
Abstract
Purpose
To evaluate the Intrastromal corneal ring segment (ICRS) implantation for visual rehabilitation in pediatric patients with keratoconus.
Methods
Patients aged ≤18 years with keratoconus who underwent ICRS implantation were included. Uncorrected (UDVA) and corrected (CDVA) distance visual acuities, manifest refraction and keratometry were recorded preoperatively and at 1–5–7– and 10–year postoperatively. Treatment was categorized as success, qualified success or failure based on short-term visual and refractive improvement, the visual and refractive stability and the comparison between the long-term follow-up and the preoperative.
Results
One hundred seven eyes (85 patients) were included. All eyes were examined 1 year postoperatively, 89 at 5 years, 69 at 7 years and 36 at 10 years. UDVA (logMAR) changed from 0.64 ± 0.38 preoperatively to 0.34 ± 0.24 one year postoperatively (P < 0.0001). CDVA (logMAR) rose from 0.19 ± 0.15 to 0.08 ± 0.08 (P < 0.0001). No eyes lost lines of CDVA 1 year postoperatively compared to preoperative, and 74.8% of the eyes gained lines. Preoperatively, 61.7% of the eyes had a refractive cylinder ≥3.00 D; one year postoperatively, 76.6% had <3.00 D. The treatment was successful in most cases at 5–, 7– and 10–year follow-ups (84.3%, 85.5%, and 88.9%, respectively), qualified success in around 8% of the eyes, and treatment failed in 6 eyes represented a cumulative rate over the 10 years <10%
Conclusion
ICRS implantation induced significant visual and refractive improvements, and in most eyes with available long-term follow-up, visual and refractive improvements were maintained, supporting ICRS as a long-term visual rehabilitation option in pediatric keratoconus.
Introduction
Keratoconus in the pediatric population poses a greater challenge than in adults. Firstly, younger age is associated with a higher risk of progression due to reduced corneal biomechanical stiffness. The risk of disease progression increases the risk of requiring a keratoplasty for visual rehabilitation.1–3 Furthermore, the inverse correlation between age and keratoconus severity at the diagnosis moment4–8 may imply a significant patient's visual quality degradation; however, baseline severity does not invariably predict subsequent visual deterioration.
Corneal crosslinking (CXL) is a widely accepted treatment to halt or slow down the progression of keratoconus,9,10 although its effectiveness seems to decrease in pediatric patients. The long-term studies of CXL in pediatric keratoconus, which reached a follow-up of 5 years or more, reported a progression rate range between 0–34%.11–20 Hence, CXL is effective in halting or slowing down the disease progression in most pediatric patients. However, it is worth noting that the CXL aims to arrest the progression of keratoconus, not to reshape the corneal morphology deformed by the disease. Hence, visual rehabilitation is limited in most cases. Therefore, a significant improvement in the visual quality and refractive parameters should not be expected after treatment. Consequently, many patients may require contact lenses for optimal visual quality, and issues related to tolerance, handling, and potential complications must be carefully monitored.21–23 Furthermore, any disease progression involving an increase in astigmatism, keratometry or decrease in visual acuity over time could worsen the visual performance compared to preoperatively.
Intrastromal Corneal Ring Segment (ICRS) implantation primarily aims to regularize corneal morphology to enhance visual quality. Hence, contrary to CXL, the treatment will be successful if patients experience improvement in visual and refractive parameters after surgery. Its effectiveness for this purpose has been demonstrated, proving its viability in improving the patient´s visual quality. 24 However, there is controversy about the stability of this procedure over the long term, with some studies reporting stable results25–31 while others report instability.32–34 Specifically in the pediatric population, only two previous studies reached an extended follow-up.25,32 Hence, a critical issue in assessing the effectiveness of ICRS implantation is whether the visual and refractive improvement induced by ICRS implantation persists over time, how much improvement persists (total, partial, or none), and for how long.
In this study, we analyzed all pediatric keratoconus patients who underwent ICRS implantation from December 2008 to December 2018, ensuring that that, in December 2023 (data-collection date), patients had a minimum potential follow-up of 5 years and a maximum of at least 10 years, aiming to quantify 12-month visual and refractive changes after ICRS in pediatric keratoconus and assess maintenance at 5, 7, and 10 years.
Patients and methods
This longitudinal retrospective study included keratoconus patients aged 18 years or younger who underwent Ferrara-type ICRS implantation (AJL Ophthalmic, Spain) from December 2008 to December 2018. That criterion implies that in December 2023 (data-collection date), patients had a minimum potential follow-up of 5 years and a maximum of at least 10 years (those who underwent surgery between December 2008 and December 2013). The study was carried out at the Fernández-Vega Ophthalmological Institute in Oviedo, Spain. The tenets of the Declaration of Helsinki were followed, and full ethical approval from the Institute was obtained. Written informed consent for surgery and enrollment in the study was obtained from the parents after receiving a complete description of the nature of the study and the possible consequences of surgery.
Inclusion criteria were pediatric patients diagnosed with keratoconus, contact lens intolerance (discomfort or inability to continue wearing contact lenses), a clear cornea, and a minimum corneal thickness of over 400 µm at the optical zone involved in the implantation (a general criterion for surgery). The exclusion criteria defined for the study were patients who had keratoconus stage IV (according to Amsler-Krumeich classification), previous corneal or intraocular surgery, a history of herpetic keratitis, a diagnosed autoimmune disease or a systemic connective tissue disease. Patients undergoing any other ocular procedure were excluded from the analysis.
A complete ophthalmologic examination was performed on all patients before surgery, including uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA), manifest and cycloplegic refractions, keratometry, corneal topo-tomography (Pentacam, Oculus Optikgerate GmbH/ Sirius, CSO; the same device was used in each patient over the follow-up), anterior segment optical coherence tomography (Visante Zeiss-Meditec), endothelial cell count, ultrasonic pachymetry, slit lamp microscopy, Goldmann applanation tonometry, and binocular indirect ophthalmoscopy. Contact lens use was discontinued 1 month prior to corneal topography.
All eyes in this study received Ferrara-type ICRS (AJL Ophthalmic, Spain) implants made of polymethyl methacrylate and have a triangular cross-section that induces a prismatic effect on the cornea. The optical diameter of the ICRS was 5.0 mm (AFR5) with a base of 0.6 mm, or 6.0 mm (AFR6) with a base of 0.8 mm, available in variable thicknesses (0.15 mm to 0.30 mm, increasing in 0.05 mm increments) and with arc lengths of 90, 120, 150 and 210 degrees.
The protocol for ICRS implantation was first to classify the keratoconus morphology according to the five morphology phenotypes described previously. 35 Subsequently, the ICRS were implanted following the nomogram used in previous studies in each morphology phenotype36–40 (Supplementary Table 1 outlines the nomogram for each phenotype). Two experienced surgeons performed all implantation procedures (J.F.A.; C.L.). The tunnel was created at 70% of the corneal thickness, using a 60-KHz infrared neodymium glass femtosecond laser (IntraLase femtosecond laser FS60; Advanced Medical Optics, Inc) with a power of 5 mJ and employing the procedure described in previous studies.36–40 Surgery was performed under general anaesthesia in patients younger than 14 years and topical anaesthesia in patients 14 years old or older.
The clinical measurements analyzed included manifest refraction, slit-lamp biomicroscopy, UDVA, CDVA, and corneal topo-tomography. The manifest refraction was analyzed using the power vector method proposed by Thibos and Horner. 41 The variables were examined preoperatively and at 1-5-7- and 10-years postoperatively.
We conducted a case-by-case analysis to evaluate whether the visual and refractive changes induced by ICRS remains over time. To this extent, we established specific criteria to define successful treatment and applied them to each case at each visit. Below is the detailed analysis protocol followed.
First, we defined postoperative visual and/or refractive instability as the presence of at least one of the following criteria compared to the previous visit:
An increase of at least 1.5D steep K. An increase of at least 1.5D in the topographic or refractive astigmatism. A decrease in CDVA greater than 1 line.
Next, the treatment success was categorized into three levels:
- Success: The 1-year visual and/or refractive data improved compared to preoperatively and remained stable between visits (that is, absence of any of the postoperative visual and/or refractive instability criteria) - Qualified success: The 1-year visual and/or refractive data improved compared to preoperatively; however, there was postoperative instability between visits (that is, the presence of at least one postoperative visual and/or refractive instability criterion). However, the visual and refractive data remained better than preoperatively, confirmed by:
CDVA and refractive astigmatism remained equal to or better than preoperatively. CDVA is better than preoperatively, and refractive astigmatism is not higher than 1.5D compared to preoperatively. - Failure: A keratoplasty was performed during follow-up or if there was instability and the CDVA was worse than 1 line than preoperatively or refractive astigmatism higher than 1.5D that preoperatively without improvement in CDVA.
Data analysis was performed using SPSS for Windows, version 14.0 (SPSS Inc., Chicago, IL). Linear mixed-effects models were fitted including all available observations across time points to account for inter-eye correlation when both eyes were included. Time was treated as a categorical variable and a random intercept for patient was included in the model. Mean values and mean differences with 95% confidence intervals (CI) were reported. Pairwise comparisons between visits were performed using estimated marginal means with Bonferroni correction. Differences were considered to be statistically significant when the P value was <0.05. Descriptive statistics at each follow-up visit were calculated using the eyes available at that specific time point.
Results
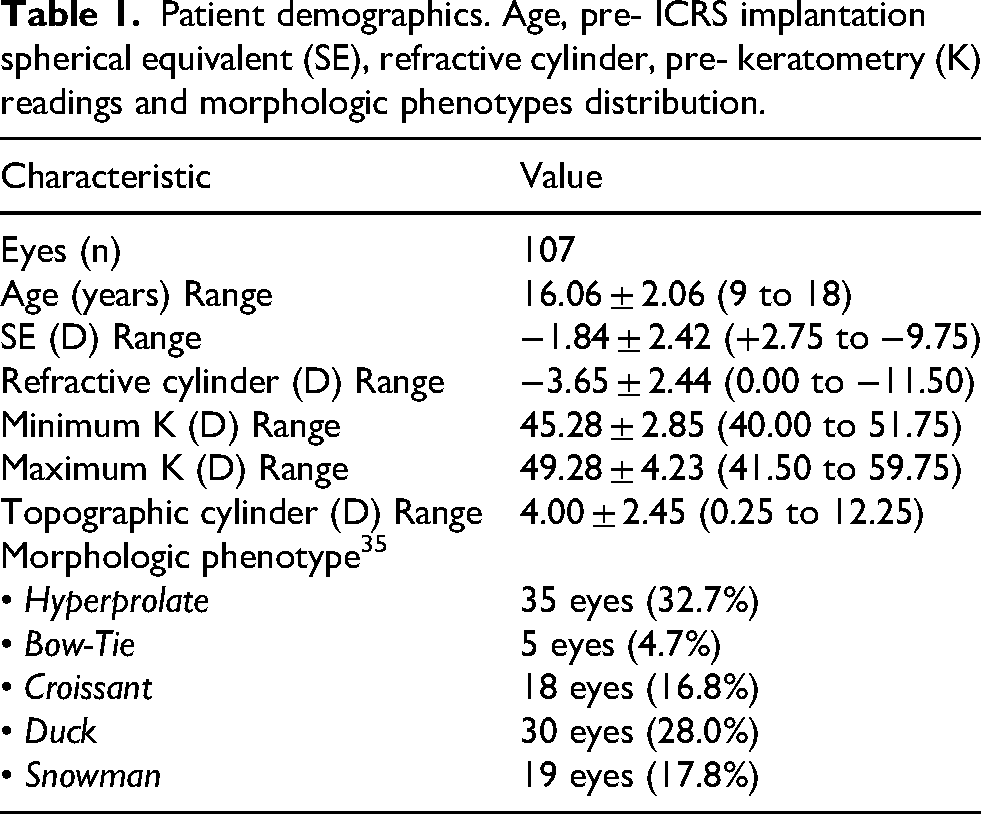
The study included 107 eyes of 85 patients with a mean age of 16.1 ± 2.1 (range 9 to 18). ICRS were successfully implanted in all cases, with no intra- or postoperative complications (corneal perforation, ICRS migration, ICRS extrusion, infection, explantation/repositioning, corneal neovascularisation). Table 1 shows patient demographics and preoperative characteristics. All patients were examined at the 1-year follow-up. Figure 1 shows the flowchart detailing the cases analyzed at the 5-,7- and 10-year follow-up visits; Supplementary Table 2 provides a detailed comparison of cases missed during the follow-up and those who attended.
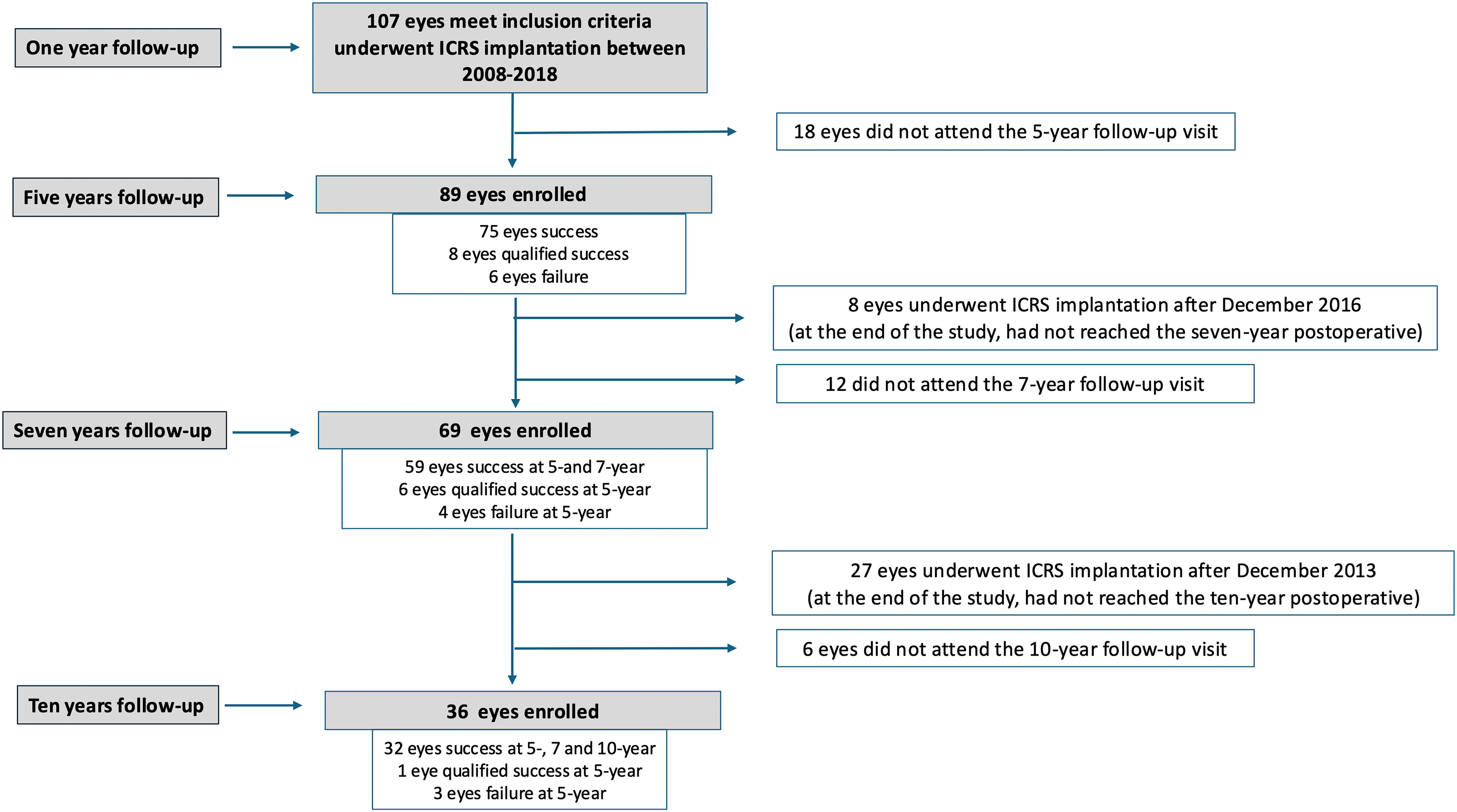
Flowchart detailing the cases analyzed at the 5-,7- and 10-year follow-up visits.
Patient demographics. Age, pre- ICRS implantation spherical equivalent (SE), refractive cylinder, pre- keratometry (K) readings and morphologic phenotypes distribution.
Visual and refractive outcomes at 1-year
Figure 2A shows the efficacy of the ICRS implantation at 1-year follow-up. The mean UDVA (logMAR) improved from 0.64 ± 0.38 before ICRS implantation to 0.34 ± 0.24 one year postoperatively (p < 0.0001). A linear mixed model showed an estimated mean change of −0.28 logMAR units (95% CI −0.37 to −0.20). The mean CDVA (logMAR) changed from 0.19 ± 0.15 before ICRS implantation to 0.08 ± 0.08 one year postoperatively (p < 0.001). A linear mixed model showed an estimated mean change of −0.11 logMAR units (95% CI −0.14 to −0.07). No eyes lost lines of CDVA 1 year postoperative compared to preoperative, and 74.8% of the eyes (80 eyes) showed a gain of lines of CDVA (figure 2B). Figure 2C shows the cumulative distribution of CDVA before surgery and 1-year later. The percentage of eyes with a CDVA of 0.1 logMAR (about 20/25 or better) increased from 40.7% to 75.0%, while the rate of eyes with a CDVA of 0.0 logMAR varied from 9.2% to 31.5%.
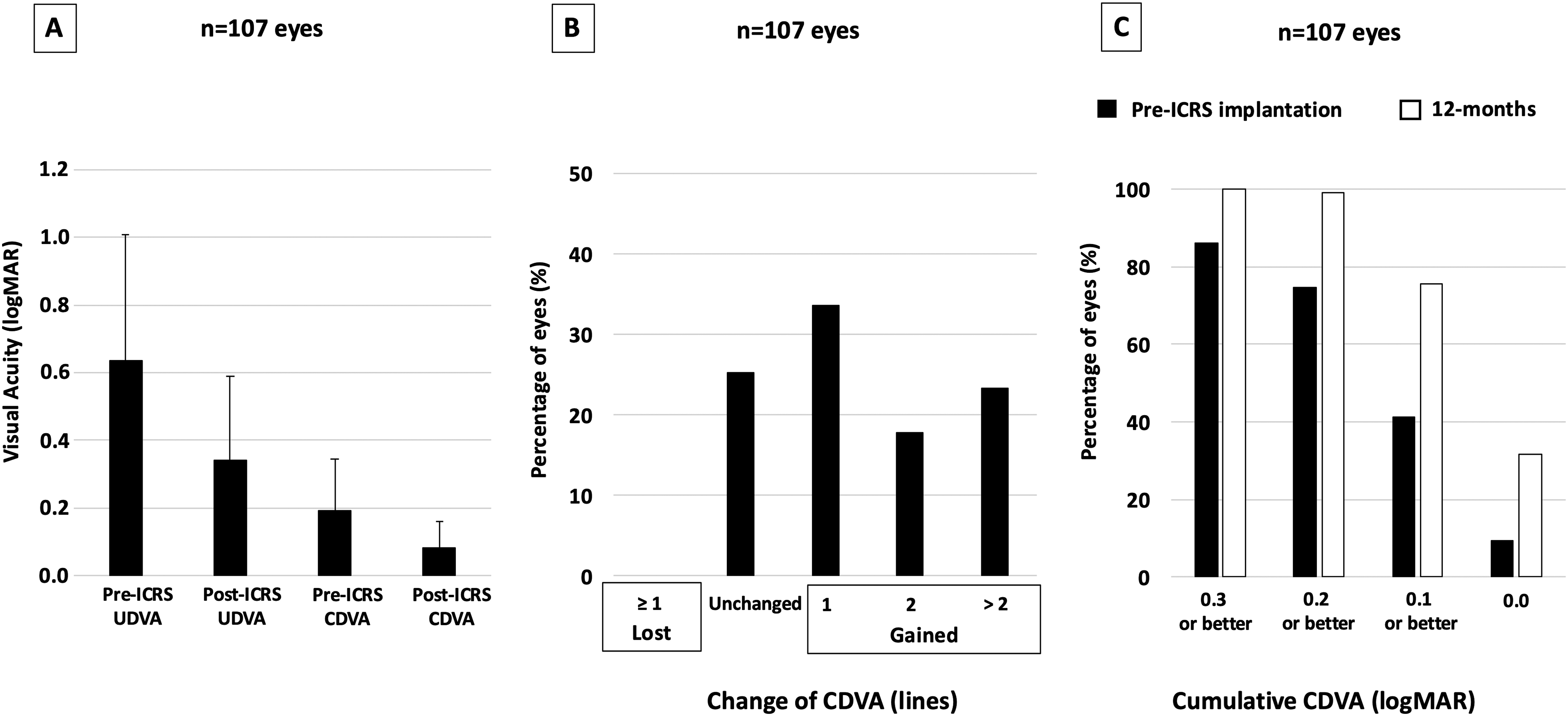
(A) uncorrected visual acuity (UDVA) and corrected distance visual acuity (CDVA) before and 12 months after intrastromal corneal ring segment (ICRS) implantation (efficacy), (B) change in corrected distance visual acuity (CDVA) 12 months after ICRS implantation (safety), and (C) plot comparing the cumulative CDVA before and 12 months after surgery.
Figure 3A shows the refractive astigmatism power vector (J0 and J45) before ICRS implantation and at 1-year. The mean refractive astigmatism changed from −3.65 ± 2.44 before ICRS implantation to −2.00 ± 2.44 1 year postoperatively (p < 0.001). A linear mixed model showed a mean change of 1.65 D (95% CI 1.12 to 2.18). Preoperatively, most eyes (61.7%) had a refractive cylinder ≥ 3.00, while postoperatively, the refractive cylinder in most eyes (76.6%) was < 3.00 D (Figure 3B).
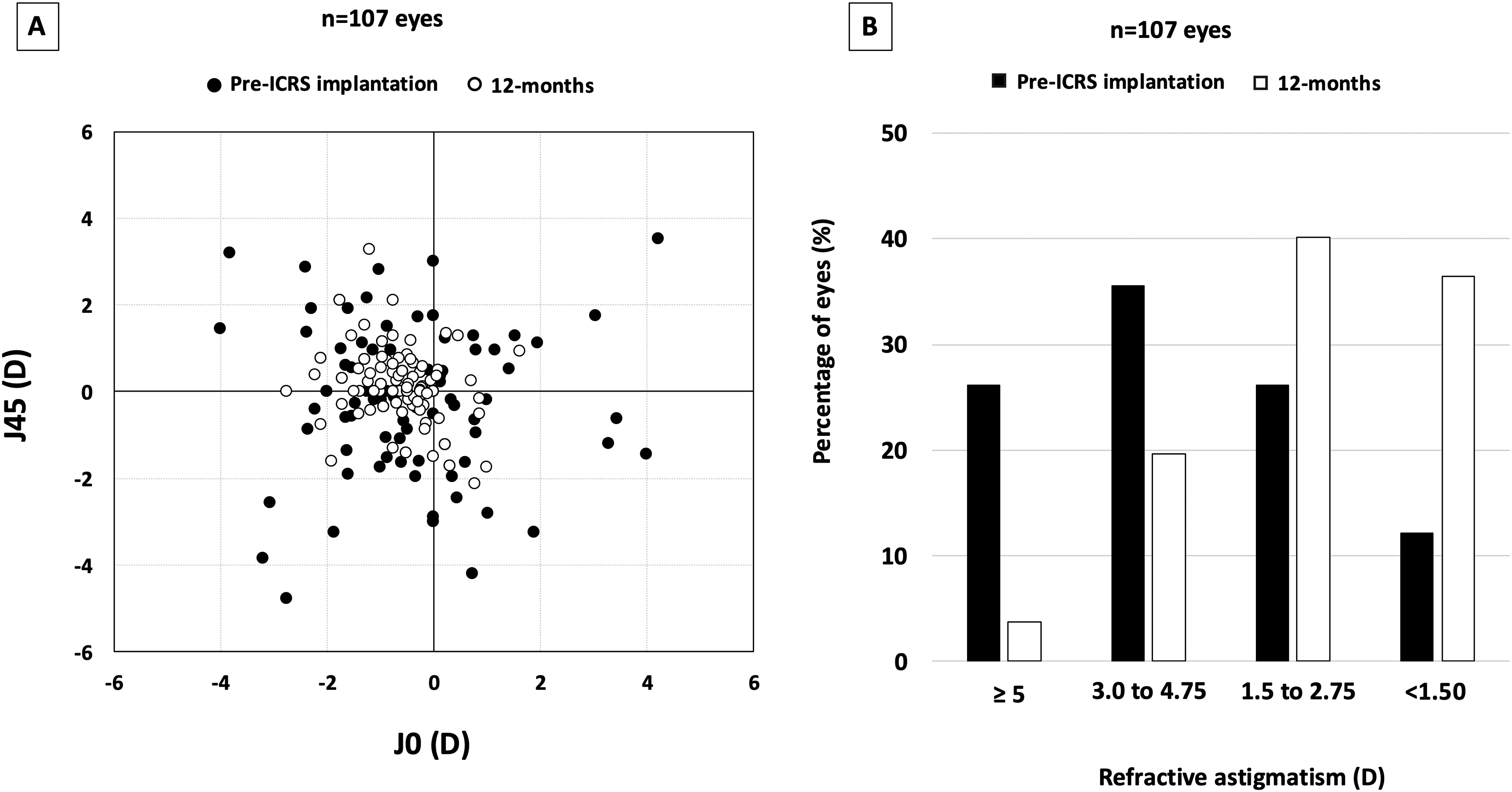
(A) representation of the astigmatic vector (J0 and J45) before and 12 months after intrastromal corneal ring segment (ICRS) implantation, and (B) distribution of the refractive astigmatism before and 12 months after ICRS implantation.
Success, qualified success and failure at 5-years
Refractive and visual outcomes showed a statistically significant improvement from the preoperative visit to the 5-year follow-up, whereas no differences were observed throughout the postoperative follow-up period (1 and 5 years).
Eighty-nine eyes were evaluated in the 1- and 5-year follow-up visits (Figure 1). At five years, in 75 eyes (84.3%), the treatment was categorized as success, in 8 eyes (9%) as a qualified success, and in 6 eyes (6.7%) as a failure (Figure 4A).
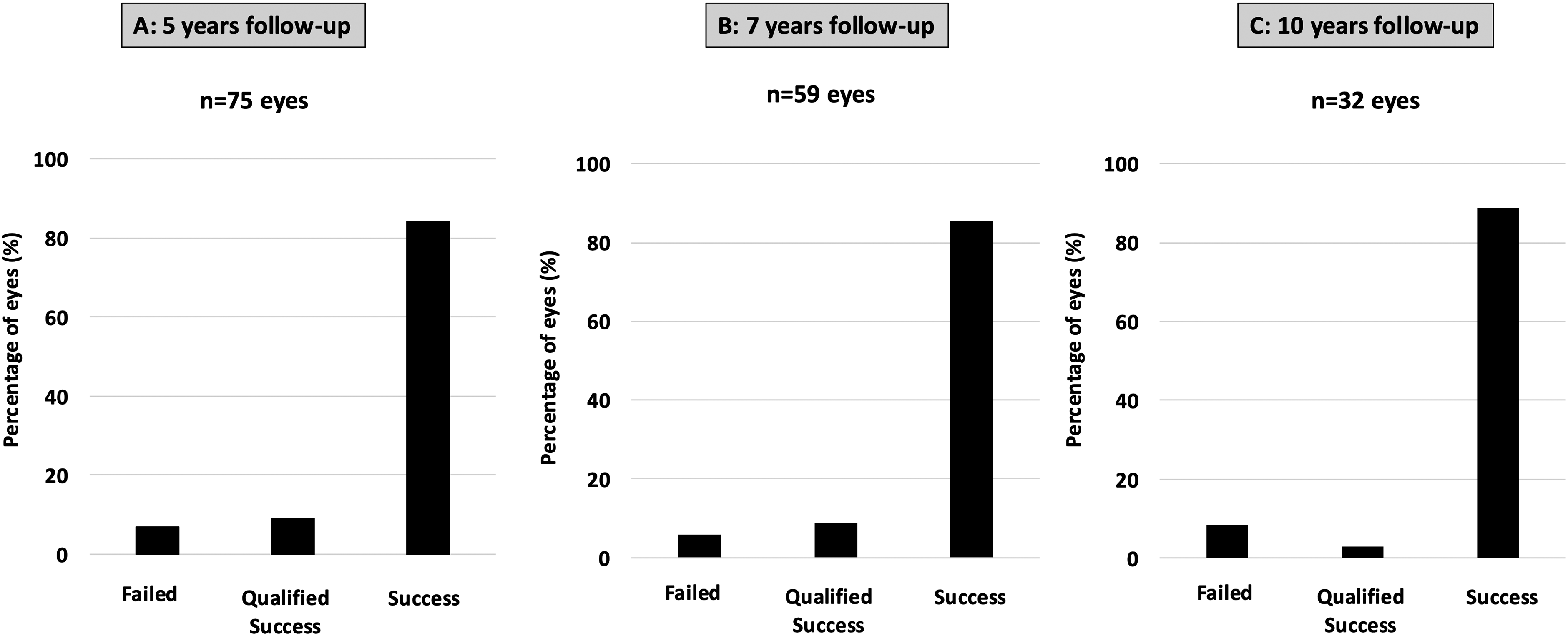
Distribution of success, qualified success and failure rates over the follow-up.
In the success cases (75 eyes), the visual and refractive parameters remained stable between 1- and 5-year follow-up visits (Figure 5), with most eyes gaining lines of CDVA compared to preoperatively and a postoperative CDVA of 0.2 or better (about 20/32) (Figure 6).
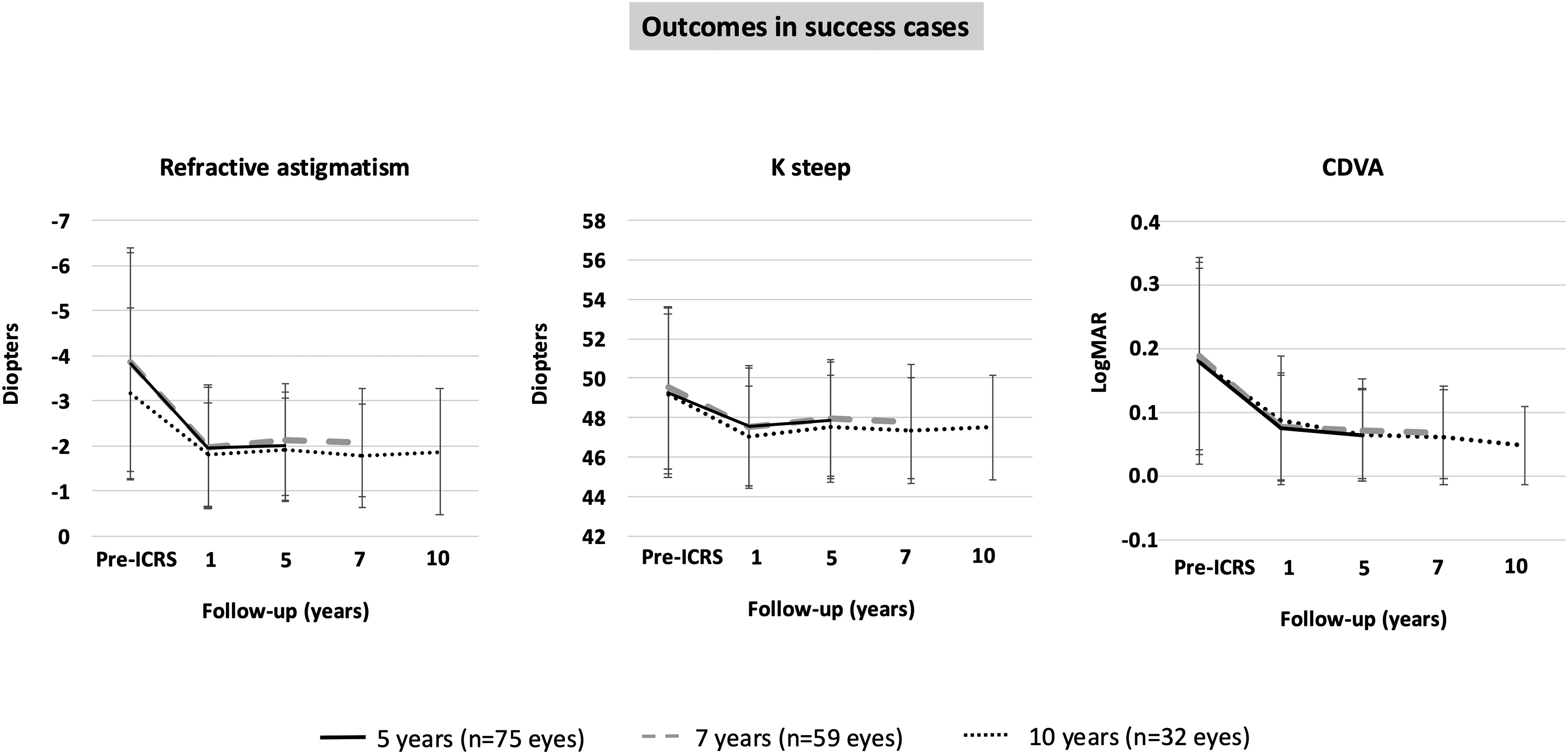
Time course of refractive astigmatism (A), K steep (B) and corrected distance visual acuity (CDVA) (C) over the follow-up in the cases where treatment was categorized as success.
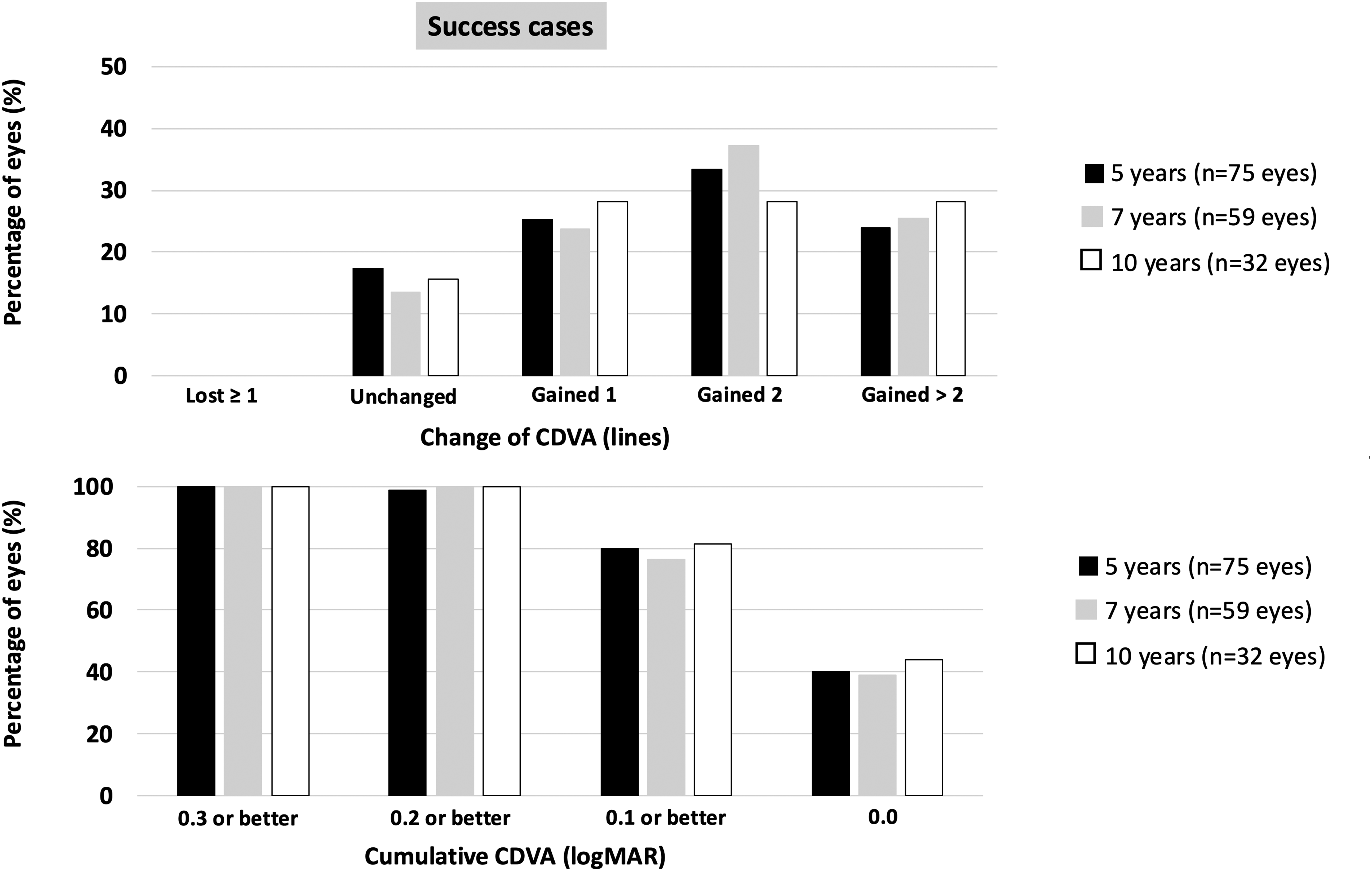
(A) variation in corrected distance visual acuity (CDVA) between preoperative and 5-,7- and 10-year follow-up visit (safety) and (B) cumulative CDVA at 5-, 7-, and 10-year post-ICRS implantation in the cases where treatment was categorized as success.
In the qualified success cases (8 eyes) (Table 2), comparing the 1- and 5-year outcomes, all eyes meet at least one of the instability criteria between (an increase of at least 1.5D steep K; an increase of at least 1.5D in the topographic or refractive astigmatism; a decrease in CDVA greater than 1 line). Comparing CDVA and manifest refraction at 5-years with preoperatively, 6 eyes gained lines of CDVA, and 2 eyes remained at the preoperative CDVA level (both cases 0.2 logMAR, about 20/32 Snellen Scale). Two eyes (Table 2; #3 and #7) had an increase in refractive astigmatism of 1.0D compared to preoperative, but the CDVA was three lines better than preoperatively.
Visual and refractive outcomes during the whole follow-up in the eyes with qualified success.
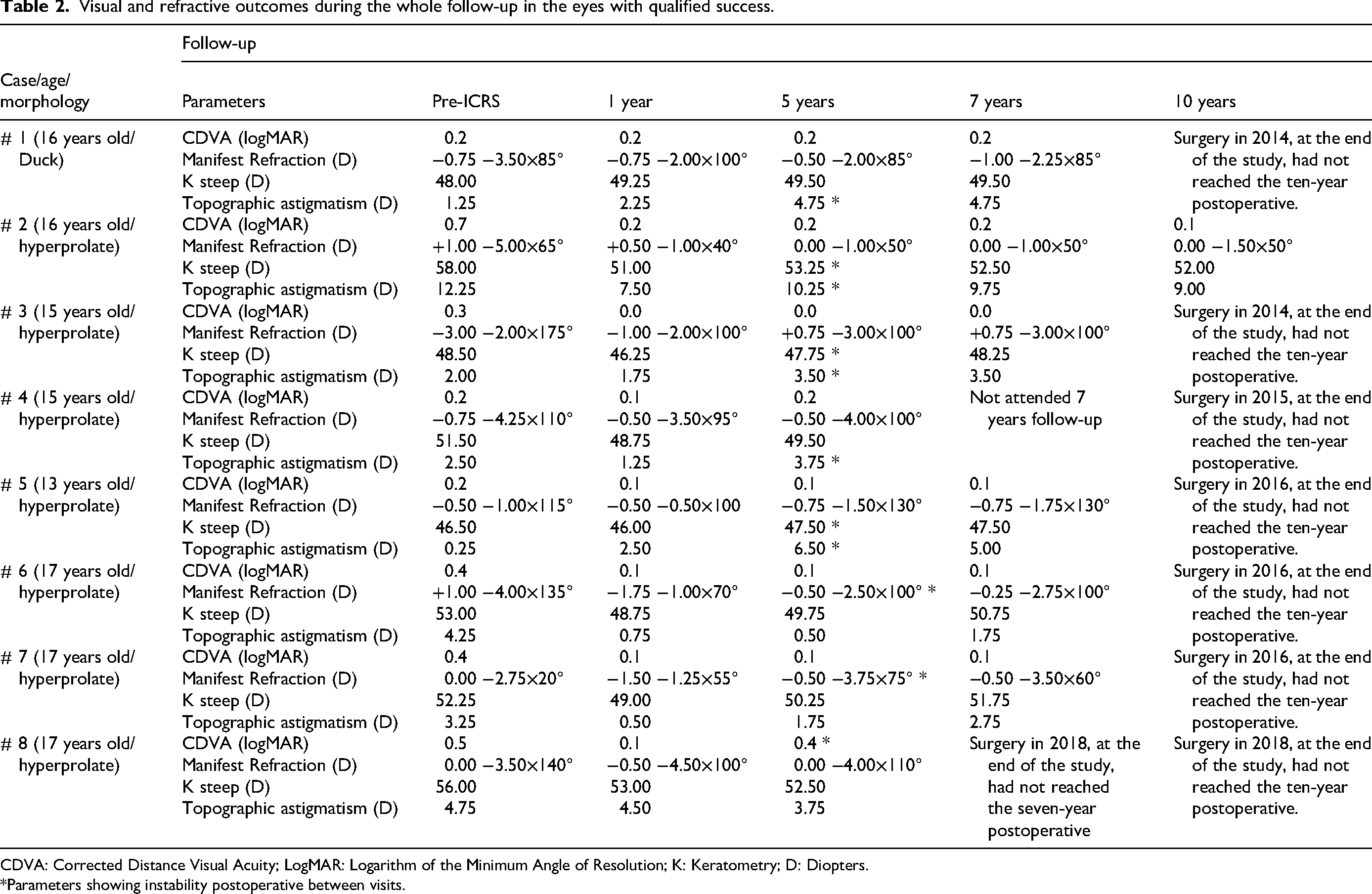
CDVA: Corrected Distance Visual Acuity; LogMAR: Logarithm of the Minimum Angle of Resolution; K: Keratometry; D: Diopters.
*Parameters showing instability postoperative between visits.
In the failure cases (6 eyes), in 3 eyes, a Deep Anterior Lamellar Keratoplasty (DALK) was performed in the period between 1 to 5 years, whereas in the other 3 eyes, the treatment was categorized as a failure because the disease progressed, and the visual or refractive outcomes at five years were worse than preoperatively. Specifically, two eyes had refractive astigmatism > 2.00D than preoperatively, although their level of CDVA at 5 years postoperatively was 1 and 2 lines better than preoperatively. In the other eye, the CDVA decreased two lines compared to preoperatively, reaching a CDVA at five years of 0.2 logMAR (about 20/32 Snellen) with a manifest refraction of −1.50 −1.00 X 85°.
Success, qualified success and failure at 7-years
Refractive and visual outcomes showed a statistically significant improvement from the preoperative visit to the 7-year follow-up, whereas no differences were observed throughout the postoperative follow-up period (1, 5 and 7 years).
Sixty-nine eyes were evaluated in the 1-, 5- and 7- year follow-up visits (Figure 1). Of these 69 eyes, in the previous visit (5 years), 59 had been categorized as success, 6 as qualified success and 4 as failure. During the 5–7 years period, no new cases of failure or qualified success were reported. Figure 4B shows the success cumulative rate over the 7 years of follow-up.
Figure 5 yields the visual and refractive outcomes of the 59 success cases over the 5 to 7 years period. 86.4% remained a CDVA better than preoperatively and all eyes had a CDVA of 0.2 logMAR or better (about 20/32) (Figure 6).
The six eyes with qualified success at 5 years visit that reached the 7 years of follow-up, showed stable visual and refractive outcomes during the 5 to 7 years period (Table 2).
No keratoplasties were performed in the 5–7 years period.
Success, qualified success and failure at 10-years
Refractive and visual outcomes showed a statistically significant improvement from the preoperative visit to the 10-year follow-up, whereas no differences were observed throughout the postoperative follow-up period (1, 5, 7 and 10 years).
Thirty-six eyes were evaluated in the 1-, 5- and 7- and 10- year follow-up visits (Figure 1). Of these 36 eyes, in the previous visits (5 and 7 years), 32 had been categorized as success, 1 as qualified success at five years with stable results at seven years, and 3 as a failure at five years. During the 7–10-year period, no new cases of failure or qualified success were reported. Figure 4C shows the success cumulative rate over the 10 years of follow-up.
Figure 5 shows the visual and refractive outcomes of the 32 success cases over the 10 years of follow-up. 84.4% remained a CDVA better than preoperatively, and all eyes had a CDVA of 0.2 logMAR or better (about 20/32) (Figure 6).
The case with qualified success at five years that reached the 10 years of follow-up showed stable visual and refractive outcomes during the 10 years postoperative period (Table 2).
No keratoplasties were performed in the 7–10 years period.
Discussion
This study aimed to assess the effectiveness of ICRS in inducing a visual and refractive rehabilitation over a long period. Our results in 107 eyes evaluated one the 1 year postoperatively indicated that all the visual and refractive parameters analyzed improved significantly after ICRS implantation. The mean improvement in UDVA was −0.28 logMAR units (95% CI −0.37 to −0.20), and in CDVA was −0.11 logMAR units (95% CI −0.14 to −0.07). 75% of the eyes reached a postoperative CDVA of 0.1 logMAR (about 20/25 or better). In turn, the percentage of eyes with a postoperative refractive cylinder < 3.00 D was around 75%.
These results suggest that ICRS implantation is an effective and safe procedure for visual rehabilitation in pediatric patients. However, considering the disease in pediatric populations is more aggressive and with a higher risk of progression, the crucial issue is whether the ICRS-induced visual rehabilitation remains for a long time, allowing the pediatric patient affected by keratoconus a personal growth with a better visual environment or, on the contrary, the effect disappears.
Two previous studies evaluated the visual and refractive outcomes of ICRS implantation in the pediatric population spanning at least five years of follow-up.25,32 Abreu et al. 32 analyzed 14 pediatric eyes implanted with Intacts or Intacs SK (Addition Technology Inc., USA) using a standard technique of tunnel creation by mechanical dissection with a mean follow-up of 6.36 ± 0.97 years. The visual and refractive parameters significantly improved after ICRS implantation, remaining stable without statistically significant changes during the follow-up, although the authors pointed out the surgery did not halt the keratoconus progression. Our research group reported 25 the five years of follow-up in 23 eyes implanted with Ferrara-type ICRS using a femtosecond laser. Similar to the study by Abreu et al., 32 the visual and refractive parameters significantly enhanced after surgery, and most eyes exhibited visual and refractive stability over five years. 25
The current study increased the number of eyes that reached 5 years of follow-up, 89 eyes. Furthermore, 69 eyes reached 7 years, and 36 eyes reached 10 years of follow-up. To our knowledge, this study includes the largest sample of pediatric keratoconus after ICRS implantation with the most extended follow-up. Furthermore, treatment success was analyzed case by case over the whole follow-up. To this extent, our research group defined new criteria that, maybe, should be submitted to an open discussion within the scientific community to redefine or fit and reach a consensus. A couple of premises were considered to determine these criteria: first, the treatment target, and second, the clinical criteria that should be applied to conclude that such a target has been achieved.
The main goal of ICRS implantation in keratoconus is to improve the corneal shape, ultimately aiming to achieve visual restoration for the patient. Contrary to the CXL treatment, the main aim is not to arrest the progression of keratoconus. Hence, applying only criteria of disease progression for ICRS implantation could, somehow, be wrong. In the same way, improving visual and refractive parameters is not the primary criterion for defining CXL success. Beyond the widely accepted difficulty in diagnosing the keratoconus progression, it is worth noting that whether ICRS implantation is successful would induce a decrease corneal irregularity and increase visual quality. Hence, subtle changes that could evidence a disease's progression will not have the same clinical impact as if such improvement is not achieved after treatment.
Therefore, for the success of the ICRS implantation treatment, the procedure must first induce a significant improvement in the visual and refractive parameters. Secondly, such enhancement must remain (either because the disease is not in progression, or the natural halting of the disease, or such as Vinciguerra et al. 42 hypothesized because the ICRS generate a new biomechanical environment which favours the stable visual and refractive outcomes). With this in mind, we defined the treatment as successful based on the short-term improvement, the stability of the visual and refractive outcomes and the comparison between the long-term follow-up and preoperative.
Overall, the treatment was successful in most cases (80%) at 5-, 7- and 10-year follow-ups (Figure 4). That is, the visual and refractive improvement 1 year after surgery remained stable at the more extended follow-up visits (Figure 5). The treatment was a qualified success for around 8% of the eyes. That is, there was a visual and/or refractive instability over follow-up, but the visual and refractive parameters at 7- and 10-year postoperatively were equal or better than preoperatively (Table 2). These results imply that more than 90% of cases experienced a visual and/or refractive improvement over a long period compared to preoperatively. Finally, the treatment failed in 6 eyes. Interestingly, the failures and the instability in the qualified success cases, occurred in the first five years after implantation.
As we pointed out before, we cannot confirm the mechanism behind these results: whether the disease was not progressing, the natural halting of the disease, or the ICRS enhances the biomechanical environment; what we can confirm from the results obtained is that the ICRS-induced improvement was maintained in most cases with follow-up of 5, 7, and 10 years, indicating its effectiveness in restoring vision in pediatric patients with keratoconus.
Abdelmassih et al. 43 reported the results of sequential ICRS implantation and CXL in 17 eyes of patients under 14 years of age and a follow-up of up to 4 years. The authors concluded that this sequential procedure was effective and safe for visual restoration with long-term stability. In our study, long-term stability was achieved in most eyes (around 80%) without the need for associated CXL treatment. Hence, our results agree with those authors who postulated that it is not urgent to perform CXL treatment in child patients without evidence of disease progression,14,18 even further considering that CXL is not a procedure free of potential complications.9,12–14,17,20 Beyond close monitoring to perform the CXL treatment as promptly as signs of disease progression appear, it would be interesting to identify preoperative characteristics that may represent risk factors for experiencing postoperative instability. Unfortunately, our study did not have a homogenous sample of eyes in the three groups to properly compare the preoperative characteristics among groups (75 eyes with postoperative stable results (success), 8 with postoperative instability (qualified success) and 6 eyes with failure. However, it is worth noting that in 7 of the 8 eyes (87.5%) with qualified success, the morphologic pattern was hyperprolate (Table 2), which represented 20% of all eyes analyzed with this morphological pattern (Table 1). Ferdi et al. 7 , in a systematic review and meta-analysis of keratoconus including 11.529 eyes, reported that younger than 17 years and Kmax steeper than 55.0D had a significantly higher risk of disease progression. Notably, a steeper Kmax is a characteristic feature of a hyperprolate pattern. Perhaps young age and the hyperprolate morphologic pattern are risk factors for postoperative instability after ICRS implantation. However, further studies should be conducted to properly evaluate the potential risk factors, including topo-tomographic parameters, eye rubbing, and allergies, and identify other inherent factors that may represent a risk for disease progression. Anyway, these patients should be closely monitored for the earliest signs of progression and timely CXL treatment.
Finally, it is important to note that all eyes were implanted with Ferrara-type ICRS using femtosecond laser (which provides safety and predictability to the procedure44,45), and following a protocol that implies first classifying the keratoconus morphology according to the five morphology phenotypes 35 and subsequently, selecting the nomogram for ICRS implantation specific for each morphology.36–40 Modifications to this protocol could lead to different results.
Despite the encouraging results, we must note some limitations of the study, such as its retrospective design, the absence of a control group, and the inability to collect data from all patients throughout the entire follow-up, which means we cannot ensure that those patients who did not complete the entire follow-up did not experience instability over time. However, the comparison between cases who attended postoperative visits and those missing in follow-up, as shown in supplementary Table 2, suggests that patients with better outcomes are less likely to attend follow-up visits. Anyway, further prospective studies which collect a larger number of cases over an extended follow-up duration and include comparisons with other strategies, such as ICRS combined with CXL and CXL alone, are required to validate these findings and evaluate the most effective first-line therapy approach in this population.
In summary, the first-line therapy aim in this sample of pediatric keratoconus was to reshape corneal morphology to ameliorate visual quality. Our results show that this aim was achieved, and in most eyes with available long-term follow-up, visual and refractive improvements were maintained, supporting ICRS as a long-term visual rehabilitation option in pediatric keratoconus.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721261437863 - Supplemental material for Intrastromal corneal ring segment implantation in pediatric keratoconus: Up to 10 years of follow-up
Supplemental material, sj-docx-1-ejo-10.1177_11206721261437863 for Intrastromal corneal ring segment implantation in pediatric keratoconus: Up to 10 years of follow-up by Luis Fernández-Vega-Cueto, Carlos Lisa, Belén Alfonso-Bartolozzi, Aranzazu Poo-López, Irene Martinez-Alberquilla, David Madrid-Costa and José F. Alfonso in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721261437863 - Supplemental material for Intrastromal corneal ring segment implantation in pediatric keratoconus: Up to 10 years of follow-up
Supplemental material, sj-docx-2-ejo-10.1177_11206721261437863 for Intrastromal corneal ring segment implantation in pediatric keratoconus: Up to 10 years of follow-up by Luis Fernández-Vega-Cueto, Carlos Lisa, Belén Alfonso-Bartolozzi, Aranzazu Poo-López, Irene Martinez-Alberquilla, David Madrid-Costa and José F. Alfonso in European Journal of Ophthalmology
Footnotes
Ethics approval and consent to participate
This study was conducted in compliance with the tenets of the Declaration of Helsinki, and full ethical approval from the Fernández-Vega Ophthalmological Institute was obtained. After receiving a complete description of the nature of the study, all patients provided informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors have no proprietary interest in any of the materials mentioned in this article.
Data availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.