
Abstract
Introduction
The current case series presents the triangular suture technique (TST) for managing intraocular lens (IOL) subluxation in pseudoexfoliation (PXF) syndrome patients, a condition increasing the risk of IOL dislocation post-cataract surgery. The series includes three PXF patients treated with TST for dislocated IOLs.
Case description
The first case is an 88-years old woman with recurrent IOL dislocation post-Hoffman pocket fixation. TST resulted in successful IOL centration and significant visual acuity improvement, with uncorrected visual acuity (UCVA) improving from 6/60 to 6/15 and best-corrected visual acuity (BCVA) reaching 6/7.5 at three months. The surgery took 21 min with no major complications. The second case involves a 90-year-old man with posterior IOL dislocation and poor vision (UCVA of counting fingers at 1 meter). TST achieved good IOL repositioning and improved BCVA to 6/20 at three weeks. The last case presents an 82 years old woman with PXF and glaucoma, experiencing IOL subluxation post-traumatic cataract surgery. TST successfully centralized the IOL, improving non-corrected visual acuity from 6/30 to 6/10 at six weeks, and BCVA to 6/6.67 at four years. Intraocular pressure remained well-controlled.
Conclusions
This series highlights TST as an effective and safe solution for IOL subluxations in PXF patients, with successful outcomes in all cases. TST offers ease of learning and faster execution, suitable for anterior segment surgeons without extensive vitreoretinal experience. Further studies are needed to confirm the long-term efficacy and safety of TST, ideally involving larger cohorts and longer follow-ups.
Keywords
Introduction
IOL subluxation can arise from various conditions that may compromise zonular support and capsular bag stability, including trauma, pseudoexfoliation syndrome (PXF), surgical complications, connective tissue disorders (such as Marfan syndrome, Ehlers-Danlos Syndrome and Weil-Marchesani's syndrome) and high myopia.1,2 Its prevalence is likely higher than previously recognized, underlining its importance in ophthalmic surgery.1,2
IOL subluxation is a sight-threatening complication following cataract surgery, manifesting as decreased vision, diplopia, and glare. 3 It may also lead to complications such as angle-closure glaucoma and uveitis-glaucoma-hyphema syndrome. 3
Over the years, the management of IOL subluxation has seen significant progress, with a wider array of surgical approaches becoming available. These techniques encompass both anterior chamber IOLs and posterior chamber IOLs fixated to either the iris or the sclera (scleral-fixated intraocular lenses, SFIOLs). 4 Depending on the specific situation, the intervention may involve repositioning or replacing the dislocated IOL. 4
Advancements in surgical techniques have propelled SFIOLs to the forefront of IOL fixation, leading to improved visual and ocular outcomes. 5 For example, Newer IOL designs, such as the CZ70BD (Alcon, Fort Worth, TX) and Akreos AO60 (Bausch and Lomb, Rochester, NY), incorporate suture eyelets to minimize suture slippage and subsequent IOL dislocation, the introduction of 9-0 polypropylene and 7-0 Gore-Tex (CV-8) sutures addresses concerns about the long-term stability of 10-0 polypropylene sutures and suture burring under the sclera or conjunctiva reduced the risk for endophthalmitis. 5
SFIOLs can be implanted using either sutured or sutureless methods, each offering distinct advantages and potential complications. The choice of IOL and surgical approach is highly dependent on the specific clinical context, highlighting the importance of individualized treatment plans.5,6
First described by Lindberg in 1917, PXF is characterized by the deposition of fibrillary material throughout the eye and body.5,6 Ocular involvement, particularly in the trabecular meshwork, cornea, lens, and iris, can lead to cataract formation, glaucoma, and zonular weakness, ultimately causing lens dislocation. 6 The syndrome affects over 60 million individuals worldwide, primarily those above 50 years old and exhibits geographic and ethnic variations. 6
Pseudoexfoliation syndrome (PXF) presents a unique challenge for cataract surgeons as the compromised zonular fibers in PXF patients increase the risk of capsular bag dislocation. 6 To mitigate this risk and achieve optimal outcomes, meticulous preoperative and intraoperative planning are crucial.5,6 Surgeons must employ techniques to manage smaller pupils and perform careful capsulorhexis and phacoemulsification, minimizing stress on the already fragile zonules. 6
PXF is a well-established risk factor for IOL subluxation or dislocation following cataract surgery. Studies report an approximately six-fold increased risk of dislocation in PXF patients. 7 Furthermore, PXF is implicated in over 50% of late IOL dislocations, complications estimated to occur in 1.7% of patients after 25 years. 7 These findings underscore the significant impact of PXF on surgical outcomes.
This case series describes the application of a novel scleral fixation technique, the “triangular suture technique” (TST) for scleral fixation of dislocated intraocular lenses (IOLs) in three PXF patients suffering from IOL dislocation. Using this technique an artificial sulcus is created posterior to the IOL optic and capsular bag. This technique restores the natural structure of the IOL-capsular bag complex through anteriorization and centration and is applicable to both vertically and posteriorly dislocated IOLs, with a similar surgical approach. This technique offers several potential advantages over existing methods. First, unlike traditional repositioning techniques that fixate the IOL at just two peripheral points, the triangular suture effectively cradles the IOL, providing central multi-point support along the suture path. This enhanced central support may reduce the risk of IOL tilt compared to techniques relying solely on peripheral fixation. Second, the procedure is designed for ease and speed of execution. Third, the TST might be suitable for anterior segment surgeons without posterior segment surgery experience. Notably, posterior vitrectomy, often required in other techniques, may not be mandatory with this approach and is reserved for cases with significant IOL dislocation and concern for vitreous prolapse into the anterior chamber. Finally, this technique holds promise as a preventive measure to enhance capsular support. It could potentially prevent clinically significant IOL dislocation in high-risk patients with substantial pseudophakodonesis.7,8
The triangular suture technique (TST)
The surgery begins with the administration of 1% tropicamide, 2.5% phenylephrine, and 1% Tetracaine eye drops at two 15-min intervals to facilitate peribulbar anesthesia and pupil dilation. Then, under aseptic conditions, retrobulbar anesthesia is administered. Aseptic conditions are ensured by applying a 5% solution of povidone-iodine to the periocular area and instilling it into the eye. The surgery commences with marking three limbal points at 2, 6, and 10 o’clock, which will serve as landmarks for the needle's transitions, as demonstrated in step 1 in Figure 1 that presents pictures taken during surgery and schematic illustrations of the different procedural steps. In cases where posterior vitrectomy is indicated, three trocars are inserted infero-temporally, supero-temporally, and supero-nasally 3.5 mm posterior to the limbus, with trocar positions verified (step 2). The next phase involves suture configuration and placement. A double-armed 10-0 Polypropylene suture (Prolene; Ethicon, Inc) with a 16-mm straight needle is inserted from 11 o’clock at a distance of 3.50 mm from the limbus into the posterior chamber behind the subluxated IOL. Then, a 25-gauge needle is used as a docking guide, inserted also 3.50 mm from the limbus into the posterior chamber behind the IOL and positioned 180° away toward the center. The needle is then pushed into the docking guide until is well captured (about 4–5 mm). The docking guide is then externalized, grabbing the needle inside along its length (step 3). Subsequently, the needle is passed under the conjunctiva in a direction from 3 o’clock to 9 o’clock (step 4). The same technique is applied, and a second transition is made from 7 o’clock to 1 o’clock (step 5), passing the needle under the conjunctiva toward 2 o’clock as shown (step 6). The last transition is from 2 o’clock to 10 o’clock (step 7), passing the needle under the conjunctiva toward 11 o’clock as shown (step 8). Maintaining a free suture length of approximately 2–3 mm when securing the suture knot is recommended. This length enables the thread to be buried harmlessly beneath the conjunctiva, preventing it from protruding and causing tissue injury. Conversely, an insufficient thread length may result in the suture becoming exposed, potentially leading to tissue irritation or erosion of the ocular surface (step 9). The case presented here suffered from a posterior dislocation with no significant decentration when lying prostrate. In cases where decentration exists, at this stage, a 23G limbal opening is made, and the intraocular lens (IOL) is centered and positioned atop the previously formed suture structure, allowing for straightforward centration and eliminating lens tilt. Figure 2 demonstrates the needle tract in the procedure (A) and the final triangular artificial sulcus created under the IOL at the end of the procedure (B). When indicated, a core or a complete vitrectomy is then performed (step 10), accompanied by a comprehensive 360-degree examination of the posterior pole. The surgical procedure concludes with the removal of all trocars, ensuring no leakage occurs. Subconjunctival Cefuroxime at a dosage of 1 mg is administered for infection prevention. Finally, the eye is patched and shielded for added protection. A detailed video demonstrating the surgical steps of the TST is available online (supplementary file 1).
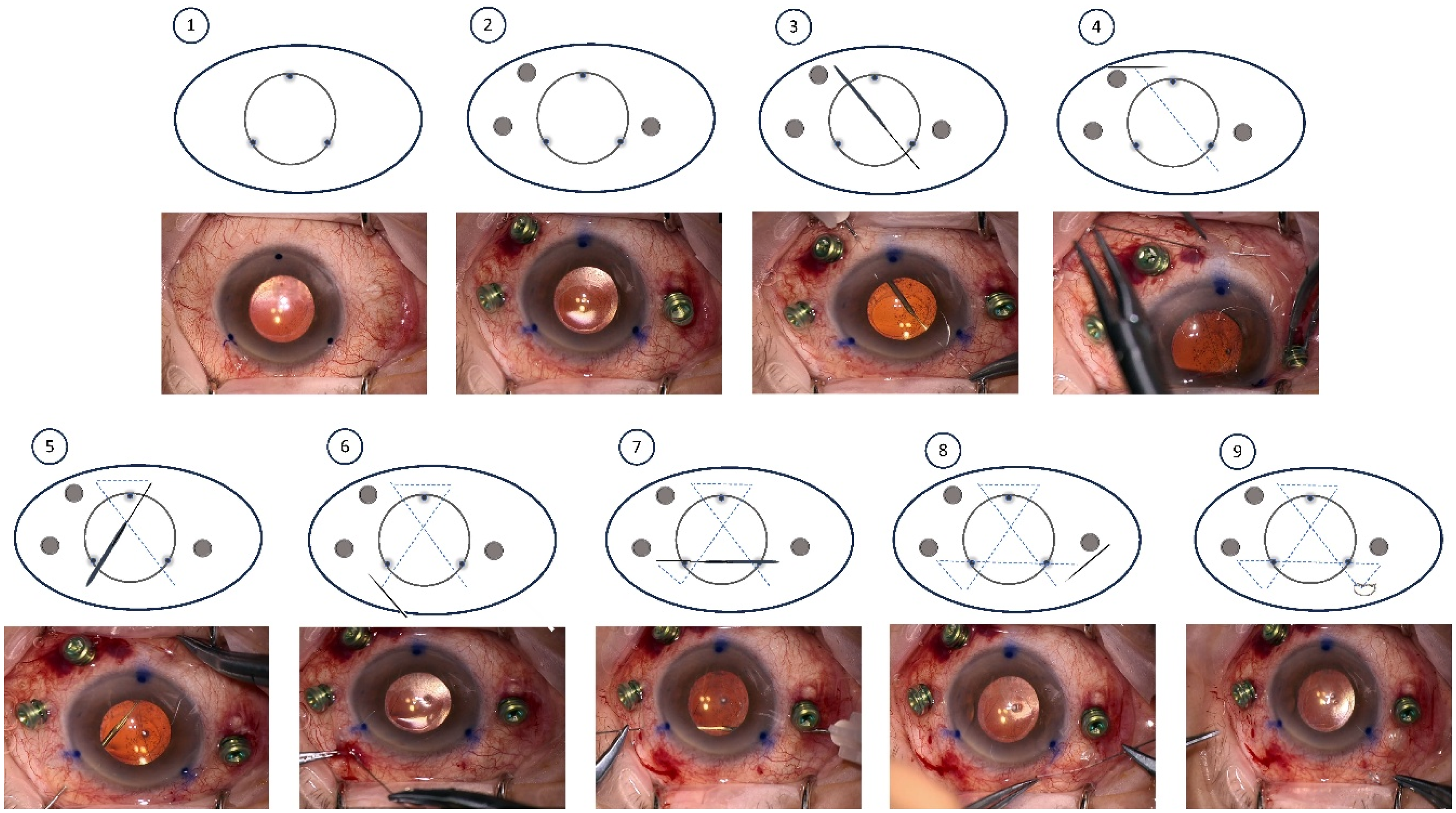
Intraoperative photographs accompanied by corresponding schematic illustrations demonstrating the key steps of the TST for IOL fixation.
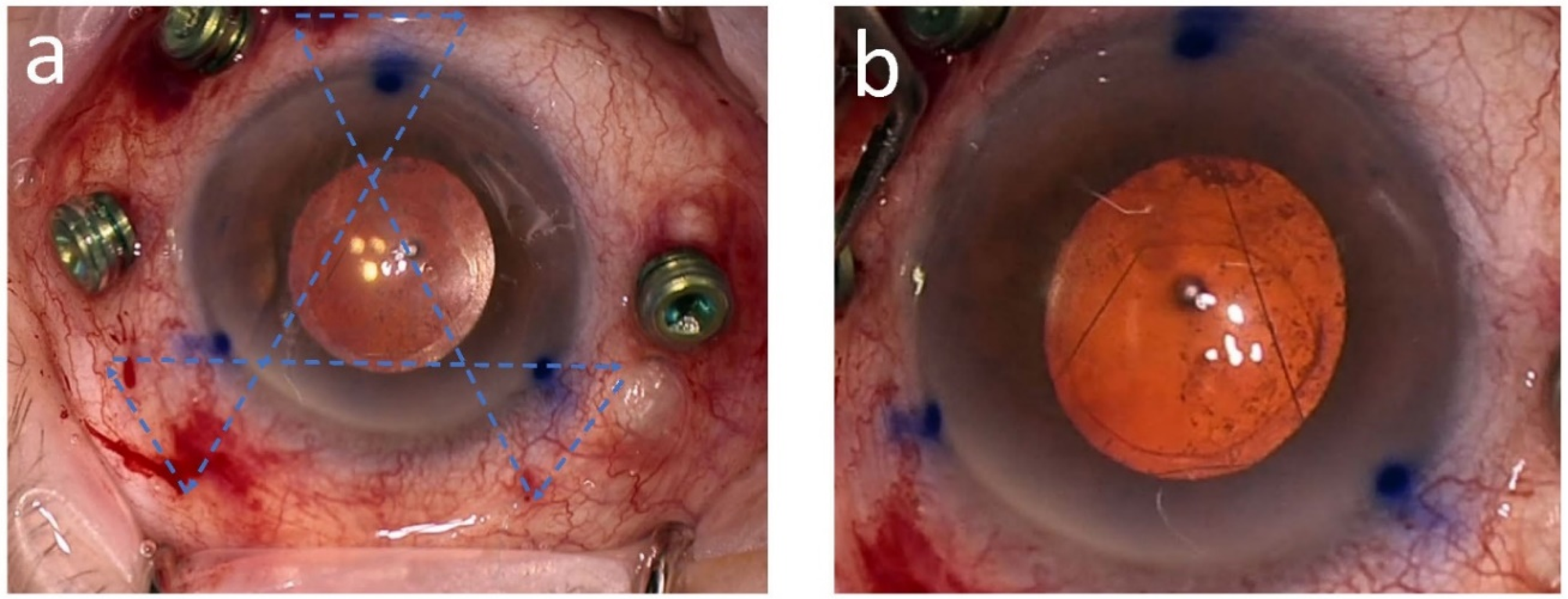
Intraoperative images demonstrating key steps of the triangular suture technique. Panel A: Intraoperative photograph demonstrating the needle tract during the procedure. Panel B: Intraoperative photograph showing the triangular artificial sulcus beneath the IOL at the end of the procedure.
Case 1
An 88-year-old woman with a history of pseudoexfoliation (PXF) syndrome and mild non-neovascular AMD underwent uneventful cataract surgery in the right eye with in-the-bag IOL implantation in 2013. The procedure achieved favorable outcomes resulting in a spherical equivalent of approximately plano and non- corrected visual acuity of 6/7.5. Four years post-operatively, the patient noticed a gradual, painless decline in vision in the operated eye. Ophthalmic examination revealed subluxation of the IOL due to zonulysis, with no reported history of trauma. Visual acuity at this stage was 6/8.5. Given these findings, it was decided to proceed with IOL scleral fixation using two Hoffman pockets. The surgery was uneventful, and the IOL was successfully repositioned. Six months later, the patient unfortunately experienced a recurrence of the IOL subluxation. This was accompanied by a gradual worsening of visual acuity in the operated eye over the subsequent months. On examination six months after the beginning of the symptoms, significant IOL dislocation and tilt were evident with posterior displacement of the IOL nasally and anterior displacement temporally, pushing the iris slightly forward as evident on the anterior segment OCT imaging (Figure 3a). The non-corrected visual acuity at this stage was 6/60. Given these findings, the decision was made to proceed with a second scleral fixation attempt, this time using the innovative TST. The surgery was uneventful and performed under retrobulbar anesthesia. The surgery was completed in in a brief 21 min. On postoperative day one, examination revealed good IOL centration despite poor visual acuity (hand motions) attributed to corneal edema. Anterior segment OCT performed seven days postoperatively confirmed good IOL centration and proper positioning within the posterior chamber (Figure 3b). At three months post-surgery, visual acuity improved significantly. Uncorrected visual acuity (UCVA) measured 6/15, with best-corrected visual acuity (BCVA) of 6/7.5. Refraction test revealed a spherical equivalent of −1.25 D with a total cylinder of −1.50 D at 23°. K readings demonstrated a corneal cylinder of −1.75 D at 8°, suggesting a corneal source for the majority of the astigmatism. No significant post-operative complications were documented in 3 months of follow-up.
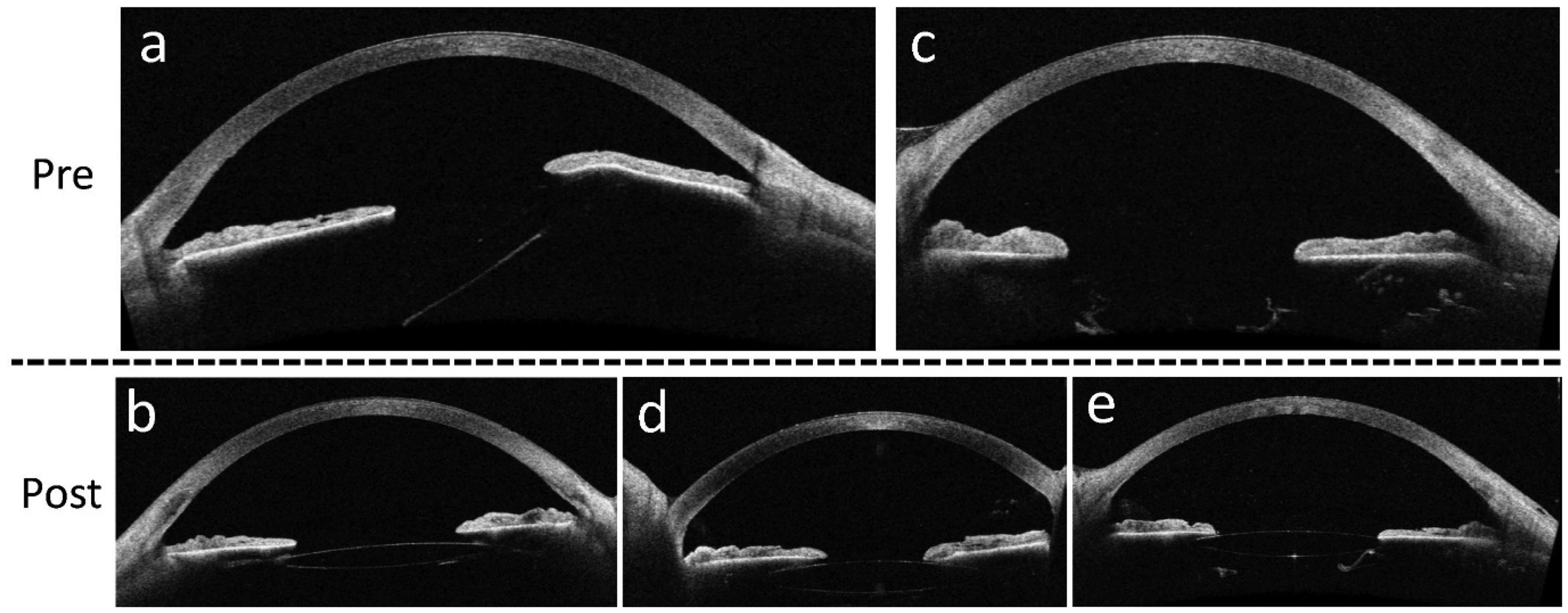
Preoperative and postoperative anterior segment OCT images demonstrating IOL dislocation and subsequent fixation using the TST.
Case 2
A 90-year-old man with a history of pseudoexfoliation (PXF) syndrome, bilateral pseudophakia, axial myopia (right eye: 27.0 mm, left eye: 26.79 mm) and a prior right eye dacryocystorhinostomy (DCR) for dacryostenosis presented to the emergency department with a one-month history of progressive, painless vision loss in the left eye, with a significant worsening ten days before arrival. No history of trauma was reported. Slit-lamp examination revealed significant posterior dislocation of the intraocular lens (IOL) due to zonular weakness. Anterior segment OCT confirmed the IOL malposition, demonstrating its absence from the expected location within the posterior chamber adjacent to the iris (Figure 3c). On arrival, uncorrected visual acuity (UCVA) was counting fingers at 1 meter. Refraction revealed a significant hyperopic shift (sphere +7.25 D, cylinder −1.00 D at axis 100°). Considering these findings and the potential risk of IOL prolapse into the vitreous cavity, the decision was made to proceed with triangular suture IOL scleral fixation for lens stabilization and centration. The procedure was performed uneventfully under retrobulbar anesthesia, successfully achieving good IOL repositioning. The surgery duration was brief, requiring only 35 min. On postoperative day one, examination revealed good IOL centration supported by the triangular configuration of 10-0 Prolene sutures positioned posterior to the optic. Anterior segment OCT confirmed good IOL centration and no tilt (Figure 3d). At one-week post-surgery, an expected myopic shift, attributed to the anteriorization of the lens position, was observed during refraction (sphere −1.50 D, cylinder −1.25 D at axis 109°). Uncorrected visual acuity (UCVA) was 6/120, and mild postoperative corneal edema was observed. By the three-week follow-up, best-corrected visual acuity (BCVA) improved to 6/20, and the IOL remained well-centered. No postoperative complications were identified, and intraocular pressure (IOP) remained well-controlled.
Case 3
An 82-year-old woman of Russian origin with a history of pseudoexfoliation (PXF) syndrome and topically controlled glaucoma (Latanaprost) underwent cataract surgery in the left eye. Intraoperatively, significant capsular instability was encountered during capsulorhexis, with prolapsed vitreous strands into the posterior chamber necessitating anterior vitrectomy. The IOL was eventually implanted in-the-bag using a capsular tension ring (CTR) for capsular support. One week postoperatively, examination revealed inferior IOL subluxation due to zonular weakness, with uncorrected visual acuity (UCVA) of 6/18. By four weeks, the subluxation had worsened, further reducing UCVA to 6/30. Given these findings, the decision was made to proceed with triangular suture IOL scleral fixation for lens stabilization and centration. The procedure was performed uneventfully under retrobulbar anesthesia, successfully achieving good IOL repositioning. The surgery duration was brief, requiring only 35 min. On postoperative day one, examination confirmed good IOL centration and stability. Subsequently, there was progressive improvement in visual acuity. At one-week post-surgery, uncorrected visual acuity (UCVA) improved to 6/15, with further improvement to 6/10 at six weeks post-operatively. One-week postoperative refraction revealed a spherical equivalent of −1.50 D with a total cylinder of −1.50 D at 82°, consistent with minimal IOL decentration and tilt. Six weeks post-surgery, anterior segment OCT confirmed good IOL centration and no tilt (Figure 3e). This innovative scleral fixation technique maintained IOL centration for nearly four years, with a final best-corrected visual acuity (BCVA) of 6/6.67 at last follow-up. No postoperative complications were observed, and intraocular pressure remained well-controlled with topical treatment alone.
Discussion
This case series describes our experience with a novel scleral fixation technique, the, TST for managing intraocular lens (IOL) subluxation in three patients with pseudoexfoliation (PXF) syndrome. All procedures were performed at our institution (Hadassah Medical Center, Jerusalem, Israel). This case series provides the first detailed description and illustration of the technique. The TST employs a prolene suture in a triangular configuration to craft an artificial sulcus underneath the IOL optic. This configuration facilitates both centration and stabilization of dislocated IOLs, minimizing tilt. 5 The technique also holds promise as a preventive measure in cases of severe pseudophakodonesis with compromised capsular support, potentially preventing future subluxation before it becomes clinically significant.5,6
The TST presents several advantages, each contributing to its appeal in intraocular lens (IOL) surgery. Firstly, it offers the potential for enhanced IOL support, distributing support across multiple central points along the IOL optic rather than relying on two-point fixation with IOL haptics. This multi-point support system holds promise for greater stability, although further research directly comparing this technique to others is warranted to fully understand its benefits. Additionally, the procedure is tailored for ease and speed of execution, boasting simplicity and a relatively short surgery duration of approximately 30 min in our case series. This efficiency not only benefits surgeons by streamlining the process but also appeals to patients seeking quicker procedures. Furthermore, the TST can reduce the need for vitrectomy, offering a viable option for anterior segment surgeons who lack training in vitreoretinal surgeries. This aspect expands the accessibility of the technique, potentially benefiting a broader range of practitioners and patients. Finally, the technique prioritizes IOL preservation, avoiding the more invasive route of IOL replacement. This approach mitigates the risks associated with larger corneal incisions, additional sutures, and postoperative complications such as leakage and astigmatism. By maintaining the original IOL, the TST presents a potentially less disruptive and more favorable alternative for patients undergoing IOL surgery.
In this case series, application of the TST achieved stable IOL centration and stabilization for up to four years, with improvement in visual acuity, minimal astigmatism, and no significant complications, including intraocular pressure spikes in both glaucomatous and non-glaucomatous eyes.7,9
This case series demonstrates the TST's promise as a safe and effective surgical approach for managing IOL subluxation in PXF patients. These encouraging results warrant further investigation to confirm the technique's long-term efficacy and safety compared to established methods. 10 Future studies with larger cohorts, broader inclusion criteria, and longer follow-up periods are necessary for a more comprehensive evaluation. Additionally, direct comparisons with other techniques would be valuable in determining the optimal treatment strategy.
Footnotes
Statement of ethics
Written informed consent was obtained from the patients for the preparation of this work (including publication of images).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.