
Abstract
Introduction:
The routine use of proximal femoral modularity was discouraged in total hip arthroplasties (THAs). However, titanium dual-taper (DT) implants may provide some advantages over single-taper (ST) stems in cases of complex deformity. A registry study comparing ST and DT stems in dysplasia was designed, aiming to assess: (1) survival rates at long-term; (2) reasons for revision; (3) the profile of failed implants.
Methods:
The arthroplasty registry RIPO was investigated for cementless THAs performed for dysplasia since 2000. ST implants were compared to titanium-on-titanium DT stems. Demographics and implant features were collected. Survival rates and reasons for revision were compared. The profile of DT stem failures in dysplasia was defined.
Results:
6429 implants were included in the study, 3642 ST and 2787 DT. The demographic and implant features of the 2 cohorts were not comparable. The DT cohort achieved higher survival rates at long-term (93.9% vs. 91.6%, p = 0.018). DT implants showed a higher rate of implant breakage (0.6%, p = 0.011) and a lower rate of aseptic loosening (p = 0.005). There were no differences in terms of revisions for dislocation. No metallosis occurred. There were more revisions in DT implants in males <65 years, with a 28-mm head size or smaller.
Conclusions:
Modularity did not result in lower survival rates in dysplastic patients and may even reduce the rate of aseptic loosening in comparison to ST stems. The rate of implant breakage is not negligible. Younger males are not good candidates for titanium DT stems.
Introduction
Proximal modularity was introduced into the market to provide independent combinations of version, offset and length, with the aim of improving soft tissue tensioning, hip biomechanics and implant stability.1,2 However, in total hip arthroplasties (THAs), dual-taper (DT) modular implants, which provide an additional junction at the neck-stem interface, failed to demonstrate superior outcomes over single-taper (ST) stems (with only head-neck modularity). Moreover, modular implants showed a high rate of implant-related revisions, sometimes leading to implant recalls. 1 National registry reports comparing the survival rates and the reasons for revision of exchangeable and fixed neck implants recommend avoiding the routine use of modularity, carefully evaluating the benefits, and reserving these implants for proximal femoral deformities.3,4
In developmental dysplasia of the hip (DDH), modularity may be of help. 1 However, the outcomes of modularity in DDH are described in single-centre retrospective case series, mainly without a control group.5–17
Thus, an arthroplasty registry study was designed to compare the outcomes of DT and ST implants in THAs undertaken for osteoarthritis after DDH. Only DT implants with proximal titanium-on-titanium modularity were admitted. The aims of the investigation were: (1) to compare the survival rates at long-term in DT and ST cohorts; (2) to evaluate the reasons for revision in the 2 cohorts; (3) to define the risks for implant failure in DDH. We hypothesised that modularity improves survival rates and reduces revisions for dislocations but may be unsuitable for younger males.
Methods
The regional arthroplasty registry RIPO (Registro dell’Implantologia Protesica Ortopedica) has been providing active data on hip, knee and shoulder arthroplasties since January 2000 in the Italian region of Emilia-Romagna (around 4,500,000 inhabitants).18,19 The registry involves 68 orthopaedic facilities.18,19 All surgeons performing primary arthroplasty or revision surgeries are required to fill in the RIPO form, specifying the clinical condition of patients, devices (batch and code) and surgical technique (approach and fixation). The registry collects a database with a reported capture rate of 98%.18,19 The 2% of missing data are due to the lack of adherence.18,19
The RIPO registry was asked about all the primary cementless THAs performed in the Emilia-Romagna region from January 2000 to December 2018.
The inclusion criteria were: patients resident to the region (to minimise the loss of patients at follow-up: all the arthroplasty procedures performed on residents are billed back to the region itself, thus are captured by the registry); THAs performed for osteoarthritis after DDH (as specified in RIPO form).18,19
The exclusion criteria were: THAs performed for reasons other than DDH; non-resident patients; metal-on-metal implants with head size >32 mm; DT implants mixing metal alloys, like cobalt-chrome necks on titanium alloy stems. In these cases, a high rate of failures was reported, almost doubling the revisions of the titanium-on-titanium cohort. 3
The selected THAs were stratified into 2 cohorts, ST and DT, according to proximal modularity: ST had only head-neck modularity, whereas DT had an additional neck-stem junction. Demographic and implant-related features of both cohorts were collected and compared. The survival rates of the cohorts were calculated and compared. The reasons for revision were analysed and compared. Finally, the profile of the implants at a higher risk of failure in DDH was defined.
Institutional board review was waived due to the nature of the study and data anonymity.
Statistical analysis
Statistical analyses were performed using SPSS software (version 14.0.1, Chicago, IL, USA) JMP, version 12.0.1 (SAS Institute Inc, Cary, NC, 1989-2007). Demographics, implant-related features and reasons for revision were reported as raw data, ranges, and percentages. The differences between the 2 cohorts for preoperative and implant-related parameters were detected using Student t-test, Fisher test and chi-square test. The survival curves were calculated and plotted according to the Kaplan-Meier method. Each curve was flanked by a pair of 95% confidence interval (CI) curves. The implants were considered “surviving” at the last date of observation (date of death or 31 December 2018) when no single component was replaced. Log rank and Wilcoxon tests were used to detect the differences between the survival curves (threshold: p = 0.05). A multivariate Cox regression model (variables: 65 years, sex, 28-mm head size) was estimated to profile the implant at a higher risk of failure, using the Wald test to calculate p-values. Hazard ratios and their corresponding 95% CI were calculated. The threshold for significance was p = 0.05.
Results
6429 implants were included in the analysis, 3642 ST and 2787 DT stems. The 2 cohorts were not comparable in terms of age, gender, weight and body mass index (BMI) (p < 0.001) (Table 1). The distribution of head sizes and bearing surfaces were different in the 2 cohorts: ST implants had more polyethylene liners and smaller heads (⩽28 mm) than DT.
The demographic and implant -related features of the 2 cohorts were not comparable concerning age, gender, weight and BMI.
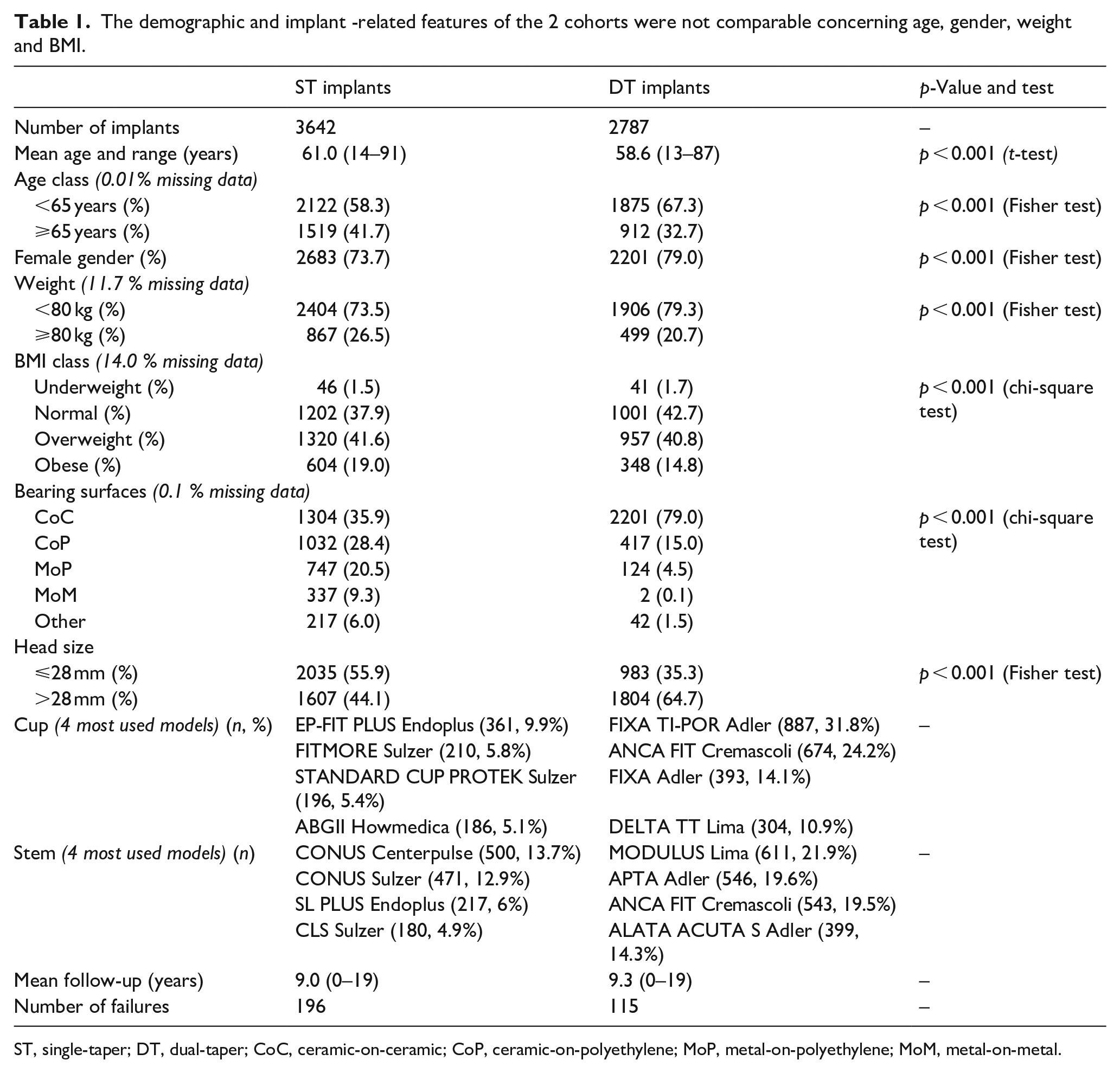
ST, single-taper; DT, dual-taper; CoC, ceramic-on-ceramic; CoP, ceramic-on-polyethylene; MoP, metal-on-polyethylene; MoM, metal-on-metal.
The mean follow-ups were 9 years in ST and 9.3 years in DT.
DT stems were homogenously implanted over time, overall representing 40–50% of the devices adopted for DDH every year since 2000 (Figure 1).
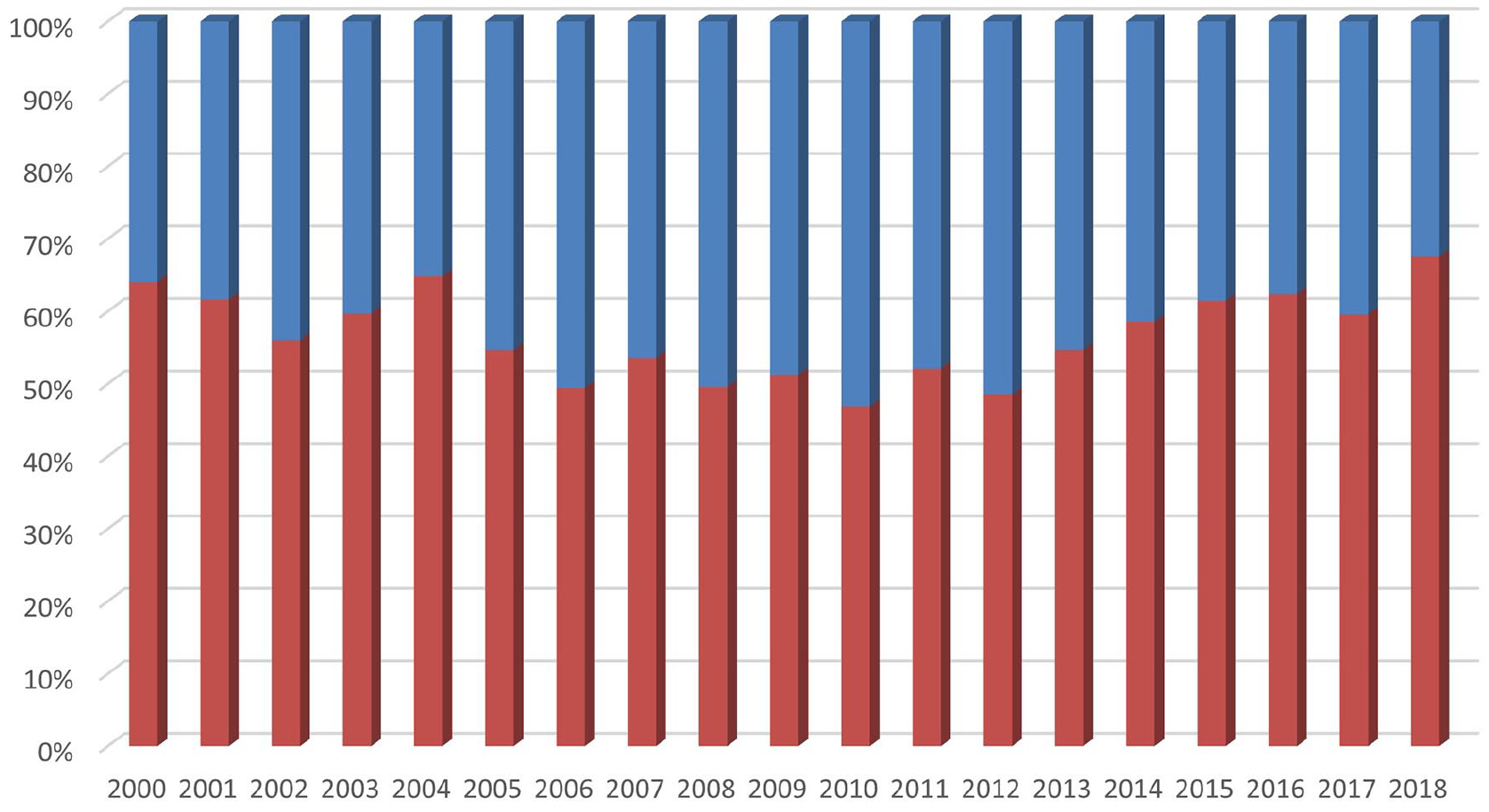
The distribution of the ST (red – lower) and DT (blue – upper) implants over the time showed a quite regular adoption of modular devices, accounting for 40–50% of the THAs for DDH per year.
Survival rates
DT implants showed significantly better survival rates than ST at every follow-up (p = 0.018, Log rank test) (Figure 2). At 15 years, when >15% of the implants were still at risk in both cohorts, DT achieved a survival rate of 93.9%, whereas ST had a lower performance (91.6%).
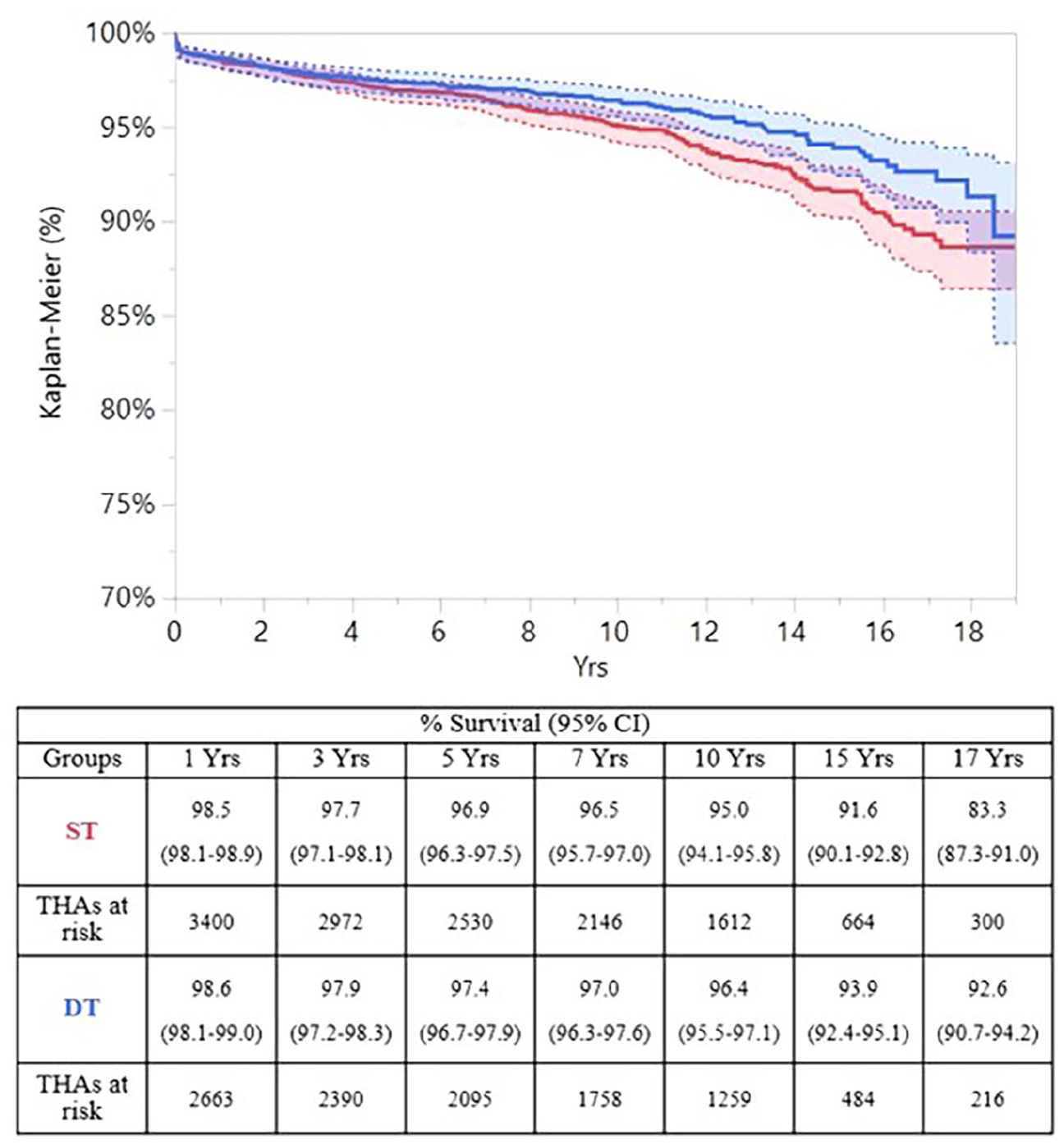
The DT cohort, in blue (lower and paler), outperformed the ST cohort, in red (upper and darker), at every follow-up (p = 0.018).
Incidence and distribution of the reasons for revision
The ST cohort showed 5.4% of revisions (196), whereas in the DT group the percentage was lower (4.1%, 115). The most frequent reason for revision was cup aseptic loosening in the ST cohort (1.6% in ST and 0.3% in DT of all the implants) and stem aseptic loosening in the DT group (0.5% in ST and 0.6% in DT of all the implants). The percentage of cup aseptic loosening was 1.6% in the ST and 0.3% in DT cohort. Recurrent dislocations occurred in 0.7% of ST implants and 0.6% of the DT. The percentage of implant breakage was 0.6% in the DT group and 0.2% in the ST cohort. No revision for metallosis was performed in DT implants.
DT and ST cohorts were similar in terms of revisions for periprosthetic infection (p = 0.792), revisions for dislocations or primary instability (p = 0.478), revisions for stem aseptic loosening (p = 0.343). On the other hand, the DT cohort showed a significantly lower risk of aseptic loosening in general (p = 0.005) and a significantly higher risk of implant breakage (p = 0.011) (Figure 3).
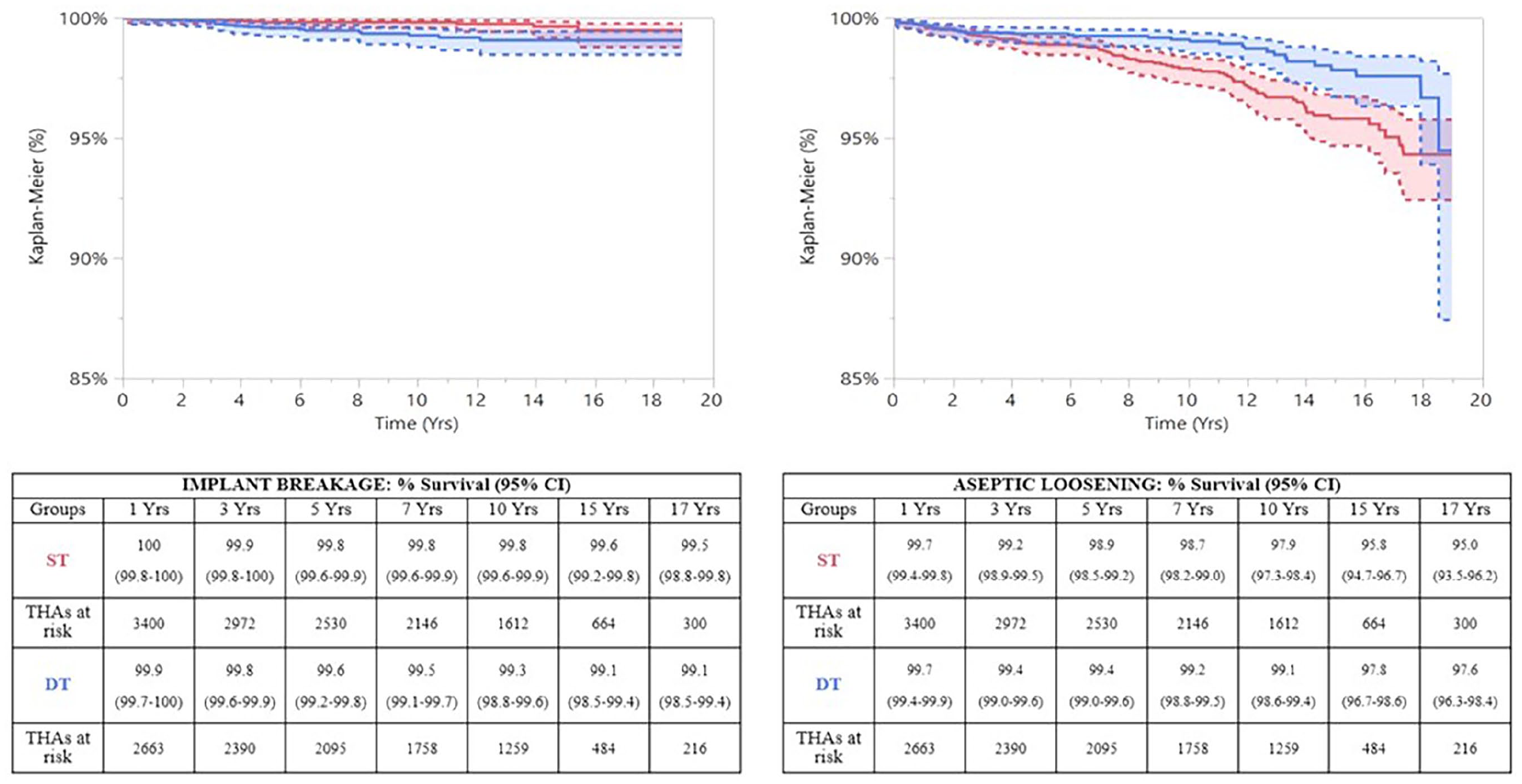
DT implants were significantly more prone to fail for implant breakage than ST, but the rate of aseptic loosening was significantly lower.
The cup choice (3D-printed cups vs. all the other sockets) did not improve survival rates (p = 0.146) and rates of cup aseptic loosening in the DT cohort (p = 0.702).
Defining the implants at higher risk for failure
The Cox regression analysis adjusted for age (65 years), gender and head size (28 mm) showed that there is no significant difference between DT and ST implants (p = 0.0596).
Most of the failures in DT implants occurred in male patients of 65 years or less and a head diameter of 28 mm or smaller. Using a Cox regression analysis adjusted for age (65 years), gender and head size (28 mm) in the DT cohort, only male gender was statistically associated with a higher risk of failure (hazard ratio [HR] 2.08; CI 95%, 1.39–3.05).
The most implanted DT stems were also analysed (Table 2). Alata Acuta Adler stems (conical tapered implants with modular necks) were more prone to stem aseptic loosening and primary instability (p = 0.0175 and p = 0.0369). Apta Adler stems (anatomical implants with modular necks) were more likely to fail due to implant breakage (p = 0.001).
The main reasons for revisions in DT stems were stratified according to the type of implant.
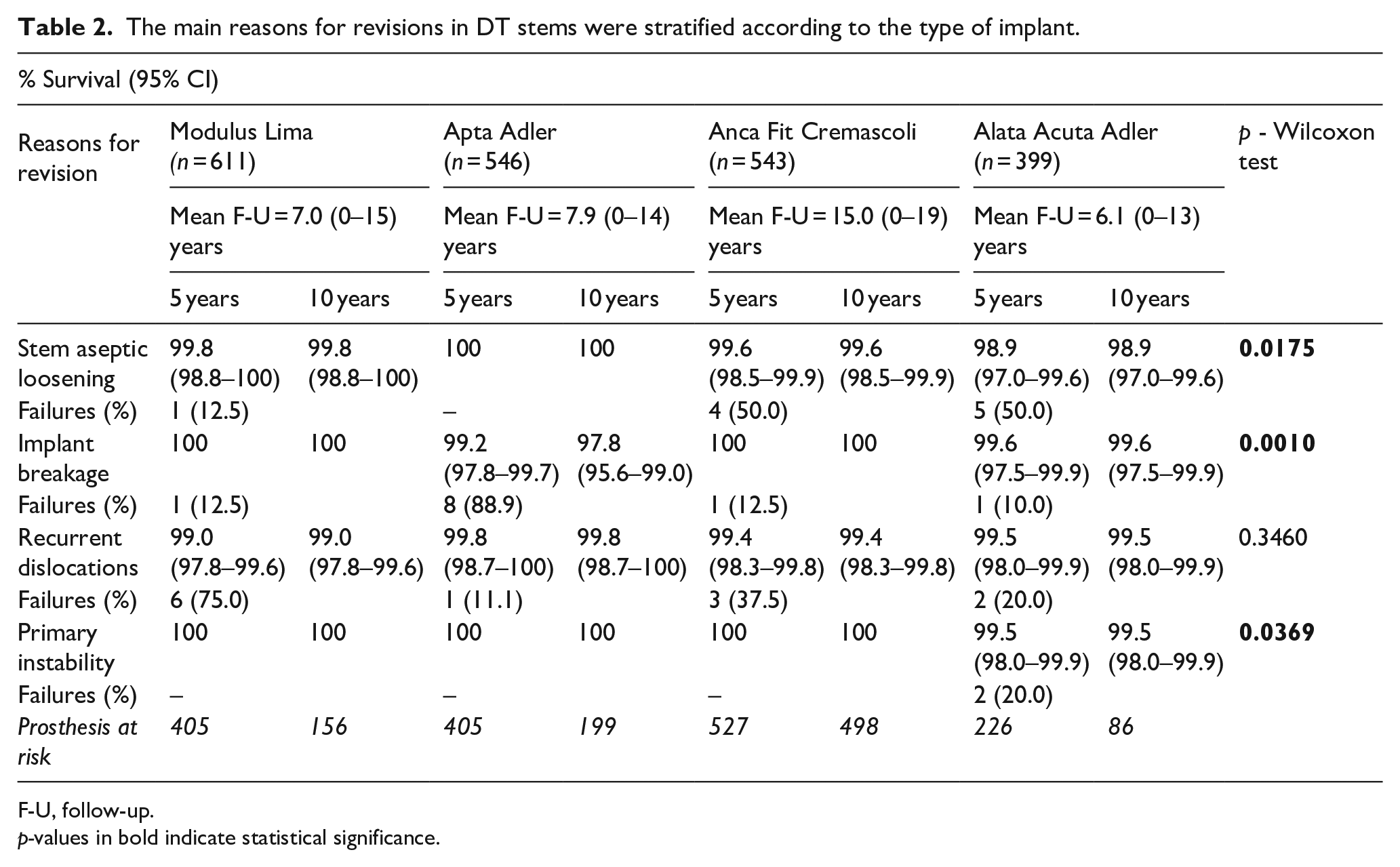
F-U, follow-up.
p-values in bold indicate statistical significance.
Discussion
Proximal femoral titanium modularity did not prove to be inferior to non-modular implants in THAs after DDH in the long-term. The DT cohort showed a lower rate of aseptic loosening, which was not dependent on the implanted cup. The rate of revisions due to implant breakage was significantly higher than in ST cohort: 0.6% at a mean follow-up of 9 years. The analysis of the failed THAs showed that young age, male gender and small head sizes impacted survival rates more than modularity, and in DT implants, younger males were more likely to undergo revision.
The current study supports the good outcomes reported in the available literature concerning titanium DT implants in DDH (Table 3).5–17 The comparative studies by Sakai et al. 5 and Kong et al. 16 reported better outcomes for DT implants than for ST implants, with low rates of dislocation and osteolysis. The current registry report confirms the good outcomes, but ascertains an analogous incidence of revisions due to dislocations or primary instability in both cohorts, similar to large case series of modular neck implants in mixed populations (DDH and non-DDH patients).18,19 While revisions due to dislocations did not seem to be reduced by modularity, the significantly lower rate of cup aseptic loosening reported in the present study is somewhat surprising. 20 Improved combined anteversion, reduced neck-cup impingement and lower stresses at the bone-cup interface due to improved proximal hip biomechanics may be advocated: 20 nonetheless, these hypotheses are merely speculative and should be assessed with proper biomechanical studies. On the other hand, implant breakages occurred in a significantly higher number of DT implants than in ST devices. The rate was quite modest (0.6%), similar to the rates reported in the literature in non-selected populations (0.5–1.1%).3,18,19 Metallosis or corrosion was not investigated in published reports on titanium modularity in DDH, nor it was evident in the current registry study (Table 3). As described in large registry studies and in comparative retrieval papers, cobalt-chrome DT implants were much more prone to revision in general: the reasons for revision were mainly due to mechanically assisted crevice corrosion.3,21,22 On the contrary, titanium modularity was at risk of fatigue failures.3,21,22
The clinical outcomes of modular stems in DDH cases were described in 13 case series up to October 2020, among them 2 comparative studies; no complications related to modularity were found.
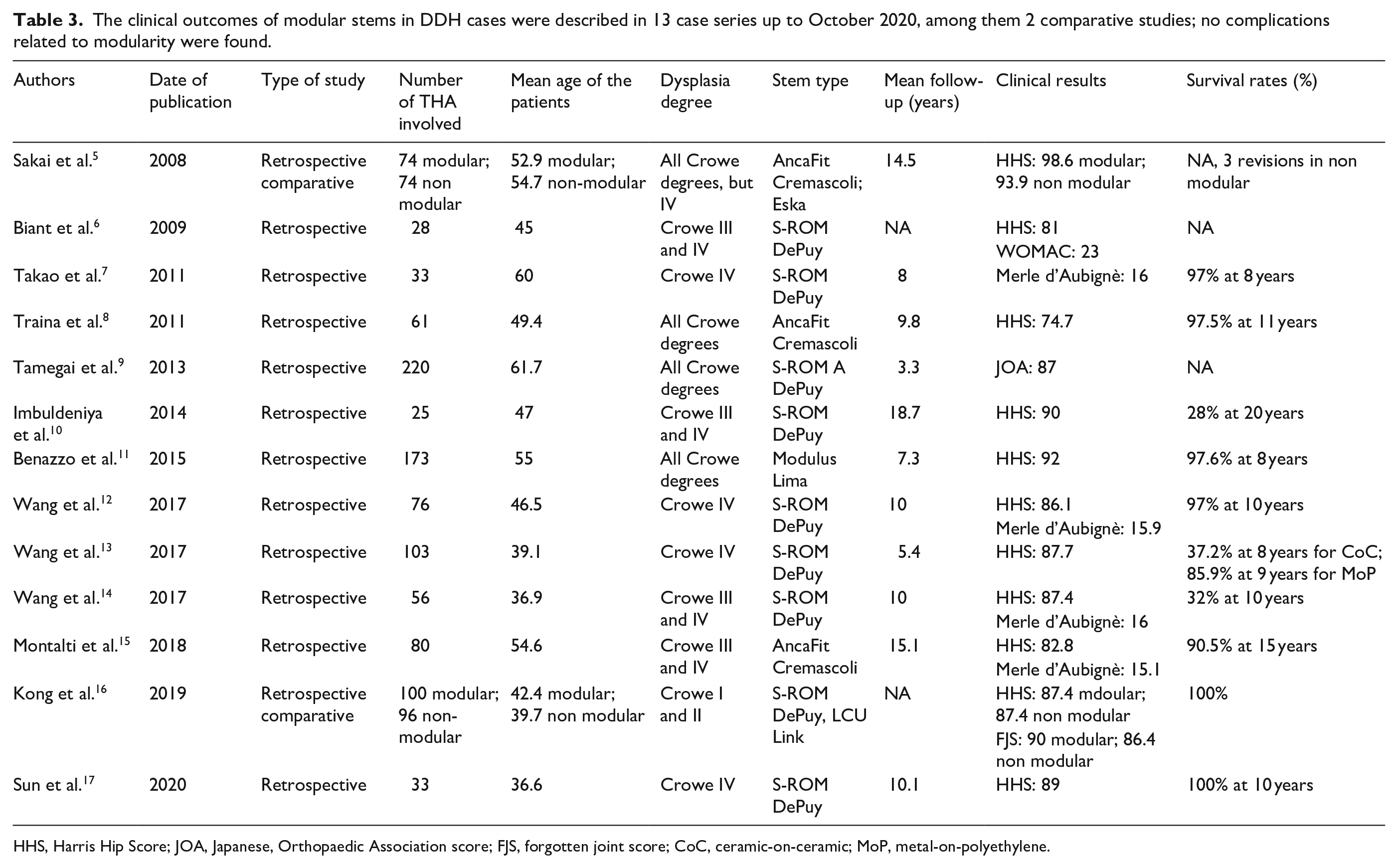
HHS, Harris Hip Score; JOA, Japanese, Orthopaedic Association score; FJS, forgotten joint score; CoC, ceramic-on-ceramic; MoP, metal-on-polyethylene.
The regression analysis highlighted that DT and ST stems did not show significant differences in terms of revision rates. Moreover, while a higher risk of revision may be applicable for younger males with small head sizes regardless of the type of implant, younger males are high-risk candidates for modularity, as demonstrated by the present report and literature findings.21,22 In the literature, many failures (mostly implant breakage) are attributed to heavier, highly active male patients with long lever arms, but specific implant features should also be considered.21,22
This study has some limitations, mainly related to the nature of the registry. Preoperative deformities and postoperative hip reconstruction could not be clinically or radiographically evaluated. Femoral shortening osteotomies could not be detected. The non-comparable demographics and implant-related features in the DT and ST cohorts could have biased the outcomes and may have been only partially controlled by the regression analysis. Conservatively-treated dislocations can not be captured by registries. The limited number of DT implant designs prevented any generalisation about breakage; moreover, 1 of the most used stems worldwide (s-ROM, DePuy, Warsaw, IN, USA), was not well represented in the report [TAB 3]. On the other hand, this study provides a comparison of large numbers at long-term, giving a clear idea of survival rates and reasons for revision (in particular, implant-related ones), which cannot be properly assessed in clinical studies without having access to thousands of cases.
In summary, proximal femoral titanium modularity did not prove inferior to ST implants or reduce the rate of revision due to aseptic loosening (and not due to dislocations), but at the price of a modest rate of implant breakage. Younger male patients may be high risk candidates for modularity, at least with some implants. Only propensity score matching in large clinical trials will provide some definitive conclusions about the use of modularity in DDH and the profile of the ideal candidate for DT implants.
Footnotes
Availability of data and materials
Data are collected from RIPO and are available online (![]() ) or at Rizzoli Orthopaedic Institute Medical Technology Laboratory. This article is a part of a larger project about stems in DDH producing a previous paper by Di Martino et al.
20
) or at Rizzoli Orthopaedic Institute Medical Technology Laboratory. This article is a part of a larger project about stems in DDH producing a previous paper by Di Martino et al.
20
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: publication of the article was financially supported by Bibliosan (Italian Ministry of Heal