
Abstract
Background:
The postoperative management of femoroacetabular impingement (FAI) is variable with favourable surgical outcomes. Yet there is no evidence on the efficacy of hydrotherapy in athletes undergoing hip arthroscopy for FAI. The purpose of this study was to evaluate the role and the impact of hydrotherapy on return to sports following hip arthroscopy for symptomatic FAI.
Methods:
2 cohorts of mixed level of athletes from various sports: a hydrotherapy group that followed land-based exercises in combination with hydrotherapy exercises and a control group that followed solely the same land-based exercises. Pre- and postoperative pain and hip-specific outcome scores were completed, and patient satisfaction was rated.
Results:
A total of 88 hip arthroscopies were included with a minimum of 2 years follow-up; the hydrotherapy group comprised of 36 hips and the control group, 52 hips. There was a significant improvement in time to return to previous performance (HR 1.91, 95% CI, 1.21–3.01; p = 0.005) in the hydrotherapy group compared with the control. The hip-specific scores and patient satisfaction were considerably improved in the hydrotherapy group.
Conclusions:
The analysis of our data indicates that the incorporation of hydrotherapy into postoperative rehabilitation for hip arthroscopy for FAI accelerates the return of athletes to their pre-injury performance, since recovery time decreased significantly.
Keywords
Introduction
The femoroacetabular impingement (FAI) is recognised as a cause of hip pain in young, active individuals. 1 Lately, more athletes have been diagnosed with this condition.1–3 Athletes subject their hips to great amounts of stress, be it axial or torsional forces according to their athletic activities and therefore, they are at greater risk of presenting with intra-articular hip pathology that may lead to disability, disruption to athletic performance and daily living activities. 1 Femoroacetabular impingement with its associated injured intra-articular structures, can be successfully managed and treated with hip arthroscopy if, nonoperative therapy has failed.1–3
The postoperative management is variable and depends on surgeon’s preferences, complexity of surgical procedure and access to rehabilitation facilities. Several rehabilitation protocols have been proposed with favourable surgical outcomes.4–6 Recovery modalities include stretching, massage and passive range of motion (ROM) at early stages, followed by strengthening and resisted exercises, muscle endurance and cardiovascular conditioning.4–6 Incorporation of hydrotherapy into postoperative rehabilitation for hip arthroscopic surgery for FAI is not standard, although it has been widely used as part of rehabilitation for chronic conditions,7–11 in rheumatology or neurology,7,8 mostly for elderly people or chronic lower back pain.9,12,13 However, rehabilitation after orthopaedic surgery has received little attention as systematic reviews report.5,6,10,14,15 The aquatic environment due to its properties (buoyancy, hydrostatic pressure, cohesion, viscosity) provides improvement in mobility, strength, flexibility, muscular endurance and cardiovascular conditioning. 16 Yet, there is no evidence on the efficacy of hydrotherapy combined with land-based exercises as a standard method of rehabilitation in athletes undergoing hip arthroscopy for FAI. Ultimately, the quality of recovery techniques is crucial for restoring the physiological processes for the high performance of athletes.
The purpose of this study was to evaluate the role and the impact of hydrotherapy on return to sports following hip arthroscopy for symptomatic FAI. We hypothesised that hydrotherapy incorporated into postoperative rehabilitation after hip arthroscopic surgery for FAI, accelerates the return of athletes to their pre-injury level of performance.
Methods
All athletes underwent hip arthroscopy between March 2007 and December 2009 for symptomatic FAI after unsuccessful non-surgical treatment, as they were not able to perform their sports due to debilitating hip pain and restriction of movements of the hip joint. A single orthopaedic surgeon performed acetabular rim recession (including pincer resection when present), labral procedure (repair with 2 suture anchors or selective debridement) and femoral osteochondroplasty on all cases operated on. Additional procedures such as microfracture technique or repair of the capsulotomy were not performed. We excluded non-athletes, patients who had undergone any previous hip operation on the respective hip, simultaneous hip arthroscopies or for indications other than FAI, and revision hip surgery. All athletes were assessed in a standardised way, consisting of clinical examination and imaging of the affected hip. Data for demographics, medical history, clinical examination and imaging, type of sport and level of competition were prospectively collected.
We designed a controlled study engaging a mixed level of athletes, and we divided them retrospectively regarding their availability in a hydrotherapy setting into 2 cohorts: a hydrotherapy group that followed a standardised rehabilitation programme in combination with hydrotherapy exercises, and a control group (non-hydrotherapy) that followed solely the standardised land-based programme. Postoperatively, the athletes used crutches and were partial weight-bearing for 2–4 weeks. The standardised rehabilitation programme started 2 days after surgery and entailed 3 stages: each stage was built upon the previous, allowing for a safe progression to the next stage only once the athletes completed all exercises comfortably and pain free. Hydrotherapy commenced 2 weeks after the healing of the wounds, following the same principles as the standardised land-based rehabilitation programme starting in pool with chest-deep water progressing to waist-deep water. All patients followed the same supervised exercises whether it was land-based or aquatic exercises. Stage 1 consisted of early ROM, protection of healing tissues with avoidance of high hip flexion, controlling pain and inflammation. The athletes started on stationary bike, and closed chain exercises of adductors and abductors followed by Stage 2 with strengthening: open chain exercises of flexors, adductors, and abductors. Stage 3 introduced balance, core stability and proprioception exercises and progressed to sport-specific exercises.
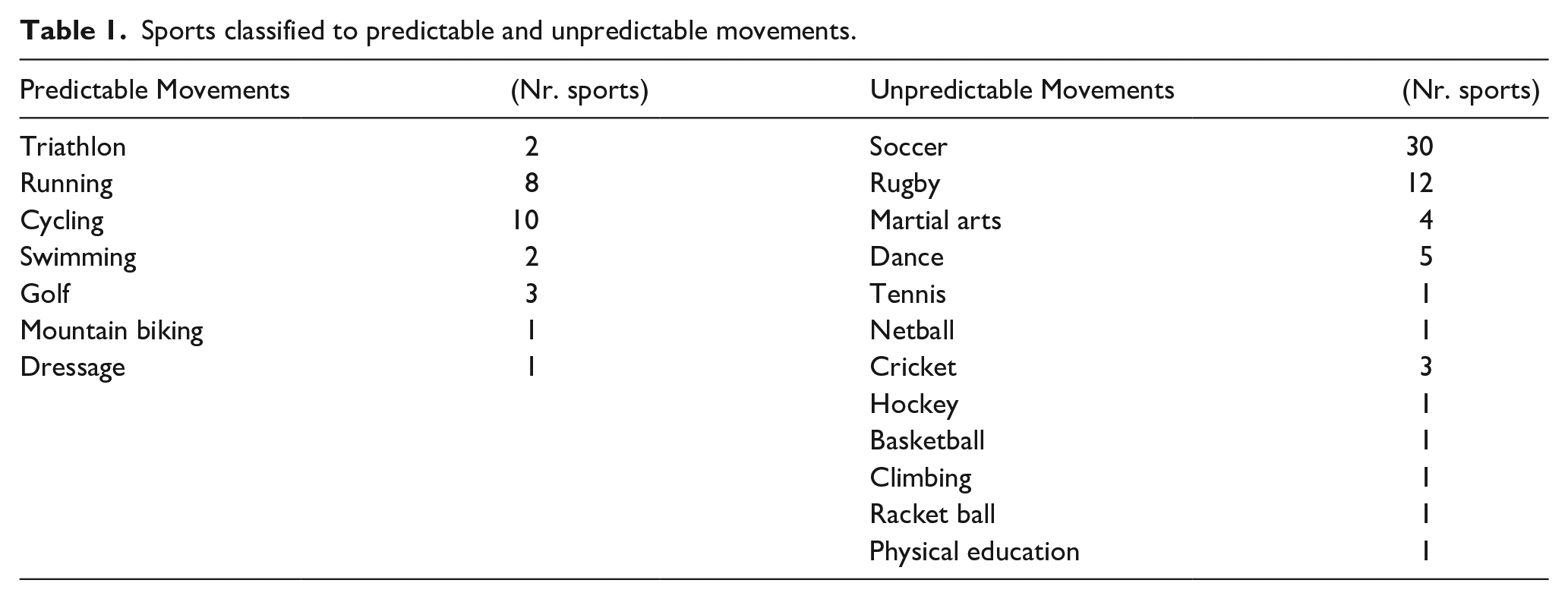
Sports were defined according to the predictability and variability of movement, 17 and thus they were categorised as sports with predictable and unpredictable movements achieving at the same time homogeneity (Table 1). Regarding the level of competition, there were mixed groups of professional and amateur athletes; professional was defined as the athlete with a paid steady job and amateur as the athlete with a recreational, intense participation in sports.
Sports classified to predictable and unpredictable movements.
The return to sports and the level of sport the athletes returned to were recorded. Athletes were assessed in clinic at 2 weeks, 8 weeks, 6 months, 12 months and annually. We included athletes with a minimum of 2 years follow-up. All patients completed hip-specific outcome scores pre and postoperatively: at 2 months, 6 months, 1 year and then annually. A 100-point scale was used for Modified Harris Hip Score (mHHS) and Sports Score (the function, sports and recreational activities section of the Hip disability and Osteoarthritis Outcome Score [HOOS]). The pain was scored on a visual analogue scale (VAS) and patient satisfaction was rated from 0 to 10 with 10 being very satisfied.
The study was a clinical audit; approval was obtained from the institutional review board following the waiver statement from National NHS Health Research Authority.
Statistical analysis
Statistical analysis performed to assess whether the time to return to previous performance differed by group (hydrotherapy/ control). A Cox proportional hazards model estimating hazard ratios (HR) and 95% confidence intervals (CI) was used with and without adjustment for: gender; level of competition; age at surgery; and operated side. Athletes were followed-up from surgery to the time they returned to their pre-injury performance; those who did not return were censored at the time of last follow-up at which they were still ‘at risk’ of returning. The proportional hazards assumption was assessed using scaled Schoenfeld residuals and the associated chi-square tests. The differences in patient satisfaction and in postoperative mHHS between the hydrotherapy and control cohorts were assessed using Mann-Whitney (Wilcoxon rank sum) tests. P-values < 0.05 were considered as evidence of a difference. Statistical analysis was performed using in the statistical software R (R Core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria).
Results
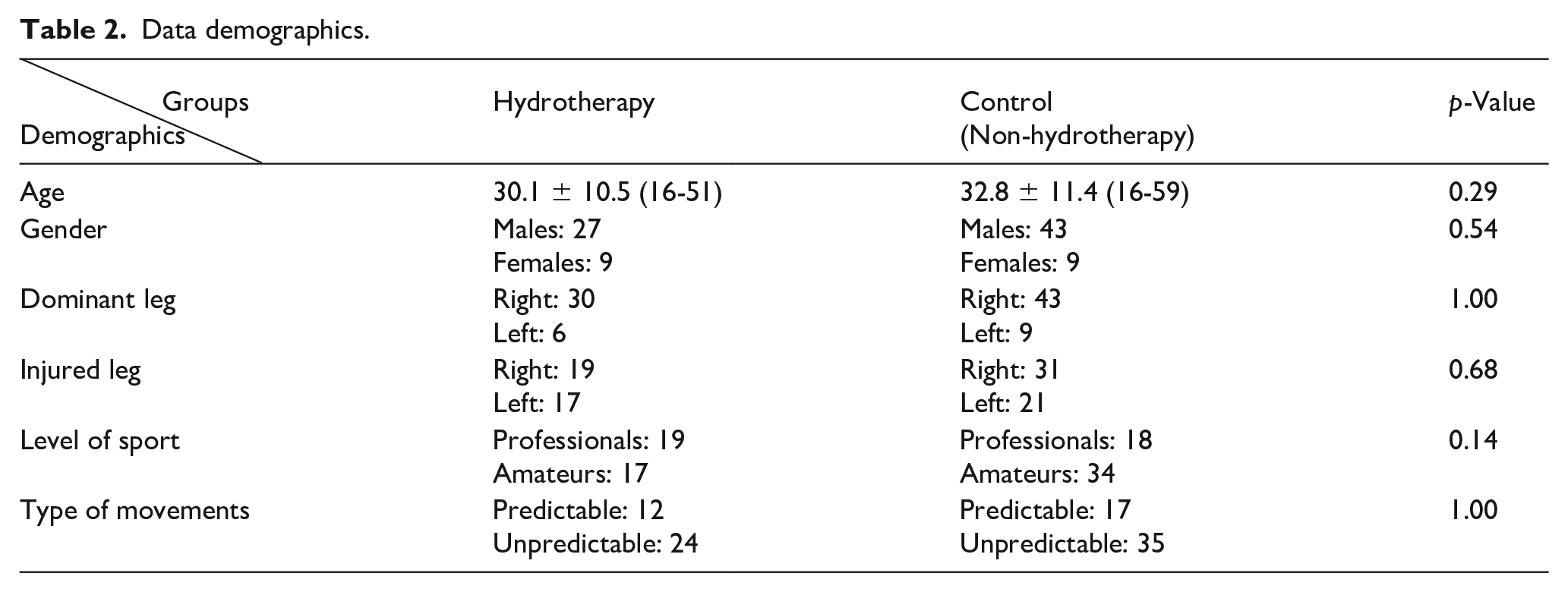
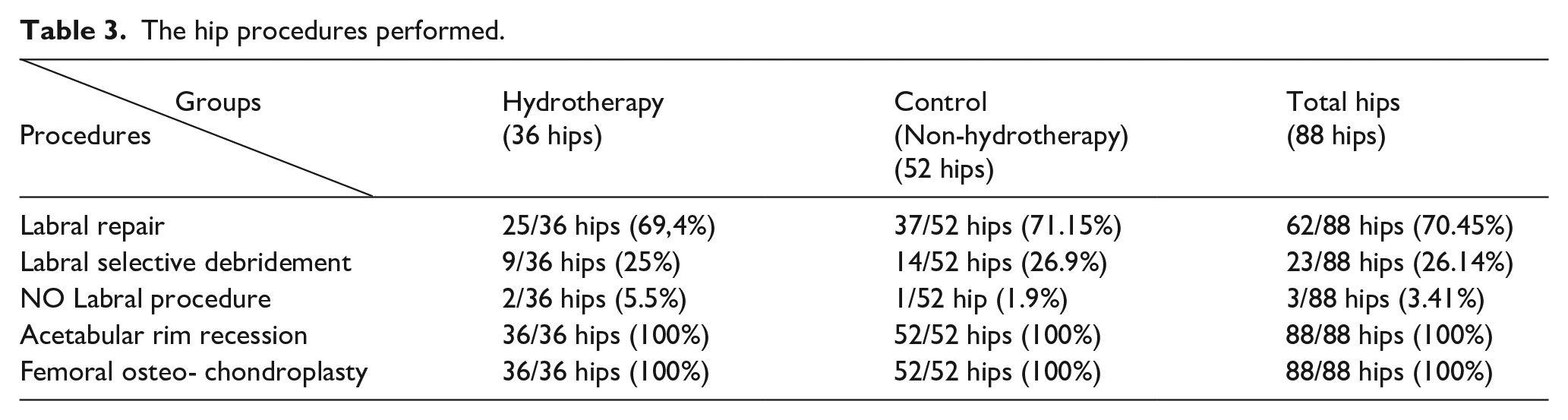
The study involved 88 hip arthroscopies for FAI. The athletes were divided into 2 cohorts: the hydrotherapy group involved 36 hips (40.9%) and the control group included 52 hips (59.1%). The average age for the hydrotherapy group was 30.1 years (16–51 years, standard deviation [SD] 10.5) and for the control group was 32.8 years (16–59 years, SD 11.4). Each group engaged a mixed level of athletes; there were 17 amateurs and 19 professionals in the hydrotherapy group and 34 amateurs and 18 professionals in the control group. The demographic data for each group and the procedures performed are presented in Tables 2 and 3 respectively.
Data demographics.
The hip procedures performed.
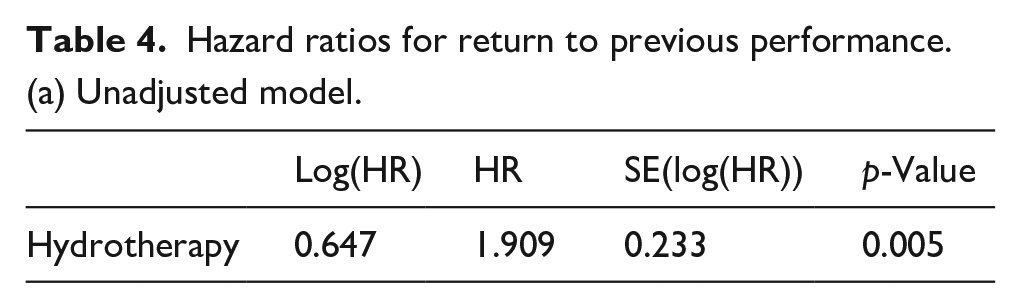
Athletes in the hydrotherapy group were more likely to return to previous performance (Figure 1), both without (HR 1.91; 95% CI 1.21–3.01; p = 0.005) and with adjustment for age at surgery, gender, level and operated leg (HR 1.84; 95% CI 1.12–3.00; p = 0.015) (Table 4). Scaled Schoenfeld residuals showed that the proportional hazards assumption for hydrotherapy was plausible (p = 0.25 and p = 0.15 for unadjusted and adjusted model, respectively).
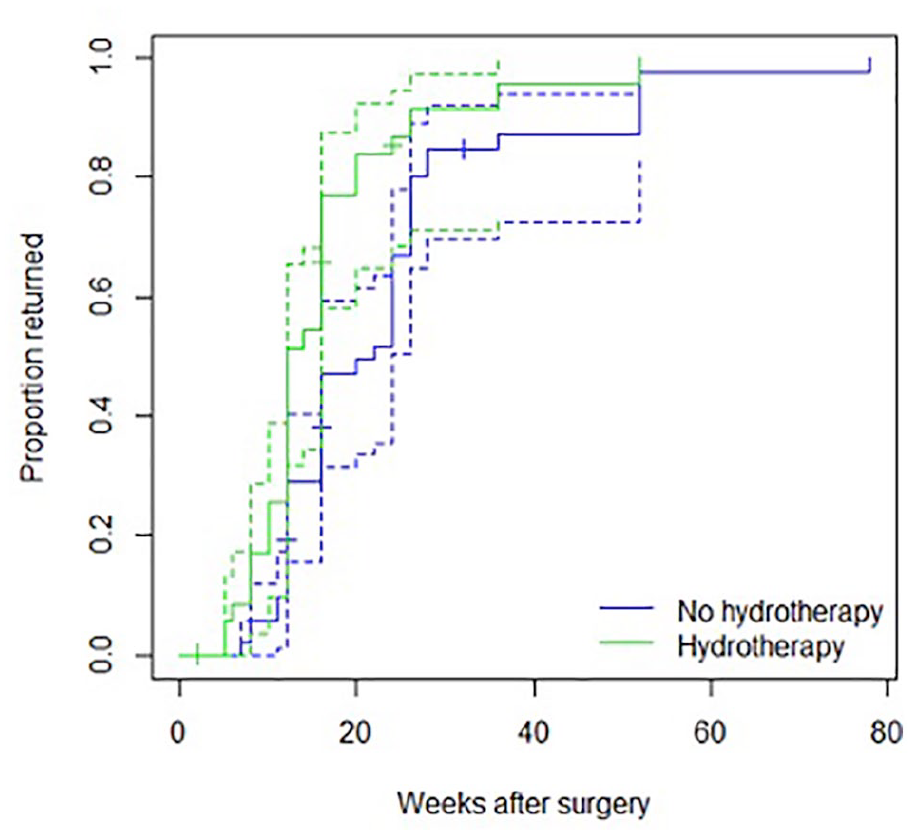
Cumulative incidence curves for return to performance by group.
Hazard ratios for return to previous performance.
(a) Unadjusted model.
(b) Adjusted model.
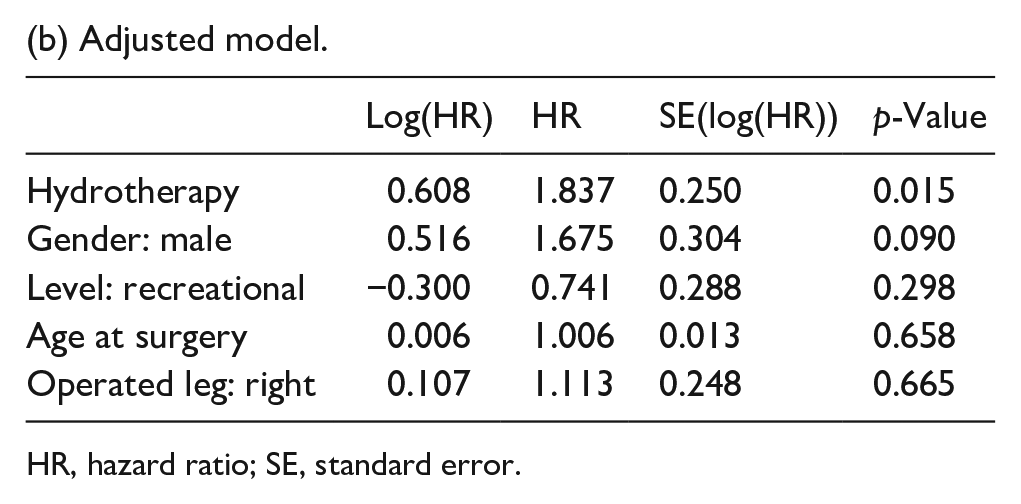
HR, hazard ratio; SE, standard error.
There were considerable improvements in the mean mHHS in hydrotherapy group (preoperative 62.9 [SD 13.7]; postoperative 94.9 [SD 10.9]) and mean Sports Score (preoperative 56.1 [SD 26.7]; postoperative 92 [SD 16.3]) (Figure 2). Pain was improved from 6.8 (SD 2.4) to 1.1 (SD 2.2) and patient satisfaction was scored with a median of 10 (IQR 1). In control group preoperative mean mHHS from 65 (SD 11.4) was improved to 92.8 (SD 9.56) postoperative and mean Sports Score from 57.2 (SD 25) preoperative to 92.8 (SD 12.8) postoperative. The pain was improved from 7 (SD 1.96) to 1.5 (SD 2) postoperative and patient satisfaction was scored as high as 9 (IQR 3). Comparing the postoperative mean mHHS between the 2 groups, the hydrotherapy group showed a higher average score compared to control group (Mann-Whitney U-test p = 0.019). Patient satisfaction was higher in the hydrotherapy group [mean 8.8 (SD 2.4) as opposed to control group 8.1 (2.3), Mann-Whitney U-test p = 0.013].
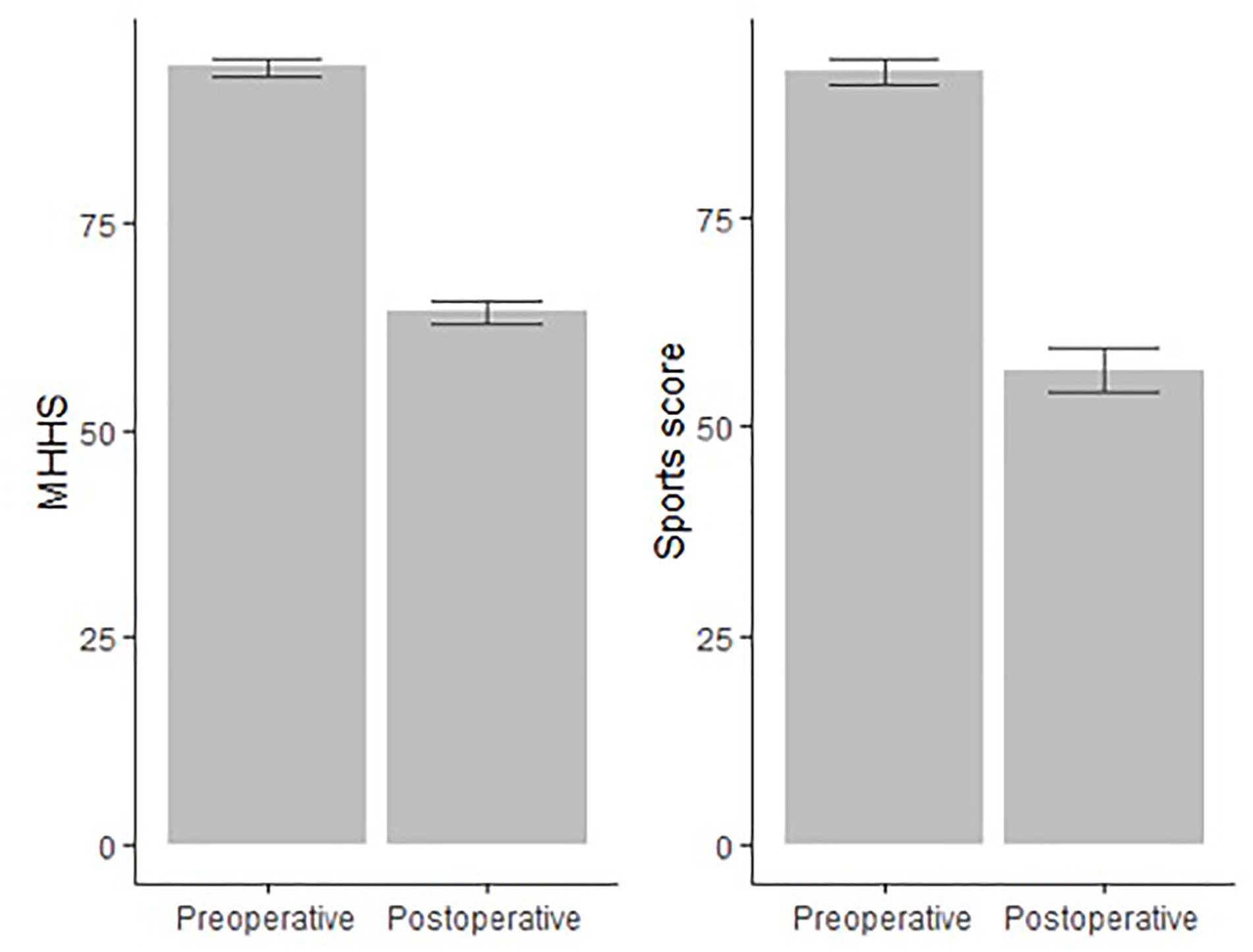
Means and standard errors of preoperative and postoperative MHHS and Sports score.
The hydrotherapy group returned to pre-injury performance on an average of 15 weeks (5–52 weeks, SD 9.1) while the control group on an average of 22.3 weeks (7–78 weeks, SD 14.07). Overall, 93.1% of athletes returned to their pre-injury level of performance at 2-year follow-up. From the hydrotherapy group, 2 amateur athletes (1 proceeded to a total hip arthroplasty due to advanced degenerative changes) and a professional athlete (for medical reasons unrelated to his hip) were not able to return to performance. From the control group, 2 amateur athletes (1 proceeded to a total hip arthroplasty due to advanced degenerative changes while a runner elected not to run fearful to re-injury his hip) and a professional soccer player (who was awaiting to undergo spinal surgery) did not return to performance.
Discussion
The most important finding of the present study was the difference in time to return to pre-injury performance; between the 2 groups. The athletes who followed the hydro-based protocol returned to play at 15 weeks while the control group took 22.3 weeks. Patients’ outcomes were also considerably improved in the hydrotherapy group suggesting that hydrotherapy is beneficial in the postoperative rehabilitation (higher postoperative outcomes scores (mHHS) and patient satisfaction). The comparison of the two groups revealed no other significant differences with respect to age, gender, joint movement type or level of sports.
Hydrotherapy is widely used as a rehabilitative and therapeutic method for other physically disabling conditions,7,8,11–13 however, in orthopaedic surgery it has received little attention.10,14–16 Moreover, early hydrotherapy within 3 months after orthopaedic surgery is sparsely reported in literature.5,15 Systematic reviews revealed a dearth of high-quality evidence to support a specific protocol for rehabilitation following hip arthroscopy;5,6,10 the protocols were variable and poorly reported. Despite the rationale for hydrotherapy in recovery, only 2 studies based on the same guidelines mentioned it sporadically in their predominantly land-based postoperative protocols.4,19 To the best of our knowledge, our study is the first to evaluate the efficacy of hydrotherapy in early postoperative period after arthroscopic FAI surgery in athletes by comparing it with standard land-based exercises and to assess the time to return to pre-injury level of performance.
The rehabilitation for athletes is fundamental and requires a systematic approach to ensure a successful return to performance. The return to training following land-based protocols has been reported between 12 and 20 weeks postoperatively and to competitive environment between 12 and 32 weeks.18,20 Philippon et al. 21 stated a return to skating/drilling in hockey players after 13.6 weeks, and return to play the first professional game between 18.8 and 36.8 weeks2,3 while athletes of various sports were allowed to return to full competitive activity between 12 and 16 weeks. 22 None of these studies compared athletes following different rehabilitative modalities or investigated the factors for accelerating the recovery. Moreover, athletes were professionals with financial motivations to return to sports.2,3,21,22 A mixed group of high-level athletes, including professional and collegiate athletes, revealed that 79% of patients were able to return to play at a mean of 37.6 weeks, 23 while elite athletes (mixed levels and various sports) returned to sports on an average 34 weeks. 1 Malviya et al. 24 reported on return to sporting activities after a mean of 21.6 weeks, in which 16.8 weeks was indicated for professional athletes while recreational returned at 27.2 weeks. Our findings clearly demonstrate that a significant difference between the 2 comparable groups was the time to return to their pre-injury performance; the athletes who followed the hydro-based protocol returned to play at 15 weeks (5–52 weeks, SD 9.1) while the control group on 22.3 weeks (7–78 weeks, SD 14.07). Hydrotherapy helps athletes to return to their athletic activities early and speeds up the rehabilitation process. 16 However, little is known regarding rehabilitation of athletes based on aquatic exercises.
Postoperative rehabilitation requires temporary rest and discontinued training from sport. Numerous studies have published that maximal oxygen consumption declines between 6–14% in well-trained athletes who refrained from training for 3–6 weeks leading to a significant loss of cardiovascular fitness.11,16 Therefore, early restarting of exercises is considered crucial to the successful return to pre-injury activity. Hydrotherapy allows athletes to start exercising earlier and to maintain the cardiorespiratory endurance while regaining mobility, muscle coordination and strength.15,25 Control of pain and inflammation while maintaining the range of movements and muscle strength without exacerbating the inflammation are the early postoperative goals after hip arthroscopy.4,20 Thus, the optimal healing environment would be an aquatic, where the aerobic training may be initiated well before athletes commence such exercises on land.14,26 The physical properties of water provide a unique environment for improving mobility, muscle strength, flexibility, balance ability and cardiovascular conditioning.16,25 The hydrostatic pressure during immersion of the human body in water decreases oedema, maintains muscle function, 25 provides pain relief and a calming effect by desensitising patients (nociceptors hypersensitivity) due to sensory input from the water pressure and temperature.9,12,16 Buoyancy decreases the effects of gravity on the body enabling greater range of movement without excessive muscle activation and therefore the progression to more advanced strengthening is smoother and easier when compared to land-based exercises. 26 The body weight decreases proportionally to the degree of immersion; in chest-deep water the weight-bearing load is approximately 40% of the total body weight, whereas waist-deep water increases the weight-bearing load to approximately 60%.25,26 Thus weight-bearing joints and particularly hips, may regain mobility while resting the operated leg, bear weight in the early postoperative period and gradually increase muscle strength and resistance by changing the depths of water.12,14,25,26 The static and dynamic balance is increased after hydrotherapy, coordination and posture are enhanced as the treatment for chronic lower back pain has demonstrated.12,13
Currently, as athletes compete harder at greater loads and take less time for recovery, they face increased pressure to return to sports. Hip arthroscopy rehabilitation protocols should allow the required time for tissue healing, yet to restore ROM, flexibility, muscular endurance, and strength, and reach the goal of safely returning athletes to high levels of functioning at a prompt time. Rehabilitation following hip arthroscopy is an integral part for a successful outcome in athletes therefore, consideration should be given in hydrotherapy as a treatment strategy at early stages for hip arthroscopy and structured protocols should be designed.
Limitations
While our study aims to assess the impact of hydrotherapy in rehabilitation and highlights its benefits, it does not attempt to establish a specific programme or the forms of hydrotherapy that may be most effective during the rehabilitation process. We attempted to limit the arthroscopic treatment only for FAI and labral tears excluding the wide variety of other intra- and extra-articular causes of hip pain in athletes and thus to evaluate the effectiveness of recovery.
The variety of sports in both groups was categorised by reflecting on the complexity and variability of movements within each sport, thus maintaining homogeneity and reducing bias. Additionally, the classification system used can estimate more accurately the load impact on the hip during sports. To avoid performance bias one surgeon operated all athletes and the technical variability was minimised as athletes underwent hip arthroscopy only for FAI and labral tears. Both groups were heterogeneous, including professional and amateur athletes together in an attempt to minimise the bias associated with the financial motivations and pressures from third parties for an early return to their competition.
An interesting point from data extraction is that hydrotherapy may not be available to professional athletes. The number of patients included was restricted by the number that was feasible to include. The 2 groups were not matched, but we adjusted for the main potential confounders in the analysis. However, there may still be residual confounding.
Conclusion
The analysis of our data indicates that the incorporation of hydrotherapy into postoperative rehabilitation for FAI hip arthroscopic surgery accelerates the return of athletes to their pre-injury performance since the recovery time decreased significantly.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.