
Abstract
Purpose
To investigate safety and efficacy of the XEN gel stent in patients with pigmentary glaucoma (PG).
Methods
A retrospective analysis of 26 eyes of 19 patients with PG undergoing XEN gel stent implantation was performed. Best-corrected visual acuity, intraocular pressure (IOP), and number of antiglaucoma medications were analyzed preoperatively, and at 2 weeks and 3, 6, 12, and 24 months after surgery. Success, needling, and complications were analyzed. Complete success was defined as an IOP reduction of >20% and achieving a target IOP of ≤18, ≤15, or ≤12 mmHg without antiglaucoma medication. Qualified success was indicated if the IOP target was reached with or without medication.
Results
Mean IOP decreased significantly from 27.6 ± 14.3 (standard deviation, SD) mmHg to 14.3 ± 4.6 mmHg after one year (p < 0.001) and 15.1 ± 2.7 mmHg (p < 0.001) after two years. The median number of hypotensive drugs declined significantly from 4 (range: 3–5) to 0 (0–2) and 0 (0–3) after one and two years, respectively. After two years, complete success with an IOP of ≤18 mmHg and ≤15 mmHg was achieved in 73.1% and 61.5%, respectively. Half of the eyes required needling after a median time of 8 months (0.5–34 months). No sight-threatening complications were observed.
Conclusion
The XEN gel stent is a safe and effective surgical treatment option for PG. Needling is an important part of the procedure and should be communicated preoperatively to the patients.
Introduction
Pigmentary glaucoma (PG) is a secondary open-angle glaucoma with a regionally varying prevalence, 1 , accounting for between 0.6% and 1.5% of all glaucoma cases.2–5 An Indian study suggested a population prevalence of only 0.04% 6 while an incidence of 1.4/100,000 per year was detected in a US American study. 7 PG accounts for 0.6% of all glaucoma patients in Congo, 2 0.92% in China, 3 and 1 to 1.5% of all glaucoma cases in the Western countries.4,5 The prevalence of PG is higher in men and in patients with myopia. 8 PG typically occurs between the third and fourth decade of life.9,10 Characteristic is the clinical pattern of Krukenberg's spindle, mid-peripheral transillumination defects of the iris, posterior bowing of the iris, and homogeneously increased pigmentation of the trabecular meshwork.11,12 The concavity of the iris shape causes a rubbing of the posterior iris pigment epithelium against the lens zonules, releasing pigment into the anterior chamber.13,14 The term PG is used only if, in addition to the signs of pigmentary dispersion, the optic nerve is damaged and/or visual field defects are present. 15 The risk for individuals with pigment dispersion to develop PG has been estimated at 5–10% at five to six years after diagnosis,7,16 and 15% at 15 years. 7 Other studies, however, suggested higher conversion rates of 20% at seven years, 17 or 50% at four years. 11
Treatment options for PG are the same as in primary open-angle glaucoma (POAG). Surgical treatment is usually considered if antiglaucoma medication fails to provide adequate control of intraocular pressure (IOP). Trabeculectomy is still considered the gold standard but is associated with several sight-threatening complications such as hypotony maculopathy, late-onset bleb leakage, and endophthalmitis.18,19 The XEN gel stent (AbbVie Inc., North Chicago, IL, USA) is a bleb-forming minimally invasive glaucoma surgery device, which has been developed with the goal to reduce the risks of filtration surgery. It is a 6 mm long gelatin tube, which is inserted ab interno without a conjunctival incision. Two models with different lumen sizes (45 µm and 63 µm) are currently available. The XEN45 gel stent has been shown to be effective and safe in the treatment of POAG and other open-angle glaucoma forms.20–22 Studies have confirmed the efficacy and safety of the XEN45 gel stent in pseudoexfoliation glaucoma23,24 and in uveitic secondary glaucoma.25,26 However, little is known about the role of the XEN gel stent in the treatment of PG. The aim of this study was to investigate the efficacy and safety of XEN45 gel stent implantation in patients with PG.
Materials and methods
Study design
This was a retrospective study of patients with PG who underwent XEN45 gel stent implantation between July 2016 and October 2020 at a single tertiary center. Patients with PG inadequately controlled on maximum tolerated medication, and a minimum postoperative follow-up period of 12 months, were included. Exclusion criteria included any subtype of glaucoma other than PG, a history of uveitis, or insufficient follow-up data. Previous glaucoma surgery or laser treatment was not an exclusion criterion. Informed consent was obtained from each patient prior to surgery. Ethical approval was granted by the ethics committee of the University of Tübingen (project number: 423/2021B02). Because of the retrospective study design, the need for consent for the study was waived by the ethics committee. The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Surgical technique
Surgery was performed by a single experienced surgeon. Under topical anesthesia with oxybuprocaine eye drops, two points at a distance of 3 mm from the limbus were marked in the superonasal quadrant. A small bubble of 25 µl of mitomycin C (MMC; 0.2 mg/ml, resulting in 5 µg of MMC) was injected into the subconjunctival space at 5 mm from the limbus at the 12 o’clock position. In three cases, 100 µl (20 µg) MMC was used, and in one case, 100 µl of 5-FU (50 mg/ml, resulting in 5 mg 5-FU) was applied instead. The bleb was gently moved over the anticipated area for micro-stent insertion in the superonasal quadrant. This injection technique aimed to avoid subconjunctival bleeding in the area of the intended filtering bleb. A 20G side-port knife was used for the main incision 1 mm inferotemporally into the clear cornea and a smaller side-port incision at the 11 o’clock position or the 2 o’clock position for the right or left eye, respectively. After injection with lidocaine, the anterior chamber was filled with the Healon® PRO Ophthalmic Viscoelastic Device (OVD; Johnson & Johnson, NJ, USA). The XEN45® injector was inserted through the main incision in the anterior chamber, with the needle pointing toward the superonasal quadrant, under gonioscopic control. Then, the needle was carefully advanced through the sclera and into the subconjunctival space 3.0 mm from the limbus between the two marked points. The gel stent was then released, and the injector was withdrawn. After the correct position of the gel stent had been verified, the viscoelastic material in the anterior chamber was flushed out with balanced salt solution, which resulted in formation of a filtering bleb. Cefuroxime was injected into the anterior chamber at the end of the procedure.
Preoperative and postoperative management
Baseline IOP was assessed under the patients’ topical antiglaucoma medication when the indication for surgery had been made. Two weeks prior to surgery, the topical therapy was discontinued, and oral acetazolamide (250 mg twice daily) and unpreserved dexamethasone eye drops (four times daily) were administered until the night before surgery. No medication was given on the day of surgery. After surgery, moxifloxacin eye drops were administered four times daily for 1 week. Additionally, unpreserved dexamethasone eye drops were administered with a tapering dose regimen over 7 weeks, starting with five drops per day on the first postoperative day. Patients were examined on the first two postoperative days, including a funduscopic exam with dilated pupil. Further follow-up visits were scheduled at 2 weeks, as well as at 3, 6, 12, 18, and 24 months, after surgery.
In cases of inadequate IOP control in the postoperative course, needling was performed first, instead of prescribing IOP lowering medication. The indication for needling was also given if any clinical signs of scarring of the filtering bleb were detected. The decision to perform needling was made at surgeon's discretion.
Needling was performed under topical anesthesia with oxybuprocaine eye drops, as previously described. 25 A 30G needle was bent and used to inject a small subconjunctival bubble of mepivacaine next to the XEN gel stent. Fibrotic tissue around the gel stent was then disrupted with sweeping movements of the needle tip. The stent was gently moved to assure free mobility of its tip. The decision to inject 5-FU or MMC or no antimetabolites was made intraoperatively by the surgeon. After needling, moxifloxacin eye drops were prescribed four times daily for 3 days, starting on the first postoperative day. Additionally, unpreserved dexamethasone eye drops were administered with a tapering dose regimen over 5 weeks, starting with five drops per day on the first postoperative day.
Outcome measures
The methodology of this study is based on the World Glaucoma Association (WGA) guidelines for the design, conduct, and reporting of glaucoma studies. 27 The primary outcome of the study was the change in IOP after two years. Secondary outcomes included the number of antiglaucoma medications, changes in best-corrected visual acuity (BCVA), success rates, needling rate, and complications rate. In accordance with the WGA guidelines, success of the procedure was defined as a reduction in IOP of >20% and achieving a target IOP of ≤18 mmHg. Success rates were additionally analyzed with IOP cutoff levels of ≤15 mmHg and ≤12 mmHg. Complete success indicated that the target IOP was reached without antiglaucoma medication, while qualified success indicated that the target IOP was achieved with or without additional medication. Preoperative and postoperative numbers of medications were defined as the total number of classes of hypotensive drugs being used. In the case of combination preparations, the individual active ingredients were considered. Hypotony was defined as an IOP of <6 mmHg. Failure was defined as loss of light perception or the need for additional surgical procedures, other than needling, for IOP control. Complications were referred to as early or late when they occurred within or after the first postoperative month, respectively, in accordance with the recommendations of the WGA guidelines. 27
Statistical analysis
The JMP 16.0 statistical package (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis. Data were expressed as number (percentage), mean (standard deviation [SD]), mean (95% confidence interval [95% CI]), or median (range) as appropriate. A paired-sample t-test was performed to compare normally distributed data, and the Wilcoxon signed-rank test was used to evaluate changes for non-normally distributed data. Success rates were assessed using a Kaplan–Meier analysis. P-values below 0.05 were considered statistically significant.
Results
Characteristics of the population
In this study, 26 eyes of 19 patients with PG were included. Demographic and ocular baseline characteristics of the study population are described in Table 1.
Baseline characteristics of the study population.
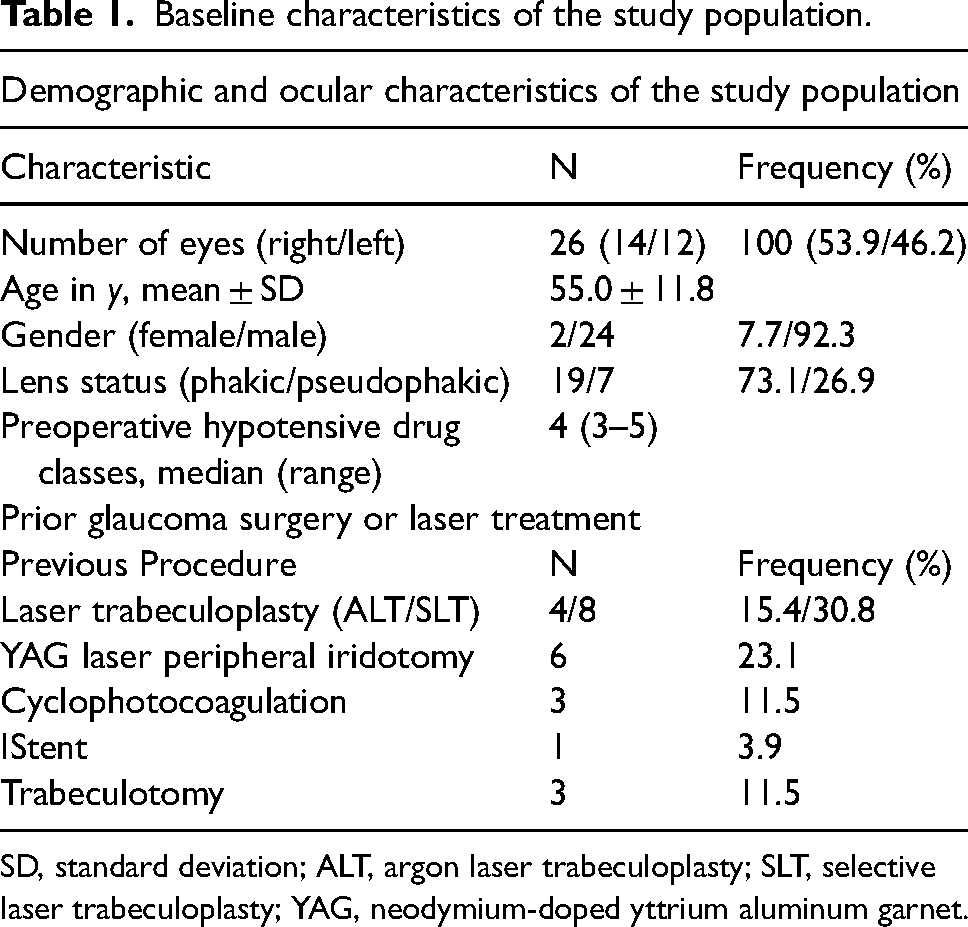
SD, standard deviation; ALT, argon laser trabeculoplasty; SLT, selective laser trabeculoplasty; YAG, neodymium-doped yttrium aluminum garnet.
Development of IOP control, best-corrected visual acuity (BCVA), and medication
The mean IOP decreased from 27.6 ± 6.6 mmHg to 14.3 ± 4.6 mmHg after one year (p < 0.001) and to 15.1 ± 2.7 mmHg after two years (p < 0.001). This equates to an IOP reduction of 48.3% and 45.4% after one and two years, respectively. The median number of antiglaucoma medications was reduced significantly from 4 (3–5) to 0 (0–2) after one year and to 0 (0–3) after two years (p < 0.001 for both). The mean IOP values and numbers of medications taken at every visit are shown in Figure 1. In Figure 2, IOP changes at one and two years postoperatively are visualized in a scatterplot. BCVA did not change significantly (baseline: 0.13 ± 0.26 logMAR) after one year (0.11 ± 0.19 logMAR; p = 0.48) or after two years (0.14 ± 0.26 logMAR; p = 0.67). None of the patients had a worsening of visual acuity greater than 0.2 logMAR.
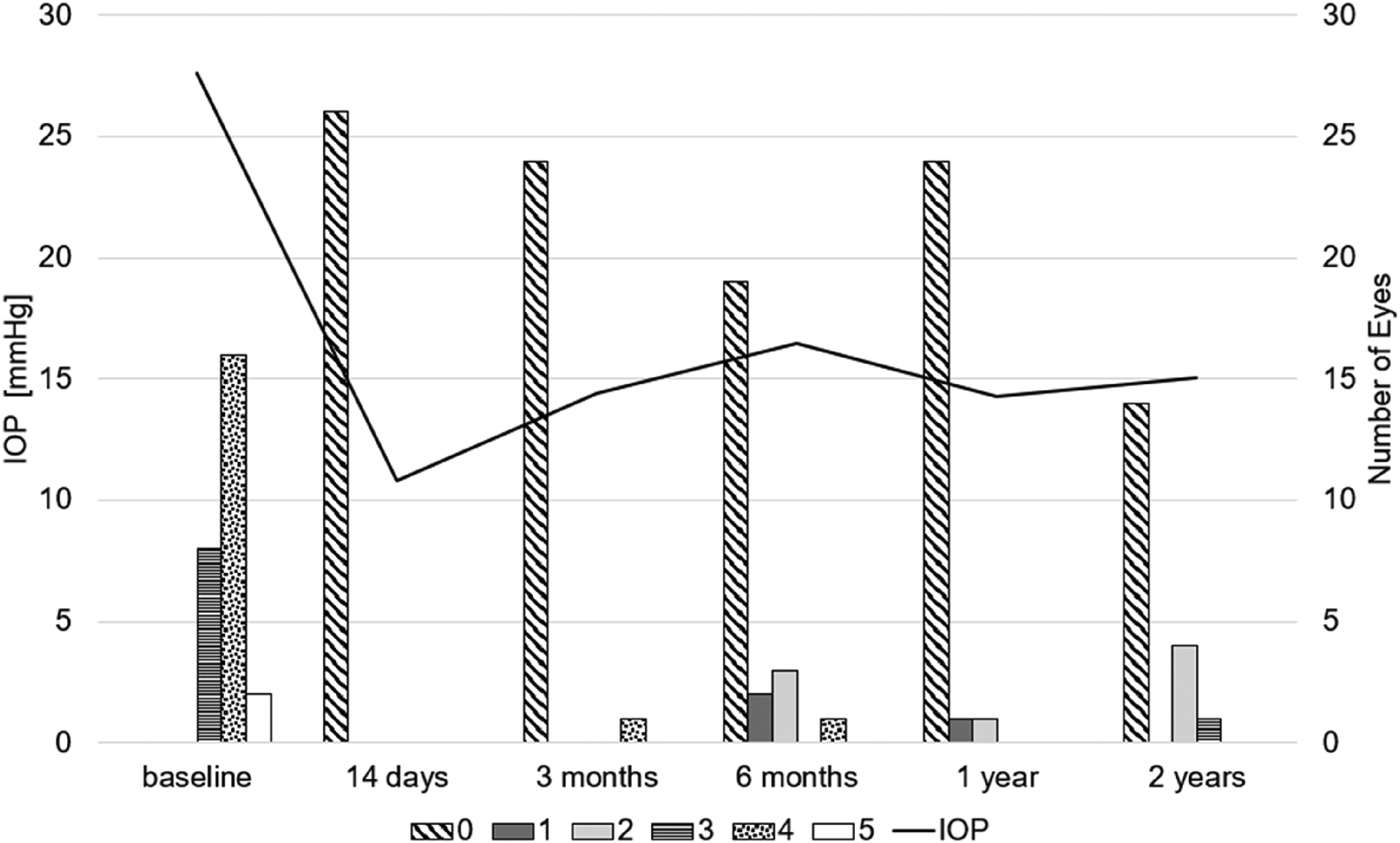
Mean IOP at every visit is plotted as a black line. The bar chart shows the absolute number of eyes taking a specific number of hypotensive drugs at each visit. Fixed combination medications were counted according to the number of active ingredients contained. IOP, intraocular pressure.
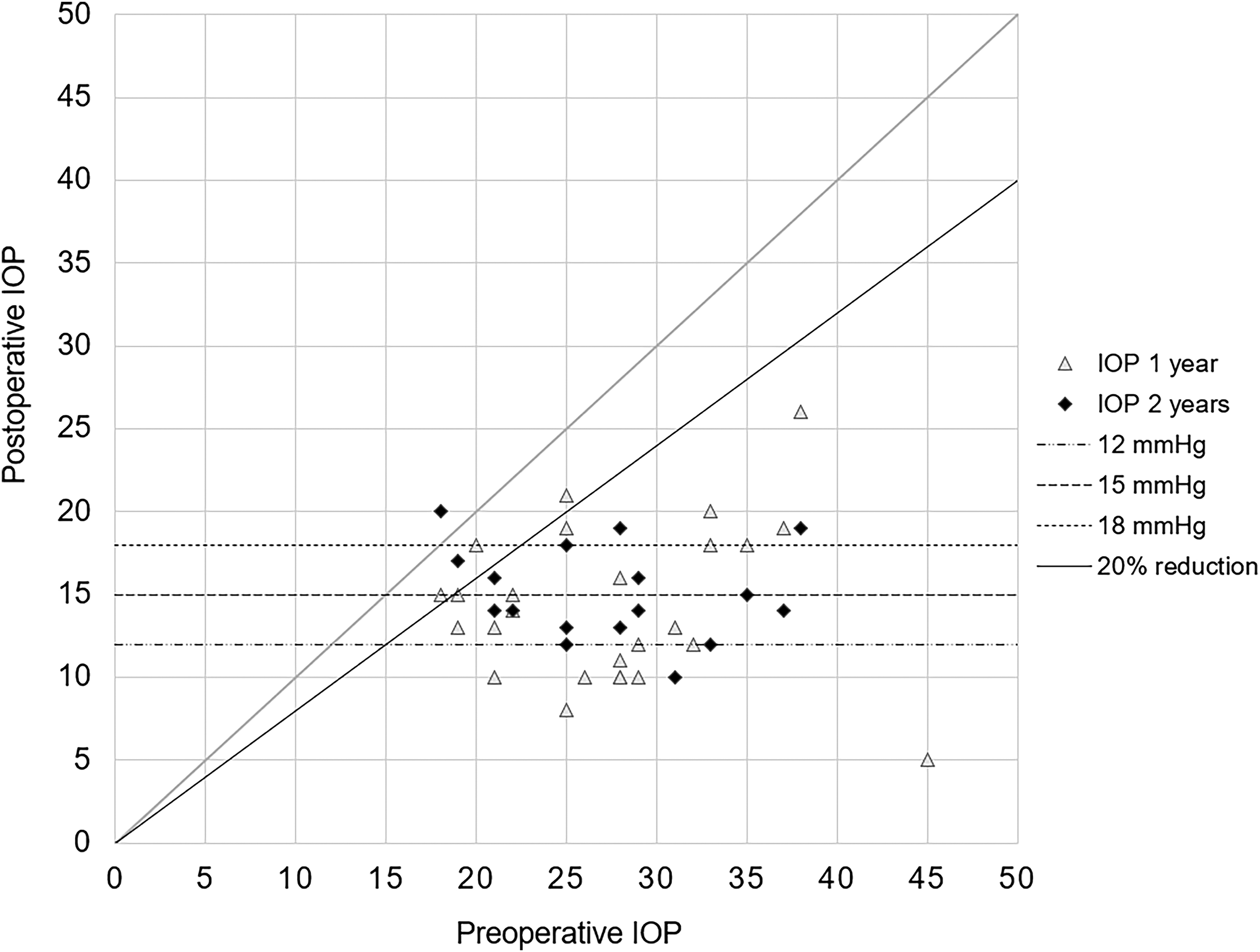
Scatterplot of IOP development 1 and 2 years after XEN45 gel stent implantation. IOP, intraocular pressure.
Success rates
With an IOP cutoff level of 18 mmHg, complete success was achieved in 73.1% of the patients after both one and two years. Qualified success was achieved in 80.8% of the patients after both one and two years. Regarding the IOP cutoff level of 15 mmHg, 61.5% had complete success and 65.4% achieved qualified success at both time points. At the IOP cutoff level of 12 mmHg, 38.5% of the patients achieved complete success after one and two years, and the qualified success rate did not differ from the complete success rate at the two time points. The Kaplan–Meier curve for each IOP level is shown in Figure 3.
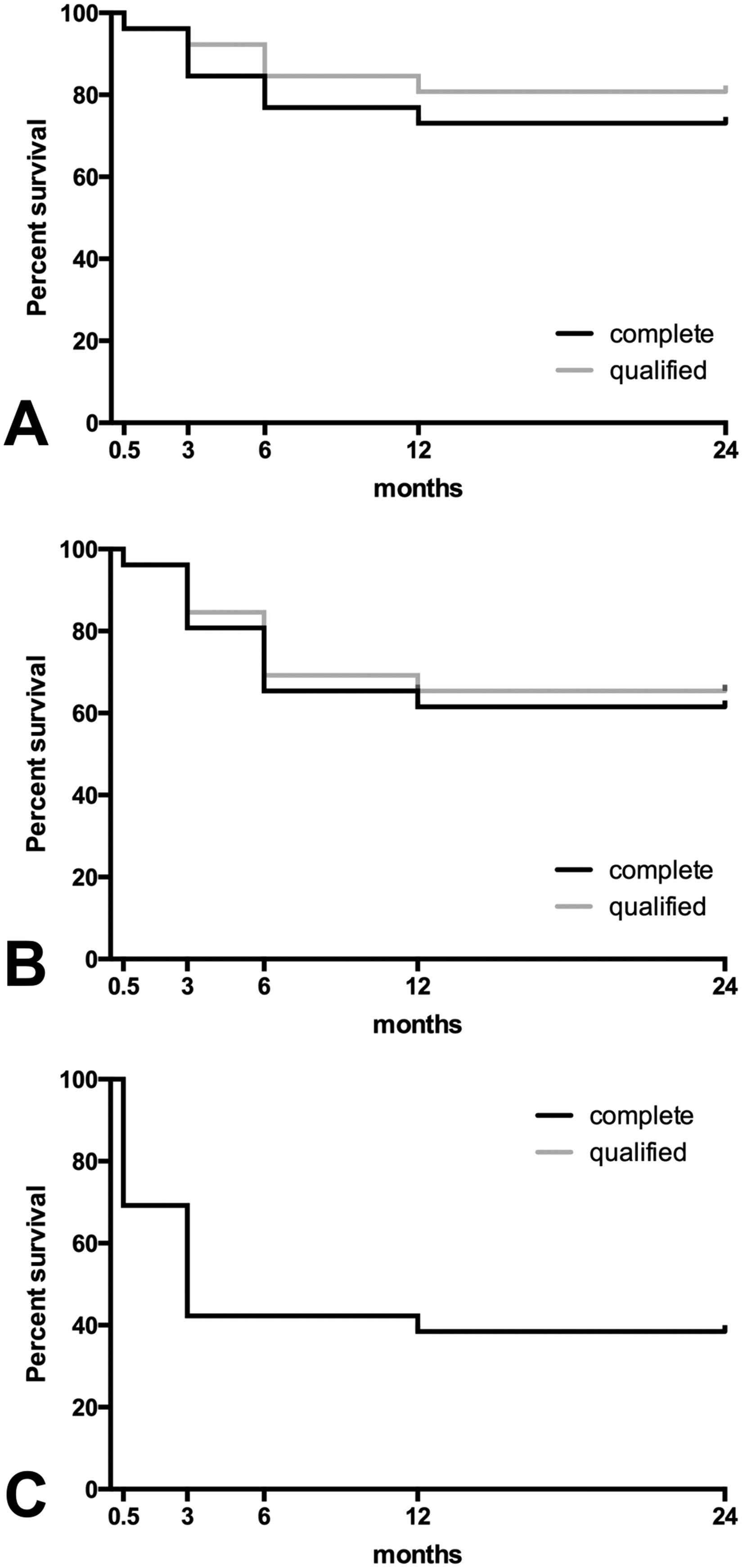
The Kaplan–Meier survival analysis at 2 weeks and 3, 6, 12, and 24 months after XEN45 gel stent implantation. “Complete success” was defined as an IOP reduction of ≥20% and achievement of the respective target IOP without antiglaucoma medication. “Qualified success” indicates that the same criteria have been met with or without additional antiglaucoma medication. The survival rates with IOP cutoff set at (A) ≤ 18 mmHg, (B) ≤15 mmHg, and (C) ≤12 mmHg. IOP, intraocular pressure.
Needling
A needling procedure was necessary at least once in 13 eyes (50.0%) to maintain the functionality of the filtering bleb during the postoperative course. The median time to the first needling was 8 months (range: 0.5–34 months). In nine eyes (34.62%), a second needling was necessary at a median time to needling of 9 months (range: 3–18). In three eyes (11.5%), a third needling with 5-FU (one eye) or MMC (two eyes) at a median time to needling of 11 months (range: 11–18) was performed. An overview of the postoperative needling procedures carried out and details on the use of antimetabolites are provided in Table 2.
Overview of postoperative bleb interventions and frequency of peri- and postoperative complications.
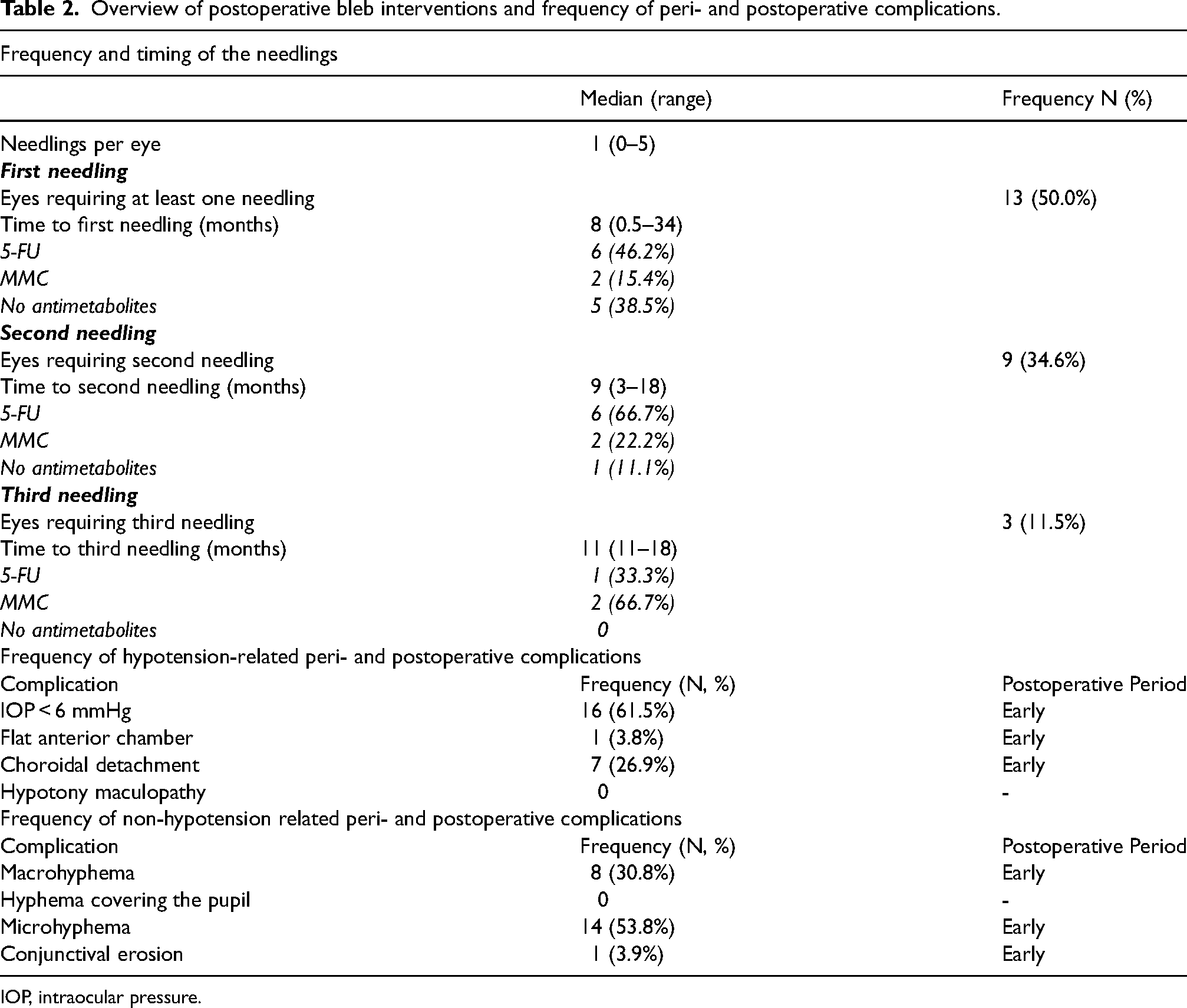
IOP, intraocular pressure.
Perioperative and postoperative complications
Transient hypotony was the most frequent complication, occurring in 16 eyes (Table 2). Hypotony recovered spontaneously in nine of those eyes within 2 weeks. The other seven eyes showed transient choroidal detachment. In five of those, the choroidal detachment receded spontaneously within 14 days. In the other two eyes, a Healon® injection into the anterior chamber was administered and resulted in complete recovery. A flat anterior chamber was noticed in one eye on the first postoperative day. The anterior chamber recovered after instillation of Healon®. At the 3-month follow-up visit, none of the eyes showed an IOP of <6 mmHg or other signs of hypotony. We did not observe any case of hypotony maculopathy.
Microhyphema (flared or layered blood of ≤1 mm in the anterior chamber) was the second most common postoperative complication. In all eyes, hyphema resolved spontaneously and without sequelae within 4 weeks.
In one case, a conjunctival erosion over the implant was reported at the 14-day follow-up visit. The erosion was successfully closed with a conjunctival suture. At the subsequent visits, no conjunctival defect was present. No sight-threatening complications were observed throughout the follow-up period. An overview of the perioperative and postoperative complications is presented in Table 2.
Failure
None of the eyes lost light perception. Two eyes (7.7%) failed because of inadequate IOP regulation; one underwent trabeculectomy and the other required implantation of a PreserFlo® MicroShunt.
Discussion
The efficacy and safety of the XEN45 gel stent in various types of glaucoma have been demonstrated in several studies.28–30 To the best of our knowledge, this is the first study demonstrating long-term efficacy and safety of the XEN45 gel stent in patients with PG.
Several studies exist investigating the XEN gel stent in POAG or in heterogeneous study populations with mixed open-angle glaucoma subtypes. In a large multicenter case series from the UK with a heterogeneous mix of glaucoma types, also comprising PG patients, a 26.4% IOP reduction after 12 months was detected. 31 Other studies on XEN in POAG previously observed IOP reductions of 25.0%, 32 29.3%, 33 and 41.8% 34 after one year. In comparison, our study revealed a higher efficacy, with an IOP reduction of 48.3% after one year. Thus, the efficacy of the XEN gel stent does not appear to be inferior in PG compared with POAG.
In a prospective study examining the XEN45 gel stent in 64 patients, Lenzhofer et al. did not find any differences in efficacy between patients with PG or POAG. 35 However, only 7% of the study population had PG. The authors observed a mean IOP reduction after four years was 40%. 35 Although safety was not specifically reported in the PG group in the study by Lenzhofer et al., overall, the authors did not observe any sight-threatening complications. These results compare well to our study, with similar reductions in IOP and medications after two years.
Trabeculectomy is effective in the treatment of PG in the long-term as shown by an eight-year Chinese study. 36 In this study, IOP was significantly reduced from 34.5 ± 4.7 mmHg to 13.7 ± 2.5 mmHg eight years after trabeculectomy, which is a greater percentage reduction in IOP and a slightly lower final IOP compared to our results. Another study comparing Trabectome in patients with PG and POAG found similar success rates between both groups one year after surgery, with an IOP decreasing from 24.4 ± 7.7 mmHg to 17.1 ± 5.0 mmHg in PG patients. 37 In comparison, the IOP was lower one year after XEN implantation in our study.
In a retrospective case series of 12 patients with PG undergoing combined phacoemulsification and trabecular micro-bypass stent implantation, a mean IOP reduction of 25% after 36 months was achieved, without any cases needing additional surgery. 38 The mean IOP decreased from 19.50 ± 6.7 mmHg to 14.68 ± 3.0 mmHg at 36 months postoperatively. An IOP reduction of ≥20% was reported in 55% of the eyes after three years. 38 In comparison, although our study had a shorter follow-up, mean IOP outcomes were similar and the success rate was higher, which is noteworthy as our success criteria were stricter.
Needling is often required after filtering surgery in order to improve the function of the filtering bleb. Needling rates after XEN45 gel stent implantation vary between 14.1% and 51.3% after one year21,29,32,34,39 and between 37.7% and 45% after two years21,40–42 in various types of open-angle glaucoma. In comparison, the needling rate in our study was 50% after two years. However, needling rates are difficult to compare because the decision to perform needling is solely at the surgeon's discretion and no universally accepted needling criteria exist. In our understanding, the goal of filtering surgery is to provide adequate IOP control without antiglaucoma medication. Therefore, we perform a needling procedure instead of starting antiglaucoma medication in patients whose IOP is not well controlled or when signs of a fibrotic bleb occur. This approach is demonstrated by similar complete and qualified success rates in our study. Also, younger age is a known risk factor for bleb failure after filtering surgery.43–45 Notably, the mean age of our cohort was lower than in previous studies of the XEN45 gel stent in POAG.
Various frequencies of transient postoperative hypotony are reported in former studies on XEN gel stent in POAG and mixed glaucoma types, including 2%, 42 2.4%, 46 2.8%, 47 20.5%, 34 and 34.7%. 31 Many of the studies reporting very low rates of hypotony, however, defined hypotony as the presence of choroidal effusion or detachment. In our study, hypotony was defined as an IOP of <6 mmHg and was detected in 61.5%, whereas choroidal detachment appeared in 26.9% of the cases. In comparison, our rates of hypotension and choroidal detachment are relatively high. This could be due to the demographic and pathophysiological differences between PG and POAG. PG tends to occur in younger and myopic people, and myopic eyes are at higher risk of postoperative hypotony after XEN gel stent implantation, 48 deep sclerectomy, 49 and trabeculectomy. 50 However, in every case of hypotension observed in our study, complete recovery was achieved within the first 14 postoperative days, either spontaneously or after instillation of Healon®. Previous studies comparing XEN gel stent implantation and trabeculectomy in open-angle glaucoma found higher rates of hypotension following trabeculectomy.51–53 In the literature, the rates of hypotony after trabeculectomy vary widely, also depending on the definition of hypotension in each study. Hypotony rates between 2% 44 and 69.6%, 54 and up to 85.7% in a study on highly myopic eyes, 52 are described.
Regarding transient hyphema as a complication after XEN gel stent implantation, Widder et al. reported a frequency of 5.6% in an open-angle glaucoma study, 28 while Hengerer et al. observed a very low hyphema rate of 1.7%. 22 Here, as well, the definition of hyphema differs depending on the study, which makes it difficult to compare them. In the current study, we reported microhyphema as early as the appearance of erythrocytes in the anterior chamber on slit-lamp examination in the first postoperative days, probably leading to comparatively higher frequencies. In every case of hyphema observed in our study, complete recovery was observed within 14 days postoperatively.
We acknowledge that our study has several limitations due to its retrospective design. Most of the eyes received 5 µg MMC, but 20 µg MMC was used in three eyes and 5-FU was used in one eye. These numbers were too small to analyze which MMC dose is most appropriate. Our earlier data (not yet published) demonstrated, however, comparable efficacy of the XEN45 gel stent used with 5 µg, 10 µg, or 20 µg MMC. In addition, the use of antifibrotic agents during the needling procedures was at the discretion of the surgeon. Again, the low number of eyes receiving MMC, 5-FU, or no antifibrotic agent did not allow further analysis of the data.
In conclusion, our study demonstrated a mean IOP reduction of 45.4% and a complete success rate of 73.1% (for the cutoff level of 18 mmHg) after two years. The complications were manageable, and we did not observe any sight-threatening events. Half of the eyes required at least one needling procedure during the two years of follow-up. Needling is an important part of minimally invasive bleb surgery with the XEN45 gel stent, and this should be communicated preoperatively to the patients.
Footnotes
Acknowledgements
We gratefully acknowledge Dr. Gunnar Blumenstock from the Institute for Clinical Epidemiology and Applied Biometry, Eberhard Karls University of Tübingen, for his valuable support with statistical analysis in the study.
Contributors
CJG analyzed data and wrote the manuscript; EN analyzed data; DAW analyzed data and revised the manuscript; BV designed the study and revised the manuscript. All authors have read and approved the final manuscript.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
BV has received speaker honoraria from AbbVie, Santen and Novartis. CJG, EN, and DAW declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was granted by the ethics committee of the University of Tübingen (project number: 423/2021B02). The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Funding
CJG was supported by the Junior TÜFF program of the Medical Faculty, Eberhard Karls University of Tübingen (application number: 2723- 0-0).
Informed consent
Informed consent for surgery was obtained from each patient prior to surgery. The need for consent to the study was waived by the ethics committee in view of the retrospective design and all the procedures being performed were part of the routine care.