
Abstract
Purpose:
The aim of the study was to determine the restoration of hip biomechanics through lateral offset, leg length, and acetabular component position when comparing non-arthroplasty surgeons (NAS) to elective arthroplasty surgeons (EAS).
Methods:
131 patients, with a femoral neck fracture treated with a THA by 7 EAS and 20 NAS, were retrospectively reviewed. 2 blinded observers measured leg-length discrepancy, femoral offset, and acetabular component position. Multivariate logistic regression models examined the association between the surgeon groups and restoration of lateral femoral, acetabular offset, leg length discrepancy, acetabular anteversion, acetabular position, and component size, while adjusting for surgical approach and spinal pathology.
Results:
NAS under-restored 4.8 mm of lateral femoral offset (43.9 ± 8.7 mm) after THA when compared to the uninjured side (48.7 ± 7.1 mm, p = 0.044). NAS were at risk for under-restoring lateral femoral offset when compared to EAS (p = 0.040). There was no association between lateral acetabular offset, leg length, acetabular position, or component size and surgeon type.
Conclusions:
Lateral femoral offset is at risk for under-restoration after THA for femoral neck fractures, when performed by surgeons that do not regularly perform elective THA. This indicates that lateral femoral offset is an under-appreciated contributor to hip instability when performing THA for a femoral neck fracture. Lateral femoral offset deserves as much attention and awareness as acetabular component position since a secondary analysis of our data reveal that preoperative templating and intraoperative imaging did not prevent under-restoration.
Introduction
More than 1.7 million femoral neck fractures occur each year worldwide. 1 By 2050, femoral neck fractures will increase more than 300% in men and 240% in women paralleling the rapid increase in the prevalence of osteoporosis, 2 resulting in a 2.3-fold increase in the number of hip fractures over the next 3 decades. 3 Although the treatment algorithm for femoral neck fractures has improved, as indicated by the improvement in postoperative complications, 4 mortality still approaches 30% within the first year placing a premium on early mobility and reducing reoperation after femoral neck fracture. 5
Hemiarthroplasty is frequently used to treat a femoral neck fracture. Reconstructing only the femoral side avoids the additional stress of acetabular component positioning during total hip arthroplasty (THA). With a low hemiarthroplasty to a THA conversion rate (0.1%), many surgeons elect for a more straightforward hemiarthroplasty. 6 This is despite evidence that suggests THA for a femoral neck fractures may be a better option when compared to hemiarthroplasty or internal fixation. THA offers less long-term pain, higher outcome scores, and a lower reoperation rate.7–11 The National Institutes for Health and Care Excellence (NICE) guidelines suggest femoral neck fractures be treated with THA if the patient can walk independently with no more than a cane, is cognitively intact, and medically fit for anaesthesia. 12 Although the use of THA has increased over the past 20 years, this increase is slower than expected. 13 The use of THA increased from 6% in 1999 to 7% in 2011 in all femoral neck fractures while hemiarthroplasty increased from 62% in 1999 to 64% in 2011. Bishop et al. demonstrated surgeons with fellowship training in arthroplasty performed a higher percentage of THAs for a femoral neck fracture, increasing from 4% in 1999 to 21% in 2011. Miller et al. 14 validated these therapeutic trends, showing the increase in arthroplasty utilisation for a femoral neck fracture was predominantly hemiarthroplasty utilisation. 88% of surgeons said they performed THA for femoral neck fractures, but only 13% of these same surgeons preferred THA compared to 85% who preferred hemiarthroplasty. 15
For optimal function, restoration of the hip biomechanics is imperative during THA. Lateral offset, leg length, and acetabular component position are critical for obtaining a stable hip.16–19 Even though THA in the right patient population performs well after a femoral neck fracture, it has a higher incidence of instability when compared to hemiarthroplasty.7,20,21 Historically, acetabular component positioning was the focus of hip stability, since it represent the major difference between THA and hemiarthroplasty, explaining the prevalence of hemiarthroplasty after a femoral neck fracture.16,18 Recent data also supports incomplete restoration of lateral femoral offset as a major predictor of hip instability. 22 The objective of this study was to determine restoration of hip biomechanics comparing surgeons that do not regularly perform elective THA (non-arthroplasty surgeons [NAS]) to surgeons that regularly perform elective THA (elective arthroplasty surgeons [EAS]). We hypothesised NAS restore lateral femoral offset below the minimally clinical important difference (MCID) after a THA for a femoral neck fracture more frequently than EAS. We also conducted exploratory analyses of the differences in lateral acetabular offset, relative leg length discrepancy, acetabular component size, or femoral head size while controlling for patient characteristics, surgical approach, and the prevalence of spinal pathology.
Material and methods
The Internal Review Board at our institution hospital approved the retrospective study. Inclusion criteria for the study included patients with femoral neck fractures treated with a THA, 1 unoperated and 1 operated hip and treated at Stanford Medicine between January 2009 and April 2018. Patients with radiographical undefinable acetabular landmarks (e.g., acetabular teardrop), a previously arthritic hip (e.g., decreased joint space), contralateral hip surgery, or with unavailable postoperative radiographs were excluded from the study. Based upon the above stated criteria, 131 patients were retrospectively reviewed. The mean age was 71.9 ± 10.5 years and 63% (82 THAs) were performed in females (Table 1). Surgeons were divided into 2 groups: surgeons who performed 50 or more elective THA procedures per year (EAS = 7) and surgeons who performed no elective THA procedures and only performed non-elective THA while on-call for femoral neck fractures (NAS = 20). 15
Patient characteristics of total hip arthroplasty performed for a femoral neck fracture by elective and non-elective arthroplasty surgeons.
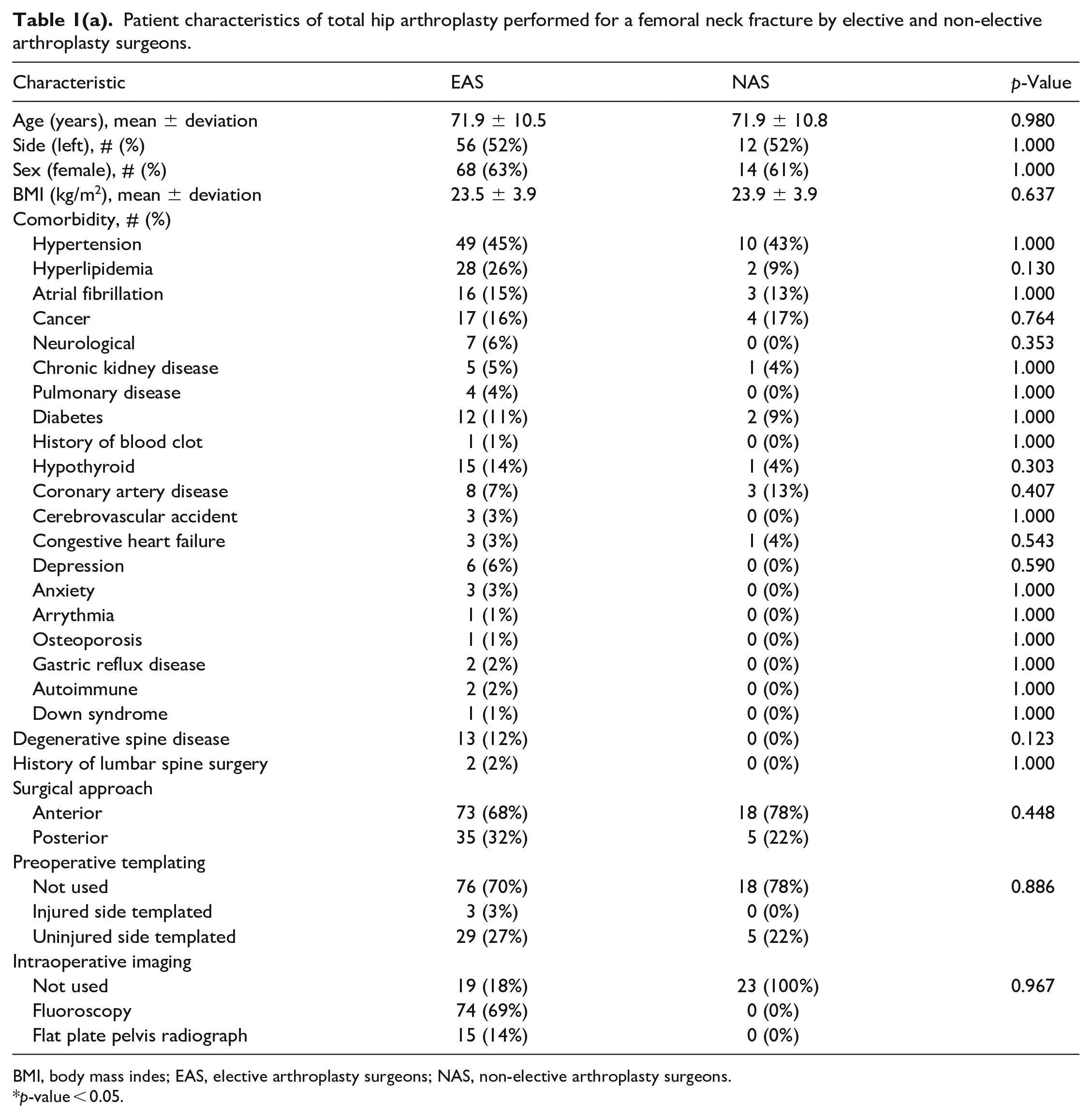
BMI, body mass indes; EAS, elective arthroplasty surgeons; NAS, non-elective arthroplasty surgeons.
p-value < 0.05.
Implants used during total hip arthroplasty for a femoral neck fracture.
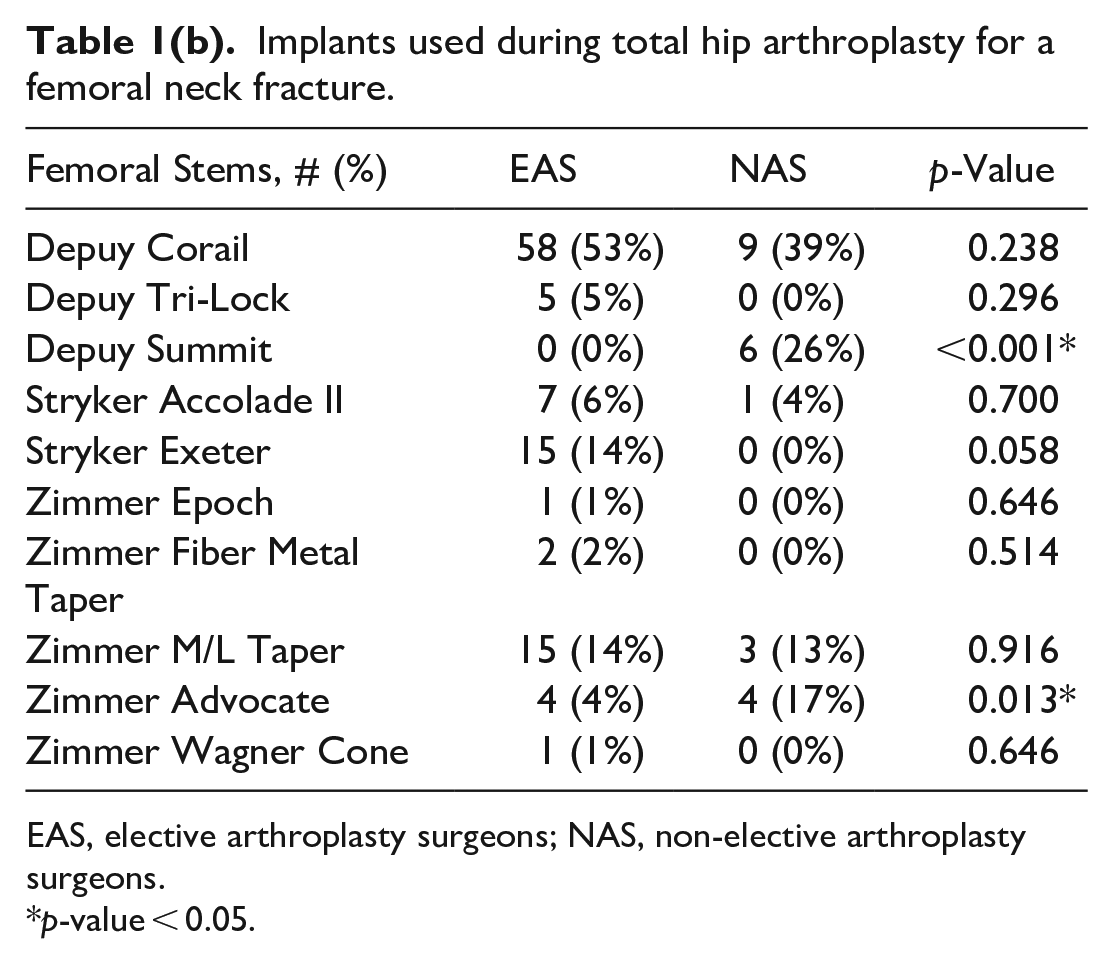
EAS, elective arthroplasty surgeons; NAS, non-elective arthroplasty surgeons.
p-value < 0.05.
All patients had a pre- and postoperative AP radiograph of the pelvis with definable anatomic landmarks needed for attaining appropriate measurements. All radiographs were obtained at Stanford Medicine on equivalent x-ray machines (GE Healthcare, DefiniumTM 656 HD x-ray system). All radiographs were taken with a standard 25 nm magnification marker. 2 blinded observers (HNS and AAB) measured lateral femoral offset, lateral acetabular offset, and relative leg length at 2 intervals at least 2 weeks apart for the uninjured and reconstructed side using the pre- and postoperative anteroposterior (AP) radiograph of the pelvis for all patients (Figure 1). To estimate intra- and inter-rater reliability, intraclass correlation coefficients using two-way random effects model for consistency and average were calculated for all measures. All intraclass correlation coefficients were excellent, ranging from 0.95 to 0.99, for all radiographic measurement collected. 23 The Martell hip analysis suite (Chicago, IL) was used to measure acetabular inclination and anteversion. 24 The Martell method has a previously published excellent intra-observer agreement.25,26 Lateral femoral offset was defined as the perpendicular distance from the ceneer of the femoral head to a line marking the centre of the intermedullary femoral canal (Figure 1). 27 Lateral acetabular offset was defined as the perpendicular distance from the centre of the femoral head to the ilioischial line.28,29 Total femoral offset was defined as the sum of lateral femoral and acetabular offsets. Relative leg length was defined as the difference in distance from the most prominent feature of the lesser trochanter to the inter-teardrop line between the uninjured and injured sides (Figure 1). 30 The presence of degenerative spine disease or prior lumbar spine instrumentation, the surgical approach (e.g., anterior or posterior), the use of preoperative templating, intraoperative fluoroscopy, or flat plate radiography (Table 1(a)), choice of femoral stem (Table 1(b)), acetabular component size, and femoral head size were documented as well (Figure 2).
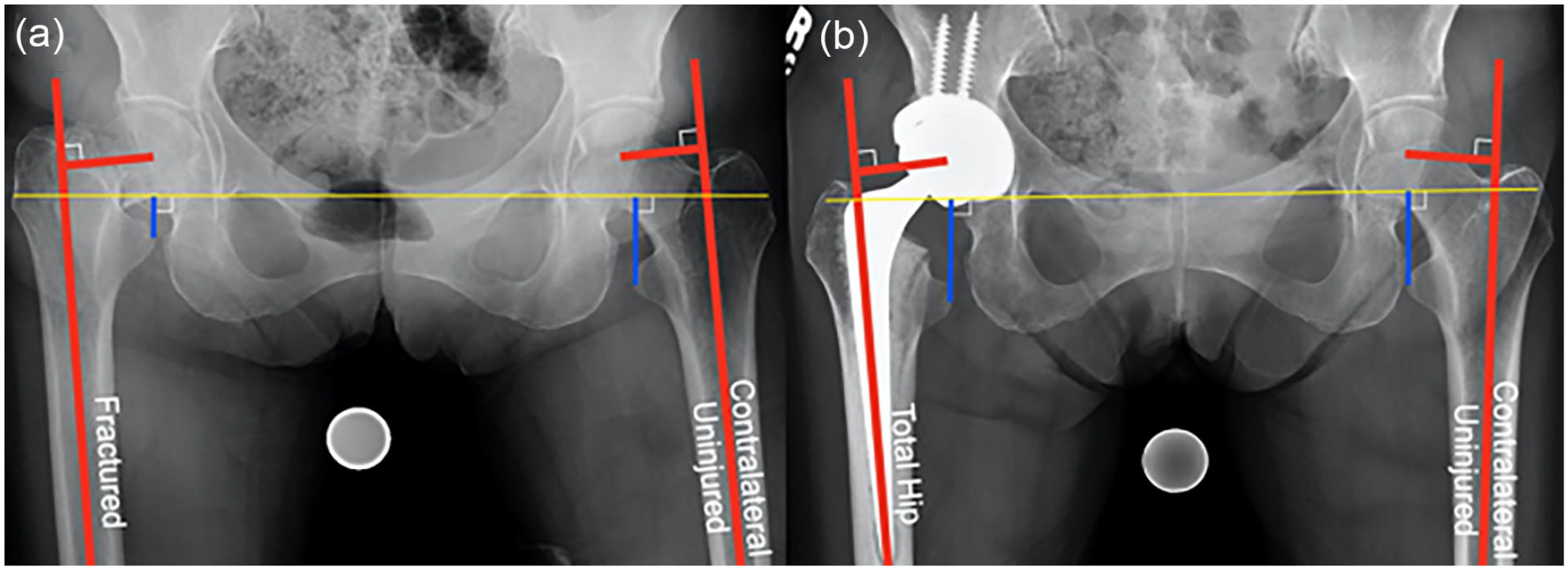
Radiographic images of lateral femoral offset and relative leg length measurements: (a) on the injury AP pelvis view and (b) reconstructed AP pelvis view, lateral femoral offset was defined as the perpendicular distance from the centre of the femoral head to a line marking the centre of the intermedullary femoral canal; relative leg length was defined as the difference in distance from the most prominent feature of the lesser trochanter to the inter-teardrop line.
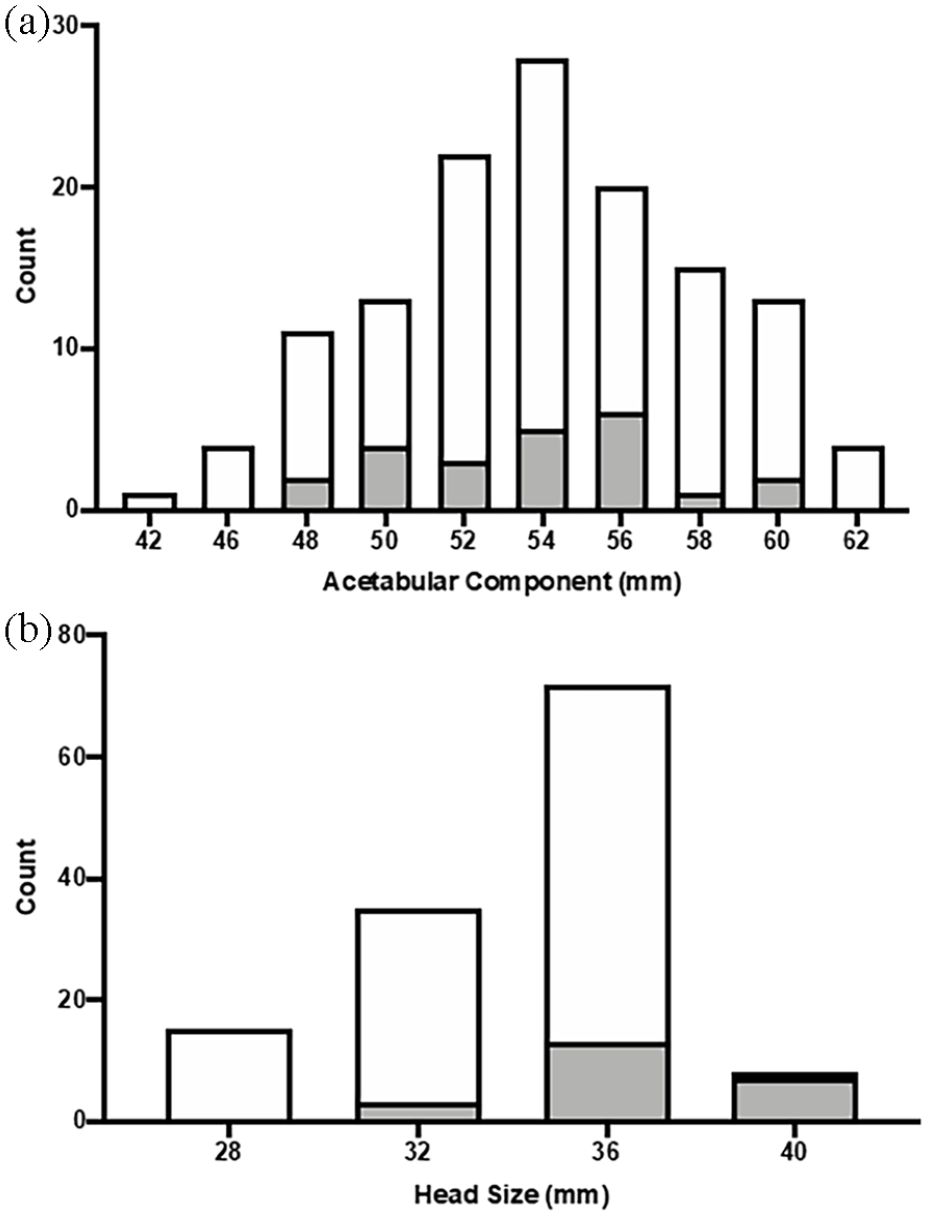
Histograms of acetabular component and femoral head sizes used during total hip arthroplasty for femoral neck fracture: (a) there was no statistically significant difference in the mean acetabular component size (54.1 ± 4.2 mm; mode: 54 mm for EAS (white) and NAS (grey, 53.7 ± 3.4 mm, mode: 56 mm, p = 0.669) and (b) the mean femoral head size as 33.9 ± 3.7 mm (mode: 36 mm) for EAS (white) this was smaller than the 36.7 ± 2.6 (mode: 36 mm) for NAS (grey, p < 0.001).
Statistical analysis
Data were analysed using R version 3.6.3 (Vienna, Austria) and Rstudio version 1.2.5001 (Boston, MA). Continuous variables are presented as the mean with standard deviation and compared using a Student’s t-test. Categorical variables are presented as the frequency with percent and compared using a Fisher exact or chi-square test where appropriate. The primary outcome was restoration of lateral femoral offset using established minimal clinical important difference (MCID) for lateral femoral offset within −3 mm of the uninjured side by calculating the differences in the lateral femoral offset of the THA and uninjured sides on the postoperative AP pelvis radiograph. 31 A difference ⩽ −3 mm was considered unrestored (range −22.6 to −3.0 mm) and a difference > −3 mm was considered restored (range −2.9–14.3 mm). 32 Multivariate logistic regression was used to evaluate lateral femoral offset with respect to surgeon experience with THA (e.g., EAS or NAS), adjusting for surgical approach, presence of degenerative spine disease, or prior lumbar spine instrumentation (Table 1). Differences were also calculated for lateral acetabular offset (MCID > −3 mm), 33 relative leg length (MCID > −5 mm), 32 acetabular component anteversion (MCID between 5–25°), 16 acetabular component inclination (MCID between 35–55°), 16 acetabular component size (MCID between 51 and 57 mm), 34 and femoral head size (MCID ⩾ 32 mm).35,36 Exploratory multivariate logistic regression models were used to evaluate these reconstructive variables as well to examine the effect of surgeon experience with THA, adjusting for surgical approach, presence of degenerative spine disease, or prior lumbar spine instrumentation (Table 1). A power analysis indicated there was 80% power with an alpha error of 5% to detect an effect size of 0.7 mm for using these measurements of a THA on the postoperative AP pelvis radiograph to examine surgeon experience.
Results
When evaluating acetabular component position after THA for a femoral neck fracture, the mean acetabular component inclination was 41.3° ± 6.6° and anteversion was 16.5° ± 5.5°. There was no statistical difference in mean acetabular component inclination for EAS (41.7° ± 6.3°) and NAS (39.3° ± 7.9°; p = 0.274). There was also no statistical difference in mean acetabular component anteversion for EAS (16.9 ± 5.3°) and NAS (14.2 ± 6.3°, p = 0.118). There was no difference in the frequency of acetabular components placed outside the safe zone between EAS (16, 15%) and NAS (5, 22%, p = 0.399) (Figure 3). 16
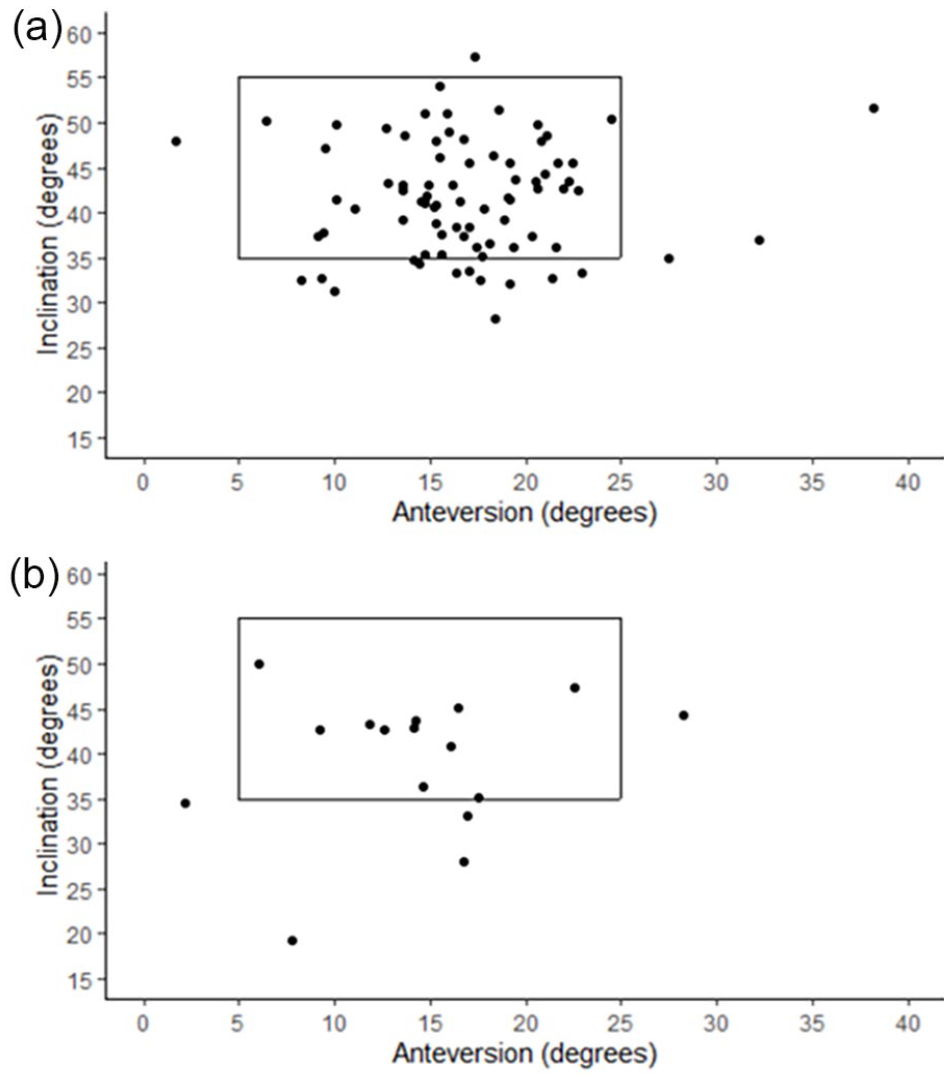
The acetabular component with Lewinnek safe zone. Graph of the inclination and anteversion of each acetabular component (dot) placed by a (a) non-elective arthroplasty surgeon or (b) elective arthroplasty surgeon with a box indicating the boundaries of the Lewinnek et al. 16 safe zone.
When evaluating femoral component position, NAS under-restored 4.8 mm of lateral femoral offset after THA (43.9 ± 8.7 mm) compared to the uninjured side (48.7 ± 7.1 mm, p = 0.044) (Table 2). EAS and NAS adequately restored lateral acetabular offset and relative leg length after THA (Table 2). A multivariate regression for lateral femoral offset after THA for a femoral neck fracture found lateral femoral offset was restored to within −3 mm of the uninjured side 63% of the time by EAS but only 39% of the time by NAS (p = 0.040) (Table 3). EAS had over double the odds (odds ratio [OR] 2.67; 95% confidence interval (CI), 1.06–7.01; p = 0.040) of restoring lateral femoral offset when compared to NAS after adjusting for surgical approach, spine diagnosis, and history of spine surgery. Multivariate regressions did not find any other reconstructive differences in acetabular offset, leg length discrepancy, acetabular component position, or component choice between the EAS and NAS (Table 3).
Femoral component position after a total hip arthroplasty for a femoral neck fracture based on surgeon.
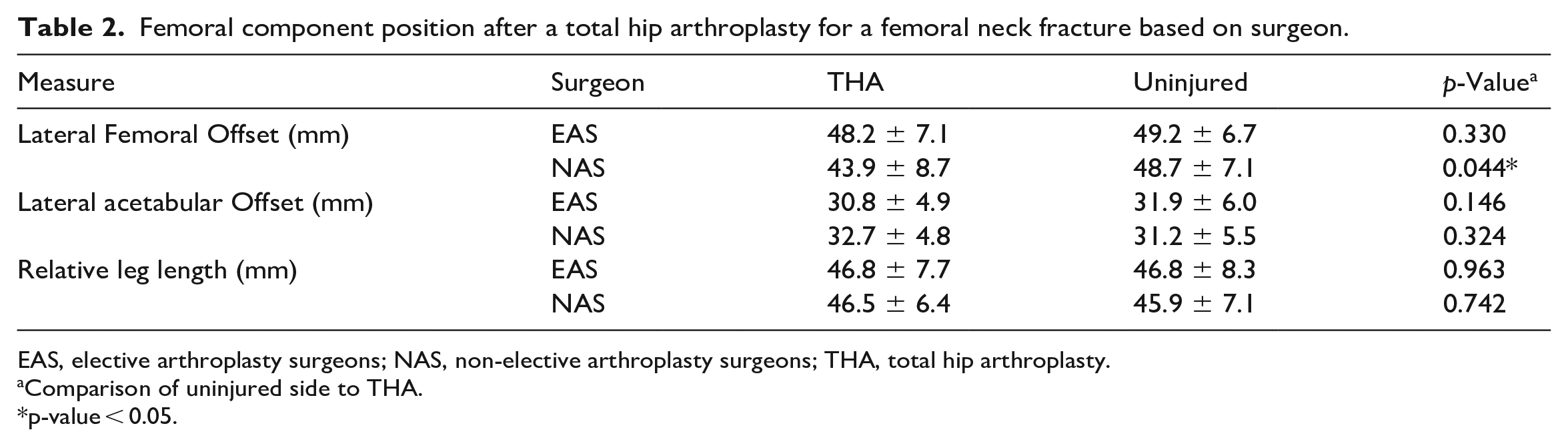
EAS, elective arthroplasty surgeons; NAS, non-elective arthroplasty surgeons; THA, total hip arthroplasty.
Comparison of uninjured side to THA.
p-value < 0.05.
Multivariate logistic regression of hip restoration after a total hip arthroplasty for a femoral neck fracture based on surgeon.
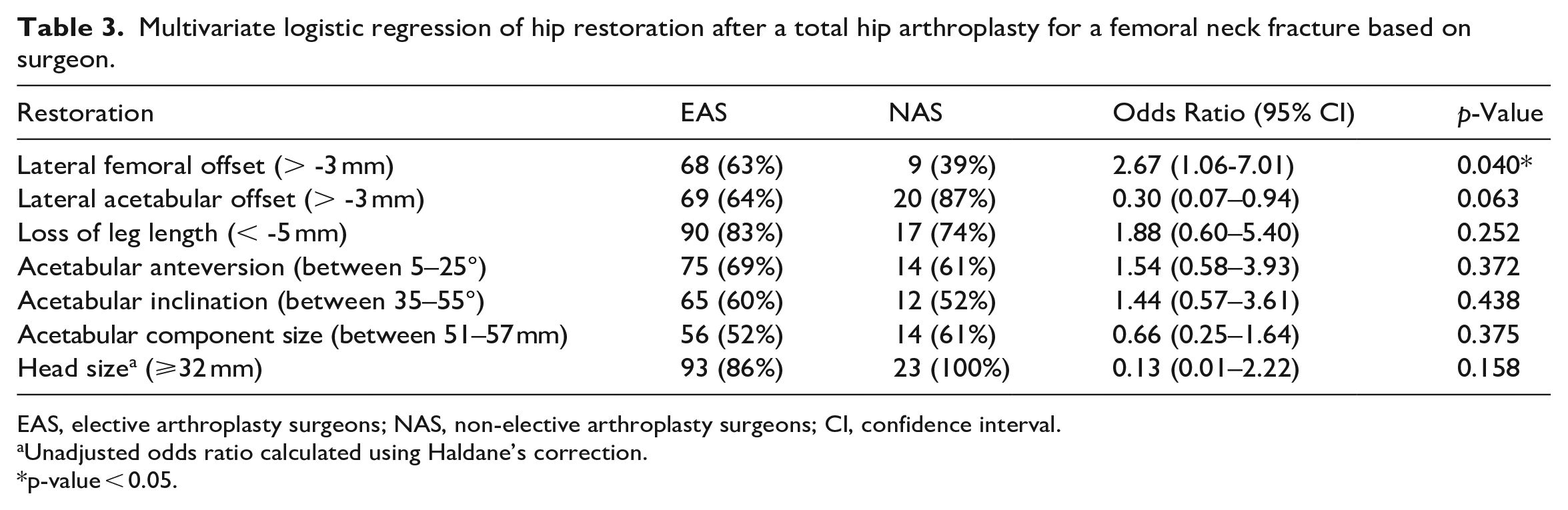
EAS, elective arthroplasty surgeons; NAS, non-elective arthroplasty surgeons; CI, confidence interval.
Unadjusted odds ratio calculated using Haldane’s correction.
p-value < 0.05.
Effect of preoperative templating
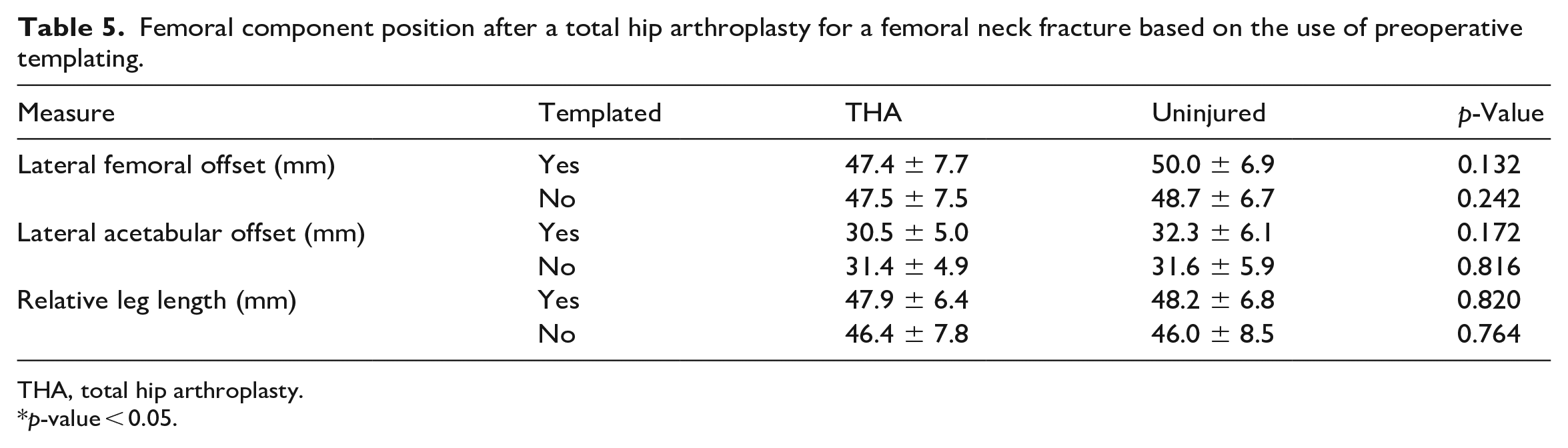
37 THAs were performed after preoperative templating (28%), and 94 THAs were performed without preoperative templating (72%). There was no difference in restoration of lateral femoral offset with the use of preoperative templating prior to a THA for a femoral neck fracture (OR 1.23; CI, 0.57–2.74; p = 0.606), after adjusting for surgical approach, presence of degenerative spine disease, or prior lumbar spine instrumentation (Table 4). There was no difference in the mean lateral femoral offset after a THA with templating (47.4 ± 7.7 mm) when compared to the uninjured side (50.0 ± 6.9 mm; p = 0.132) or without templating (47.5 ± 7.5 mm) when compared to the uninjured side (48.7 ± 6.7 mm; p = 0.242) (Table 5).
Multivariate logistic regression of hip restoration after a total hip arthroplasty for a femoral neck fracture based on the use of preoperative templating.
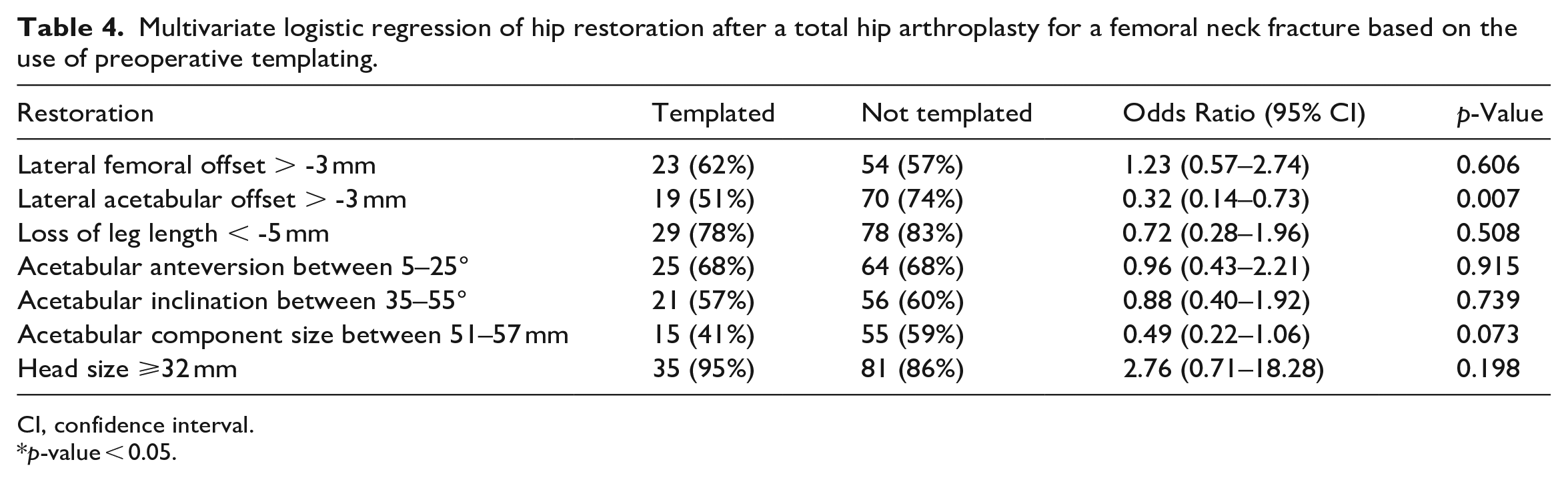
CI, confidence interval.
p-value < 0.05.
Femoral component position after a total hip arthroplasty for a femoral neck fracture based on the use of preoperative templating.
THA, total hip arthroplasty.
p-value < 0.05.
Effect of intraoperative imaging
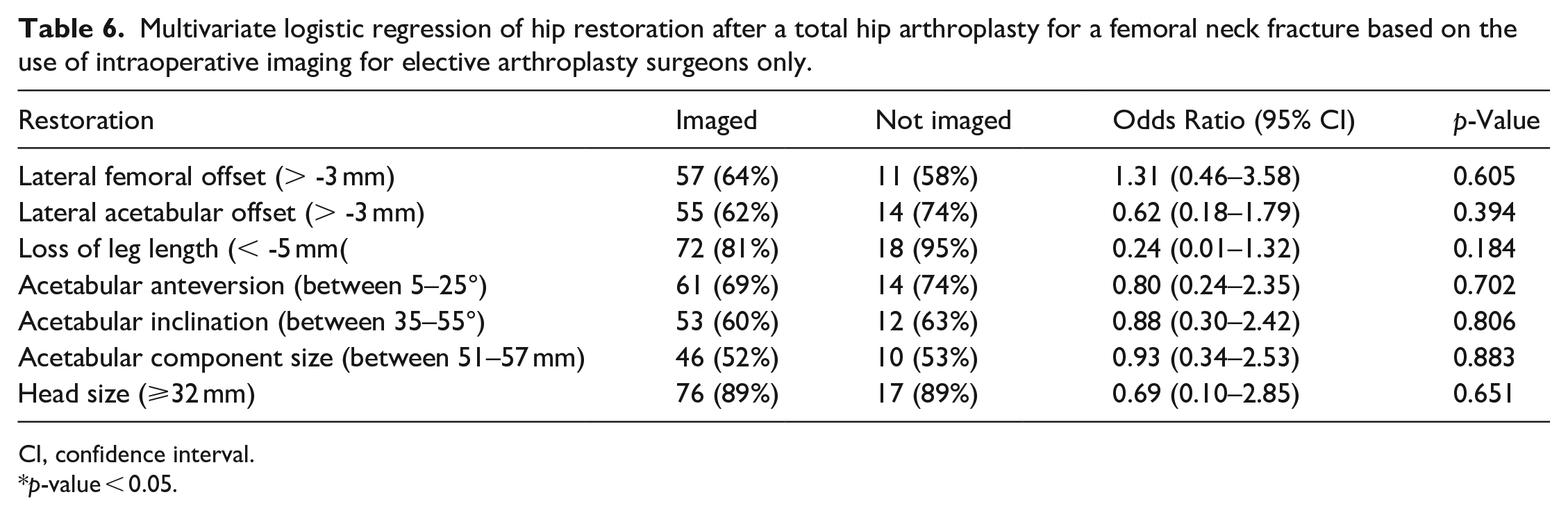
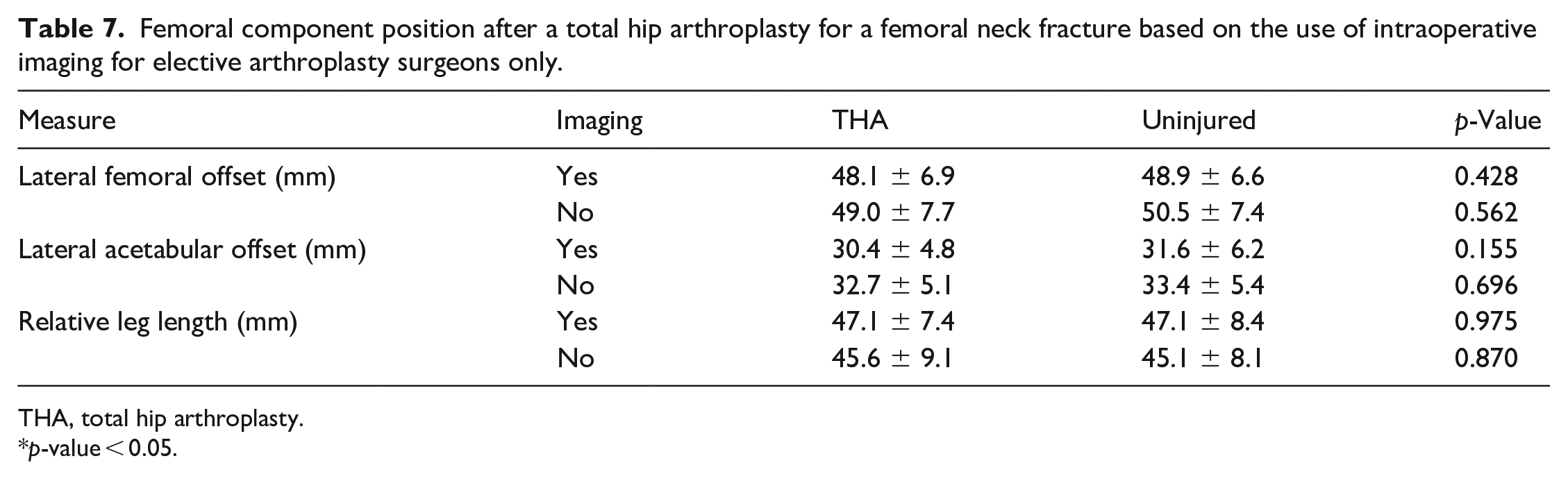
Of the 108 EAS cases, 89 (82%) THAs were performed with intraoperative imaging, and 19 (18%) THAs were performed without intraoperative imaging. There were no NAS cases that were performed with intraoperative imaging. There was no difference in lateral femoral offset restoration between the imaged and unimaged groups (Table 6). There was no difference in the mean lateral femoral offset after a THA with intraoperative imaging (48.1 ± 6.9 mm) when compared to the uninjured side (48.9 ± 6.6 mm; p = 0.428) or without intraoperative imaging (49.0 ± 7.7 mm) when compared to the uninjured side (50.5 ± 7.4 mm; p = 0.562) (Table 7).
Multivariate logistic regression of hip restoration after a total hip arthroplasty for a femoral neck fracture based on the use of intraoperative imaging for elective arthroplasty surgeons only.
CI, confidence interval.
p-value < 0.05.
Femoral component position after a total hip arthroplasty for a femoral neck fracture based on the use of intraoperative imaging for elective arthroplasty surgeons only.
THA, total hip arthroplasty.
p-value < 0.05.
Instability
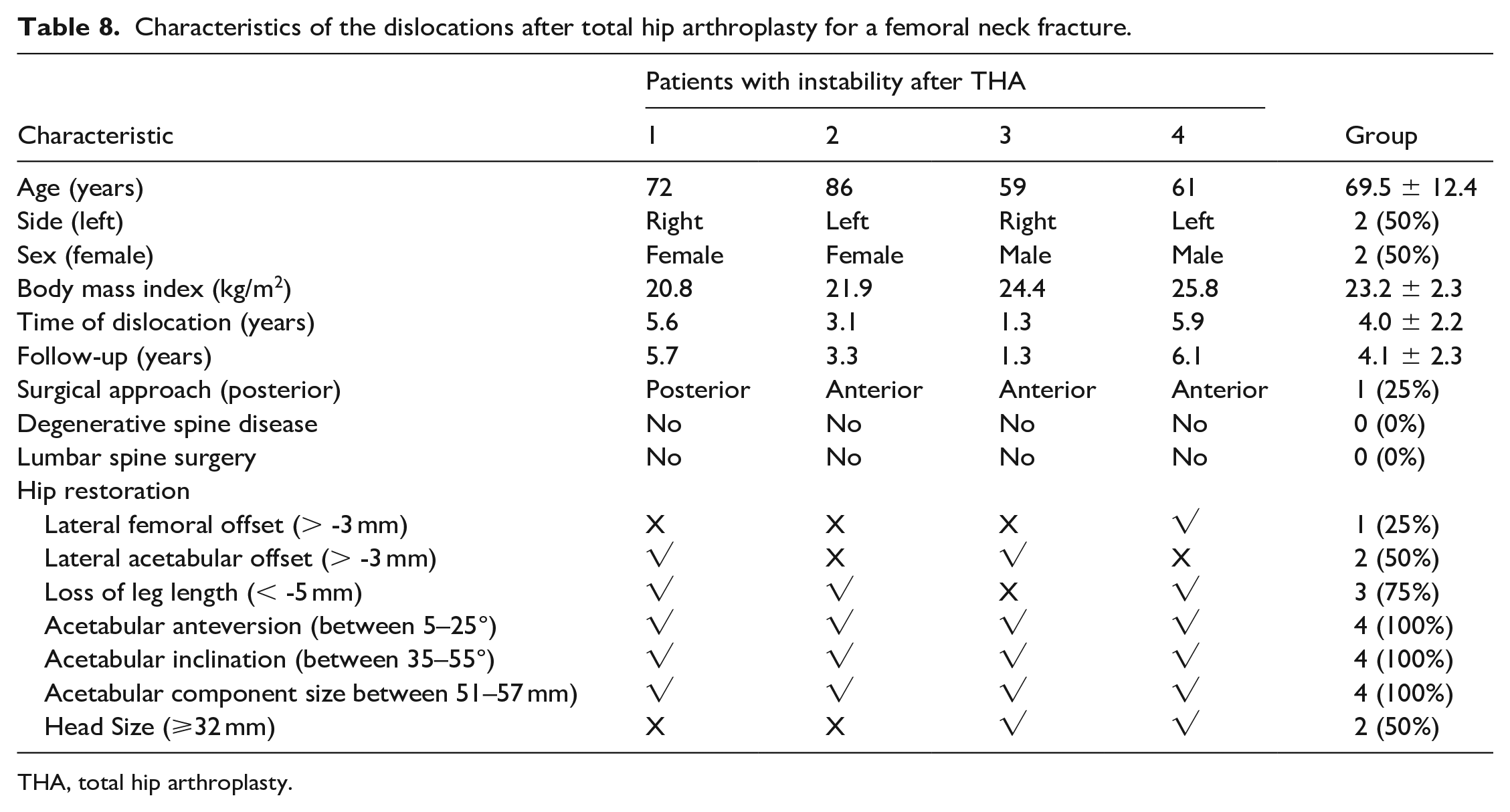
There were 4 dislocations after THA for a femoral neck fracture in this cohort (3%) – 3 after an anterior approach (75%) and 1 after a posterior approach (25%) – with a mean follow-up of 4.1 ± 2.2 years and a mean time to dislocation of 4.0 ± 2.2 years (Table 8). The mean lateral femoral offset of a dislocation was 47.6 ± 8.0 mm after THA and 51.8 ± 6.7 mm on the uninjured side (p = 0.449), while the mean did not reach significance 3 (75%) dislocations had an under-restored lateral femoral offset. The mean lateral acetabular offset was 32.5 ± 6.6 mm after THA and 35.8 ± 3.1 mm on the uninjured side (p = 0.411), with 2 (50%) dislocations having an under-restored lateral acetabular offset. Relative leg length was 47.3 ± 6.5 mm after THA and 47.4 ± 8.3 mm on the uninjured side (p = 0.994), with 1 (25%) dislocation having an under-restored leg length. The mean inclination was 36.5° ± 1.9°, and the mean anteversion was 17.1° ± 2.3°. It should be noted all the dislocations had the acetabular component positioned within the safe zone (Table 8). 16
Characteristics of the dislocations after total hip arthroplasty for a femoral neck fracture.
THA, total hip arthroplasty.
Discussion
Hip fractures are a worldwide health concern with 1-year mortality rates still as high as 30%.3–5 The utilisation of THA to treat a femoral neck fracture remains uncommon despite successful results.13–15 The appropriate placement of components while balancing soft tissues to restore hip biomechanics is an important factor in preventing hip instability after THA.16,32–35,37–39 We demonstrate that anecdotal concerns that acetabular component positioning may place NAS at risk for hip instability are likely unwarranted, since both EAS and NAS surgeons were able to place the acetabular component in an acceptable position. The exact role the acetabular component “safe zone” plays in instability after THA has been called into question, but there remains no doubt placement of the acetabular component is crucial for establishing hip biomechanics. 40 Yet, the safe zone is not sufficient to protect THAs from a dislocation. A hip instability can occur with any combination of acetabular anteversion and inclination, since more than half of the dislocations coming from within the safe zone.41,42 In our study, acetabular position was equal between both surgeon groups. Also, all of the dislocations occurred within the safe zone, pointing to another reason for hip instability after THA for femoral neck fracture.
Restoration of lateral femoral offset, however, is a serious concern and remains statistically unrestored in THAs performed by NAS. Appropriate lateral femoral offset establishes abductor strength, functional outcomes, and range of motion while decreasing the risk of instability.7,38,39 Restoration of femoral offset is potentially the most important factor for dislocation in THA in the setting of a well-positioned acetabular component.22,43,44 If 3 mm of femoral offset is added to the preoperative position, there is a reduction in the rate of hip instability, with an odds ratio of 0.94. 22 In our study, NAS under-restored lateral femoral by 3 mm or more over 60% of the time by a mean of 4.8 ± 6.0 mm during THA for a femoral neck fracture. There are 2 biomechanical consequences to under-restoring lateral femoral offset: (1) a reduction in the abductor moment leading to an inadequate joint reactive force22,43,44; and (2) impingement of the femoral component on the acetabular component (intra-prosthetic) or other soft tissues (extra-articular) earlier as a result of reduced clearance. 45 When lateral femoral offset is restored, or slightly increased, it provides optimal impingement free range of motion.31,42
Our study suggests that preoperative templating did not affect the restoration of lateral femoral offset as there was no significant difference seen in the measurement with the presence or absence of templating prior to the surgery. Similarly, intraoperative imaging did not affect lateral femoral offset restoration since there was no significant difference in the measurement between surgeries that employed the technique and those without imaging. However, no NAS used intraoperative fluoroscopic or flat plate radiographic assistance and only 5 THAs were performed by one NAS using preoperative templating, limiting our ability to assess the effect of these modalities on mitigating the under-restoration of lateral femoral offset in the at-risk cohort. Altogether, our study determined preoperative templating and intraoperative imaging did not account for the significant difference seen in lateral femoral offset restoration when performed by EAS. 46 Other confounding factors may account for this difference such as length of training, 47 annual number of THAs performed, 48 or patient specific considerations dictating the surgeon’s decision making. 49 It should be noted that there was a statistical trend to having preoperative templating (p = 0.132) and intraoperative imaging (p = 0.158) help restore lateral femoral offset to within 3 mm of the uninjured side, but we were not powered to make a definitive conclusion regarding this outcome. Hence, further research should be conducted to establish the causal and preventive events that lead to the differences in lateral femoral offset restoration during THA after a femoral neck fracture when performed by either EAS or NAS.
Although our data shows clear and simple areas of technical improvement, it is not without additional limitations. Our data was limited by the retrospective review of the record. Additionally, we only had access to records from our institution leading to an incomplete capture of all the complications these patients may have experienced. Finally, we did not measure anteversion of the femoral stem which could correct or distort restoration of the hip, particularly as it relates to lateral femoral offset. 31
NAS surgeons tended not to restore lateral femoral offset during THA for a femoral neck fracture. Anatomical restoration of hip biomechanics is critical for establishing stability after elective THA. 37 Our data suggest the importance of restoring the lateral femoral offset in the setting of an urgent THA is just as important, if not more, than acetabular component positioning in the setting of a femoral neck fracture.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.