
Abstract
Background:
Prior investigations have shown a decrease in periprosthetic bone mineral density (BMD) of the calcar following total hip arthroplasty (THA). The purpose of this investigation was to study proximal femur BMD in a cohort of young, active patients following THA at 1 year postoperatively using a recently introduced stem design.
Methods:
This was a prospective, IRB-approved investigation of patients with an age <65 years, BMI <35 kg/m2, and presymptomatic UCLA score of
Results:
31 patients (mean age of 52.6
Conclusion:
This study demonstrates the maintenance of medial calcar bone density at 1 year postoperatively in young, active patients undergoing THA. Further longitudinal analysis of this stem design is necessary to elucidate the significance of this finding.
Introduction
The utilisation of total hip arthroplasty (THA) in the United States continues to rapidly increase with patients <65 years of age constituting the fastest growing subset of patients seeking THA.1,2 However, as younger, more active patients continue to seek THA, the longevity of these implants continues to be scrutinised. The primary mode of failure following THA remains aseptic loosening, 3 with periprosthetic bone loss and bone resorption recognised as contributing factors. 4 Periprosthetic bone loss is known to increase the risk of aseptic loosening, component migration, periprosthetic fracture, and pain.4,5 Following THA, femoral bone resorption can occur secondary to decreased load transfer through the metaphyseal region and implant-specific stress shielding. 6 This decreased area of proximal implant-bone support increases the potential for late failure, periprosthetic fracture, and potentially thigh pain.
The measurement of periprosthetic bone mineral density (BMD) is a useful tool to determine the area of implant fixation and physiologic load transfer following THA. Femoral stem design is known to impact the degree of stress shielding, with stem material, stem size and modulus of elasticity, mode of fixation, design and geometry all influencing the change in periprosthetic bone density. 7 Prior investigations have shown stiffer, larger, noncemented, cobalt-chromium stems to increase the occurrence of stress shielding.8–10 However, additional investigations studying the use of titanium, proximally coated stems designed to engage the metaphysis have consistently shown periprosthetic bone loss over time with the medial calcar most affected.6,7,11,12 Thus, even advancements in stem material, design, and geometry have failed to restore a physiologic load transfer through the medial calcar following THA.
The continued investigation of stem design and its impact on proximal femur bone density remains crucial as it provides insight into potential etiologies of persistent pain and also design modifications that could lead to a more physiologic stress transfer, bone preservation, and potentially improved implant longevity. The purpose of this investigation was to study proximal femur BMD in a cohort of young, active patients following THA at one year postoperatively using a recently introduced stem design.
Methods
This study was a prospective, IRB-approved investigation performed at a single institution. Between January 2014 and May 2015 patients were enrolled in a single cohort, prospective evaluation designed to study the use of a modular, dual mobility acetabular prosthesis (Modular Dual Mobility, Stryker Orthopaedics, Mahwah, NJ, USA) in young, active patients. All patients in this study received a titanium, proximally coated, tapered cementless femoral stem (ACCOLADE II, Stryker Orthopaedics, Mahwah, NJ, USA). The femoral prosthesis used has several design modifications different from its predecessor. It was designed using a large computed tomography database with an anatomy analysis tool to try to enhance the fit in the femur such that the stability of the stem is maintained compared to the previous generation despite being shorter. The design rationale has been described in a prior publication. 13 The Accolade II stems feature a size specific medial curvature, a proportional incremental stem growth across size range, a modest reduction in stem length, and an increased distal taper. In addition, the stem material was changed from TMZF to titanium alloy, while the proximal hydroxyapatite coating was retained. It was hypothesised that these design changes would lead to an improved implant fit as well as reduction in stem micromotion. A subset of these patients agreed to receive additional imaging studies to evaluate the impact of this stem design on proximal femur bone mineral density. All patients provided informed consent prior to study inclusion.
Inclusion criteria for this study were patients between the ages of 18 and 65, with a body mass index of
Periprosthetic BMD was measured using dual energy X-ray absorptiometry (DEXA; Discovery A model; Hologic, Bedford, MA, USA). DEXA is a well-validated method to assess BMD in patients who have undergone THA.16,17 The same technician obtained scans and measurements at 6 weeks, 6 months, and 1 year postoperatively using the same template each time for the patient, and standard foot and knee supports. Prosthetic hip software (Hologic) was used to measure BMD in the 7 Gruen zones of the femur 18 (Figure 1). The 6-week BMD values were used as the baseline to calculate the percent change in BMD at 6 months and 1 year as previously reported.9,19,20 Prior reports have used a preoperative BMD measurement as the “baseline” measurement for comparison, 21 but we believe an early postoperative baseline measurement is more accurate given the sensitivity of the DEXA-analysis software to changes in the template area to be measured along with bone removed during the actual procedure. Comparison of DEXA images preoperatively to postoperatively (after component implantation) is unreliable due to loss of some of the preoperative bony landmarks for template standardisation. Furthermore, the metal implant can distort the actual quantity of bone to be measured, and use of a preoperative BMD measurement as the baseline overestimates the change in BMD and stress shielding postoperatively. 22 Therefore, the 6-week postoperative BMD measurement was used as the “baseline” value in this investigation.
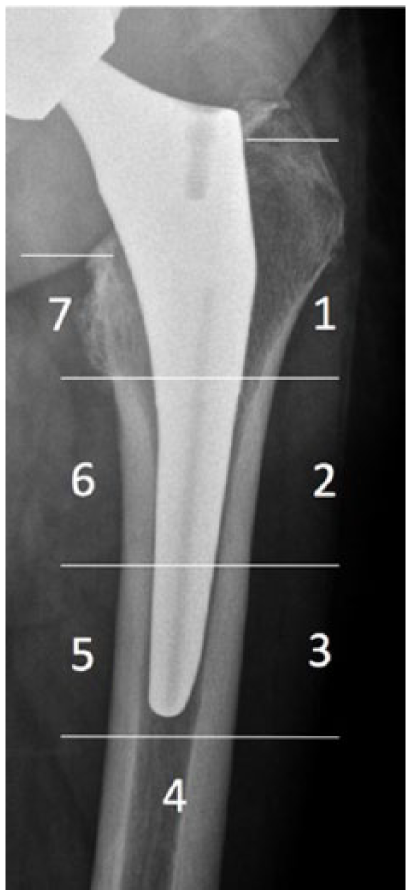
Radiograph demonstrating the 7 Gruen zones where bone mineral density measurements were performed in patients undergoing total hip arthroplasty.
All patients were also asked to complete a previously described pain-drawing questionnaire (Figure 2).
23
The questionnaire asked participants to identify whether or not they experienced pain in 8 anatomical areas of interest: groin, anterior thigh, lateral thigh, posterior thigh, buttock, lower back, trochanteric region, and the knee. Pain intensity was rated using a pain scale scored from 0 to 5, with 0 being “no pain,” and 5 being “pain that wakes you up at night, or pain all the time.” Patients reporting scores between 2 and 5 were considered to have “moderate to severe” symptoms. For comparison, patient-reported pain in this investigation was compared to a previously published study assessing the incidence and location of pain in patients undergoing primary THA meeting the same inclusion criteria.
23
In this prior investigation, patients received one of 3 cementless, titanium, proximally coated and tapered stems (Synergy, Smith and Nephew Inc., Memphis, TN, USA; Anthology, Smith and Nephew Inc., Memphis, TN, USA; Versys Fiber Metal Taper, ZimmerBiomet Inc., Warsaw, IN, USA) and were evaluated at a mean of 2.9
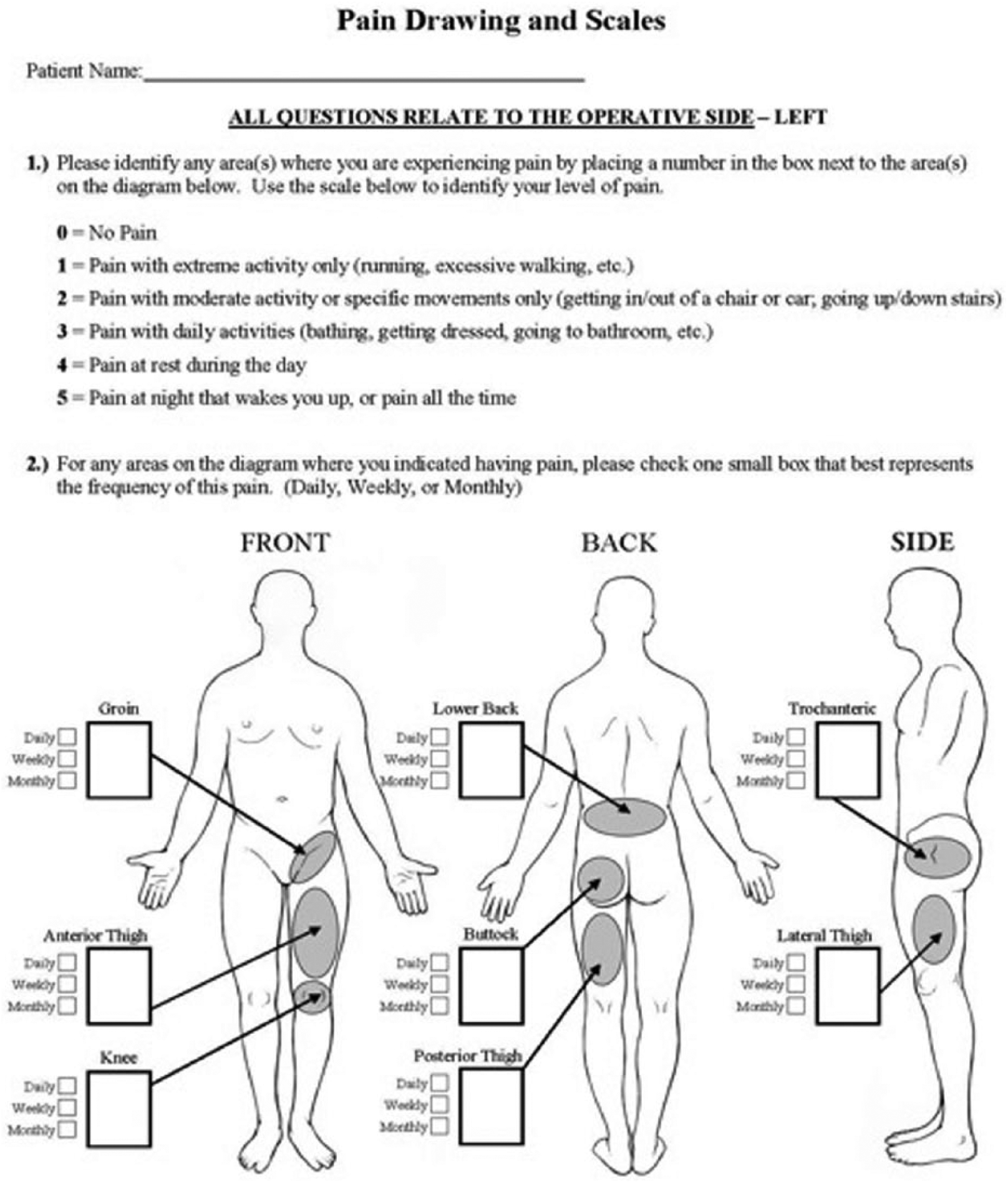
The pain drawing questionnaire completed by study participants.
Statistical analysis
Baseline demographics and clinical scores were reported using descriptive statistics. To examine the change of BMD during the study period (6-week, 6-month, 1-year), a mixed model with repeated measures was constructed. Compound symmetry covariance structure was used when taking into consideration with-subject correlations. Age, gender, body mass index (BMI), and UCLA activity level were included in the model as important adjustment covariates. Comparisons of patient-reported pain were performed using Chi-square or Fischer’s Exact test analyses. All tests were 2-sided. SAS 9.1 (SAS Institute Inc., Cary, NC, USA) was used for all statistical procedures.
Results:
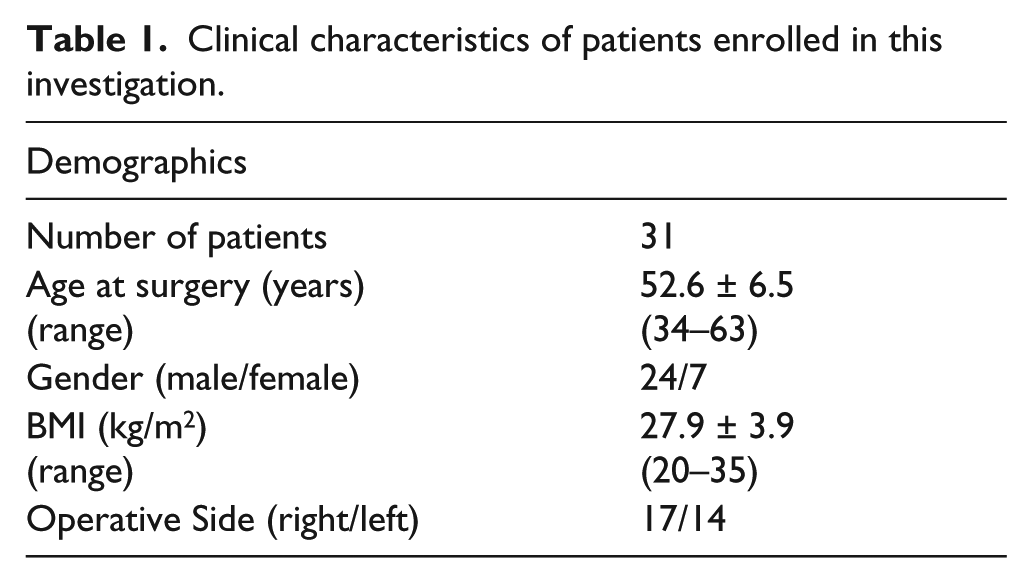
To date, 31 patients (31 THAs) have been prospectively enrolled in this investigation and received DEXA scans at 6 weeks, 6 months, and 1 year postoperatively. The average age of patients was 52.6
Clinical characteristics of patients enrolled in this investigation.
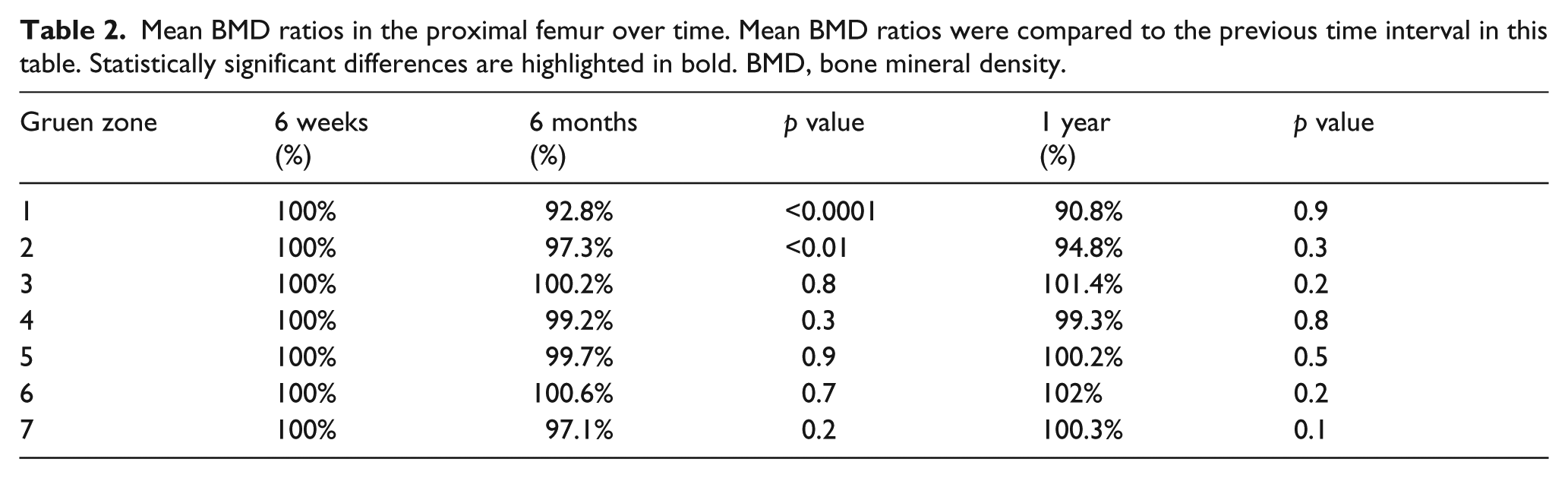
The mean BMD ratios for each Gruen zone in our cohort of patients are presented in Table 2. The mean BMD ratio was decreased at the 6 months and 1 year interval in Gruen zones 1 and 2, although the decrease between the 6 months and 1 year interval did not reach statistical significance. The mean BMD ratio was maintained in Gruen zones 3 thru 7 at both the 6 months and 1 year intervals. In Gruen zone 7 (medial calcar), there was a non-significant decrease in BMD ratio at 6 months, but at 1 year the BMD in this region was maintained at 100% of the baseline level. There was no correlation in proximal femur BMD over time with age, gender, UCLA activity level, or BMI.
Mean BMD ratios in the proximal femur over time. Mean BMD ratios were compared to the previous time interval in this table. Statistically significant differences are highlighted in bold. BMD, bone mineral density.
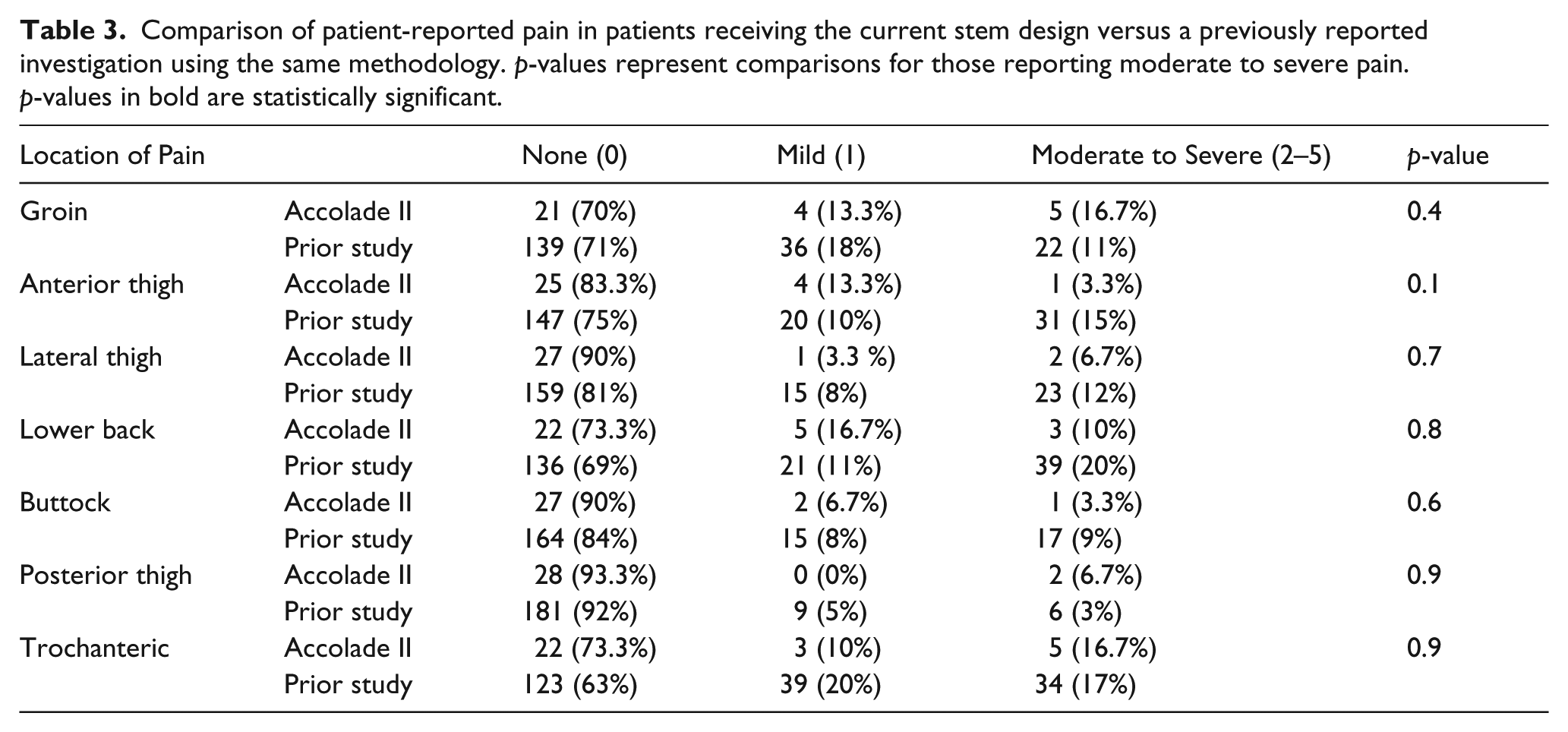
Thirty patients completed the pain-drawing questionnaire. Patients most commonly reported the presence of moderate to severe pain in the groin (16.7%) and trochanteric region (16.7%). Only one patient (3.3%) reported moderate to severe pain in the anterior thigh and 2 patients reported moderate to severe pain in the lateral thigh (6.7%). With this limited data, the percentage of patients reporting pain in these regions was less compared to the previously published investigation (15% and 12%, respectively), although these values did not reach statistical significance (Table 3).
Comparison of patient-reported pain in patients receiving the current stem design versus a previously reported investigation using the same methodology. p-values represent comparisons for those reporting moderate to severe pain. p-values in bold are statistically significant.
Conclusion
A number of investigations have analyzed periprosthetic bone mineral density of the proximal femur following THA,6–10 but to our knowledge few have specifically studied this in a cohort of young, active patients. 12 Younger age and increased activity have both been associated with increased patient-reported pain and symptoms following THA.23,24 Thus, it is important to analyze potential factors that could contribute to patient satisfaction in this growing subset of patients. While it remains difficult to synthesise the findings of prior studies analyzing proximal femur BMD due to heterogeneity of their study populations and differences in stem designs, one consistent finding is that implantation of a THA leads to decreased periprosthetic BMD postoperatively. In a systematic analysis, Knutsen et al. found the greatest bone loss to occur in the calcar region (Gruen zone 7) even with the use of a titanium alloy, proximally coated cementless stem design. 7 The preliminary results of this investigation demonstrate the maintenance of medial calcar bone density at 1 year postoperatively in a cohort of young, active patients following THA using a recently introduced stem design. While the clinical impact of this finding on component survivorship and clinical symptoms has not been elucidated, to our knowledge this is the 1st study to report maintenance of BMD in the calcar region suggesting the presence of a more physiologic stress transfer through this region.
This study has several limitations that must be recognised prior to interpretation of our results. 1st, a DEXA scan was used to quantify BMD in this investigation, which may be of concern in the presence of a metal implant. 16 However, prior studies have utilised this technique and shown a low degree of variation between repeat measurements and a low coefficient of variation.16,17,25 Furthermore, variability was reduced in this study by using the same DEXA scanner, the same technician to perform the scans, and the same template to measure bone density for the scans. 2nd, the size of this prospective cohort is relatively small, and thus these results should be considered preliminary. However, it is important to report the early results of a recently introduced prosthesis to ensure there are not unexpected findings of significant stress shielding or component loosening. 3rd, as our investigation focused on changes in BMD and the potential of stress shielding, we are unable to elucidate the clinical impact of these alterations of BMD on patient-reported outcomes and satisfaction. The clinical impact of alterations in proximal femur BMD continues to be an area of further investigation, but one can infer that maintenance of BMD in the calcar region would be a positive finding. 4th, long-term follow-up is necessary to determine whether these findings of periprosthetic BMD are maintained, and this cohort of patients will obtain further imaging at both 2-year and 5-year postoperative intervals to address this concern. Lastly, it is important to note that only young, active patients were included in this investigation based on our strict inclusion criteria. Thus, the generalisability of this study’s results to other patient populations may be limited and should be applied with caution.
Periprosthetic bone loss following THA, whether from osteolysis or stress shielding, remains a major concern due to the potential complications of loosening, component migration, periprosthetic fracture, and pain. 7 Furthermore, a reported late sequela of proximal stress shielding and more distal loading of the femoral component includes stem fracture. While historically the issue of stress shielding was believed to be a phenomenon of the use of fully porous-coated, cobalt chrome femoral prostheses, 10 recent investigations have highlighted periprosthetic bone loss to occur even with the use of a proximally coated, titanium, cementless prosthesis. 11 Freitag et al. demonstrated a decrease in BMD of 17.2% after short stem (Fitmore; Zimmer, Winterthur, Switzerland) and 16.7% after straight stem (CLS; Zimmer, Winterthur, Switzerland) implantation at 1 year postoperatively in the medial calcar following THA. 6 In a similarly designed study of 45 THAs receiving a cementless femoral stem of one of 3 designs (Synergy, Smith and Nephew Inc., Memphis, TN; Anthology, Smith and Nephew Inc., Memphis, TN; Versys Fiber Metal Taper, ZimmerBiomet Inc., Warsaw, IN), Nam et al. demonstrated a consistent decrease in periprosthetic BMD in Gruen zones 1, 2, and 7 at up to 5 years postoperatively, with the greatest decrease occurring in the medial calcar (zone 7; 89.2% of baseline at 5 years). 12 Although the clinical significance of decreases in BMD must be elucidated, a significant proportion of these patients also reported persistent pain in the anterior (15%) and lateral thigh (12% – Table 3). Of note, this prior study by Nam et al. used the same pain-drawing questionnaire and same patient inclusion criteria as used in this study. Prior investigations have noted a similar incidence of reported thigh pain after the use of a cementless femoral prosthesis. MacDonald et al. noted the incidence of thigh pain to be 9% in patients receiving a proximally coated cementless stem versus 6% in those receiving a fully coated cementless stem. 26 In addition, Kinov et al. in a retrospective review of 98 THAs who received a proximally coated cementless femoral component found 13% to report thigh pain postoperatively. 27 In contrast, patients in the current investigation with preserved medial calcar bone density demonstrated a decrease reporting of anterior (3.3%) and lateral (6.7%) thigh pain, although it must be emphasised that these results are preliminary and based on a small cohort of patients. Although the occurrence of stress shielding can be attributed to a number of variables including activity level, implant design, stem material, stiffness, geometry, and surgical technique, 26 the long term consequence of this phenomenon remains a concern considering the evolving demographics of patients undergoing THA. In contrast, prior studies have noted surface replacement arthroplasty to maintain proximal femur bone density including a more physiologic load transfer.12,28 Thus, the preliminary results of the current study demonstrating preserved medial calcar BMD at 1 year and the potential for decreased thigh pain warrants continued investigation.
In conclusion, to our knowledge this investigation is the 1st to present a femoral stem design demonstrating preservation of proximal femur BMD in the medial calcar following THA. It is important to take into consideration the aforementioned limitations of this investigation including the strict inclusion criteria used for enrollment in this study. In addition, it must be emphasised that the clinical relevance of preserved proximal femur BMD and whether this finding will persist over time must still be elucidated. However, this study indicates that stem design does have the ability to impact periprosthetic femoral bone density and that maintenance of calcar bone stock should be the goal of prosthetic designs and is potentially achievable. While this data remains preliminary, information from this investigation will prove useful in identifying specific design modifications that may aid in creating a more physiologic stress transfer postoperatively. Future investigations will focus on following periprosthetic BMD with the use of this prosthesis while also attempting to identify the impact of alterations in proximal femur BMD on clinical outcomes and satisfaction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: One author (RLB) is a paid consultant and has received research support from Stryker Inc. (Mahwah, NJ, USA) whose products are studied in this investigation.
Research support for this investigation has been provided by Stryker Inc. (Mahwah, NJ, USA).