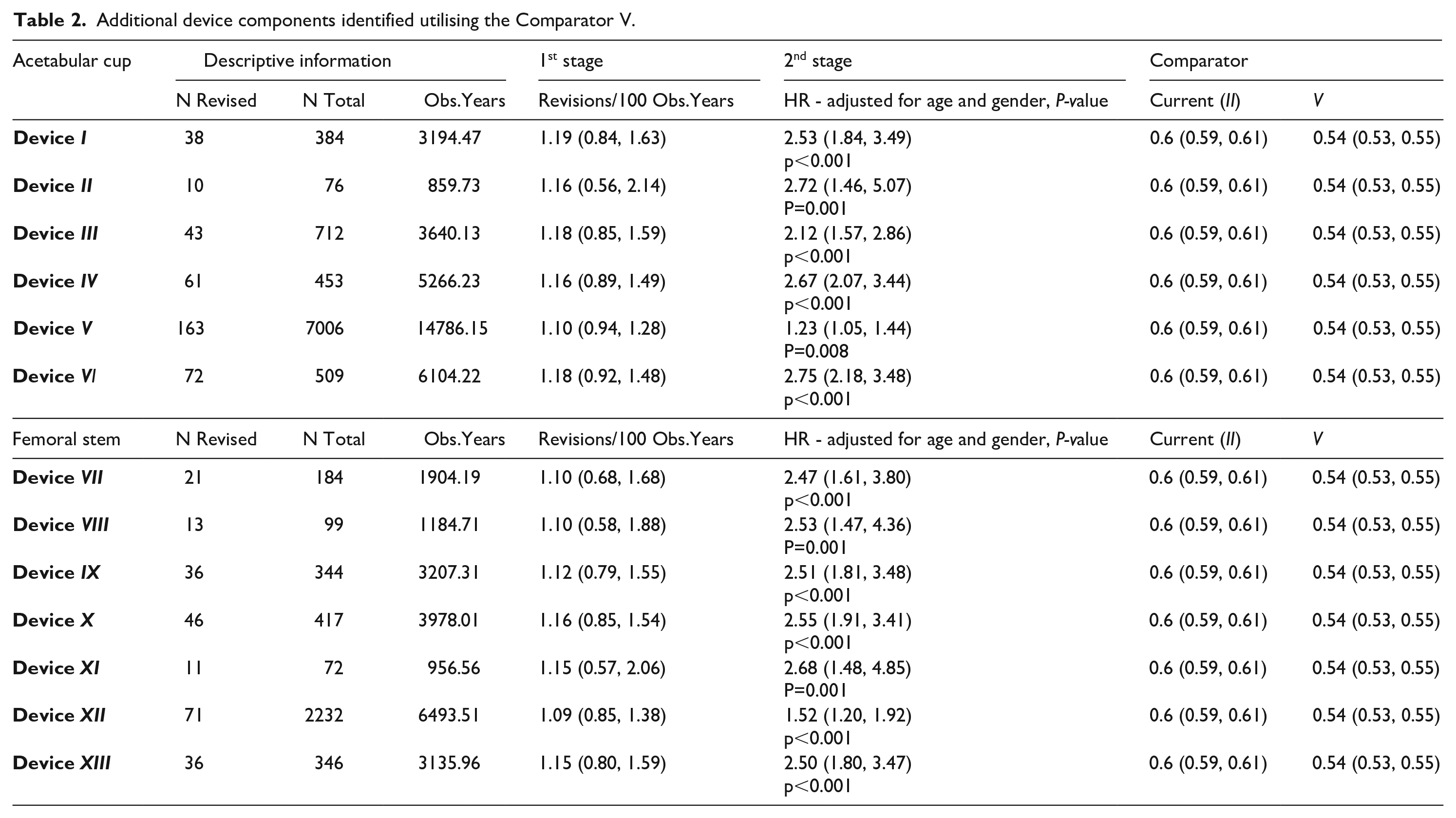
The additional prostheses were identified using Comparator V as the comparator rather than the current comparator (Comparator II). The revision rates per 100 component years of these individual devices exceeded twice that of Comparator V (but not twice than that of Comparator II). In addition, there are significant differences in HRs of the identified devices with the Comparator V over the entire period. The first 2 stages of the AOANJRR standard procedure detected 13 additional device components utilising the modified Comparator (V), including 7 femoral stems and 6 acetabular components (Table 2).
Additional device components identified utilising the Comparator V.
Discussion
This study has demonstrated that the rate of revision declines with selective exclusions of devices from the nominated comparator group. Therefore, using only contemporary device components (Comparator V) has the potential to be a more relevant comparator for the early assessment of modern primary total hip prostheses. The more restricted comparator cohort (modified Comparator V) led to the identification of additional devices after the 2nd stage of the AOANJRR standard procedure.
Reviews of prostheses included in the comparator cohort and exclusion of high-risk designs or those used for specific purposes and complex patients are required periodically to ensure a more relevant and effective comparator. In future studies, the modified comparator (V) may contribute to the early detection of an outlier prosthesis with a smaller sample size and shorter length of follow-up.
While Comparator V had the lowest CPR, there was only a marginal difference between Comparator IV and V. This was because many of the HTARR prostheses were already excluded because they were LHMOM, modular-neck femoral components, or used non-modern bearings.13,20,21 The AOANJRR approach to the identification of outlier procedures takes into account the complexities of a small number of procedures, 22 devices implanted by a single surgeon, 23 and the confounding impacts of other components in an individual device. 10 Identification can generally bring a device to the attention of surgeons, alerting them to the fact that it shows a higher rate of revision. 9 After device identification by the AOANJRR, the use of the device usually declines. For example, the ASR acetabular component was first identified in 2008 and was removed from the market in Australia by the manufacturer the following year. 24 The use of all LHMoM prostheses peaked in 2009 and after identification in the 2010 Annual Report, there was an 87.5% reduction the following year.25,26
There are limitations to this research. Other factors related to patient, surgeon, and surgical approach may be important in the variability of prosthesis performance but were not included in this study. For example, the HRs were not calculated when adjusted for body mass index (BMI) and American Society of Anesthesiologists (ASA) score. The registry has BMI data from 2015 and national data on ASA scores since 2012. Further study may need to be conducted to estimate primary total hip outcomes by specific prosthesis design constructs while controlling for the confounding factors. However, there are also some strengths, including large high-quality data with minimal loss of follow-up over a longer-term period provided by the AOANJRR, which allowed us to compare the study populations effectively. Registry outlier detection is a process that needs to evolve to optimise the detection. This would be enhanced by international collaborations between registries including data sharing. 27 The results of this study indicate that increasing the relevance of the comparator may be helpful for the early identification of a higher number of outlier prostheses.
Conclusion
Using a comparator that only includes contemporary devices with modern bearings may be a more appropriate way of identifying devices with HTARRs than is currently employed.
Footnotes
Acknowledgements
The authors acknowledge the AOANJRR, whose data made this study possible and supported the study design and statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.