
Abstract
Objective:
To evaluate the predicting value of 99mTc-hydroxydiphosphonate (HDP) pinhole bone scan in development of osteonecrosis of femoral head (ONFH) in patients with femoral neck fracture after cannulated screw fixation.
Methods:
Pinhole bone scan of patients with metallically fixed femoral neck fracture from 2001 to 2015 were retrospectively reviewed. Initial pinhole bone scan was obtained within 2–3 weeks after surgery. Findings of initial pinhole bone scan were divided in to 4 groups. Group CU included cold defect in affected femoral head, group HU with no cold defect. Group PP with increased uptake along the inserted screws and group PN with no increased uptake along the inserted screws. More than 6 months of follow-up with pinhole bone scan and clinico-radiological evidence for ONFH was reviewed.
Results:
72 patients (mean age 54.01 years, male 22, female 50) were included. 19 patients were in group CU, 53 in group HU. 60 patients were in group PP, 12 in group PN. During the follow-up, 13 patients were diagnosed as ONFH. 9 (47.36%) patients in group CU developed ONFH and 4 (7.5%) in group HU. 4 (6.66%) patients in group PP developed ONFH and 9 (75%) in group PN.
Conclusions:
To predict ONFH of femoral head followed by neck fracture, many imaging techniques with variable results were known. In this study, cold defect in early postoperative pinhole bone scans could predict ONFH, and loss of increased uptake along screw inserted site could be a strong indicative sign of ONFH. Further evaluation with a larger population is necessary.
Keywords
Introduction
After a femoral neck fracture, osteonecrosis of the femoral head (ONFH) is a serious complication. Despite the development of surgical techniques, it occurs about 15–25% of the time.1–4 Generally, most ONFH occurs within 2 years, and radiographs are useful for diagnosis from at least 6 to 24 months. 5 Early prediction of ONFH can help early performance of joint preserving surgery, such as core decompression or vascularised fibular graft (VFG), before severe joint destruction can occur. Therefore, much effort has been made to make a diagnosis and to predict ONFH onset at an early time-point. Meanwhile, ONFH is known to be caused by structural deformation due to damage to the femoral blood flow, especially in the femoral neck region.6–8 Therefore, many methods have been attempted to evaluate blood flow. It is possible to analyse femoral blood flow relatively accurately, such as a super-selective angiography, intraosseous oxygen pressure Measurement and doppler-laser haemodynamic measurement, but it has a disadvantage of invasiveness.9–11 Dynamic magnetic resonance imaging (MRI), which is seen as highly predictable, has the disadvantage of high cost, and when the technique is used after surgery, it is difficult to obtain accurate images due to interference from the instrument. 12 Efforts have been made to detect ONFH early using PET/CT and Bone SPECT/CT.13–15
Compared to these methods, the bone scan has the advantage of being non-invasive and inexpensive. Some researchers believe that a bone scan to identify a bone perfusion is necessary before surgical treatment, irrespective of whether it is for internal fixation or arthroplasty: this is because the findings of the scan can influence the choice of surgical method.16,17 However, femoral neck fractures require surgical fixation as soon as possible, and the bone scan does not show a sensitivity of more than 95% until 72 hours after the accident. 18
The authors speculated that the increased absorption around the fixed screws in the postoperative bone scan showed the possibility of preserving femoral head blood circulation and that the presence of a pin-tract sign was related to ONFH. Furthermore, ONFH was investigated, assuming that a decrease in absorption of the femoral head is likely to occur. In addition, we hypothesised that ONFH would be more likely to occur when there is a decrease in femoral head absorption (cold uptake).
Methods
Following ethical approval by our institution, we retrospectively analysed 90 cases of femoral neck fracture, who underwent closed reduction and internal fixation with screws from January 2001–December 2015. Cases were excluded from the study when the follow-up period was < 6 months, or the initial bone scan was performed after 1 month of operation.
The bone scan was performed within 2–3 weeks postoperatively, every 3 months up until 1 year, every 6 months until 2 years after surgery, and every year thereafter. A 99mTc-hydroxydiphosphonate (HDP) pinhole bone scan was performed using an intravenous injection of 20 ~ 30 mCi. After 2 hours, the bone ingestion rate of the isotope was measured with a gamma camera and a 4-mm aperture pinhole collimator was used. The imaging time was 20 minutes per bone. GE discovery millennium and Siemens symbia E models were used.
The results of the initial bone scan were divided according to 2 criteria: firstly, they were classified into a PN (pin-tract sign negative) group, without increased absorption around the pin, and a PP (pin-tract sign positive) group, when absorption was increased (Figure 1). Then, the results were classified according to the decrease in absorption of the femoral head: the HU (hot uptake) group without a decrease in femoral head absorption and a CU (cold uptake) group when there was decrease in femoral head absorption (Figure 2). The occurrence of ONFH in each group was evaluated.
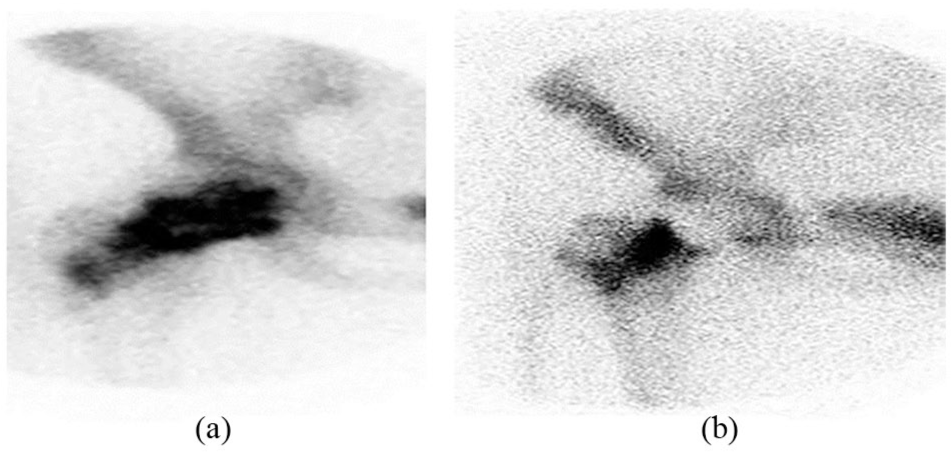
(a) The pin-hole scan shows positive pin-tract sign which hot uptake around the screws. (b) The pin-hole scan shows negative pin-tract sign which cold uptake around the screws.
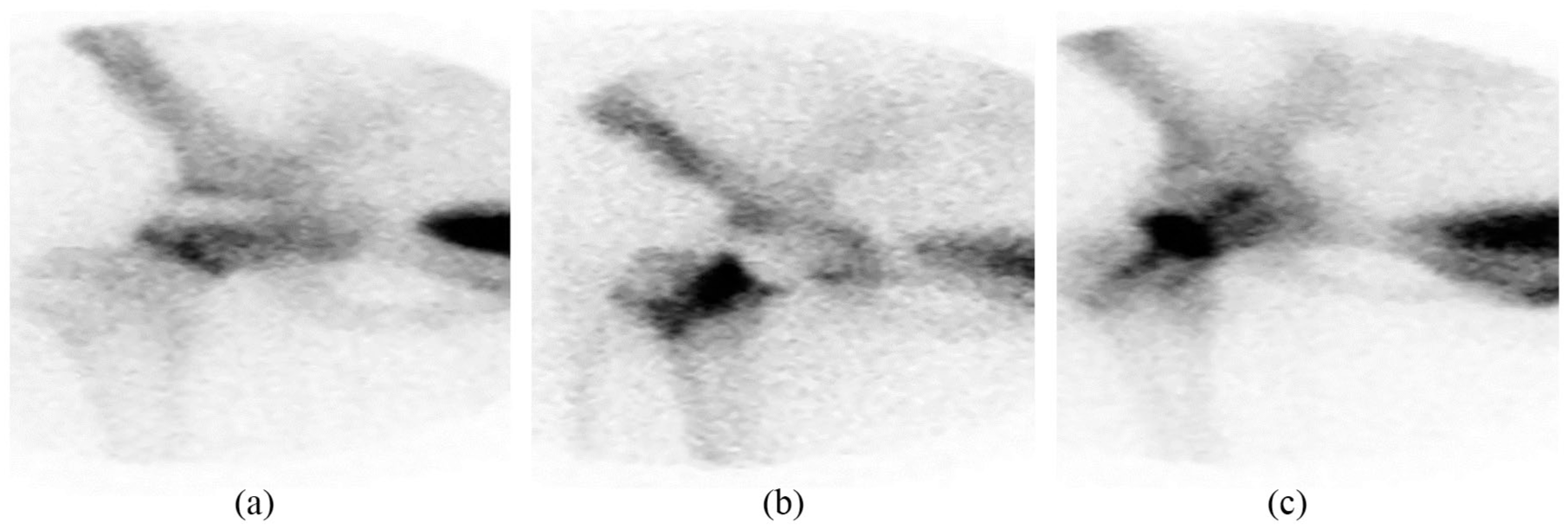
(a) The pin-hole scan shows focal cold uptake at femoral head. (b) The pin-hole scan shows diffuse cold uptake at femoral head. (c) The pin-hole scan shows no cold uptake at femoral head.
In addition, when 2 bone scan evaluation methods were applied simultaneously, pin-tract sign negative and cold-defect positive were called group A, pin-tract sign negative and cold-defect negative were called group B, pin-tract sign positive and cold-defect positive were called group C and pin-tract sign positive and cold-defect negative were called group D.
Results
Of the 90 patients in total, 14 patients who had a follow-up period < 6 months and 4 patients who had an initial bone scan at 1 month after surgery were excluded. Therefore, in total, 72 patients were analysed (Figure 3).
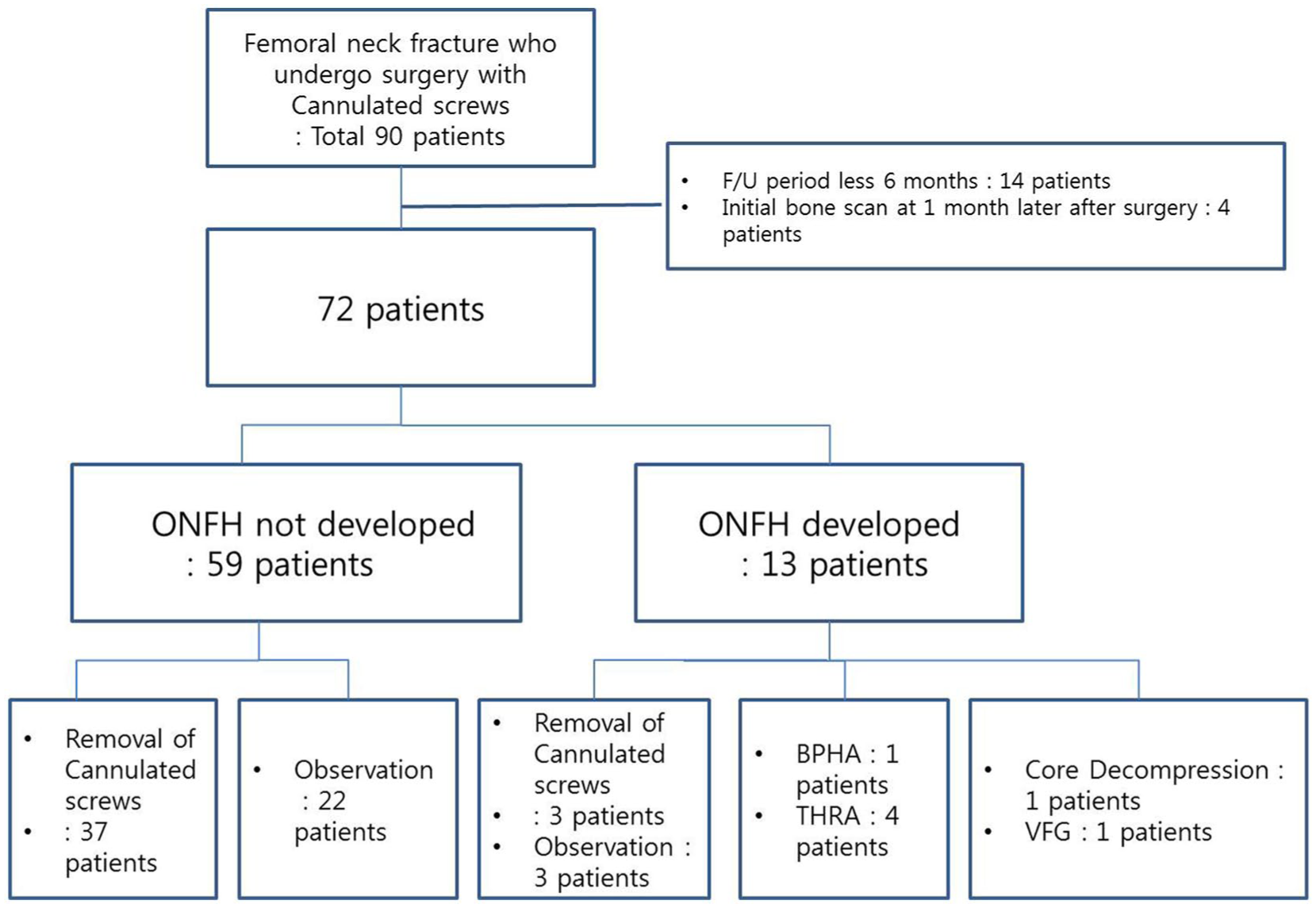
Flowchart of enrolled femur neck fracture patients.
The average follow-up period was 30.2 months (6–187 months). The mean age was 54.01 ± 3.44 (15–83) years, with 22 males and 50 females. Most of them were injured by slip down. The mean body mass index (BMI) was 21.82 ± 0.66 kg/m2 (14.24–32.04 kg/m2) and the mean bone mineral density (BMD) was −2.81 ± 0.41 (−0.9 to −5.4). According to the Garden classification, there were 25 patients with Garden stage I, 26 patients with Garden stage II, 11 patients with Garden stage III and 10 patients with Garden stage IV. The mean time from accident to surgery was 3.5 days and from visiting the emergency room to surgery was 0.88 days (Table 1).
Overall characteristics related to ONFH presence or absence.
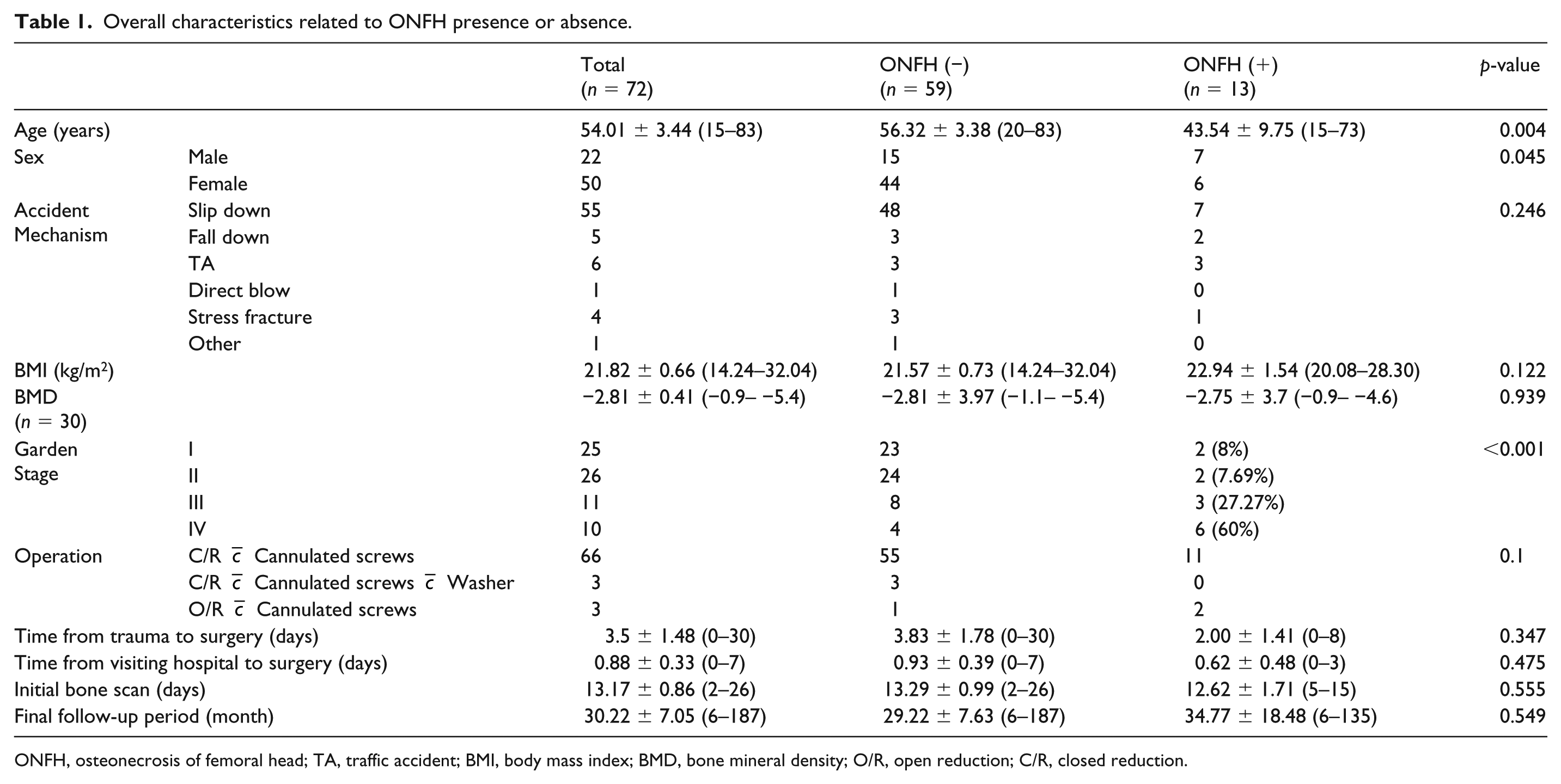
ONFH, osteonecrosis of femoral head; TA, traffic accident; BMI, body mass index; BMD, bone mineral density; O/R, open reduction; C/R, closed reduction.
Of the 72 cases, 13 cases developed ONFH. ONFH was diagnosed at average 11.4 months after the operation. ONFH occurred at a high rate in Garden stage III and IV, which is consistent with the findings of past literature.
Of the 72 cases, 53 were in the HU group and 19 were in the CU group. ONFH occurred in 4 cases in the HU group (7.54%) and 9 cases in the CU group (47.36%). Assuming that ONFH occurs when there is a cold uptake at the femoral head, the sensitivity was 69.23%, the specificity was 83.5%, the accuracy was 80.55%, the positive predictive value was 47.36% and the negative predictive value was 92.45% (Table 2).
Analysis of ONFH prediction with hot uptake or cold uptake.

ONFH, osteonecrosis of femoral head.
The PP group had 60 cases (Figure 4) and the PN group 12 cases. ONFH occurred in 4 cases of the PP group (6.67%) and in 9 of the PN group (75%). The sensitivity of the assumption that ONFH occurs when there is no pin-tract sign was 69.23%. The sensitivity is the same assuming that ONFH occurs when the cold uptake is present. However, the specificity was 94.91%, the accuracy 90.27%, the positive predictive value 75% and the negative predictive value 93.33% (Table 3).
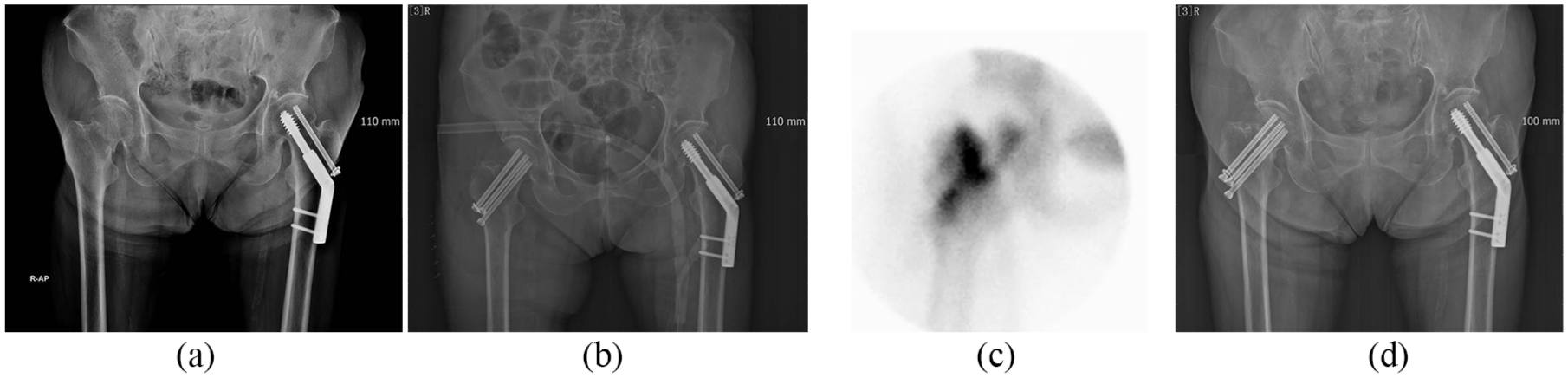
(a) and (b) 64-year-old female with femur neck (Garden stage III) fracture underwent closed reduction with cannulated screws. (c) Bone scan showed a cold uptake but positive pin-tract sign at POD 2 weeks. (d) Bone union was achieved without any complications.
Analysis of ONFH prediction with pin-tract sign.

ONFH, osteonecrosis of femoral head.
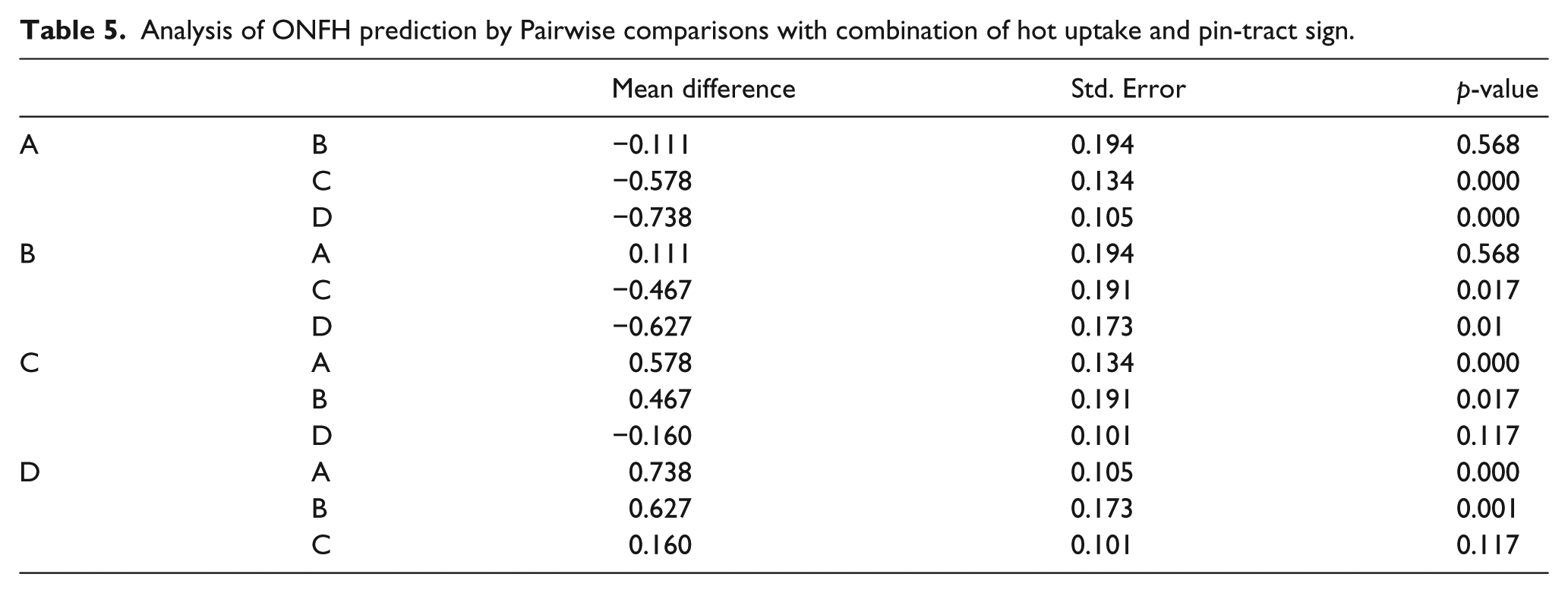
ONFH was found in 77.8% of group A, 66.7% of group B, and there was no significant difference between group A and group B. However, there was a significant difference with the other C and D groups. (A group vs. C group p = 0.01, A group vs. D group p = 0.01, B group vs. C group p = 0.017, B group vs. D group p = 0.01) (Tables 4 and 5).
Analysis of ONFH prediction with combination of hot uptake and pin-tract sign.
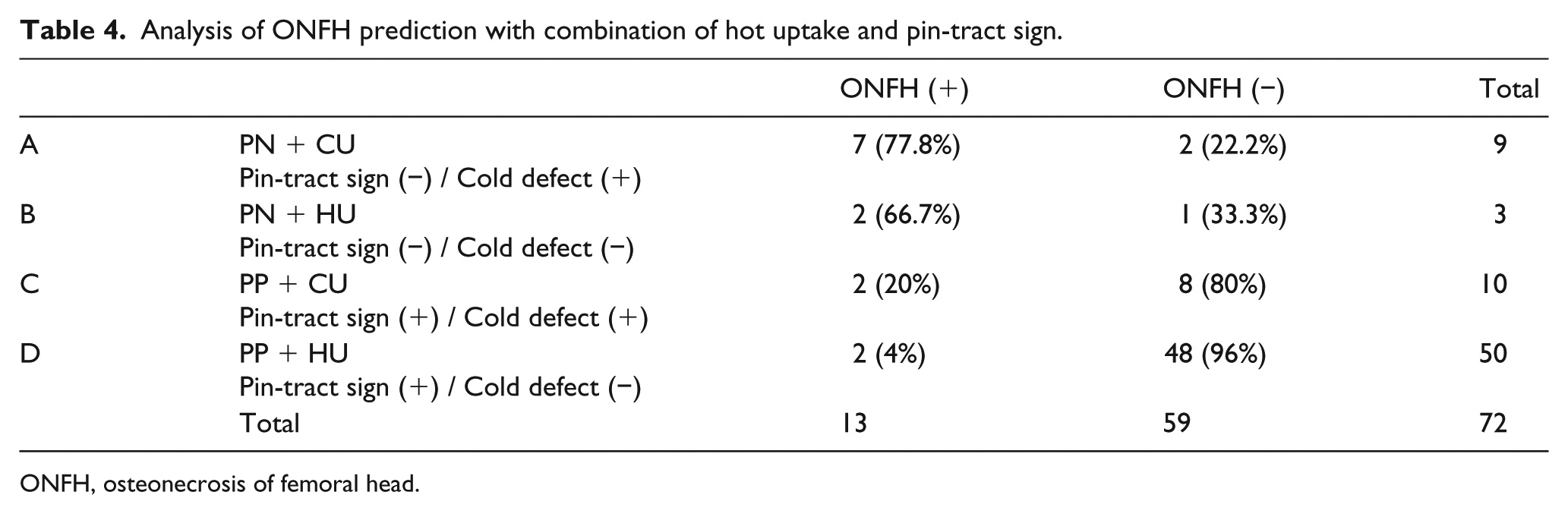
ONFH, osteonecrosis of femoral head.
Analysis of ONFH prediction by Pairwise comparisons with combination of hot uptake and pin-tract sign.
The receiver operating characteristic (ROC) curve based on the above results is as follows (Figure 5). The area under the curve (AUC) according to the hot uptake or cold uptake was 0.761 and the AUC according to pin-tract sign was 0.821. However, the AUC of the “combination” of the 2 results was the largest, 0.875. The sensitivity and specificity of the “combination” obtained through the ROC curve were 84.6% and 81.4%, respectively.
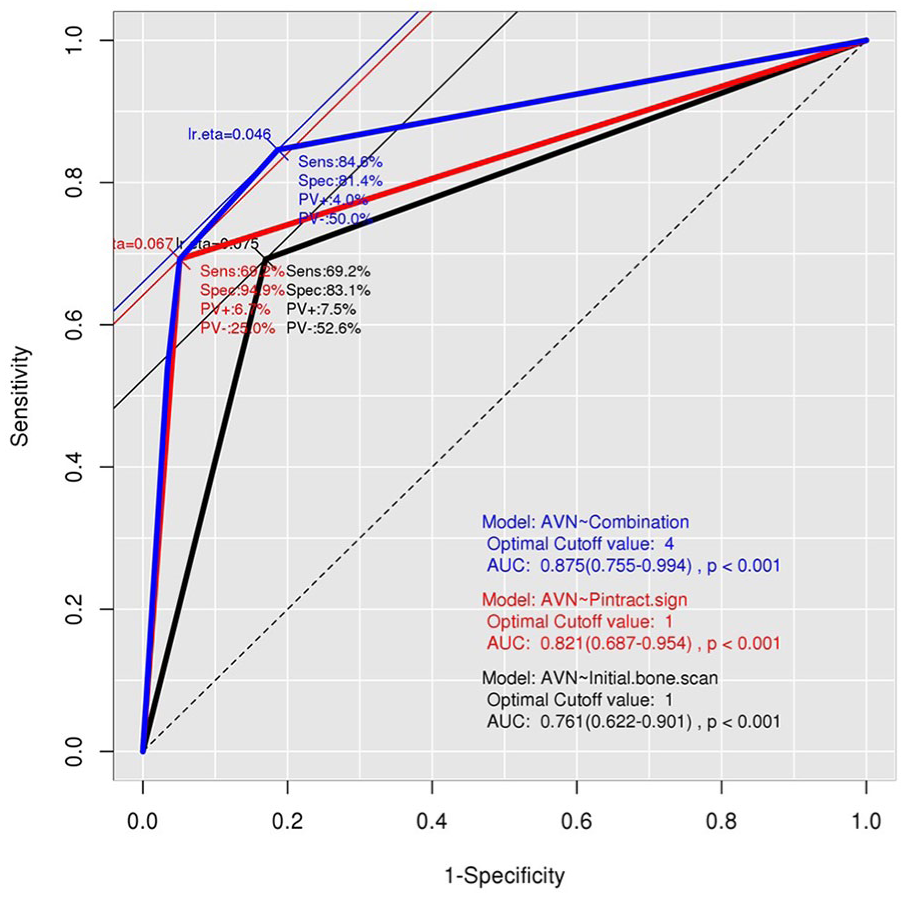
The receiver operating characteristics curve (ROC curve) based on the above results. (a) The area under the curve (AUC) according to the hot uptake or cold uptake was 0.761 and the AUC according to pin-tract sign was 0.821. However, the AUC of the “combination” of the 2 results was the largest, 0.875. The sensitivity and specificity of the “combination” obtained through the ROC curve were 84.6% and 81.4%, respectively.
Discussion
ONFH is 1 of the most important complications in femoral neck fractures and may involve several risk factors, particularly, the damage of blood flow in the femoral head and neck. The displacement of the fracture estimates the presence of vascular injury.6–8 Therefore, ONFH is seen less frequently in Garden stage I and II, without displacement, compared to Garden stage III and IV.2,19 In the present study, 27.27% and 60% of the ONFH incidence rate of Garden stage III and IV were higher than 8% and 7.69% of ONFH incidence rate of stage I and II, respectively.
However, ONFH may occur in Garden stage I and II, and ONFH may not occur in Garden stage III and IV. Therefore, various methods of evaluating and predicting whether ONFH may or may not occur have been introduced. One of them is a bone scan. The existing bone scan evaluates the overall uptake of the femoral head. However, it is not very sensitive.16,20–25 The sensitivity of 69.23% and specificity of 83.05% seen in the present study was also consistent with the previous studies. In addition, the timing of the hot uptake of the femoral head in the bone scan is not uniform, but it may be negative at first and positive during the follow-up period.25,26 This is why it is necessary to supplement it with additional measurements.
In this study, the concept of the pin-sign tract was made. Screws also cause a kind of low energy bone destruction, thus increasing the activity of osteoblasts. That is, when a bone scan is performed, it is not a hot uptake of the femoral head but a hot uptake around the fixed screw. When the pin sign tract appears, the osteoblast activity is increased along with the screw, and it is expressed as hot uptake. Therefore, it can be presumed that the blood flow to the femoral head is preserved. On the other hand, if the pin-tract sign does not appear, it can be interpreted that the blood flow to the femoral head is not good and it shows a cold uptake.
In this study, the sensitivity of the pin-tract sign as a predictor of ONFH was similar to that of conventional cold uptake, but the specificity and positive predictive value were very high. In addition, the pin-sign positive was assessed 2 weeks after surgery. Previously, we knew that ONFH predictions of bone scan would be accurate 6 months after surgery. 25 Considering the pin tract sign, early diagnosis of ONFH is higher than previous bone scan evaluation methods as well as other diagnostic methods.
Recently, there have been many studies using Bone SPECT/CT. The sensitivity is good, but specificity dropped to 49% in the early stage; specificity improved to 100% after 3 months. Therefore, it may be useful to perform Bone SPECT/CT 3 months later than the initial examination. In addition, the issue of high cost cannot be overlooked.13–15
The limitations of this study were that it was performed by a single institution and the number of cases was relatively small. There are also the disadvantages of research design due to retrospective analysis. In addition, not all patients had MRI performed and we may have failed to notice early ONFH. However, in this case, this is not significant as it does not affect the direction of treatment or prognosis. Most ONFH occurs within 2 years after femur neck fracture. 27
The most important limitation is that the average follow-up period is 30.22 months, but there are a number of patients with relatively short follow-up periods. However, it is generally known that ONFH can be confirmed from 6 months to 12 months after surgery by plain radiography. And in this study, ONFH was diagnosed by plain radiography or MRI at average 11.4 months after surgery. In addition, most of the patients who did not have any problem in radiography or clinically were follow-up lost because they obtained bone union before 1 year after surgery. This can be said to be the least likely to occur ONFH. In order to obtain accurate sensitivity and specificity, and to conduct actual clinical applications, it is necessary to support further studies with larger scale and longer research period in further studies. Nevertheless, it is meaningful that the method of adding new evaluation method concept to existing bone scan evaluation method is suggested.
Conclusion
Bone scans can be performed simply and with comparatively little cost; ONFH occurrence prediction can be done with cold uptake. At that time, the evaluation of ONFH occurrence can be more accurate by evaluating the presence or absence of the pin-tract sign. This can be confirmed as early as 2 weeks after surgery, which can be helpful in evaluating the progress of patients’ treatment and to establish later treatment methods. Further evaluation with a larger population is also necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.