
Abstract
Background:
The use of larger femoral heads in total hip replacement (THR) has increased over the last decade. While the relationship between increasing head size and increased stability is well known, the risk of revision with increasing head size remains poorly understood. The aim of this study was to compare the outcome of total hip joint replacement with 32-mm and 36-mm heads.
Methods:
We carried out a 20-year retrospective analysis of prospective data from the New Zealand Joint Registry (NZJR). All primary total hip replacements registered between January 1999 and December 2018 were included. We compared the rate of revision of 32-mm and 36-mm heads in THR. Sub-group analysis included comparisons of bearing type and all-cause revision.
Results:
60,051 primary THRs met our inclusion criteria. The revision rate per 100 component years was significantly higher with a 36-mm head than with a 32-mm head (0.649 vs. 0.534, p < 0.001). Subgroup analysis of bearing type showed no significant differences in revision rates for all combinations of 36-mm heads when compared to 32-mm (p = 0.074–0.92), with the exception of metal-on-metal (MoM); p = 0.038. When MoM was removed there was no significant difference in revision rates per 100 component years between 32-mm and 36-mm heads, 0.528 versus 0.578 (p = 0.099).
Conclusions:
Increasing head size from 32 mm to 36 mm results in no significant increase in revision in all bearing combinations except MoM.
Introduction
The global use of larger-diameter femoral heads has become increasingly common.1–7 With the rising use of more wear-resistant cross-linked polyethylene, the use of larger heads to achieve greater stability has become more acceptable. The size of femoral head used in THR has gradually increased from 22 mm in the 1960s to 28 mm in the 1990s, and thereafter to 32 mm in the mid-2000s. 8 Furthermore, registry data shows that the use of 36 mm heads has steadily increased since the mid-2000s (Figure 1).1–7 Globally the most commonly used head diameter in THR remains at 32 mm.1,3,6,7 Of note, Denmark predominantly uses 36-mm heads which comprise 62% of all Danish THRs carried out in 2017 (Figure 2). 2

Head sizes by year in the NZJR.
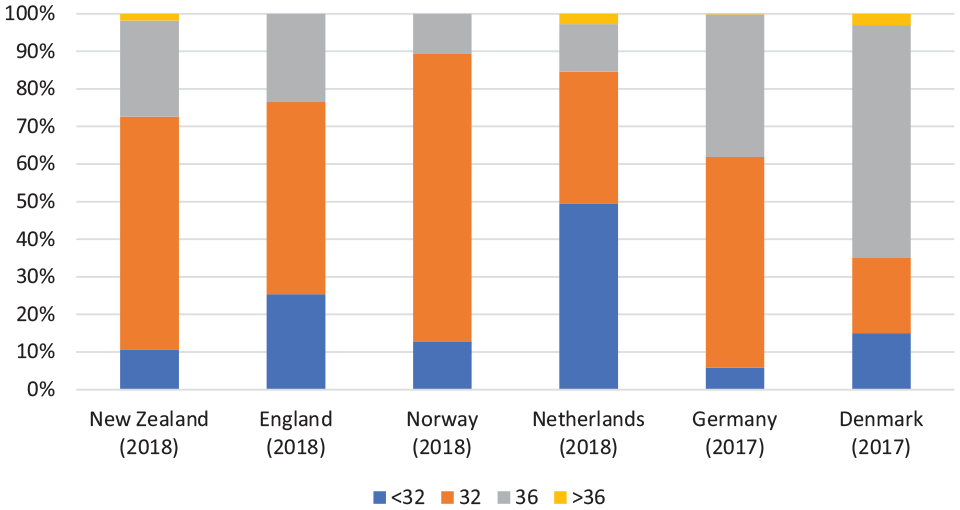
Head size use in respective country joint registries.
The intended benefit of increased head size is to reduce the risk of dislocation. Larger heads allow a wider impingement-free range of movement (ROM) 9 and a greater jump distance. 10 Many studies11–15 have shown a lower dislocation rate in THR with heads of ⩾32 mm when compared with 28-mm heads. A recent study from the Dutch Registry, which compared 32- and 36-mm heads, found a higher risk of revision for dislocation with 32-mm heads but only when the posterior approach was used. 13 A prospective study 16 using data from the New Zealand Joint Registry (NZJR) compared 3 groups with different diameters of head (<36 mm, 36 mm and >36 mm) and showed that the use of a 36-mm femoral head does reduce the risk of dislocation. It also showed that there was no clinical difference in functional outcome between the 3 groups.
Despite this, there is ongoing concern about the relationship between larger femoral heads and THR longevity from bearing wear and taper corrosion.17,18
There are only 3 studies in the literature that compare the risk of revision for 32-mm and 36-mm heads.13,19 A study by Tsikandylakis et al. 19 looked at only metal-on-polyethylene (MoP) configurations in the Nordic registry. They compared the risk of revision for dislocation and all causes between 28-mm, 32-mm and 36-mm heads. 19 They found the all-cause revision risk was higher for patients with a 36-mm head than for those with a 32-mm head (hazard ration [HR] 1.14; 95% CI, 1.04–1.26) and no difference in the revision rate for dislocation (HR 0.85; 95% CI, 0.70–1.02). Another study by Tsikandylakis et al. 20 using the Nordic registry looked at revision rates for 32- and 36-mm heads when used for proximal femoral fractures. They were not able to show any clinically relevant revision risk reduction for any reason, including dislocation, for the 36-mm heads. A study by Zijlstra et al. 13 compared head size and surgical approach using data from the Dutch Arthroplasty register. For all approaches, their data showed that 32-mm heads reduced the risk of dislocation when compared to 22- and 28-mm heads (HR 1 and 1.6, respectively). Furthermore, 36-mm heads increasingly reduced the risk of revision for dislocation but only when using the posterolateral approach (HR 0.6), while the risk of revision for other reasons was unchanged.
To date there is no conclusive evidence to confirm whether there is a survival advantage from using a 36-mm head.
We report the effect of 32 and 36 mm head sizes on survival of primary THRs in the New Zealand Joint Registry. We looked at all combinations (metal, ceramic and polyethylene bearing surfaces) and the reasons for revision.
Materials and methods
We carried out a retrospective study of 60,051 primary THRs undertaken between 1999 and December 2018 that were recorded by the NZJR.
We retrieved data on all patients recorded in the database who had undergone a primary THR for primary osteoarthritis (OA) with a 32- or 36-mm femoral head. All bearing surfaces, all approaches, all types of fixation (both cemented and uncemented), bilateral THR, and all skill sets of primary operating surgeon were included. We excluded all other indications for primary THR in the New Zealand Joint Registry including rheumatoid arthritis and other inflammatory conditions; acute and chronic fracture of neck of femur; developmental dysplasia; dislocation and post-acute dislocation; avascular necrosis; tumour and ‘other’. Resurfacing arthroplasties and dual mobility acetabular components were also excluded. When looking at revisions, we included those carried out for: loosening of the acetabular component; loosening of the femoral component; dislocation; ‘pain’; deep infection and periprosthetic fracture of the femur. We excluded those carried out for previous hemiarthroplasty and removal of components. Sub-group analysis included comparisons of bearing type; ceramic (C), polyethylene (P), metal (M) and all causes for revision.
A total of 60,051/132,550 patients (52% of 116,488 THRs undertaken for OA registered in the NZJR between 1999 and December 2018 with bearing size and material defined) met the inclusion criteria and were grouped according to the head diameter used: 32 mm (42,639 [71%]), and 36 mm (17,412 [29%]). The mean age at primary THR was 67 years (13–101 years), 53% (67,785 of 128,155) of patients were women (Table 1). 7
Demographics and technical aspects.
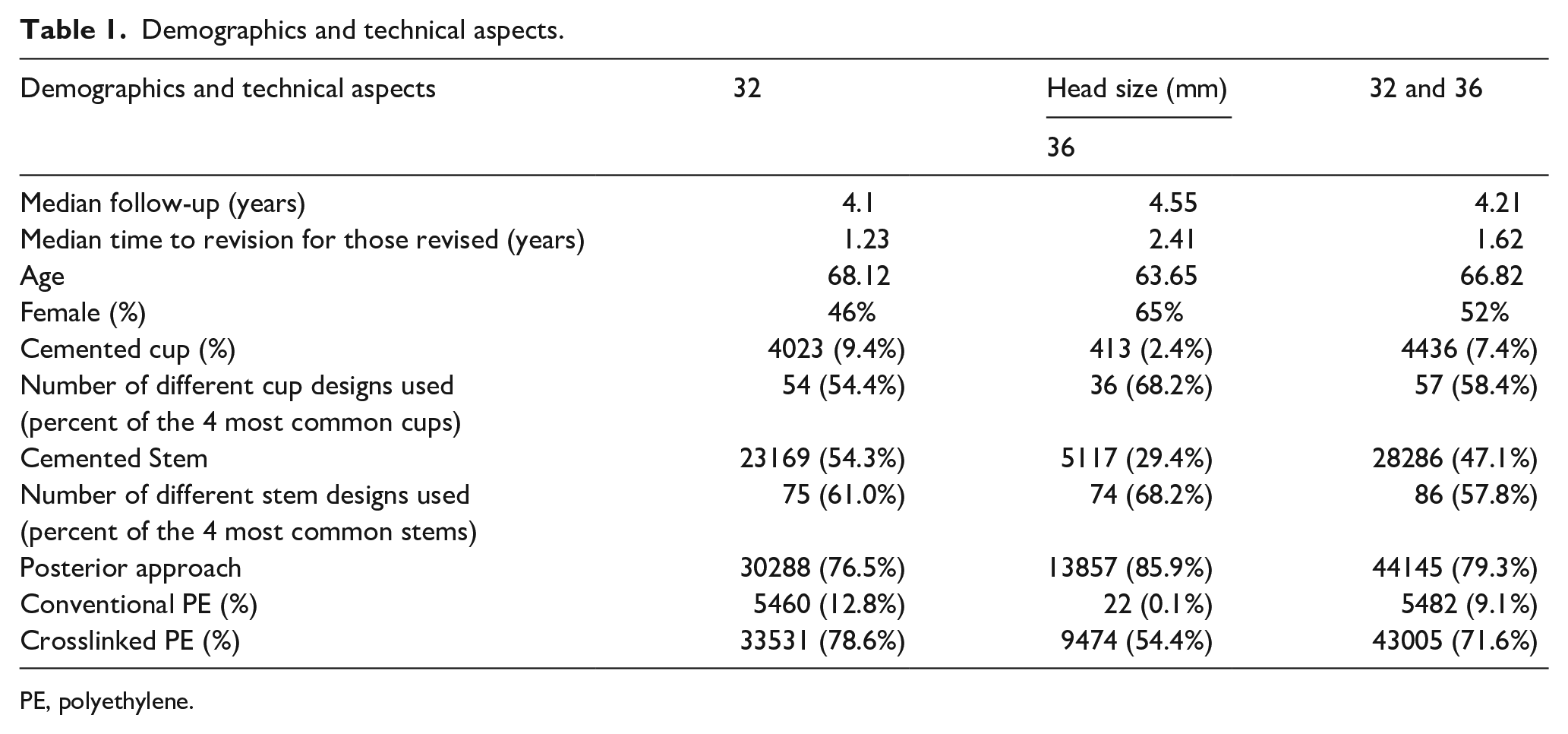
PE, polyethylene.
The primary outcome of the study was to compare the rate of revision of 32 mm and 36 mm heads in primary total hip replacement (THR). A secondary outcome was to perform a sub-group analysis of bearing type; ceramic (C), polyethylene (P), metal (M) and all causes for revision.
Revision was defined as the exchange of the entire implant or any of its parts. Procedures that involved only the removal of, or only the addition of, a component were not included: at least 1 component had to be replaced.
Comparisons of revision rates between size groups were undertaken using log-rank tests and are summarised as revision rates per 100-component years with 95% confidence intervals (CIs) derived from a Poisson approximation. Analyses were undertaken using SPSS, Version 25 (IBM, Chicago, IL, USA) and a 2-tailed p-value <0.05 was taken to indicate statistical significance. Cox proportional hazards regression models were used to generate adjusted hazards ratios.
Results
Out of 60,051 recorded primary THRs that met our inclusion criteria, we found that the revision rate for the 36-mm heads (578 out of 17,412 THRs) was significantly higher than that for the 32-mm heads (1082 out of 42,639 THRs) at 0.649 and 0.534 per 100 component years, respectively (p < 0.001). Subgroup analysis of bearing type showed no significant differences in revision rates across all combinations of 36 mm heads when compared to the 32-mm heads (p = 0.074–0.92), except for metal on metal (MoM); p = 0.038. Ceramic-on-ceramic (CoC) subgroup analysis showed a minimal difference in revision rate per 100 component years between 32-mm heads (0.539) and 36-mm heads (0.544) (p = 0.92, 138 out of 3218 [4.29%] and 225 out of 6618 [3.4%] THRs respectively). All other configurations showed some variation; ceramic-on-polyethylene [CoP] – 0.486 versus 0.606 (p = 0.074, 245 out of 13190 [1.86%] and 131 out of 6137 [2.13%]), MoM – 0.854 versus 1.26 (37 out of 432 [8.56%] and 116 out of 891 [13%]), metal-on-polyethylene [MoP] – 0.542 versus 0.614 (p = 0.505, 662 out of 25,799 [2.57%] and 83 out of 3359 [2.47%]) (Table 2). MoM accounted for 20.1% of the total revisions for 36-mm heads (116 of 578), compared to 3.4% (37 of 432) of 32-mm head revisions (p = 0.038).
Revision rates for head size comparing bearing surface.
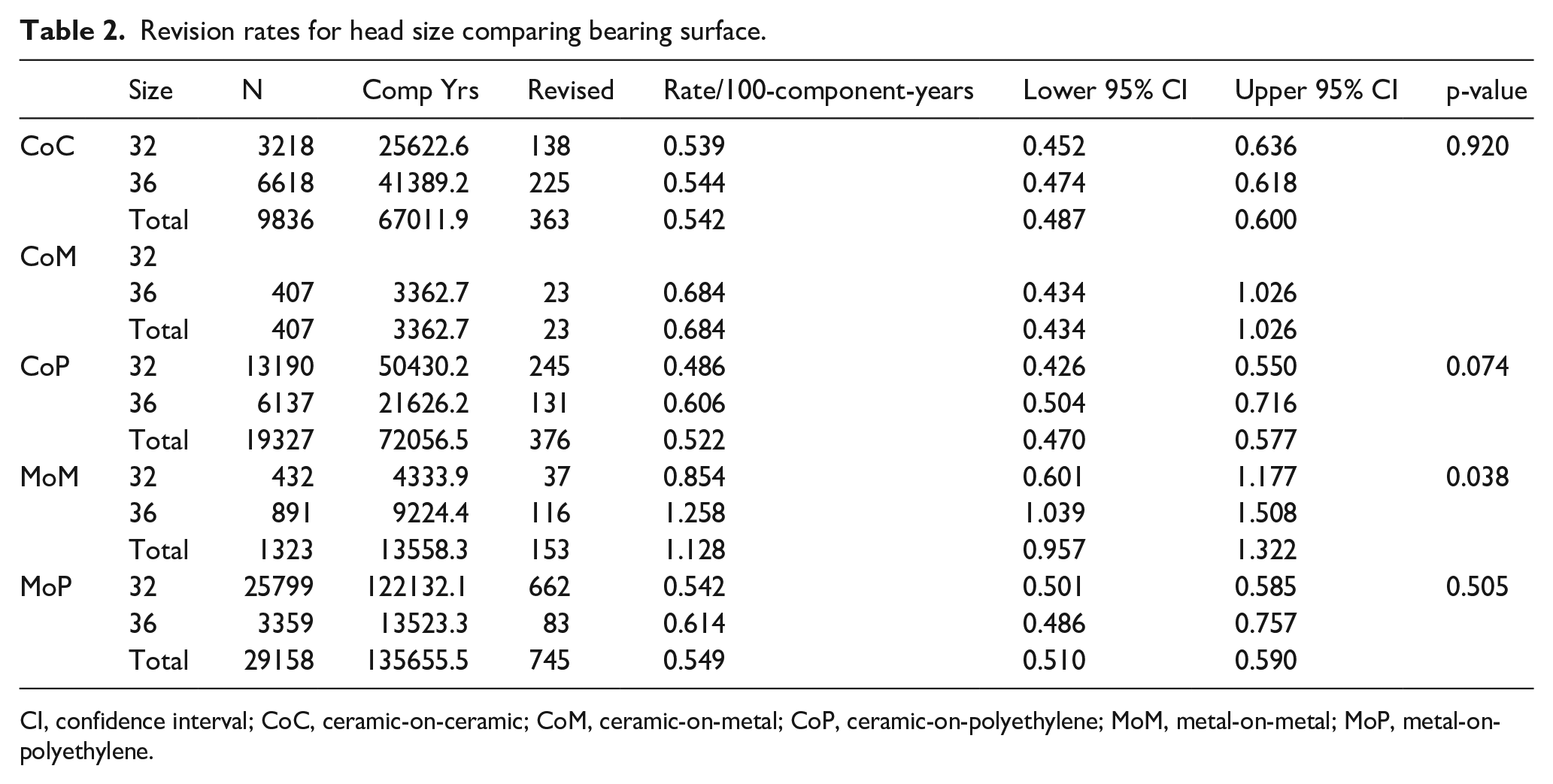
CI, confidence interval; CoC, ceramic-on-ceramic; CoM, ceramic-on-metal; CoP, ceramic-on-polyethylene; MoM, metal-on-metal; MoP, metal-on-polyethylene.
With the above in mind, further analysis was performed with MoM excluded. This showed that there was no significant difference in revision rates per 100 component years between 32-mm (1045 out of 42,207 THRs) and 36-mm heads (462 out of 16,521 THRs), 0.528 versus 0.578 (p = 0.099).
When comparing the reasons for revision, 22.8% of revisions were undertaken for dislocation of 32-mm heads compared to 13.7% for the 36-mm heads. More revisions took place for the indiscriminate cause of ‘pain’ in the 36-mm group at 20.8% compared to 10.5% in the 32-mm group. Loosening accounted for 25.1% of revisions in 32-mm heads and 22.1% in 36-mm heads. Revision for deep infection was 21.5% in the 32-mm head group and 16.3% in the 36-mm head group. Revision for periprosthetic femoral fracture was 18.4% with a 32-mm head and 13.7% with a 36-mm head (Table 3).
Reason for revision comparing head sizes.
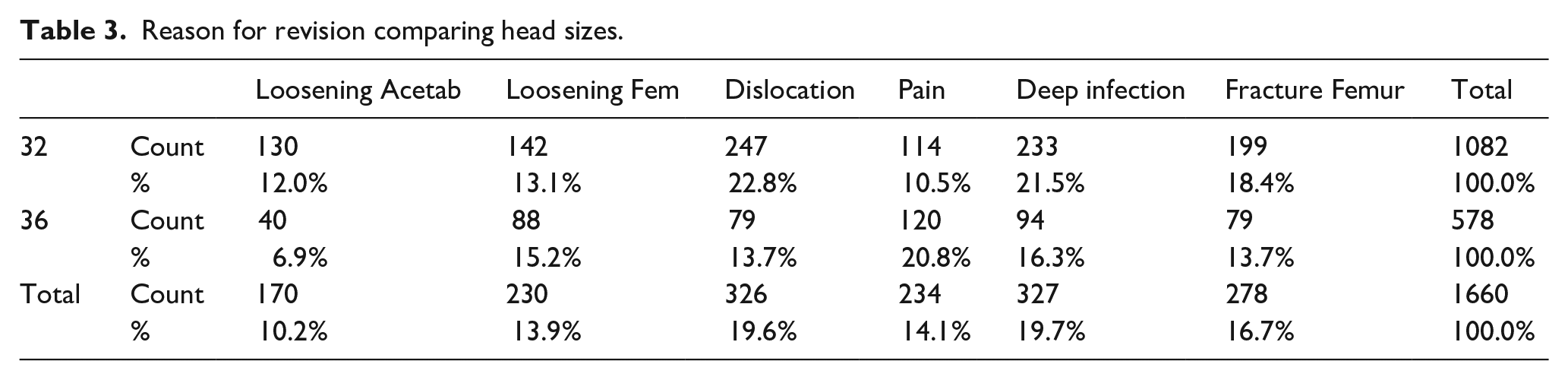
When MoM was removed, the revision percentage for dislocation increased at the same rate in both groups, (23.4% for 32 mm heads and 15.8% for 36 mm heads). Less revisions took place in both groups for the indiscriminate cause of ‘pain’, with a greater decrease in the 36-mm head group (16.5%) than in the 32-mm head group (10.1%).
The median time to revision for those revised was 1.23 years (0.1–4.1 years) in the 32-mm head group and 2.41 years (0.51–5.76 years) in the 36-mm head group. When MoM was removed, there was a proportionally larger decrease in the median time to revision for those revised in the 36-mm head group (1.83 years: 0.21–4.87) than in the 32-mm head group (1.17 years: 0.1–3.85).
The median follow-up in our study was 4.1 years for the 32-mm heads, and 4.55 years for the 36-mm heads with a interquartile rangeof 1.89–7.3 years for both head sizes.
There were considerable differences in the demographics between the two groups (Table 1). The 32-mm head group were older (68.1 years) compared to the 36-mm group (63.6 years) while the 36-mm head group had a higher percentage of women (65% vs. 46%). There were 86 different stems in total, of which the 4 most common accounted for 57.8% of those used (Table 1). Most stems were cemented in the 32-mm group (54.3%), and cementless in the 36-mm group (70.6%). There were 57 different cups, the 4 most common accounting for 58.4% of the total used. Again, there were fewer cemented cups in the 36-mm group (2.4%) than in the 32-mm group (9.4%) (Table 1). The posterior surgical approach was used in 76.5% (30288 of 42639) of the 32-mm head group, and 85.9% (13857 of 17412) of the 36-mm head group. 7
When accounting for age, sex, approach, cementation and polyethylene type (for CoP and MoP surfaces) with MoM removed, there was still no statistically significant difference between the head size groups (Table 4).
Bearing surface hazard’s ratio accounting for age, sex, approach, cementation and polyethylene type.
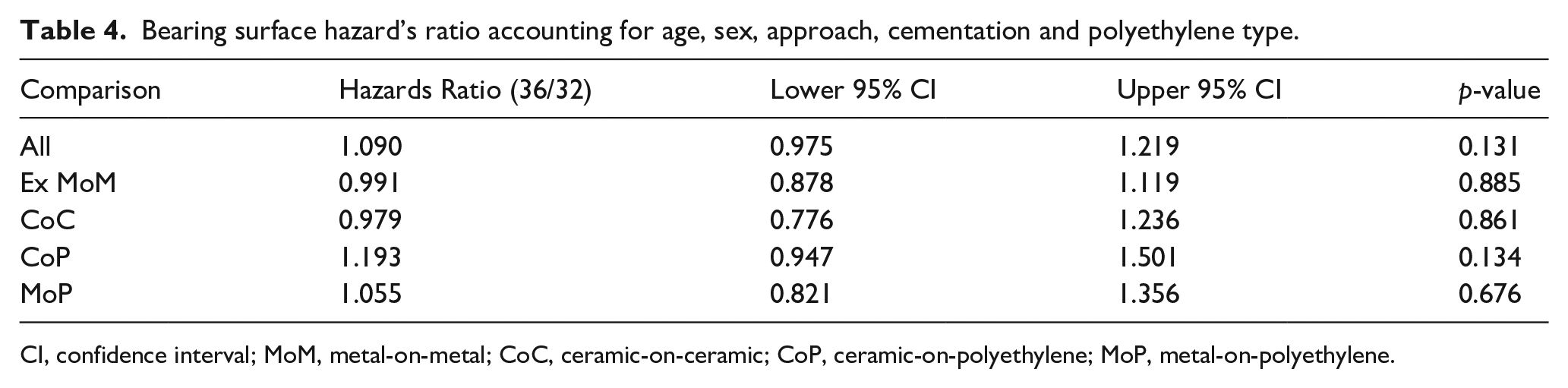
CI, confidence interval; MoM, metal-on-metal; CoC, ceramic-on-ceramic; CoP, ceramic-on-polyethylene; MoP, metal-on-polyethylene.
Discussion
We confirm that increasing the head size from 32 mm to 36 mm is accompanied by no significant increase in revision rate for most combinations of metal, ceramic and polyethylene bearing surfaces. CoP has the lowest revision rate, whilst MoM bearings show a significant increase in revision risk between 32 mm and 36 mm (0.854 vs. 1.26, p = 0.92). When MoM was removed from the overall analysis, there was no significant difference in revision rates per 100 component years between 32-mm and 36-mm heads (0.528 vs. 0.578; p = 0.099).
There is no standard head size in New Zealand. In the early stages of the NZJR, 28-mm heads were the most commonly implanted. With the rising use of more wear-resistant cross-linked polyethylene (XLPE), it became more acceptable to use a larger head to achieve greater stability and their use has been increasing annually. By 2010, more 32- and 36-mm heads were used than 28-mm heads, and the number of 28-mm heads implanted has continued to diminish.
Studies have shown that larger heads confer additional stability.9,10,21,22 More recent studies emphasise the importance of using at least a 32-mm head to further reduce the risk of dislocation.11,23–26 Our results confirm this view: a far higher percentage of revisions for dislocation occurred in the 32-mm group (22.8%) than in the 36-mm group (13.7%). The 2 main concerns with increased head size are bearing wear and taper corrosion which affect the longevity of the replaced joint.17,18 Bearing particles (polyethylene, metal, ceramic) can cause a foreign body reaction which leads to an osteolytic process and eventual implant loosening. 8 Impingement, potential instability and late dislocation can occur with increasing wear as the head moves eccentrically within the liner. We know from in vitro studies that bearing wear with XLPE and vitamin E-diffused XLPE is independent of head size up to 46 mm.27,28 A 13-year report on THR survival from the Australian Registry showed that bearings <32 mm were revised more frequently for dislocation, while bearings >32 mm were revised more frequently for aseptic loosening, a complication that can be associated with wear. 29 Figure 3 shows the proportion of revisions against time since operation comparing 32-mm and 36-mm heads with MoM removed. The proportions remain equally matched until approximately 14 years when the 36-mm group begins to steadily increase and diverge from the 32-mm group. However, this late divergence occurs when the numbers available are small (<400 in each group) so may not represent a genuine difference between the size groups. It would be interesting to repeat this study in several years’ time to see whether this late difference in revision rates persists as a robust statistically significant difference between the two size groups. During the time period studied, the graph did not significantly change when standard polyethylene was removed.
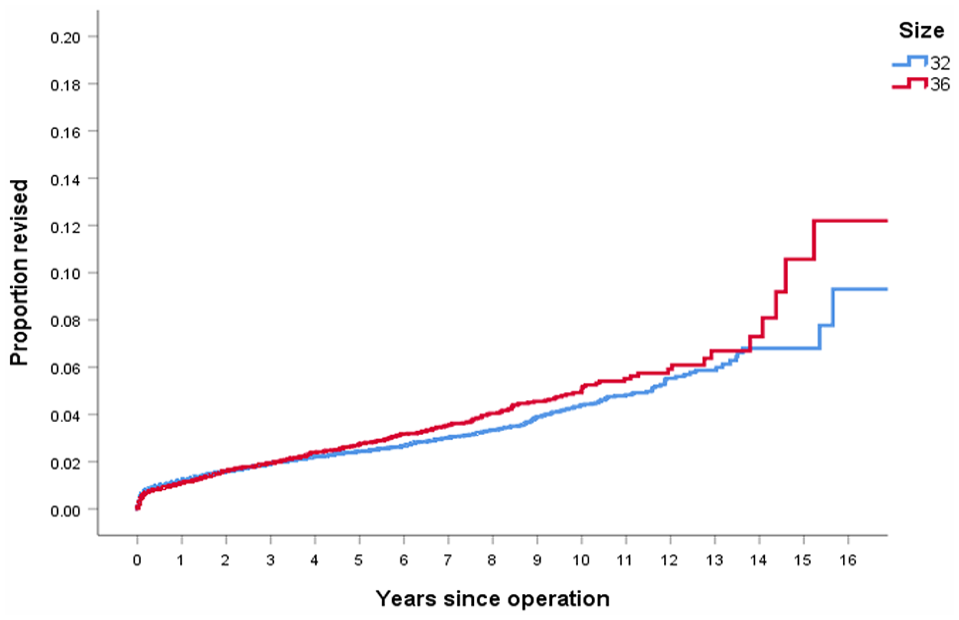
Proportion of revisions with time since operation comparing 32-mm and 36-mm heads with MoM removed.
Ceramic bearings are well known to have lower revision rates30–32 and this supports our findings. Our CoC subgroup analysis showed a minimal difference in revision rates per 100 component years between 32- and 36-mm heads (0.539 compared to 0.544; p = 0.92) compared to all other configurations. A further concern with larger heads in CoC bearings is fracture. 33 The Australian registry found a higher 13-year survival rate for 36 mm or larger CoC bearings compared with 32 mm or smaller bearings. 29 A recent study using data from the NZJR compared bearing material and risk of revision for ‘late’ dislocation (dislocation > 1 year postoperatively). 34 The unadjusted hazard ratios showed a significantly higher rate of revision for ‘late’ dislocation in CoP (HR 2.48; p = 0.001) and MP (HR 2.00; 95% p = 0.007) compared to CoC. When adjusted for head size, age and surgical approach, only CP (HR 2.10; p = 0.021) maintained a significantly higher rate of revision. Low wear and less debris, limited peri-articular inflammatory reaction and a healthy fibrotic pseudo-capsule were determined as potential factors affecting long-term stability of the hip joint.
We acknowledge that ‘pain’ is a broad term used as an indication for revision, 1 of the flaws of an observational registry study. However, there was a large difference between the 2 groups with ‘pain’ accounting for 20.8% of revisions in the 36-mm group and 10.5% in 32-mm group (with MoM included). Taper corrosion and fretting (‘trunnionosis’) at the head-neck junction may be 1 potential cause. This has caused increasing concern in recent years and is well known to occur in MoM configurations and to a lesser extent in MoP.18,35–38 Large heads, especially when combined with small taper dimensions, have been associated with trunnionosis which is thought to be the result of increased torque around the taper interface during activity.39–41 A more recent paper, 42 which studied a range of head sizes (22–44 mm) and taper designs in MoP hips, has questioned this theory and concluded that head size does not affect fretting or corrosion. This topic is still the subject of debate in the literature. It could also be associated with specific small taper designs, a difference in head and trunnion alloys and length of implantation.43,44 Other studies have shown associations between large heads and anterior impingement causing groin pain.45–48
In contrast to our results, a Nordic registry study by Tsikandylakis et al. 19 found that in the MoP group the risk of revision was significantly higher for patients with a 36-mm head (HR 1.14; 95% CI, 1.04–1.26; p = 0.007) than for those with a 32-mm head. They also found no difference in the rates of revision for dislocation between patients with a 36-mm head (HR 0.85; 95% CI, 0.70–1.02; p = 0.086) and those with a 32-mm head when adjustments were made for potential confounding variables such as age, sex, year of surgery, surgical approach, implant fixation, and type of polyethylene. 19 Another recent study, from the Dutch Arthroplasty Register, showed that there was a lower 6-year cumulative revision rate for any reason with 32-mm heads (other than MoM) than for both 22- to 28-mm (combined as 1 group) and 36-mm heads. 13
A limitation of this is study is that as a nonrandomised observational study, residual confounding may still be present. The traditional approach for patients at high risk of dislocation, such as those with alcoholism or early cognitive impairment, is to use a larger femoral head. These patients are not only at higher risk of dislocation but of all-cause revision, especially infection, and therefore the higher revision rates with 36-mm heads may in part have been caused by selection bias. For example, sicker patients with poorer bone quality may have had a larger head implanted in an attempt to reduce the risk of dislocation, while acknowledging that the threshold for revising such patients is generally high. Similarly, younger and more active patients may also have had larger heads implanted to allow a wider range of hip motion and a lower risk of dislocation but be at higher risk for revision for aseptic loosening as they live longer. Our demographics are in keeping with this concept in that the median age for patients having a 36-mm head was considerably less (63.65 years) than that of patients with a 32-mm head (68.12 years). Our demographics also show that those with a 32-mm head had a higher percentage of cemented cups and stems (9.4% vs. 2.4% and 54.3% vs. 29.4% respectively), which may have contributed to a higher threshold for revision in this group of patients than in the younger, uncemented 36-mm group. In the registry data, only revision due to dislocation was recorded but not the true dislocation rate (closed reduction without revision). It would be interesting to know the true figure as there may be more hidden dislocations in the older 32-mm group which ultimately did not undergo revision because of a higher threshold for revision.
Previous reports have shown that variables such as age, sex, year of surgery, surgeon experience, surgical approach, fixation type, BMI, patient comorbidities and polyethylene type affect the risk of revision, and could therefore affect the surgeon’s choice of head diameter.14,24,49 In our study, Cox proportional hazards regression models were used to generate adjusted hazards ratios. When accounting for age, sex, approach, cementation and polyethylene type (for CoP and MoP surfaces) with MoM removed, there is still no statistically significant difference between the head size groups (Table 4). We were unable to account for BMI and surgeon experience as this has only been measured more recently by the New Zealand Registry. Information about comorbidities that could influence the risk of dislocation or any other cause of revision is not available from the NZJR. Therefore, due to the inherent nature of registry studies, a true causal relationship between head size and the risk of THR revision resulting from dislocation and all other causes cannot fully be established from our data. They can, however, constitute a sound basis for the generation of hypotheses, which might stimulate further research in better-controlled studies.
Conclusion
We conducted a large registry study and were able to show there is no significant increase in the rate of revision between 32- and 36-mm heads when MoM hips are excluded. Our findings support the use of 36 mm rather than 32 mm heads when surgeons base their choice of head size on the anticipated risk of dislocation. Because of inherent limitations in registry-based studies, further studies with longer follow-up and improved control for confounders are needed to further investigate the importance of head size in THR. However, based on the findings in this registry study, we would encourage surgeons to favour 36-mm heads in routine THR, because they appear to provide the best compromise between stability and overall implant survival.
Footnotes
Acknowledgements
We thank Chris M Frampton and the NZ registry for their paid assistance in compiling the statistics.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.