
Abstract
Purpose
Radiation-induced scleral necrosis (RISN) is a less frequent complication of brachytherapy for uveal melanoma, and may require surgical treatment in selected cases. We aimed to identify the prognostic factors for RISN treatment.
Methods
All patients with brachytherapy for uveal melanoma treated at our institution between 01/1999 and 12/2016 who developed RISN were followed until 02/2021. Various parameters were evaluated through univariable and multivariable Cox regression analysis. The surgical intervention due to RISN was the principal outcome event of this study.
Results
Of 115 patients in the final cohort, 51 individuals (44%) underwent RISN treatment (conjunctival revision [n = 2], patching [n = 46] or enucleation [n = 3]) at median 1.80 months after RISN occurrence. Significant RISN characteristics were summarized into a novel RISN severity scale – Grade I: largest diameter ≤ 5 mm and no progression; Grade II: largest diameter > 5 mm or any progression during the follow-up; Grade III: presence of uveal prolapse; and Grade IV: leakage through open eyewall perforation. In the multivariable analysis, the RISN severity scale (aHR = 2.37 per grade increase, p = 0.01) and the time between brachytherapy and RISN occurrence (<15 months, aHR = 6.33, p < 0.0001) were independently associated with the study endpoint. The RISN severity scale showed high diagnostic accuracy for prediction of RISN treatment (AUC = 0.869).
Conclusions
In our series, about the half of RISN cases underwent surgical treatment. The presented novel severity scale for RISN might become a helpful tool for clinical management of individuals with RISN. We recommend external validation of the diagnostic accuracy of the presented scale.
Introduction
Since brachytherapy has been established as standard therapy for small- and middle-sized uveal melanoma (UM) 1 the management of its possible complications has great importance for therapy success. The radiation induced complications can be divided into early ones, that can occur within first weeks after brachytherapy (exudative retinal detachment, choroidal detachment, extensive tumor necrosis with toxic tumor syndrome, and conjunctival dehiscence) and delayed ones occurring up to years after the radiation (neovascular glaucoma, cataract, radiation retinopathy and radiation-induced optic neuropathy, vitreous hemorrhage).2–5 Timely identification and treatment of these complications is essential for preservation of the visual function and the eye itself.
Radiation-induced scleral necrosis (RISN) is considered as a rare complication after brachytherapy of UM with the incidence of about 1–11% in large series.2,5–9 Depending on the severity and clinical course, RISN might require a special treatment in selected cases.5,10–12 While for stable and mild RISN cases proper management consists of long-term observation, progressive RISN can threaten the tectonic stability of the eye and require surgical treatment like patch grafting.5,12 Furthermore, a RISN complicated with a leaky wound of an eyewall perforation might not be eligible for reconstructive surgery and therefore necessitate enucleation of the affected eye.5,10,12
As RISN is a rare complication, the literature on its management and, particularly, the evidence on the prognostic factors requiring RISN treatment are sparse. To the best of the authors’ knowledge, there is no validated classification of RISN severity. In order to fill this gap, we analyzed the course of RISN after brachytherapy for UM to identify the prognostic factors for RISN treatment. Based on the significant RISN characteristics, we have established a novel severity scale for RISN.
Materials and methods
Study design and study population
This retrospective study was approved by the Institutional Ethics Committee (Ethik-Kommission, Medizinische Fakultät der Universität Duisburg-Essen, registration number 18-8190-BO) and registered in the German clinical trial registry (DRKS, Unique identifier: DRKS00019049). The study is based on the institutional observational cohort UM patients who underwent brachytherapy at the Clinic for Ophthalmology and Radiology of University Hospital of Essen between January 1st, 1999 and December 31st, 2016. All cases with RISN documented until August 31st, 2019 were included in the final analysis. The Informed consent was obtained from all patients within the written treatment contract signed on admission.
Detailed description of UM management was published previously. 6 In short, the tumors with largest initial tumor thickness up to 6.5 mm were treated with 106Ru plaques. For larger tumors, bi-nuclide 106Ru- 125I plaques were used. The common prescribed tumor apex dose was ≥ 130 Gy for ruthenium or ranged between 70–100 Gy for bi-nuclide plaques respectively. The common prescribed sclera dose was 700–1500 Gy.
For tumor control and surveillance of radiation-related complications after brachytherapy, all patients underwent regular follow-ups at our outpatient service. According to the institutional policy, the initial follow-ups were performed in 3-months intervals in the first year. In cases with stable disease, the intervals were prolonged up to once every year. After first RISN detection patients with RISN underwent follow-ups at shorter time intervals (4-6 weeks), depending on the severity of necrotic changes in the sclera.
Full thickness scleral defect and RISN accompanied with conjunctival dehiscence, persistent longer than 4 weeks were absolute indications for surgical intervention. Furthermore the patients showing extensive RISN with protruding pigmented lesion, representing herniation of an inactive tumor through altered sclera, as well as patients with documented increase of RISN dimension during follow up undergone surgical treatment, taking into consideration the patients’ general clinical condition and preferences. Patients with RISN, demonstrating stable course, without compromising the integrity of the eyeball, were managed through observation. RISN was treated using different biological graft materials for patching (e.g., scleral, corneal patches), whereas enucleation of the eye was performed in cases of non-treatable eyewall perforation and irreparable RISN.
Data management
The electronic patient records were reviewed for initial and follow-up data until February 28th, 2021. The variables of the interests collected from the institutional UM database included the
The following
A flat subconjunctival brown pigmented mass at the tumor side on the outer scleral surface at the first clinical examination was regarded as EOE. A presence of persistent disruption of conjunctival integrity at the irradiated side without re-epithelialization for over four weeks was regarded as conjunctival dehiscence and recorded for further analysis.
The variables regarding the
Study endpoints and statistical analysis
The endpoint of the study was the identification of the parameters associated with the indication to RISN treatment, whereat the significant RISN-related characteristics were summarized into a novel RISN
The univariable and multivariable Cox regression analysis was used to assess predictors for RISN treatment. Variables, showing significance in univariable Cox regression analysis were included in multivariable analysis. Continuous variables with the differences in the univariable analysis at a P-value of 0.1 or less were additionally assessed as dichotomous variables using the cutoffs upon the receiver operating characteristic (ROC) curves. We also assessed the linearity of continuous variables and the severity scale by conducting additional analyses, categorizing these variables into quartiles, with subsequent testing of their associations with the study endpoints in Cox regression analysis. The assumption of proportional hazards was verified using SPSS. The included variables fulfilled the assumption of proportional hazards. The diagnostic accuracy of the severity scale and the final prediction model were assessed upon the area under the curve (AUC) in the ROC analysis.
Results
Patient population
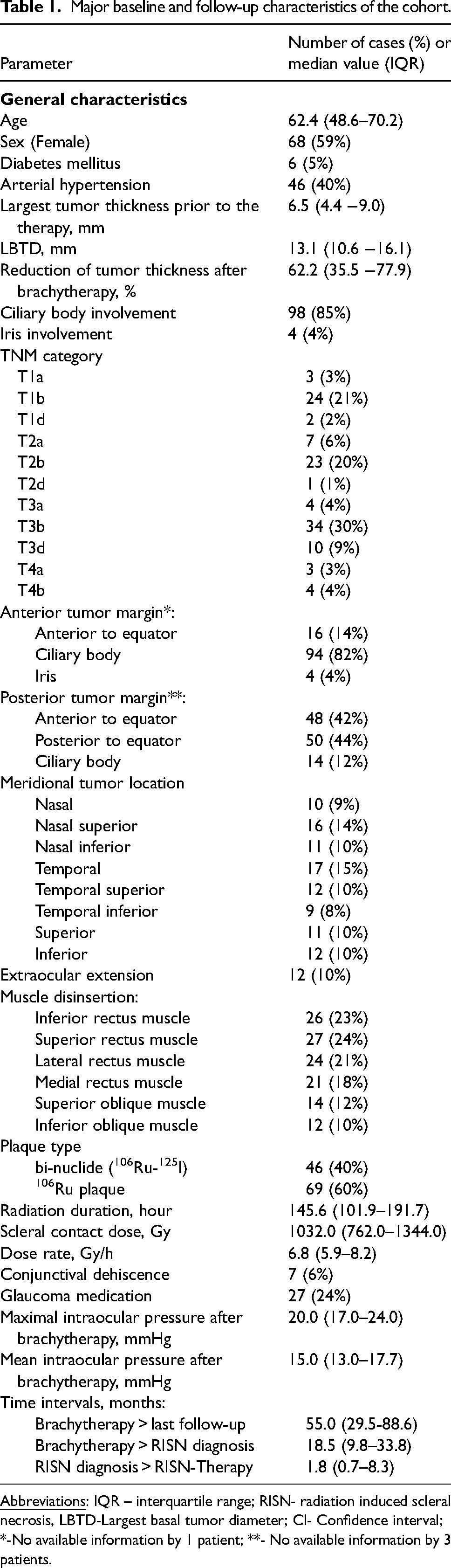
Between 01/1999 and 08/2019 3,960 UM patients underwent brachytherapy, of whom 393 (10%) patients were managed with bi- nuclide plaque and 3,567 (90%) with 106Ru plaques. Overall 115 (3%) patients developed RISN after brachytherapy and therefore were included in this study. The median age of patients was 62.4 years (IQR: 48.6–70.2) and 68 (59%) of them were female. The median post-treatment follow-up was 55.0 months (IQR: 29.5–88.6). RISN was documented at the median time interval of 18.5 months (IQR: 9.8–33.8) after brachytherapy. The detailed information on the characteristics of the analyzed cohort is listed in Table 1.
Major baseline and follow-up characteristics of the cohort.
RISN: characteristics and the clinical course
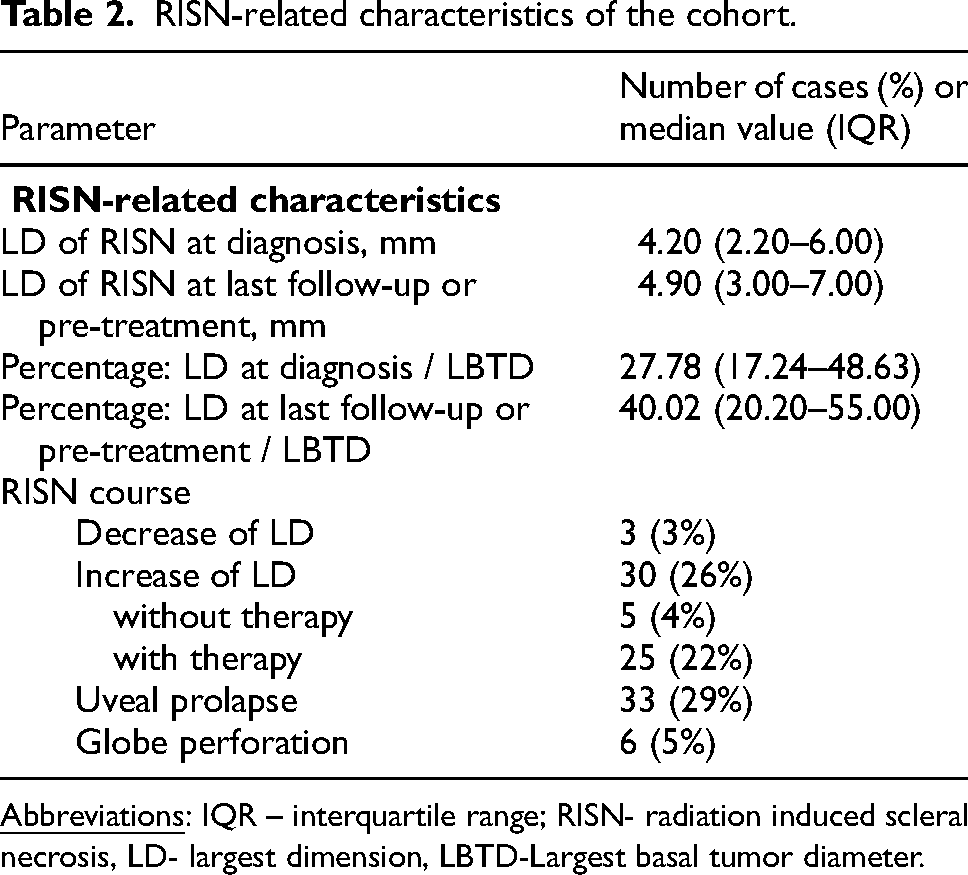
The median LD of RISN was 4.2 mm (IQR: 2.2–6.0) at first diagnosis, and 4.9 mm (IQR: 3.0–7.0) at the last follow-up or pre-treatment, whereat 30 individuals showed an increase and three ones a decrease of the LD of RISN during the observation time (Figure 1). Globe perforation was diagnosed in six cases. The detailed information on the RISN characteristics is listed in Table 2.
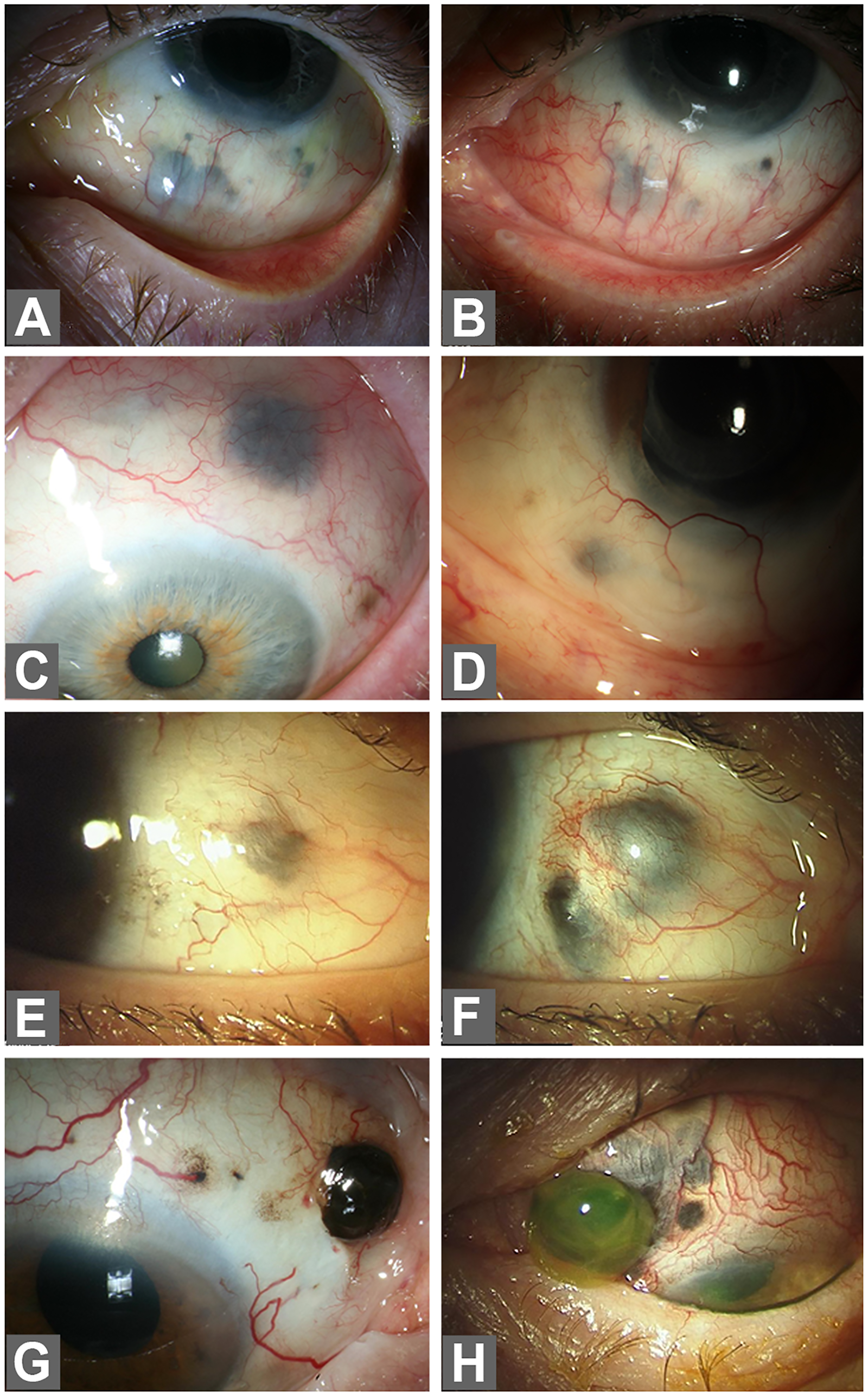
Examples of RISN with different clinical course after brachytherapy for UM: a case with RISN, which developed 36 months after brachytherapy (A) and showed regressive course over 4 years of follow-up (B); two cases (C and D) with RISN Grade I; a case with RISN, which developed 14 months after brachytherapy (E) with progression within 7 months after diagnosis (F); two examples of severe RISN presenting with uveal prolapse (Grade III, G) or globe perforation with extrusion of vitreous body (Grade IV, H). Abbreviations: RISN- radiation induced scleral necrosis.
RISN-related characteristics of the cohort.
The median follow-up after RISN diagnosis in the sub-cohort without RISN treatment (n = 64, 56%) was 27.2 months (IQR: 6.1–50.6). Surgical treatment of RISN was performed in 51 patients (44%) at the time interval between two days and 207.5 months (median: 1.80 months; IQR: 0.7–8.4) after first diagnosis. Of 48 cases with globe sparing surgical intervention on RISN, only 2 treatments were limited to conjunctival revision surgery with conjunctival plastic reconstruction and 46 patients underwent scleral patch grafting (with conjunctival revision). Conjunctival revision surgery with conjunctival plastic reconstruction was performed at median 1.5 months (IQR: 0.6–2.4) after RISN diagnosis. RISN treatment using scleral patch grafting was initiated at median time interval of 1.9 months (IQR: 0.9–8.6). Three patients with full-thickness scleral defect due to RISN and with extrusion of vitreous body underwent enucleation after 1.2 months (IQR: 0.1–9.4).
Moreover, nine other patients in the treated RISN sub-cohort and six individuals in the untreated RISN sub-cohort underwent eye enucleation due to the following reasons: suspected tumor recurrence (n = 10), secondary glaucoma with painful eye (n = 1), persistent retinal detachment with blindness (n = 1), phtisis bulbi (n = 2), a blind eye with progressive severe RISN after scleral patching (n = 1). The histopathologic examination of the enucleated eyes confirmed the presence of scleral necrosis in all cases. Viable tumor cells were detected in 7 cases without the evidence of scleral tumor infiltration. Therefore, patients with treated RISN were at higher risk for secondary enucleation during the whole post-brachytherapy follow-up period (hazard ratio [HR] = 2.19, 95% confidence interval [CI] = 1.14–4.42, p = 0.02) regardless the underlying indication to enucleation. In addition, individuals with treated RISN were at higher risk for distant metastases in the further course of disease compared to individuals without RISN treatment (HR = 2.53, 95% CI = 1.35–4.73, p = 0.002).
RISN severity scale
The following RISN-related characteristics were identified in the univariable Cox regression analysis as predictors for RISN treatment: LD > 5 mm at the last follow-up (p = 0.02), increase of the RISN size (p = 0.002), herniation or protrusion of underlying tissue through the necrotic sclera (p < 0.0001) and globe perforation (p < 0.0001, Table 3).
Univariable cox regression analysis to assess the predictors of RISN treatment.
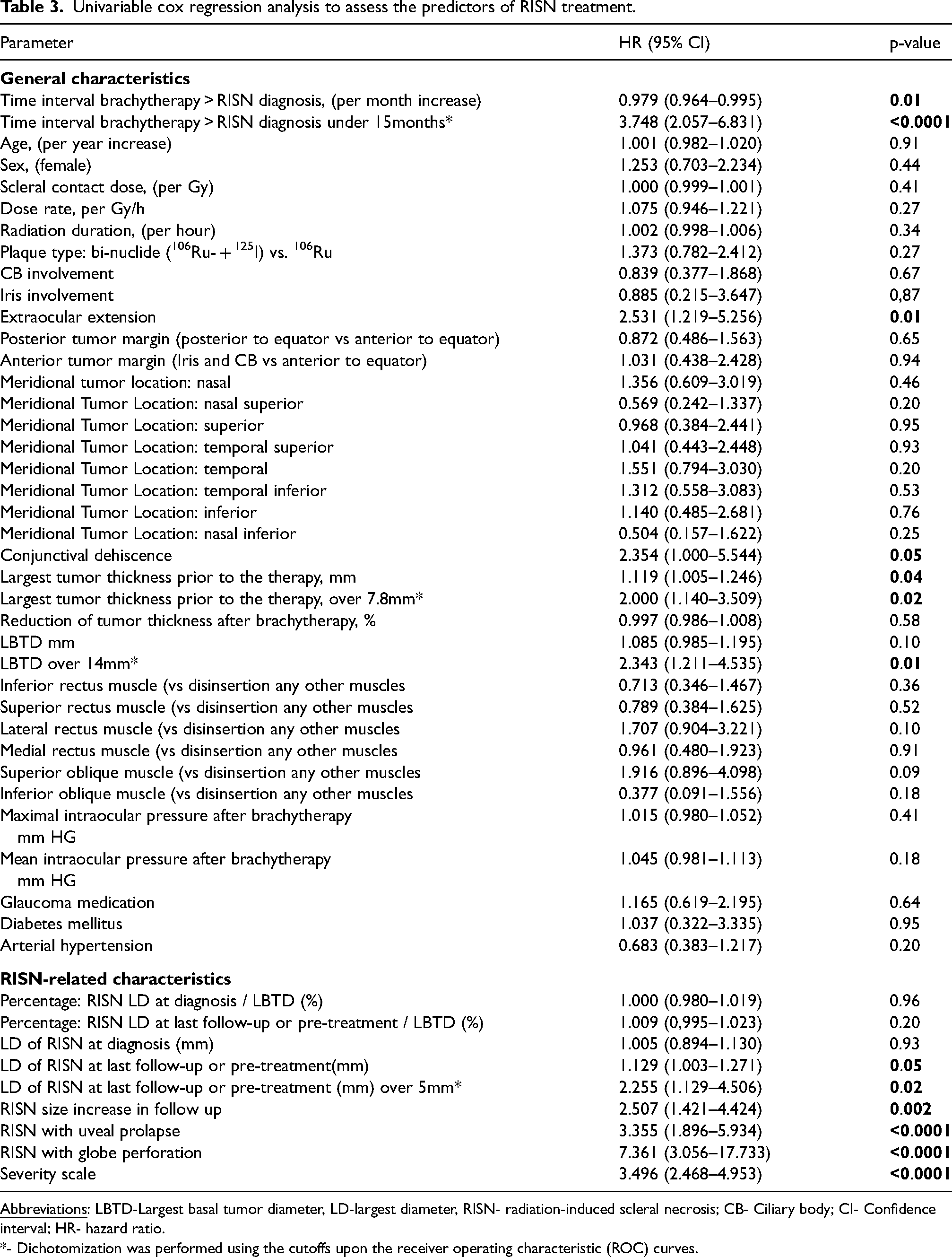
*- Dichotomization was performed using the cutoffs upon the receiver operating characteristic (ROC) curves.
The linearity test of continuous variables and the severity scale is presented in the Supplementary Table E1.
Based on these parameters, we have established a
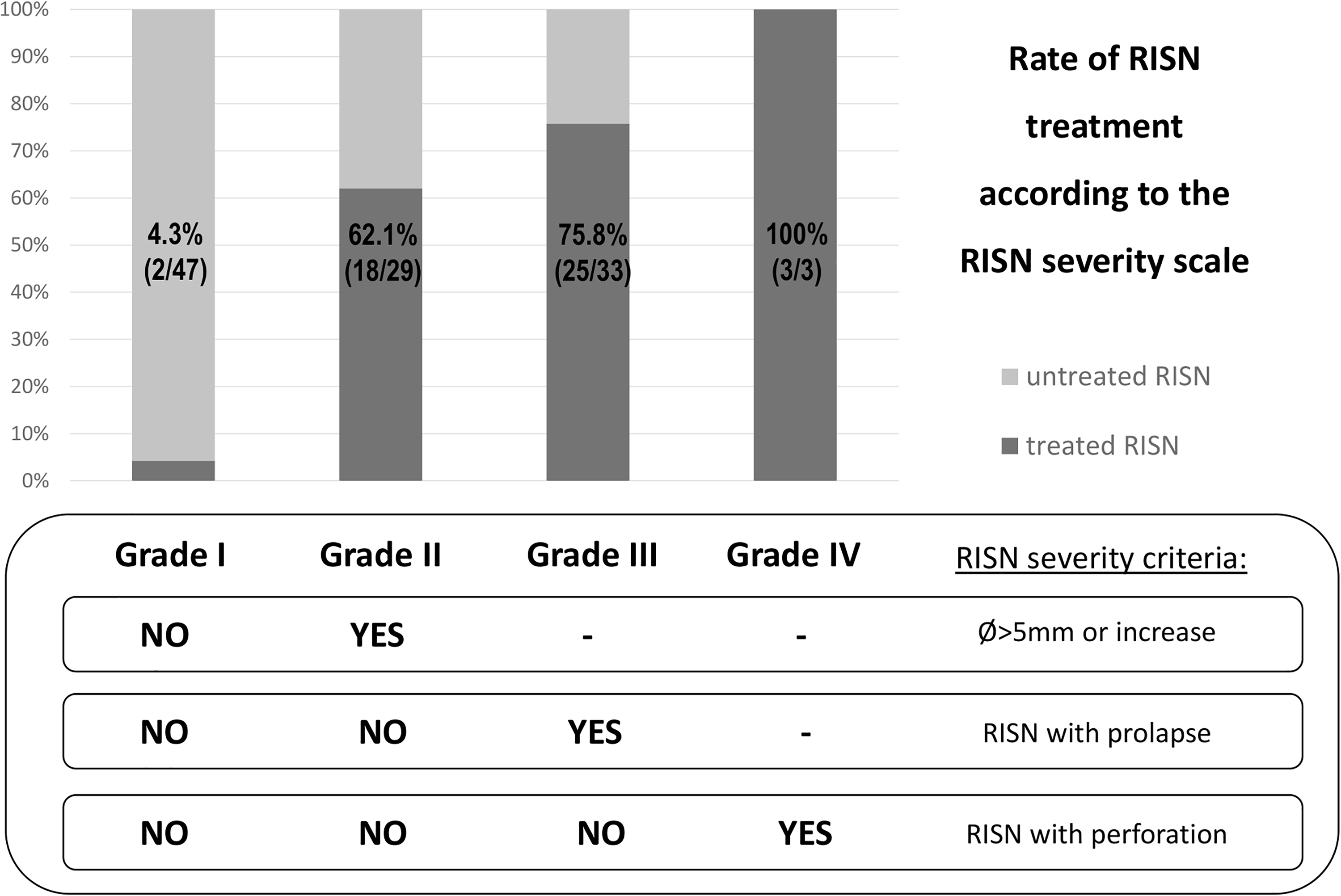
Treatment rates of RISN in each severity grade and a scheme for easy allocation of the RISN to an appropriate severity grade upon the relevant RISN characteristics (LD at the last follow-up, RISN size increase during the follow-up, presence of prolapse and globe perforation). Abbreviations: RISN- radiation induced scleral necrosis; LD- largest dimension.
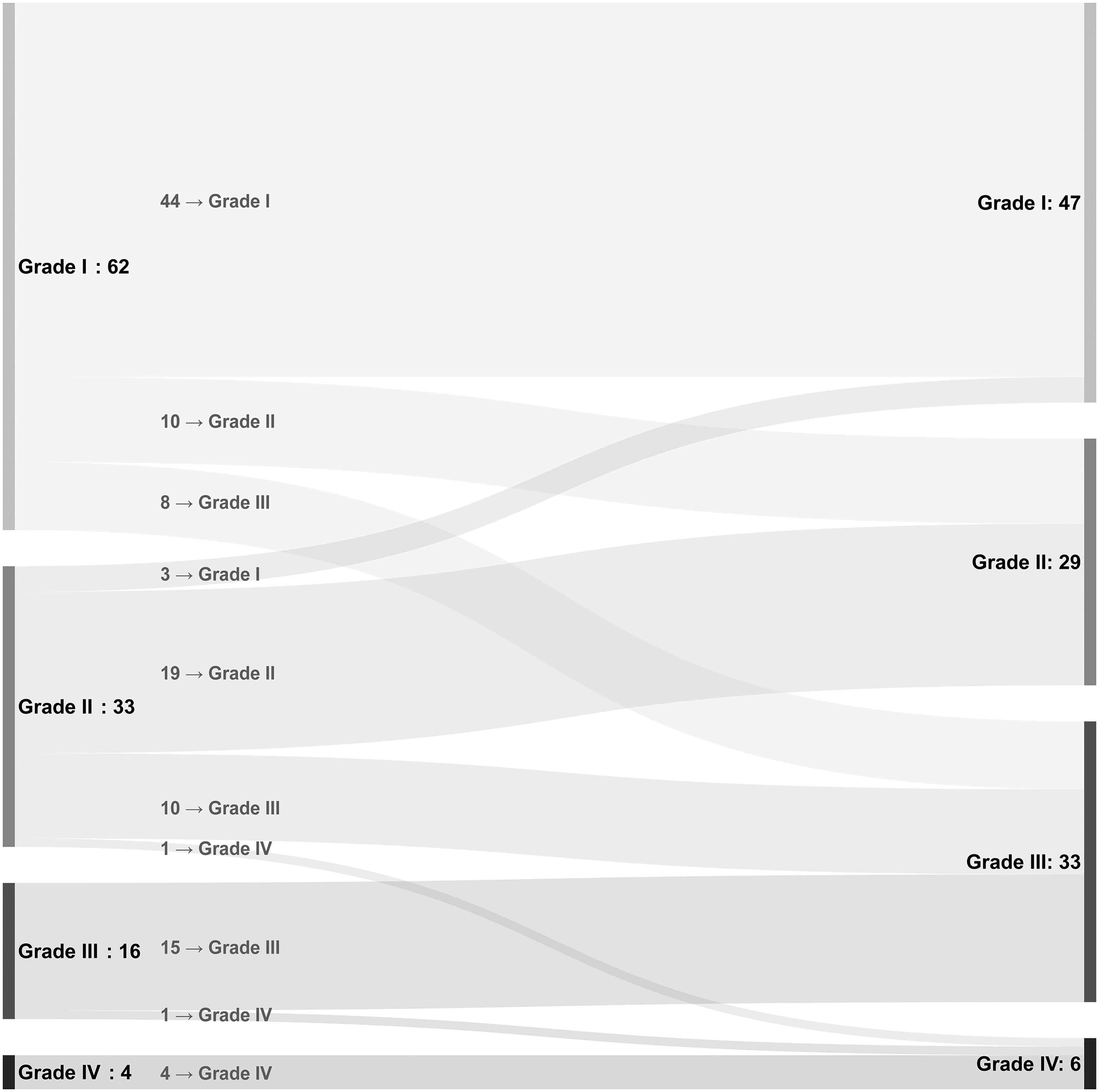
Sankey diagram showing the changes in the RISN severity scale in the analyzed cohort during the whole observational period. Abbreviations: RISN- radiation induced scleral necrosis.
The Cox regression analysis showed strong correlation between the severity scale and RISN treatment (p < 0.0001). In addition, the ROC analysis confirmed sufficient diagnostic accuracy of the severity scale for the prediction of RISN treatment (AUC = 0.869, see supplementary Figure E1). Kaplan-Meier survival plot visualized the differences in the clinical course of RISN depending on the severity grade (see supplementary Figure E2). The higher the grade of RISN severity, the rather and earlier underwent the patients the RISN treatment.
When assessing the extent of RISN treatment as a categorical variable with stepwise increasing treatment invasiveness (conjunctival plastic reconstruction vs. patch grafting vs. enucleation), the RISN severity scale also showed strong correlation with the treatment extent (p < 0.0001, r = 0.712; see also the supplementary table E3 with the frequency of different RISN management options depending on the RISN severity grade, estimated time intervals for RISN treatment (after first diagnosis) in different grade values of the severity scale for RISN in the supplementary table E4 and the complete follow-up times after RISN diagnosis for different grades of the severity scale in the supplementary table E5). Finally, there was a significant association of the RISN severity scale with the risk of enucleation at any timepoint and regardless the indication (p = 0.0284).
Predictive value of patient and tumor characteristics
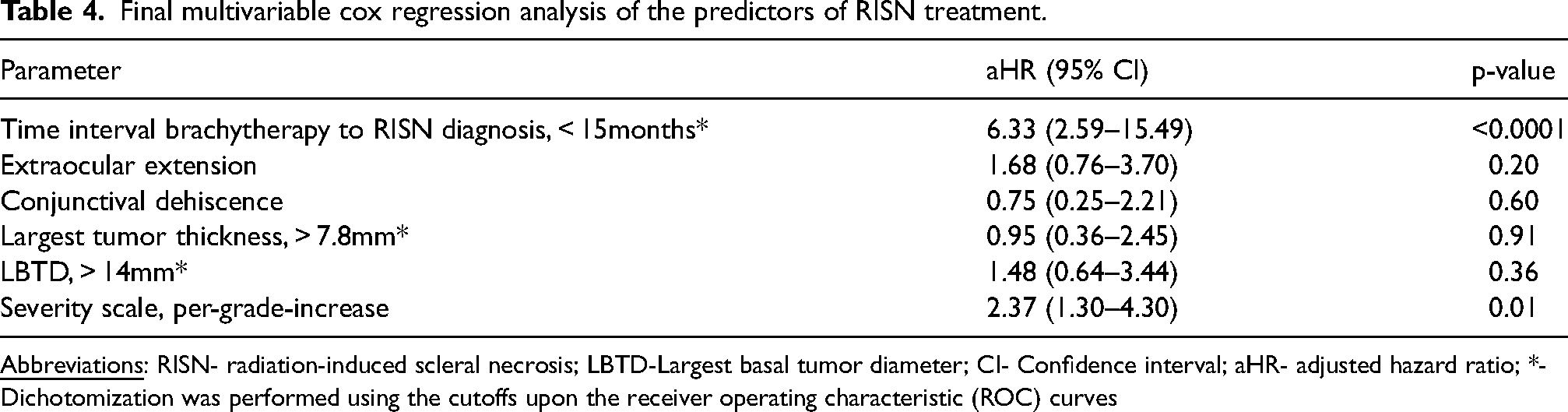
Shorter time interval between brachytherapy and RISN occurrence (<15 months, p < 0.0001), presence of conjunctival dehiscence (p = 0.05) and different tumor features like EOE (p = 0.01), maximal tumor thickness (>7.8 mm, p = 0.02), and LBTD (>14 mm, p = 0.01) were identified as predictors for RISN treatment in the univariable Cox regression analysis (Table 3). In the multivariable Cox regression analysis (Table 4), earlier occurrence of RISN after brachytherapy (<15 months, adjusted HR [aHR] = 6.33, 95% CI = 2.59–15.49, p < 0.0001) and the severity scale (aHR = 2.37 per grade increase, 95% CI = 1.30–4.30, p = 0.01) were confirmed as independent predictors of RISN requiring surgical treatment. The prediction model including both parameters (severity scale and RISN timing) showed a higher diagnostic accuracy (AUC = 0.885) for the prediction of treatment necessity than the severity scale alone (supplementary Figure E1).
Final multivariable cox regression analysis of the predictors of RISN treatment.
Discussion
In this study, we analyzed the course of RISN after brachytherapy for UM. Around half of the patients who developed scleral necrosis after brachytherapy, required surgical treatment of RISN in the further course. We developed a novel classification scale to grade the severity of the radiation induced scleral damage. This severity scale, as well as the subsequent prediction model consisting of the severity scale and time interval between brachytherapy and RISN diagnosis, reliably predicts the indication to RISN treatment.
Classification of RISN severity
Due to a relatively low incidence, the evidence on the clinical course of RISN is sparse. To analyze the late effects of irradiation on the visual system, Gordon et al presented 1995 a classification scheme for radiation induced damage of different ocular structures. 13 However, arbitrary selection of the classification components and the discrimination between the grades based on subjective assessment necessitates the clarification of the diagnostic accuracy and interobserver reliability of this classification. To avoid these limitations, we performed statistical evaluation of the potential scale components prior to their inclusion in the severity scale. We analyzed and confirmed a high diagnostic accuracy of this novel scale. Finally, the components of the presented novel severity scale are based on clearly defined morphologic changes in the sclera with simply measurable parameters allowing a robust allocation of the scleral damage to the appropriate severity grade.
RISN treatment: rate and prognostic factors
There are just few reports about RISN cases requiring treatment. In the series based on the 5057 cases treated with brachytherapy, Kaliki et al. reported 14% (10/73) and 5% (4/73) of RISN patients treated with scleral patch graft and with enucleation respectively. 5 In contrast, 11 of 15 RISN cases (73%) required surgical therapy with scleral patch and/or conjunctival flap in the UM cohort threated with 198Au brachytherapy. 10 In a large institutional series with 301 consecutive patients treated with 125I brachytherapy, 6 (2%) patients were enucleated due to RISN. 14 In our study, about the half of 115 patients underwent surgery due to RISN, whereas the occurrence of RISN in first 15 months after brachytherapy was significantly associated with the therapy indication. This association between the timing of RISN onset and later therapy requirement might be related to the severity of initial scleral damage after brachytherapy. In particular, the more advanced are radiation-induced changes in the sclera, the earlier and prominent is the breakdown of local repair mechanisms. This results in higher probability of earlier onset and rapid progression of RISN necessitating surgical treatment.
The essential role of local repair mechanisms for sclera regeneration has already been discussed with regard to the scleral recovery after diathermy. 15 Generally, sclera is a dynamic tissue with continuous synthesis and degradation of extracellular matrix. 16 Radiation induced scleral alteration can cause an imbalance between these two processes in favor of the degradation. This can cause a progressive scleral necrosis with the protrusion of inactive tumor mass up to full thickness globe perforation. In this context, the possibility of a stable course, or even of a spontaneous partial regression of RISN underlines the importance of the balance between reparative and destructive processes in the sclera after radiation therapy. In particular, we have identified three cases with partially regressive RISN in our cohort. Radin et al had also reported three RISN cases with partial regression in their study. 11 Regressive course could be explained by the prevalence of local repair mechanisms like transformation of fibrocytes into active fibroblasts following any insult to the sclera, which are able to synthesize all of the component molecules of the extracellular scleral matrix. 17
EOE was previously reported as independent predictor for RISN development. 6 In our cohort twelve patients showed a circumscribed EOE at the first diagnosis and in univariable analysis EOE predicted RISN therapy. The EOE was located in all cases anterior the equator and in 75 cases over the ciliary body. Generally diagnosis of EOE can be challenging. So, a subconjunctival pigmentation at the tumor side on the outer scleral surface at the first clinical examination must be differentiated from congenital ocular melanocytosis, which represents an accumulation of melanocytes in the episclera, sclera and uveal tract. In contrast to EOE congenital ocular melanocytosis, manifests with patchy slate-gray sectorial or diffuse scleral pigmentation, some patients may also have associated periocular cutaneous pigmentation (oculodermal melanocytosis). 18 By newly appeared progressive subconjunctival pigmentation after brachytherapy, EOE must be differentiated from RISN. Different findings might help to rule out EOE: clinical appearance of the tumor (inactive tumor with a building of circular scar around it), reduction of tumor thickness in ultrasonography, and verification of scleral thinning in ultrasound biomicroscopy. 6 In rear cases, tumor recurrence and RISN can also coexist. 5
Finally, development of RISN requiring treatment was significantly associated with the risk of enucleation (due to any reasons not limited to RISN) and distant metastases in the later course of disease The fact, that tumor related predictors for RISN treatment, that we have estimated in the univariable Cox regression analysis such as EOE, tumor size (thickness >7.8 mm, largest basal tumor diameter >14 mm) are also well known predictors for distant metastasis 19 could explain the higher risk for metastases by patients with treated RISN . Furthermore, increased tumor thickness is one of the previously reported risk factors for secondary enucleation 9 Of note, the analyzed patient cohort is too small for any causal conclusions and further investigations are needed to explore this correlation.
Limitations
The major limitation of the study is related to the retrospective nature of the presented analysis associated with lower accuracy and incompleteness of the recoded data. The study endpoint, the development of RISN necessitating surgery partially reflects the indications threshold for RISN treatment of the ophthalmologists in our clinic. Another limitation of our study is that using the same dataset to determine the cut-point and to build the Cox model exaggerates the level of statistical association. Therefore, an external validation of the clinical utility of the presented results is mandatory prior to inclusion of the proposed severity scale in the clinical routine.
Conclusion
Depending on the course of reparative and destructive processes in the sclera after brachytherapy for UM, RISN might require surgical treatment even decades after the first diagnosis. We summarized the clinically relevant characteristics of the damaged sclera into a novel RISN severity scale, which could reliably predict the indication to treatment. Along with the RISN severity scale, the time interval between brachytherapy and RISN diagnosis independently predicted the RISN treatment. After successful external validation, the presented RISN severity scale might become a useful tool in clinical management of individuals with RISN after brachytherapy for UM.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721241257979 - Supplemental material for Prognostic factors for surgical treatment of radiation-induced scleral necrosis after brachytherapy for uveal melanoma
Supplemental material, sj-docx-1-ejo-10.1177_11206721241257979 for Prognostic factors for surgical treatment of radiation-induced scleral necrosis after brachytherapy for uveal melanoma by Leyla Jabbarli, Eva Biewald, Maja Guberina, Philipp Rating, Miltiadis Fiorentzis, Dirk Flühs, Claudia H. D. Le Guin, Ekaterina Sokolenko, Wolfgang Sauerwein, Norbert Bornfeld, Martin Stuschke and Nikolaos E. Bechrakis in European Journal of Ophthalmology
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.