
Abstract
Case presentation
A male in his mid-60´s presented with left eye retinal detachment scheduled for emergency vitrectomy in January 2020. Secondary diagnoses were a well-controlled arterial hypertension, and mild chronic obstructive pulmonary disease (GOLD 1). For anesthetic procedure a retrobulbar block combined with brief initial analgosedation was chosen.
After establishing routine monitoring of vital parameters (ECG, NIBP, pulse oximetry) and placing an intravenous line, the patient received pre-oxygenation (until reaching etO2 of 80%) and a bolus of 50 µg of fentanyl und 150 mg (2 mg/Kg) of thiopental according to house standard. Immediately after loss of consciousness, the surgeon applied the retrobulbar block. A blunt 23 G needle of 32 mm length was used to apply the local anesthetic solution (2.5 ml mepivacaine 2% plus hyalase 20:1 and 2.5 ml bupivacaine 0.5%; total volume 5 ml) via a transconjunctival access at the infero-temporal margin of the orbita. Neither blood nor cerebrospinal fluid could be aspirated during the procedure. A typical proptosis during injection, however, was not observed. Subsequently, occulopression was performed without causing subsequent bradycardia. Instead, after approximately one more minute we observed a raise in heart rate (103 bpm) and blood pressure (213/133 mmHg). While urapidil was prepared, hypertension increased to a value of 270/166 mmHg, and tachycardia reached 130 bpm. After two i.v. doses of 10 mg of urapidil, the systolic blood pressure fell below 200 mmHg while tachycardia persisted. Paralleling the hemodynamic crisis, we observed that the patient did not take up respiration again. In consequence, we started bag-mask ventilation with 100% oxygen supported by a ventilator. Right eye pupil reaction was unchanged. Left eye pupil had been pharmacologically dilated in preparation of the surgical procedure. An indirect light reaction could however not be observed in the right eye. At this point we established the working hypothesis of a toxic reaction to the local anesthetic, and immediately applied a bolus of 100 ml SMOF-Lipid solution followed by two ampoules with a total amount of 500 ml over 30 min according to the standard procedures for local anesthetic intoxication of the Swiss Society for Anesthesiology and Perioperative Medicine SSAPM.
While there was persistent loss of consciousness and loss of spontaneous breathing, the working hypothesis extended to brainstem anesthesia. An arterial blood gas analysis excluded metabolic reasons of unconsciousness. The patient was then intubated and mechanically ventilated. We immediately conducted cranial CT scans (native, and with contrasting agent) to exclude further neurologic pathologies. The CT scans revealed intra-cranial air (see arrow in Figures 1 and 2) with a suspicion of a small fissure at the upper orbita and sparse blood in the left fronto-basal sulcus. The observed blood was accounted clinically insignificant. Signs of demarcated infarctions could be ruled out.
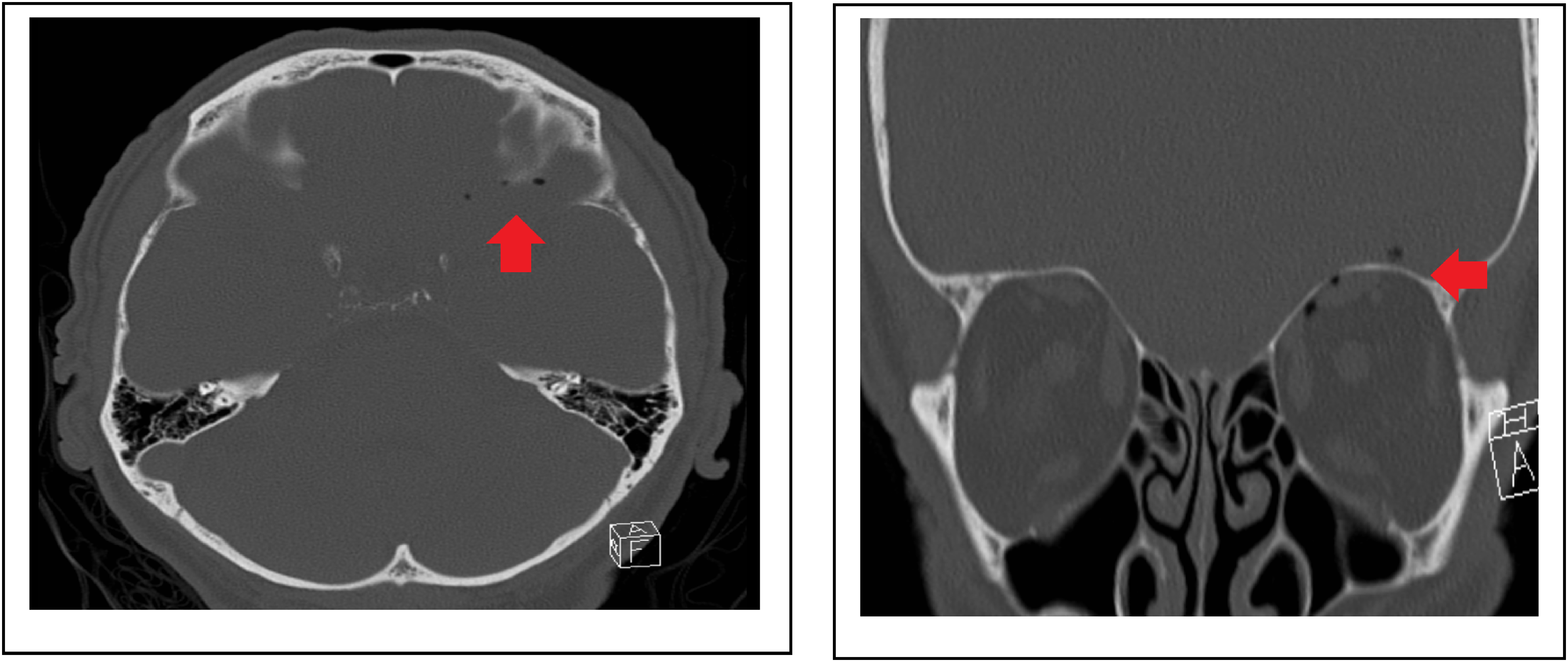
cranial CT showing intra-cranial air with suspicion of a small fissure at the upper orbita and a suspicion of blood in the left fronto-basal sulcus.
The patient was transferred to the ICU, and prophylactically treated with a single dose of intravenous Cefuroxime. Blood glucose levels and arterial blood gases were normal at any time. A couple of hours after the incident, the patient could be extubated without complications. On the following day, uneventful vitrectomy of the left eye was performed under general anesthesia. The patient was discharged without any deficits 48 h after the incident.
Informed consent has been obtained from the patient to use the data presented in this case report.
Discussion
Incidences of complications
Central nervous complications following retrobulbar anesthesia are very rare but have been reported in almost 30 cases. Most of these have been published in the past century.1–19 We found seven reports since 2010, and six more since 2000.20–32 Clinical manifestations reached from mild impairment like temporary gaze palsy up to blindness of the contralateral eye, dysphagia, respiratory depression, and cardiac arrest.1,20 The incidence of CNS complications was calculated between 0.27% und 0.79%.2,3 The frequency of respiratory depression after retrobulbar anesthesia was estimated at 0.03%.4,5,6 A study from 1987 analyzing 6’000 retrobulbar blocks found 16 cases (0.26%) in which neurologic symptoms indicated the local anesthetic had entered the intracranial space; one of these patients (0.02%) had suffered cardiac arrest. 1 In our institution, we perform more than 1’000 retrobulbar blocks per anno without any similar complication reported so far. Table 1 in the appendix gives an overview of the characteristics of cases reported since 2000. The choice of the local anesthetic agent varies and depends on availability and pharmacological properties. The main consideration in combining two different local anesthetics target a combination of fast onset (Lidocaine and Mepivacaine) with sufficient duration of the effect (Bupivacaine and Ropivacaine).33,34
Overview of cases reported since 2000.
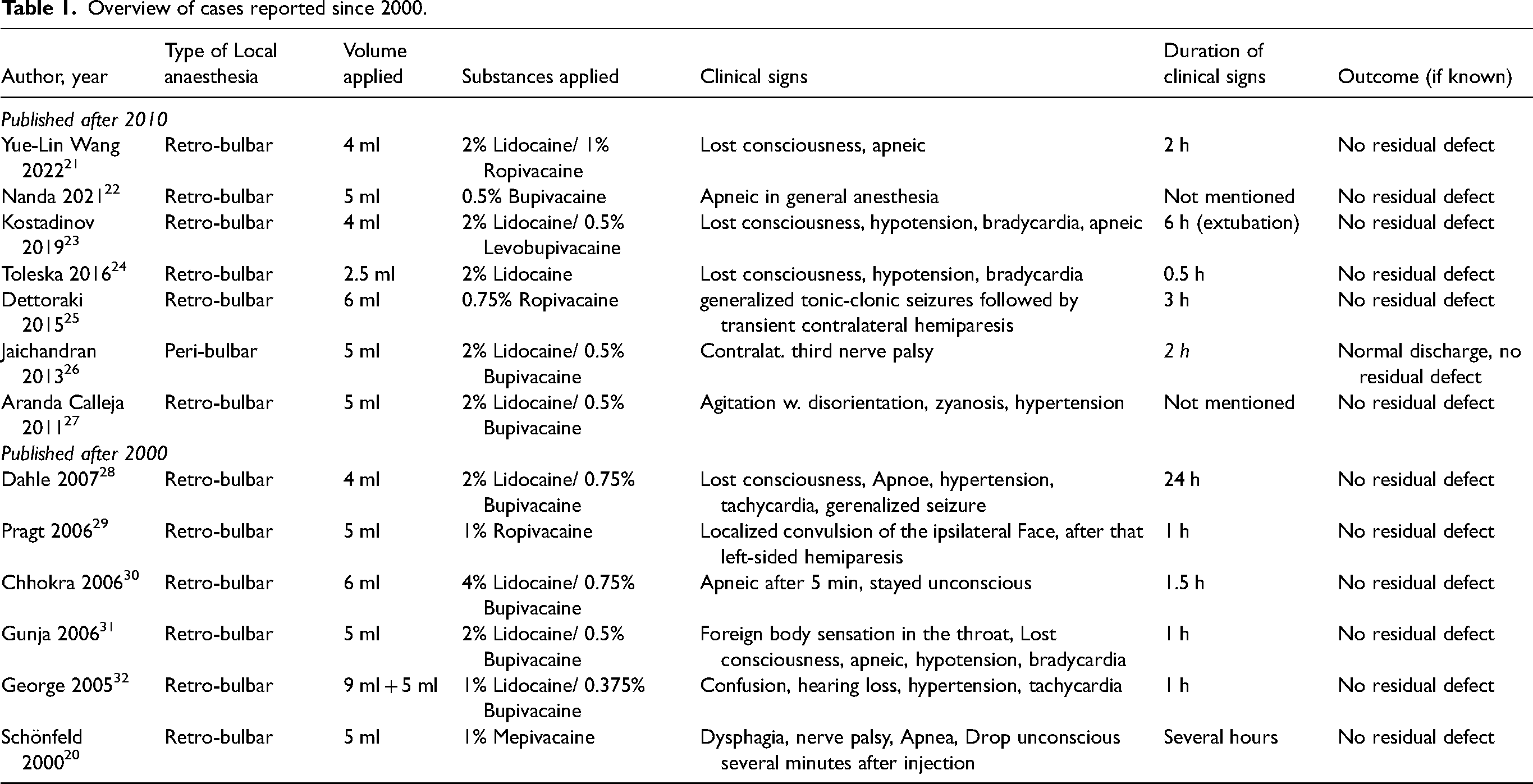
Many surgeons prefer adding hyaluronidase, as hyaluronidase facilitates the spread of anesthetic to maximize its effect while reducing volume. 34 Mentioning safety aspects, the dosage of applied local anesthetics in all the described cases were far below toxic threshold levels.35,36 In our case, for the maximum dose for Mepivacaine would have been 5 mg/kg−1 and for Bupivacaine 2 mg/kg−1.
Diagnostic considerations
In our case, analgosedation masked the typical initial symptoms of either local aesthetic intoxication (such as metal taste, nausea, or impaired vigilance), or brain stem anesthesia (such as blindness, gaze palsy, shivering, dysphagia, loss of consciousness, respiratory depression, or respiratory arrest).7,20 In the light of an unconscious patient suffering severe hypertension coupled with tachycardia, a distraction between local anesthetic systematic toxicity (LAST) and brainstem anesthesia is challenging. In LAST, the initial hemodynamic reaction is related to the stimulation of the sympathetic nervous system. Local anesthetics can cause an increase in the release of catecholamines (like adrenaline) and inhibit their reuptake, leading to an overactive sympathetic response. This results in elevated heart rate (tachycardia) and increased blood pressure (hypertension). 37 Because local anesthetics strongly affect mitochondrial metabolism, neurologic and cardiac dysfunctions occur later on with severe bradycardia and hypotension. 38 There is limited data regarding the mechanism of hypertension and tachycardia after intrathecal injection. Hamilton described the patho-mechanism as a combination of vagal and carotid sinus reflex blockade. 16 Another known description of sympathetic activation is due to a reaction of instant intracranial pressure rise. This reaction is described in animal studies: Intrathecal injections can increase cerebrospinal fluid (CSF) pressure with consecutive elevation of intracranial pressure (ICP). The rapid increase in ICP can trigger a reflex sympathetic response resulting in hypertension and tachycardia. This response is mediated by baroreceptors and chemoreceptors, which detect changes in pressure and chemical composition. 39 Tachycardia would have also brought an anaphylactic reaction into discussion. However, hypertension and the lack of erythema or bronchospasm made this diagnosis very unlikely. Intracranial hemorrhage and stroke had been ruled out by CT scanning.
What this case adds
The case presented, adds important aspects to the literature. One important point is that we were able to provide images of a morphologic correlate possibly explaining the patho-mechanism behind the clinical symptoms. CT scans clearly showed intra-cranial air and blood in the left fronto-basal sulcus which both could not be explained otherwise.
As a second important point, we add the conditions of brief analgosedation before the retrobulbar block. This technique is increasingly applied to enhance patient comfort. However, both local anesthetic intoxication, and brainstem anesthesia are primarily masked by the sedation.
In our case, the complications could be handled appropriately due to the presence of an anesthesia team. Standardized procedures including pre-oxygenation and close monitoring of vital signs were essential precautions leading to better safety margins when treating all the relevant conditions at the same time (hypertensive crisis, tachycardia, respiratory arrest). This preparation was a precondition for achieving a favorable outcome. In times of increasing ambulant practice and cost restraints, it is therefore essential to have a skilled anesthesia team available.
Technical alternatives to the retrobulbar block
To avoid complications as the one described it is of interest whether adequate alternatives are available. One possible alternative is a peri-bulbar infiltration outside of the eye muscle cone. With this method, it takes considerably more time until full anesthesia is established, and bulbar akinesia is less reliably achieved as compared to the retrobulbar approach.8,9 Another alternative is subtenon anesthesia. For this technique, Tenon's capsule is opened by incision and the local anesthetic is injected after blunt dissection.10,11 Subtenon anesthesia leads to a success rate comparable to retrobulbar block (in terms of analgesia and bulbar akinesia). Drawbacks of this block include the necessity to open the conjunctiva with the risk of infection, and subconjunctival bleeding. Subtenon block is perceived as safer, because the blunt preparation makes bulbar injuries less likely and other severe complications such as brain stem anesthesia have not been reported. Accordingly, subtenon block is preferred in health services where an anesthesia team is not readily available. We therefore recommend subtenon anesthesia for such situations as the technique of choice.
Conclusion
With this case, we present a rare but life-threatening complication of retrobulbar anesthesia for eye surgery. We report two important aspects for the first time. First, we provide imaging findings helping to better understand the patho-mechanism of action. Second, we describe this complication in the context of brief analgosedation that may mask many of the clinical signs. The presence of a skilled anesthesia team was essential for achieving a favorable outcome.
Footnotes
Acknowledgements
CT scans were kindly provided by Prof. Dr. med. A. Bink, Chief of service, Department of Neuroradiology, University Hospital of Zurich. Prof. Dr. med. D. Barthelmes, Head of Department of Ophthalmology, University Hospital of Zurich for his advise and support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was considered exempt from full ethical approval by the ethics committees of canton Zurich (Nr. Req-2022-01525)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.