
Abstract
Introduction:
The relationship between implant type, dual mobility (DM) or fixed bearing (FB), and postoperative groin pain remains unexplored. We examined the incidence of groin pain in DM implants and compare this to a cohort of FB THA patients.
Methods:
From 2006 to 2018, a single surgeon performed 875 DM THA and 856 FB THA procedures with 2.8-year and 3.1-year follow-up, respectively. Each patient received a questionnaire postoperatively and was asked if they had any groin pain (yes/no). Secondary measurements were implant characteristics such as head size, head offset, cup size, and cup-to-head ratio. Additional PROMs that were collected included: Veterans RAND 12 (VR-12), University of California Los Angeles (UCLA) activity score, Pain visual analogue scale (Pain VAS), and range of motion (ROM).
Results:
The incidence of groin pain was 2.3% in the DM THA cohort and 6.3% in the FB THA group (p < 0.001). Also, low head offset (⩽0 mm) had a significant odds ratio (1.61) for groin pain in both cohorts. There was no significant difference in terms of revision rate between the cohorts (2.5% vs. 3.3%, p = 0.39) at the latest follow up.
Conclusions:
This study demonstrated a lower incidence of groin pain (2.3%) in patients with a DM bearing compared to a FB (6.3%) and a greater risk of groin pain with low head offset (<0 mm). As such, surgeons should try to recreate offset of the hip compared to the contralateral side to avoid groin pain.
Introduction
By 2030 and 2040, it is projected that the percentage increase in annual total hip arthroplasty (THA) will be 129% and 284% in the United States, respectively. 1 THA have shown positive long-term benefits at 25–30 years of follow-up, including decreased pain and improved function and quality of life. 2 However, groin pain has been reported to occur in up to 18.3% and 12.9% of patients at 3 months and 24 months follow-up, respectively. 3 Groin pain can result from soft tissue inflammation, tendinitis and impingement of the iliopsoas tendon, and aseptic loosening of the components, most commonly the acetabular one.3,4 In addition, several preoperative factors such as smaller hip range of motion and intraoperative technical issues such as cup oversizing resulting in psoas impingement may increase the risk of postoperative groin pain.5,6
Dual-mobility (DM) implants have shown favourable outcomes in lowering dislocation rates, readmission rates, and revision rates in comparison to fixed bearing (FB) implants in both the primary and revision setting. 7 DM implants benefit from an improved head-neck ratio that allows for greater range of motion, while limiting the femoral neck impingement of metal-on-metal bearings or fixed liners. 8 Large diameter femoral heads have been associated with increased groin pain related to anterior soft-tissue impingement against the iliopsoas tendon. 9 In addition, some dual-mobility designs provide a recessed region anteriorly for the psoas tendon, which reduces risk of impingement. 10
The relationship between implant type (DM or FB) and postoperative groin pain has not been fully elucidated in the literature. 1 recent study found that DM implants were not associated with a higher risk of groin pain at 1-year follow-up despite its larger femoral head sizes. 11 The aim of the current study was to compare the impact of implant type on groin pain as well as patient-reported outcome measurements (PROMs) and revision rates at an average follow-up of 3 years.
Materials and methods
Our institution’s registry was queried to include only primary THA performed by a single surgeon at a high-volume centre from 2006 to 2018. The posterior approach was exclusively used in all procedures. 2 DM systems were used: 584 anatomic dual-mobility (ADM; Stryker, Mahwah, NJ) and 291 modular dual-mobility (MDM; Stryker) implants. 1 FB acetabular implant was used: Trident PSL Acetabular System (Stryker).
The exclusion criteria included: (1) follow-up <1 year and (2) pathological fracture of the femoral neck.
Indications for dual mobility
The use of a dual-mobility liner was at the senior surgeon’s discretion and included mostly patients at increased risk for dislocation. Such indications included patients with spinal pathology (advanced degenerative disease or fusion that has a known increased risk for hip instability), 12 smaller anatomy (in which a smaller head is needed), 13 neuromuscular conditions (i.e., Parkinsonism, cognitive impairment (e.g. dementia), 14 femoral neck fracture, conversion surgery (i.e. femoral nail to total hip arthroplasty), 15 patients that put their hip arthroplasty in a high risk situation for instability (e.g. yoga). 16
ADM was preferentially used over MDM for smaller-sized patients with acetabular component of ⩽50 mm so that a 28-mm head could be utilised.
Anatomic dual mobility
ADM is a cementless, monoblock cobalt chrome alloy cup with a titanium and hydroxyapatite outer surface. It uses an anatomic-shaped rim that matches the native acetabular socket. An anterior recess allows for a psoas cutout which was designed to reduce psoas impingement. It also incorporates a posterior and inferior buildup, mimicking the native acetabulum and increasing stability in deeper flexion. The 46-mm, 48-mm, and 50-mm shells use a 28-mm head which was the authors’ preference since it increases stability at the intraprosthetic interface.
Modular dual mobility
MDM implants consist of a modular cobalt chrome liner that is inserted into a cementless acetabular shell and allows for a DM polyethylene liner that articulates against the dual-mobility modular metal liner. A standard titanium cup can be used with the option of screws, which allows for augmentation of the fixation, particularly in weaker bone or revision surgery. With the MDM design utilised in this study, a 22-mm head was needed for liner size D (46-mm, 48-mm, and some 50-mm shells) so these smaller sizes were avoided by the senior author and an ADM was used instead.
Head offset
Every attempt was made while templating the hip replacement to ensure that the combined offset was recreated compared to the contralateral hip. This involved the selection of a “high offset stem” and the appropriate length femoral head. In addition, the senior author removed all peripheral osteophytes around the acetabular component to ensure impingement free range of motion.
Patient-reported outcome measurements
The primary measurement recorded was groin pain (yes/no). Additional PROMs that were collected included: Veterans RAND 12-Item Health Survey (VR-12), University of California Los Angeles (UCLA) activity score, Pain visual analogue scale (Pain VAS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), range of motion (ROM), and revision rate at an average follow-up of 3 years postoperatively. The secondary measurement was implant characteristics including head size, head offset, cup size, and cup-to-head ratio based on the presence of groin pain. For most patients, follow-up visits took place at 6 weeks, 3 months, 1 year, 2 years and 3 years postoperatively.
Statistical methods
The Student’s t-test was used to compare normally distributed continuous data. Logistic regression models were used to determine the odds of groin pain at 2 years depending on cup size and head offset. A p-value of <0.05 was the cutoff for statistical significance.
Results
A single surgeon performed a total of 1904 primary THA, including 875 procedures using DM implants and 921 surgeries using FB implants from 2008 to 2018. 43 were lost to follow-up in the DM cohort (4.3%) and 65 patients in the FB cohort (7.8%). Therefore, the study included 1731 patients with 875 in the DM cohort and 856 in the FB cohort. In the DM cohort, 291 implants were MDM and 584 were ADM. The patient demographics were similar in the DM and FB cohorts, including average age (66.7 years vs. 65.6 years, p = 0.06), body mass index [BMI] (32.2 kg/m2 vs. 28.9 kg/m2, p = 0.67) and male: female breakdown (342:533 vs. 367:489, p = 0.77), respectively. The average follow-up in the DM cohort was 2.8 years and the average follow-up in the FB cohort was 3.1 years (p = 0.06).
The incidence of groin pain was significantly less in the DM cohort (2.3%) compared to the FB cohort (6.3%), p < 0.0001 (Table 1). There was no difference in groin pain between the different dual-mobility designs (MDM 2.2% vs. ADM 2.4%, p = 0.13).
Postoperative PROMs between cohorts at respective follow-up.
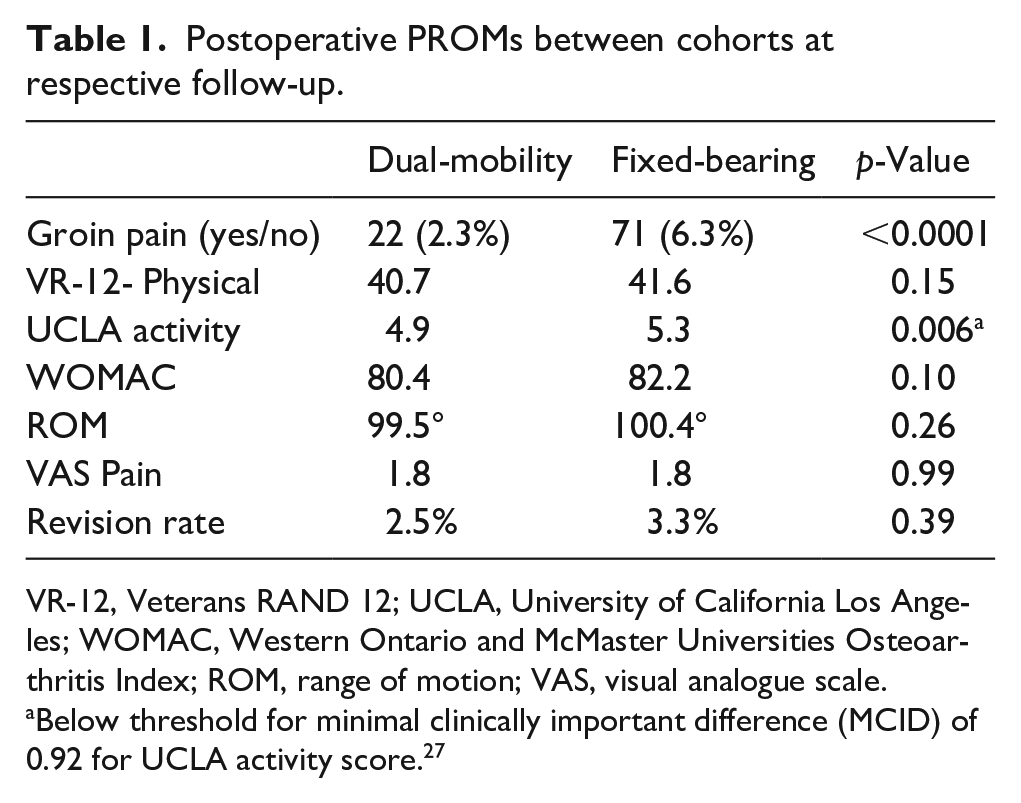
VR-12, Veterans RAND 12; UCLA, University of California Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; ROM, range of motion; VAS, visual analogue scale.
Below threshold for minimal clinically important difference (MCID) of 0.92 for UCLA activity score. 27
There were no significant differences in the PROMs between these cohorts: VR-12- Physical score (40.7 vs. 41.6, p = 0.15), UCLA activity (4.9 vs. 5.3, p = 0.006, <MCID of 0.92), WOMAC (80.4 vs. 82.2, p = 0.10), hip flexion (99.5° vs. 100.4°, p = 0.26), VAS Pain (1.8 vs. 1.8, p = 0.99), and revision rate (2.5% vs. 3.3%, p = 0.39), respectively.
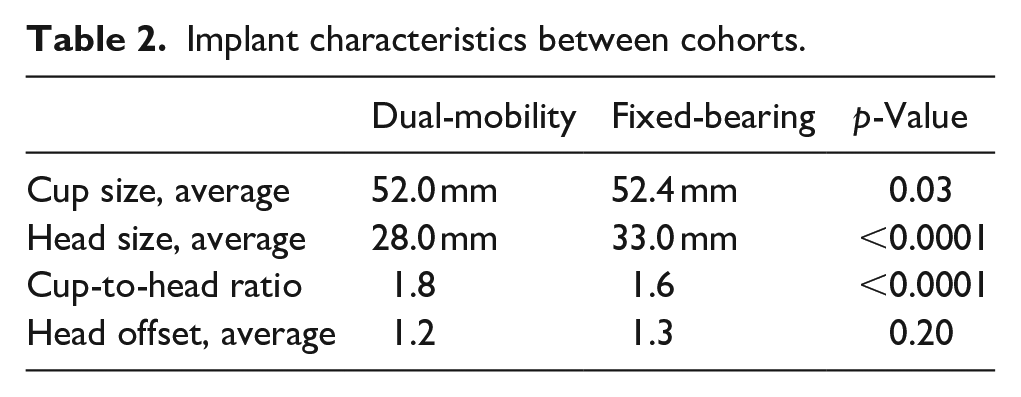
Implant characteristics did significantly differ between the cohorts with the DM cohort having a smaller average head size compared to the FB cohort (28.0 mm vs. 33.0 mm, p < 0.0001), smaller cup-to-head ratio (1.6 vs. 1.8, p < 0.0001) and smaller average cup size (52.0 mm vs. 52.4 mm, p = 0.03), respectively (Table 2).
Implant characteristics between cohorts.
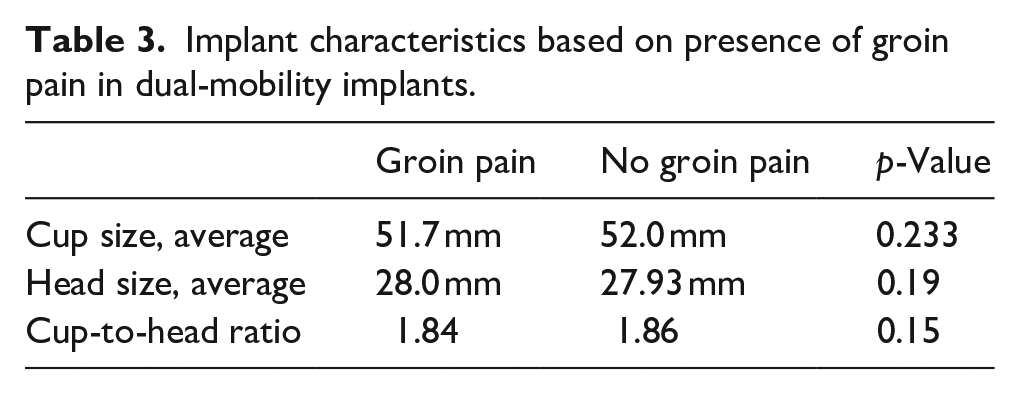
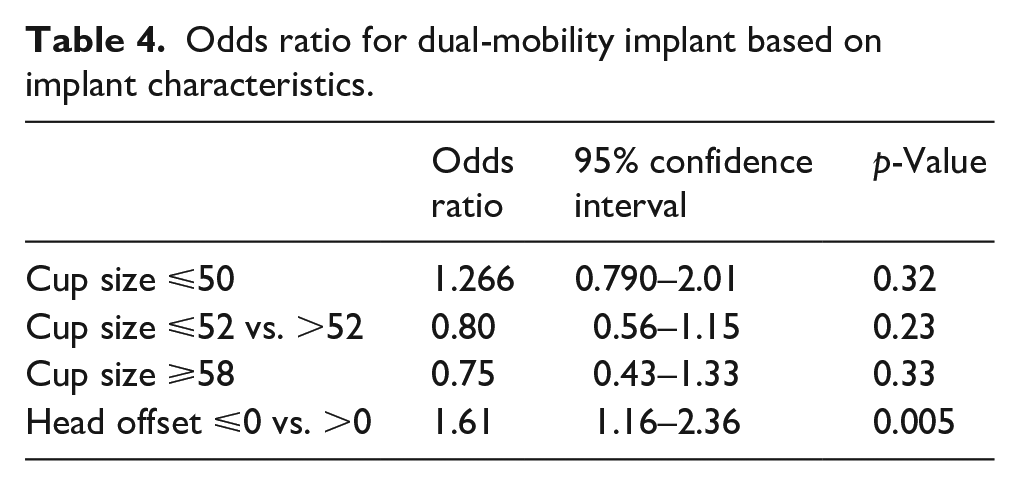
DM implants showed no difference in regard to average cup size (51.7 mm vs. 52.0 mm, p = 0.233), average head size (28.0. mm vs. 27.93 mm, p = 0.19) and cup-to-head ratio (1.84 vs. 1.86, p = 0.15) between patients with groin pain and no groin pain, respectively (Table 3). Similarly, DM implants showed no increased odds ratio (OR) for cup size ⩽50 mm (OR 1.266, p = 0.32), cup size ⩽52 mm vs. >52 mm (OR 0.80, p = 0.23), or cup size ⩾58 mm (OR 0.75, p = 0.33), but did show a significant odds ratio for head offset ⩽0 mm vs. >0 mm (OR 1.61, p = 0.005) (Table 4). However, there was no difference in terms of femoral head offset (1.15 mm vs. 1.3 mm, p = 0.19) between the DM and FB cohorts, respectively.
Implant characteristics based on presence of groin pain in dual-mobility implants.
Odds ratio for dual-mobility implant based on implant characteristics.
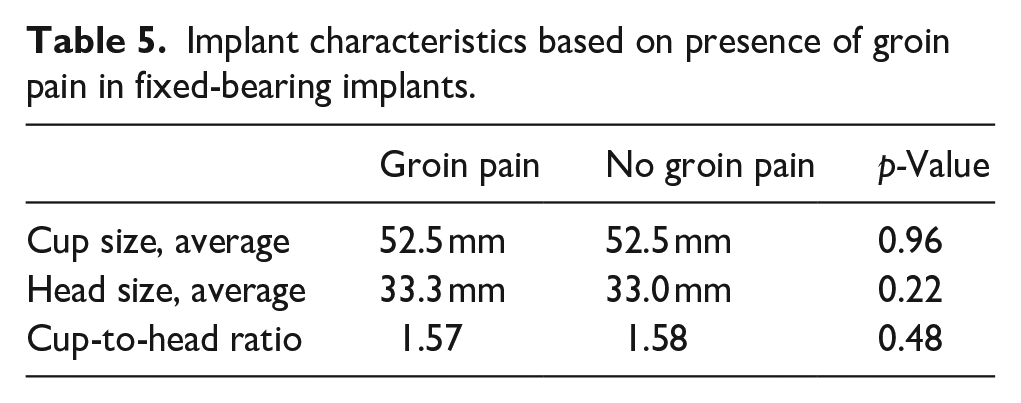
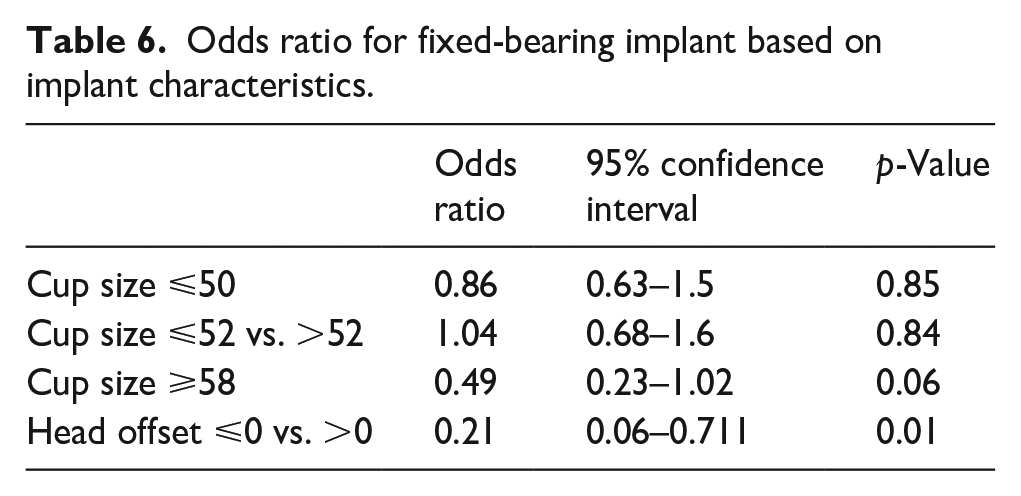
With respect to FB implants in patients with and without groin pain, there was no difference in terms of average cup size (52.5 mm vs. 52.55 mm, p = 0.96), average head size (33.3 mm vs. 33.0 mm, p = 0.22), or cup-to-head ratio (1.57 vs. 1.58, p = 0.48), but odds ratio were increased for groin pain based on head offset head offset ⩽0 mm vs. >0 mm (OR 0.21, p = 0.01) (Table 5). There was no significant increase in odds ratio in terms of cup size ⩽50 mm (OR 0.86, p = 0.85), cup size ⩽52 mm vs. >52 mm (OR 1.04, p = 0.84), or cup size⩾ 58 mm (OR:0.49, p = 0.06) (Table 6).
Implant characteristics based on presence of groin pain in fixed-bearing implants.
Odds ratio for fixed-bearing implant based on implant characteristics.
Discussion
Our major finding was that there was a significant difference in groin pain favouring the DM cohort at an average follow-up of 3 years. Our secondary finding was that low head offset (⩽0) had a significant odds ratio (1.61) for groin pain in both cohorts. The literature offers support for DM bearings in comparison to FB bearings, in terms of lower dislocation rates, functional outcome scores, and lower wear rates.7,14 Groin pain has remained a complex and unexplored issue because the evaluation and treatment measures of groin pain following THA have not been uniformly evaluated as well as the difficulty in localising the specific area of pain.
While larger femoral heads can reduce dislocation, larger fixed bearing heads have led to implant loosening, taper corrosion, and higher susceptibility to groin pain. 17 This may result from greater iliopsoas impingement through protrusion of the large prosthetic head anteriorly and scarring between the anterior capsule and tendon. 18 A contoured anatomic shape, as implemented in the ADM design, was introduced to retain the large diameter of the mobile bearing while reducing volume of material in the distal, non-articulating region. Varadarajan et al. 19 found that contoured liners reduced iliopsoas tenting over the distal regions of the mobile liner while maintaining pull-out resistance, jump distance, and impingement-free ROM. This may be attributed to the reduced and more rounded profile of the head below the equator. 20 An additional study found average contact pressure and von Mises stresses were lower in the contour design compared to the conventional implant, which may offer a solution to avoiding anterior soft-tissue impingement with large femoral heads. 21 Although we did not find a difference for groin pain in regards to MDM versus ADM (2.2 vs. 2.4%, p = 0.13), the benefits of the countered design suggest further investigation in future studies.
The literature has called for a greater comparison of DM and FB implants in relation to groin pain. One recent study by Stavrakis et al. 11 found that DM implants do not have a greater incidence of groin pain compared to FB implants at 1-year follow-up even with a greater cup-to-head ratio. The authors attribute this finding to the inner bearing of DM implants controlling most of the motion in the bearings, which may minimise the role of the large-head bearing in causing pain. 11 On the other hand, another study associated larger femoral heads with soft-tissue impingement against the iliopsoas tendon and more groin pain (15–18% vs. 7%). 22 Dual-mobility implants may allow for the majority of motion in the bearings to occur at the inner bearing and motion at the outer bearing only occurring at extreme range of motion.23,24 This may obviate several causes of pain associated with large-head bearing surfaces, including iliopsoas impingement and greater force on the femoral trunnion, which can lead to corrosion, metal release, and adverse local tissue reactions.11,25,26 The majority of the implants used in this study (584 vs. 291) utilise the ADM cup that incorporates a cut out for the psoas tendon allowing the implant rim to match the anatomic contour of the native acetabulum, which may lead to reduced groin pain but was not found in this study (2.2% vs. 2.4%, p = 0.13).
The role of head offset and its relationship to pain after THA has mixed results. 1 study examining the effects of femoral offset in THA found that increasing the femoral offset to 4 mm and 8 mm resulted in improved flexion and internal rotation. This improvement was rationalised by the reduction of the osseous impingement, which may have a positive influence on reducing groin pain. 27 Another study found that patients with an increased head offset had better outcomes according to the Oxford Hip Score (OHS). 28 However, Liebs et al. 29 found that lower offset (<5 mm) was associated with reduced pain compared to increased offset (5 mm). The literature supports that larger offset differences (5 mm) may affect postoperative outcomes, including groin pain, through altered gait kinematics. 30
We acknowledge some limitations in the current study. Groin pan was assessed via a “yes/no” scale and while a pain severity score would have provided additional information, patients were able to be differentiated based on implant. Given the temporal differences in the cohorts, there could be variance in surgical technique or experience yet the similar PROMs and revision rates support the homogeneity in surgical performance by a single surgeon. We did not look at other causes of groin pain, including trochanteric/lateral hip pain or buttock pain. The mechanism of groin pain due to iliopsoas impingement was not investigated further, including computed tomography (CT) analysis to identify anterior acetabular component overhang or diagnostic injection used to confirm the diagnosis. The largest, and most common head size for fixed-bearing implant was 36 mm followed by 32-mm heads. There was no relationship between head size and groin pain in fixed bearing implants. The aetiology of groin pain after THA is multifactorial and may not be limited to the implant design. Additionally, although the absence of pain cannot be directly attributed to DM systems, a recent paper showing 9.0% of patients reported groin pain at 1-year follow-up after undergoing FB THA provides credibility to our findings. 11 The proportion of patients with groin pain undergoing surgical invention, such as psoas lengthening or revision of the prosthesis was not included in the analysis. The strengths of the study lie in its large patient numbers, extended follow-up, and use of a single surgeon in a high-volume arthroplasty institution.
The prevalence of groin pain postoperatively in regard to DM implants has not received proper attention in the literature. Our study supports the finding that DM implants may lower groin pain in comparison to FB implants 6.3% versus 2.3%, respectively. In addition, there was a notable increased in groin in both cohorts when using head offsets ⩽0 mm at 3 years postoperatively.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GHW: Receives royalties from Exactech; paid consultant for: Stryker, Exactech, DJO; receives research support from: Stryker, Exactech, DJO.
The other author declares that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.