
Abstract
Purpose
To establish new criteria for the progression of keratoconus, taking into account a Pentacam HR (high resolution) tomographeŕs repeatability limit.
Methods
This is a retrospective observational study, including 224 eyes in 154 patients diagnosed with keratoconus and patients treated with crosslinking, with a follow-up of at least one year, in which the new progression score of the Cruces University Hospital for keratoconus progression was analyzed. This score takes into account: maximum keratometry, thinnest corneal thickness, maximum posterior elevation, vertical coma and RMS of high order aberrations, all based on the tomographer repeatability limit. The effectiveness or not of crosslinking was determined.
Results
The Receiver Operating Characteristics (ROC) curves obtained in our validation met the criteria by being far from the reference diagonal. Moreover, young patients are more likely to have keratoconus that progresses, and the percentage of patients that showed progression was 14.3% of the eyes studied, with the most advanced keratoconus showing the least progression. Taking into account the new progression score of the Cruces Hospital, we would have indicated crosslinking in 2 eyes only and we observed that none progressed one year after treatment.
Conclusions
The the new progression score of the Cruces University Hospital is a method based on the real repeatability limit for keratoconic eyes. Moreover, it is easy to interpret and can be implemented with Pentacam software. It provides a numerical value that evaluates both the anterior and posterior surfaces of the cornea and corneal aberrations in the evolution of keratoconus.
Keywords
In the monitoring and treatment of keratoconus, establishing the progression or not of keratoconus is essential for deciding on the therapeutic route to follow. Traditionally, topographic indicators of progression are based on the increase in keratometry1–7 and/or decrease in corneal thickness over time.4,5,7 The cut-off values that determine the existence or not of progression according to these parameters vary from author to author. The general opinion is an increase of 1 diopter in maximum keratometry (Kmax) in 1 year and/or a decrease in thinnest corneal thickness of between 10–20 µm.1,4,5,7,8
In 2015, the Global Consensus on Keratoconus and Ectatic Diseases defined this progression as a change consisting of at least two of the following parameters: progressive increase in anterior surface curvature, progressive increase in posterior surface curvature, and decrease in corneal thickness. However, they do not determine the magnitude that defines the progression. 9
To determine these parameters, corneal tomography is one of the essential tools. It is necessary to ensure that corneal tomographers are sufficiently accurate and reproducible, providing repeatable and reliable measurements in corneas with corneal ectasias, in order to be able to compare the parameters over time.10–15
There are studies that propose different criteria to establish the existence of keratoconus progression, but none of them take into account the repeatability limit of various tomographers in corneas with keratoconus.16–18 Based on the repeatability limit obtained in the multicenter study carried out by our group, 15 we have proposed a series of objective parameters and values which we can use to establish that there is keratoconus progression on the new progression score of the Cruces University Hospital (HUC progression score) for keratoconus.
The purpose of this study is to validate the HUC progression score (Table 1). Our hypothesis is that this score is more accurate, since it is based on the repeatability limit of the device used for the measurements and takes into account the parameters that the Global Consensus on Keratoconus and Ectatic Diseases recommend should be analyzed for the definition of progression: elevation of the anterior corneal surface, abnormal posterior ectasia and an abnormal distribution of corneal thickness.
The HUC progression score for keratoconus.
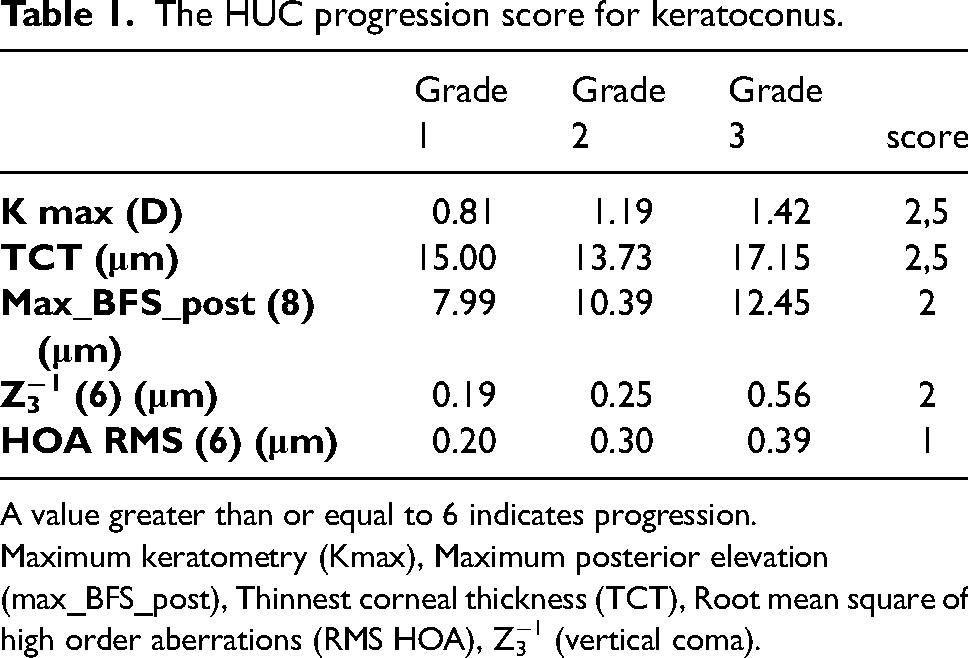
A value greater than or equal to 6 indicates progression.
Maximum keratometry (Kmax), Maximum posterior elevation (max_BFS_post), Thinnest corneal thickness (TCT), Root mean square of high order aberrations (RMS HOA), Z3−1 (vertical coma).
Taking into account the HUC progression score, we determined: 1) most frequent age of progression of keratoconus; 2) if there are differences in progression based on sex; 3) how many eyes with keratoconus progress in our area; 4) if the Cross-Linking (CxL) treatment was effective.
Material and methods
This was a retrospective observational study, which included patients from June 2010 to January 2020, complying with the standards of Good Clinical Practice and following the principles of the Helsinki Declaration. The study was approved by the Ethics Committee for Clinical Research and is registered with the Spanish Ethics Committee for Clinical Research (CEIC) under the code E21/06.
The study included patients who attended the ocular surface unit within the Ophthalmology Department of the Cruces University Hospital in Bizkaia with a diagnosis of keratoconus and follow-up of at least one year. For the analysis of keratoconus progression, those patients with keratoconus were separated from those who had undergone some type of corneal surgery. Likewise, patients undergoing CxL were analyzed, when evidence of progression could be determined with at least one year of follow-up. One year after CxL treatment, patients were evaluated to see the effectiveness of the treatment (Figure 1).
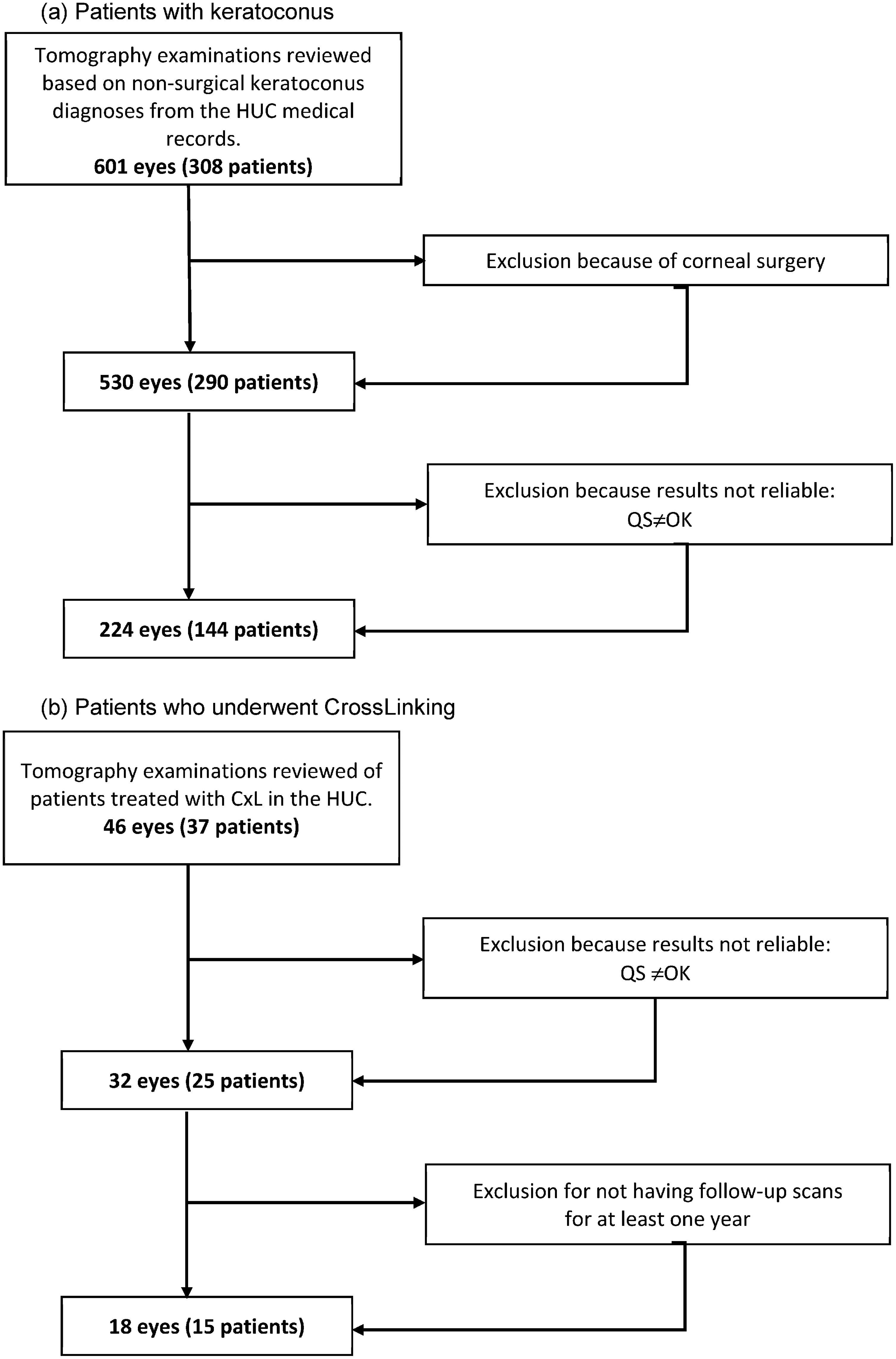
Patient inclusion diagram. (a) Patients with keratoconus. (b) Patients who underwent CrossLinking.
The tomography examinations were carried out using the Pentacam HR (high-resolution) scanner (Oculus; Optikgeräte GmbH, Wetzlar, Germany). For the tomography images to be included in the study, correct test reliability had to be obtained, i.e., to get “OK” in the verification of the test offered by the Pentacam HR.
When analyzing keratoconus by stages, they were classified into 3 groups (Grade 1, 2 and 3), taking into account the maximum posterior elevation (max_BFS_post), establishing the keratoconus with a value of max_BFS_post up to 40 μm max_BFS_post within Grade 1, Grade 2 from 41 to 75 μm max_BFS_post and Grade 3 if it is greater than 75 μm max_BFS_post.
To establish the validation of the HUC progression score (Table 1), as the gold standard we set the increase in the maximum keratometry value (Kmax) by more than one diopter and the decrease of 20 µm at the thinnest corneal thickness (TCT). In both cases, the first tomography performed on the patient (baseline tomography) was compared with the last tomography performed, with at least one year's difference between both measurements. In addition, we calculated the Receiver Operating Characteristics (ROC) with the Kmax and TCT values that were established in the traditional way, 1D and 20μm respectively. We determined the ROC by assigning Kmax and TCT the values that we had set as the repeatability limit of the Pentacam for the different degrees of keratoconus in our previous studies.
To determine whether the CxL treatment was effective, we assessed whether or not there was progression according to the HUC progression score when indicating treatment with CxL and whether or not after the one-year treatment, they progressed or not according to these same criteria.
Statistic analysis
The quantitative variables that followed a normal distribution were summarized by their mean and standard deviation, or the median and the first and third quartiles were used. The qualitative variables were represented by frequency tables, indicating the absolute and relative frequency of each of their categories. In the groups determined by the diagnostic criteria, the age and sex of the patients were compared using the t-test or the Mann-Whitney U test for quantitative variables, whether their distribution was normal or not. For qualitative variables, the tests used were the chi-square test or Fisher's exact test. To evaluate the effectiveness of the treatment, McNemar's test was used.
To determine the quality of the HUC progression score as a diagnostic criterion, the area under the ROC curve was calculated.
Statistical analyzes were performed with the statistical software R (version 4.0.1) 19 and the differences were considered statistically significant when p value <0.05.
Results
To validate the HUC progression score, 224 eyes of 144 patients with keratoconus were evaluated, 70.5% of whom were men and 29.5% women; 86 eyes Grade 1, 97 eyes Grade 2 and 41 eyes Grade 3. The mean age was 30.1 ± 10.3 years and 47.8% of right eyes and 52.2% of left eyes were analyzed.
In Figures 2 the Receiver Operating Characteristics (ROC) are shown, and all the values of the area under the curve (AUC) are greater than 0.600.
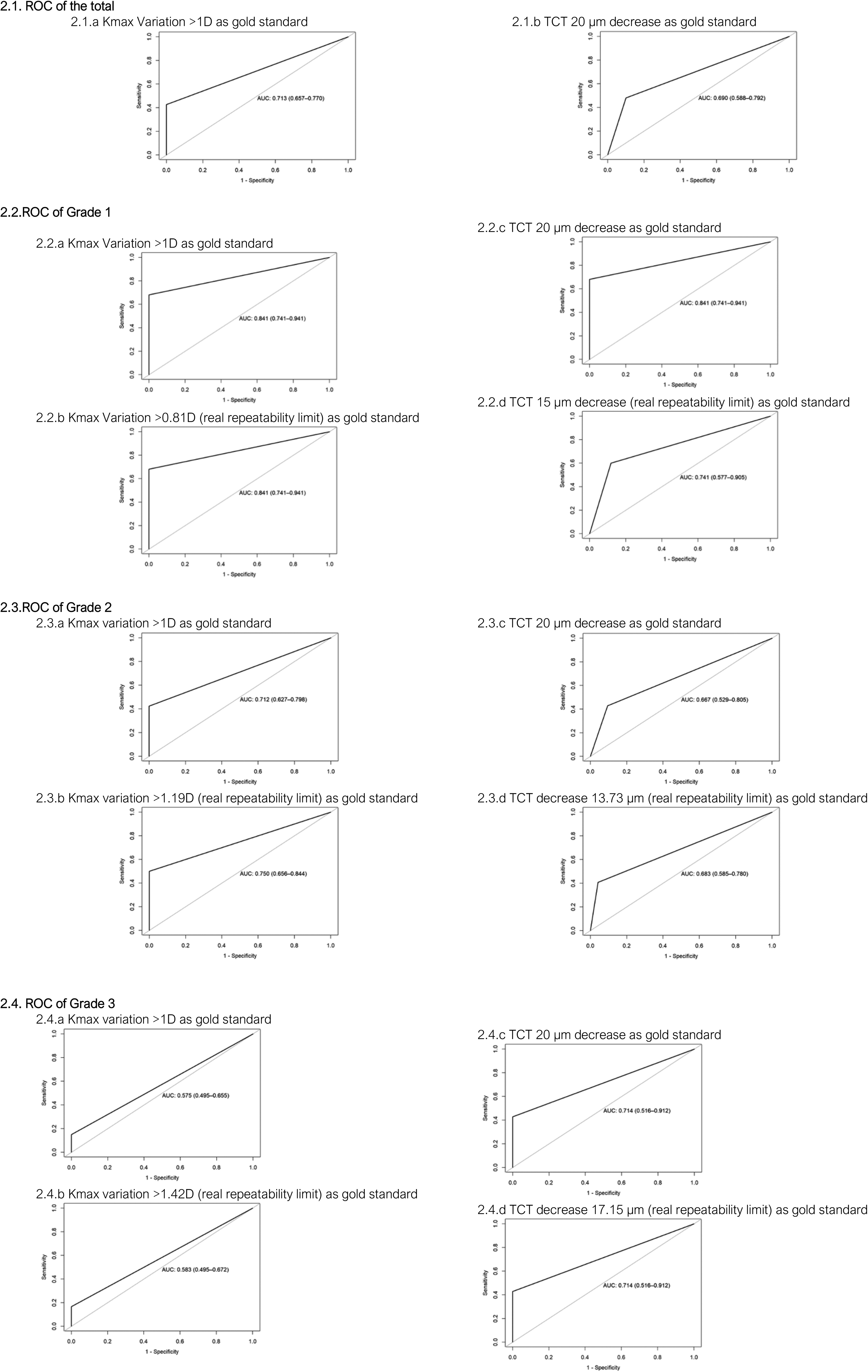
Receiver operating characteristic (ROC).
The younger the patient, the greater the probability that keratoconus will progress to all stages of keratoconus. However, sex does not correlate with greater progression (Table 2). The percentage of patients who showed progression was 14.3% of the eyes studied, which was 17.4% in Grade 1, 14.3% in Grade 2 and 7.5% in more advanced keratoconus (Grade 3).
Progression of keratoconus depending on age and sex.
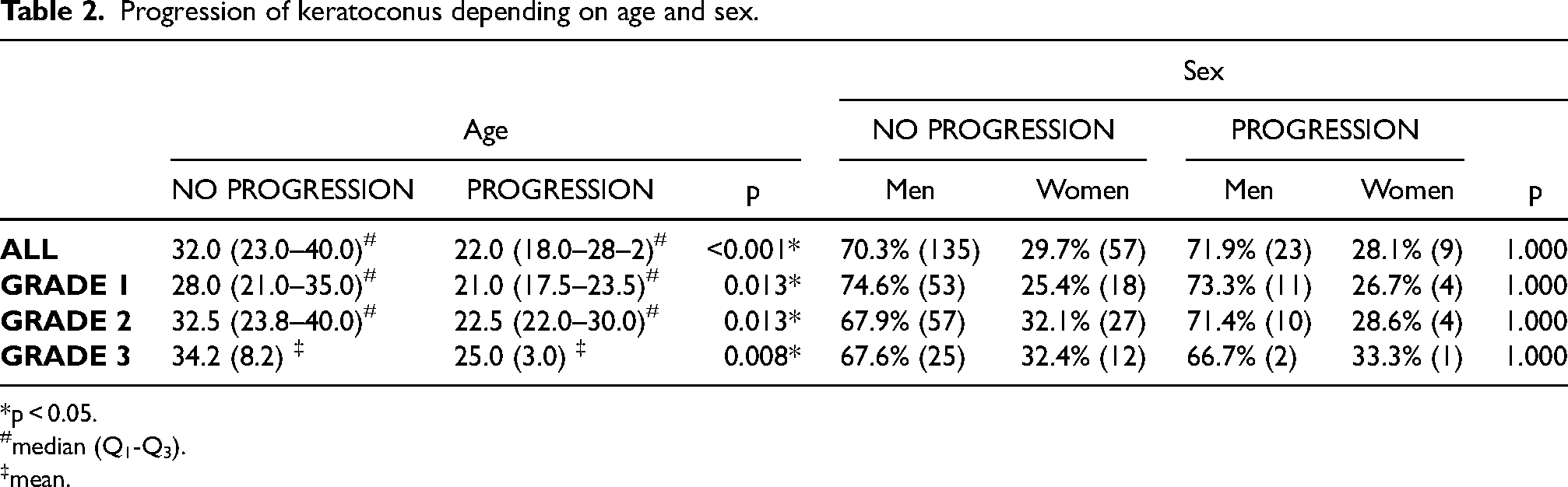
p < 0.05.
median (Q1-Q3).
mean.
To evaluate the effectiveness of CxL treatment, 18 eyes of 15 patients were analyzed. Referral for treatment with CxL began in our hospital in December 2014, and based on the traditional criterion of 1D increase in Kmax, we would have treated only 4 eyes and after treatment it was seen that none of the eyes progressed. If we use the HUC progression score, 2 eyes would have met the criteria to be treated with CxL and one year after treatment, none of the 18 eyes showed progression (Table 3).
Effectiveness of treatment with crossLinking.

Number of eyes that progress or not according to the different criteria.
Discussion
The definition and determination of whether a keratoconus progresses or not has been the subject of many studies in recent years, as it is essential for determining the therapy to be carried out in these patients and for avoiding overtreatment.
The parameter traditionally most widely used to establish the progression of keratoconus in the past has been Kmax.1–7 Various authors have established criteria for the progression of keratoconus, analyzing further parameters. Martínez-Abad et al. 20 define a new progression index, PI%, based on: sphere, spherical-like and coma-like root mean square, central mean keratometry, corneal asphericity and central astigmatism. They have established that patients requiring surgical treatment have a high PI%. Shajari et al. 21 maintain that for the definition of keratoconus progression various corneal changes must be taken into account. They suggest that, with the Pentacam tomograph, the D-index which best determines the progression is defined by: the deviation of the elevation difference of the anterior surface, the deviation of the elevation difference of the posterior surface, the deviation of the pachymetric progression, the deviation of the thinnest point and the deviation from the relational thickness-maximum ARTMax/ Ambrósio. Wisse et al. 17 propose the DUCK score, where in addition to Kmax they assess other parameters: age, quality of vision, variation in distance visual acuity without correction, and variation in the spherical equivalent. Vinciguerra et al. 16 compare the Kmax with the ABCD Progression Display of the Pentacam. They suggest a moderate correlation between the change in the Kmax and the changes in the A and B values in the progression of keratoconus, detecting keratoconus progression in more than half of the cases using the ABCD progression display than what was detected with changes in the standard Kmax.
However, these different criteria proposed to date do not take into account any error by the topographer or tomographer when measuring ectatic corneas. The purpose of proposing a new criterion for the evaluation of keratoconus progression, the HUC progression score (Table 1), is to use tomographic parameters which include the main criteria proposed by the Global Consensus on Keratoconus and Ectatic Diseases, 9 and which are based on the real repeatability limit of the tomograph used,14,15 in our case with the Pentacam. To validate this, we have taken the variation of Kmax and TCT as gold standard, obtaining AUC in all cases that are higher than the non-discrimination line of the ROC curve. As a reference, in every ROC curve graph a line called the reference diagonal or non-discrimination line is drawn from point 0.0 to point 1.0. Thus, for a test to have discriminative capacity, all its cut-off points have to produce a ROC curve away from this reference diagonal line. 22 All the ROC curves obtained in our validation comply with being far from the reference diagonal, and therefore we can consider the HUC progression score acceptable as a system that can be standardized for identifying the progression or not of keratoconus. In the HUC progression score, in addition to Kmax and TCT, we include the variation of the posterior surface and corneal aberrations which have been considered characteristics of keratoconus in various studies.23–25 Another factor that supports the use of the HUC progression score, based on the real repeatability limit, is the conclusion reached by Gustafsson et al. 26 in their study, which stated that Kmax offers great variability, especially in moderate and advanced keratoconus. Unlike other authors who include parameters such as refraction and visual acuity,16,17 we have proposed criteria based on more objective measurements. Refraction in glasses for patients with keratoconus is not usually exact and is highly variable, especially in Grades 2 and 3. 27 In addition, visual acuity is a parameter that can vary greatly depending on the optical aid (glasses, soft contact lenses, gas-permeable corneal contact lenses or scleral lenses) and whether it is up to date; in other words, it is essential to assess the best visual acuity. In Grade 2 and 3 keratoconus, the multifocality of the cornea means that spontaneous visual acuity or acuity with glasses is not assessable.
Moreover, as in other published studies, 28 we concluded in our study that younger patients have a higher risk of keratoconus progression. However, we cannot establish differences in progression between men and women. Regarding the stage of keratoconus that progresses the most, our results suggest that the mildest keratoconus is most likely to progress. This contrasts with other studies which conclude that the greater the severity of keratoconus, the greater the probability of progression.18,28,29 This may be due to analyzing tomographies with good reliability, with “OK” in the Pentacam. When this reliability parameter is not taken into account, the variability of the measurements provided by the tomograph increases so that the determination of the progression may be falsified.
Moreover, when we analyze the effectiveness of treatment with CxL, we observe that there is overtreatment. In the clinical practice in our hospital, the indication for CxL is not always based on measurable objective criteria, and thus in the patients who have undergone CxL we see that many of them did not meet the progression criteria before treatment since they were included for CxL treatment due to the fact that they were very young patients, i.e., under 20 years old. After treatment, it was determined that, taking into account the Kmax and the HUC progression score, none progressed and taking into account the traditional progression criteria, we had treated more patients than necessary.
The limitations of the HUC progression score are that it has been set for a specific scanner, the Pentacam. Further studies with different tomographs would be necessary to try to unify criteria with all tomographs used in the diagnosis and follow-up for keratoconus.
In conclusion, we propose a new criterion for the progression of keratoconus, the HUC progression score. It is a more accurate method than those that currently exist and that can be implemented in Pentacam software, providing a numerical value that evaluates both the anterior and posterior surfaces of the cornea and corneal aberrations in the evolution of keratoconus, making it an easy method to interpret.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.