
Abstract
Purpose
This study investigates the relationship between pupil size during biometry examinations and the chord mu value in candidates for cataract surgery.
Methods
Retrospective analysis of ocular biometry measurements was performed on consecutive cataract surgery candidates above 50 years of age, examined between 2018 and 2020 at a single tertiary referral center. Statistical analysis assessed the association between pupil size and the chord mu value. The population was categorized into groups based on pupil size, and an analysis was conducted on the barycenter positions of the iris and pupil center for each group.
Results
The analysis included 2877 patients. A weak positive correlation was observed between the chord mu value and pupil size using Pearson's test (r = 0.160, p < 0.01). Group stratification by pupil size indicated temporal and inferior shifts in pupil center barycenter as pupil size increased, reflecting asymmetrical pupil dilation during mydriasis. A moderate positive correlation between the chord mu value and chord alpha value was identified (Pearson's test, r = 0.641, p < 0.01). As expected, no correlation was found between chord alpha value and pupil size.
Conclusions
Chord mu values were higher in patients with mydriatic pupils, likely due to asymmetric pupil dilation and center displacement. Evaluating chord mu values requires considering pupil status and conducting biometry under standardized lighting to prevent misinterpretation caused by pharmacological dilation. This caution is crucial to avoid erroneously excluding eligible patients from multifocal IOL implants. Alternatively, the chord alpha value could serve as a more appropriate alternative in such scenarios.
Keywords
Introduction
Angle kappa is an important optical angle that is defined as the angle between the visual and pupillary axes. 1 This angle can be approximated by biometers by measuring the displacement between the corneal light reflex and the pupil center (referred to as the apparent chord mu). 1 In recent years, chord mu has gained renewed interest due to its potential role in determining the suitability of patients for multifocal intraocular lens (MFIOL) implantation. High chord mu values have been associated with reduced visual quality 2 and photic phenomena such as haloes and glare following refractive 3 and diffractive 4 MFIOL implantation.
Angle alpha represents the angle between the visual axis and the optical axis, 1 while chord alpha is the displacement between the corneal light reflex and the limbus center. 5 Higher values of chord alpha have also been linked to lower optical quality after MFIOL implantation 6 and is considered to be more reliable and stable value than chord mu after cataract surgery. 7
Another important distinction between chord mu and chord alpha is that chord mu is closely related to the pupil by definition, whereas chord alpha is related to the limbus. The pupil size is determined by the iris, which is a highly dynamic tissue that is impacted by environmental conditions. Chang and Warring warned that the pupil center could shift during miosis compared to mydriasis, and that the chord mu value should ideally take into account the state of the pupil. 1 In practice, biometric measurements are often taken regardless of the pupil state, and in some cases, pharmacologic dilation is performed before the biometry exam. This practice is based on several studies that have reported that pharmacological cycloplegia and dilation do not significantly impact biometry results or only affect less important values, such as anterior chamber depth, central corneal thickness, and white-to-white length.8,9
In this study, we investigated the relationship between chord mu and pupil size in a large retrospective cohort of cataract surgery candidates. We analyzed the pupil center position in subgroups defined by pupil size and compared it to the iris center position.
Methods
Patients
The biometry results of cataract surgery candidates over 50 years of age, who had biometry test done at Hadassah Medical Center, a tertiary hospital, between August 2018 and March 2020, were retrospectively reviewed. This study was approved by the institutional ethics committee of the Hadassah Medical Center (study#: HMO-0459-18) and data was coded anonymously. Exclusion criteria included pseudophakic or aphakic eyes, previous refractive surgery or pars plana vitrectomy, suboptimal quality exams resulting in failed measurement of at least one biometric parameter, and incomplete demographic information. In the case of bilateral phakic patients with successful biometry measurements available for both eyes, one eye was chosen randomly.
Biometric measurements
Ocular biometric measurements were performed with swept-source technology using the IOL Master 700 (Carl Zeiss Meditec AG, Jena, Germany). If multiple exams were done on the same day, only the most accurate exam was included in the analysis (determined by the fewest warning alerts by the device algorithm). If several exams were done on different days, only the exam from first visit was included in the analysis.
Biometric parameters included in this study were: axial length (AL), mean keratometry (K), mean astigmatism, anterior chamber depth (ACD), lens thickness (LT), central corneal thickness (CCT), white-to-white length (WTW), pupil size (PS), chord mu length, shift of the corneal vertex toward the pupil center (Px, Py) and toward the iris center (Ix, Iy).
Departmental protocol at Hadassah Medical Center includes is to pharmacologically dilation of patients’ pupils (Tropicamide 0.5% + Phenylephrine 10%) for examination before biometric measurements, therefore, the vast majority of the patients in this study were dilated.
Chord mu and chord alpha
Chord mu and chord alpha represent vectors that are defined by a length and an angle. For the purposes of this study, we focused on the length of these vectors and did not analyze their respective angles.
During the biometric assessment conducted by the IOL Master 700 device, the chord mu is obtained through automatic calculation based on pupil center coordinates. However, chord alpha is not provided as an output by the device. To derive this measurement, we utilized a Pythagorean equation with the Ix and Iy coordinates, as outlined below:
Coordinates calculations
To allow for comparison of the iris center and pupil center with respect to the corneal vertex, we defined the coordinates of the pupil and iris centers as PC(-Ix, -Iy) and IC(-Px, -Py), respectively. Furthermore, to enable comparison between the right and left eyes included in the study, we defined the X-axis direction as nasal in both eyes.
Statistical analysis
The normality of the data was confirmed using the Kolmogorov Smirnov test. Normally distributed continuous variables were presented by mean and standard deviation, and differences among groups were tested by two-sample t-test and one-way ANOVA. Non-normally distributed continuous variables were presented as medians with inter-quartile ranges, and group differences were tested by Mann-Whitney and Kruskal-Wallis tests. Analysis of correlations between chord mu and chord alpha and other biometric parameters was performed using Pearson's coefficient. A univariate and multivariate linear regression models were applied to assess the effect of pupil size and AL on chord mu value, while accounting for potential confounding factors. A statistically significant result was considered as p < 0.05 in a two-sided test, with adjustments made for multiple comparisons using the Bonferroni correction. The analysis was performed using SPSS software (IBM SPSS Statistics, Version 27.0, Chicago. Armonk, NY: IBM Corp).
Results
Patient and eye characteristics
During the study period, a total of 2767 patients aged 50 years and above underwent biometry exams for both eyes. Following exclusions due to suboptimal quality biometry exams (n = 184), lack of demographic information (n = 92), and previous eye surgery (n = 76, including 69 refractive surgeries and 7 vitrectomies), only one eye of each patient was included in the final analysis. In total, 2415 eyes (from 2415 patients) met the inclusion criteria and were included in the study, representing 87% of all eyes. Among the included eyes, 48.8% (n = 1179) were right eyes, and 54.9% (n = 1326) of the patients were female, with a mean age of 72.5 ± 9.1 years.
The biometric characteristics of the eyes included in the study are provided in Table 1. The mean chord mu and chord alpha values were 0.353 ± 0.207 mm and 0.491 ± 0.220 mm, respectively. The mean pupil size was 4.93 ± 2.02 mm. Among the 2415 eyes analyzed, 215 (8.9%) met the criterion for high chord mu according to Holladay's definition (> 0.6 mm), 10 while 98 eyes (4.1%) had a chord mu greater than 0.767 mm, which was defined as the mean plus two standard deviations.
Biometry parameters, chord mu, and chord alpha
The Pearson's correlation test demonstrated a weak positive correlation between chord mu and pupil size (r = 0.160, p < 0.01), a moderate positive correlation between chord mu and chord alpha (r = 0.641, p < 0.01), and weak negative correlations between chord mu and both ACD (r = −0.186, p < 0.01) and AL (r = −0.114, p < 0.01). Furthermore, chord alpha was also weakly negatively correlated with ACD (r = −0.203, p < 0.01) and AL (r = −0.218, p < 0.01), but not significantly correlated with pupil size (r = 0.025, p > 0.05).
Chord mu and chord alpha demonstrated higher values as axial length decreased (Kruskal-Wallis test, p < 0.01; Figure 1). Furthermore, the comparison between highly myopic eyes (AL > 26 mm) and short eyes (AL < 22 mm) demonstrated a significant increase of 43.9% in chord mu (0.31 ± 0.23, 0.45 ± 0.28, respectively; unpaired t-test, p < 0.001) and a significant increase of 49.7% in chord alpha (0.38 ± 0.20, 0.57 ± 0.24, respectively; unpaired t-test, p < 0.001).
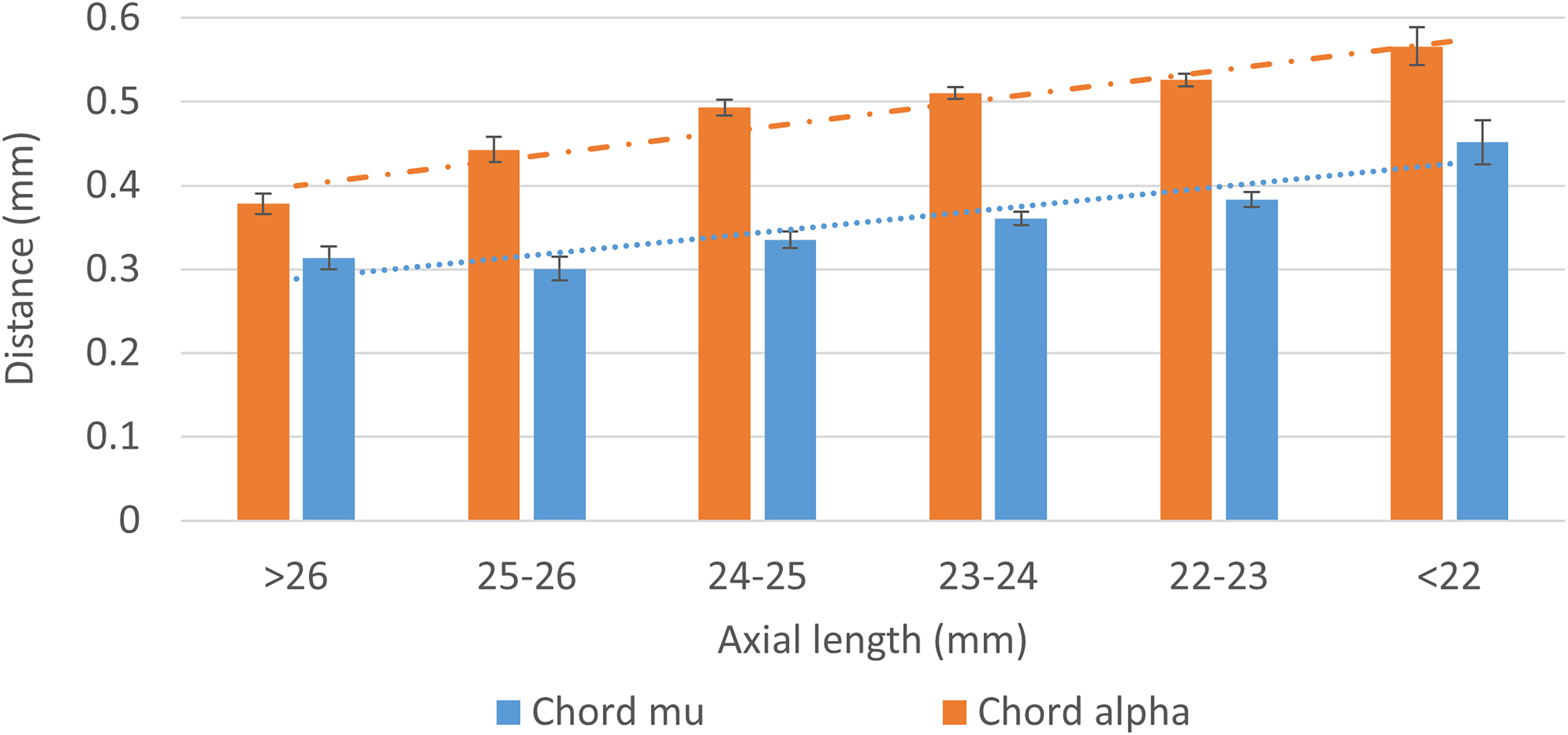
Comparison of chord mu and chord alpha by axial length.
After stratification for subgroups based on pupil size, we observed that the chord mu increased with an increase in pupil size, while the chord alpha remained stable (Kruskall Wallis, p < 0.01; Figure 2). It is worth noting that, unlike the chord mu value, the chord alpha is independent of the pupil state, as per its definition. The maximum amount of the increase in chord mu, as observed in patients with very small pupils (<2.5 mm) and those with extremely large pupils of 7.5–8.5 mm (after eliminating patients with a pupil size above 8.5, which could cause inaccurate pupil detection), is 39% and is of clinical significance (0.28 ± 0.14 and 0.39 ± 0.21, respectively). Table 1 provides the biometric data for each of the pupil size groups.
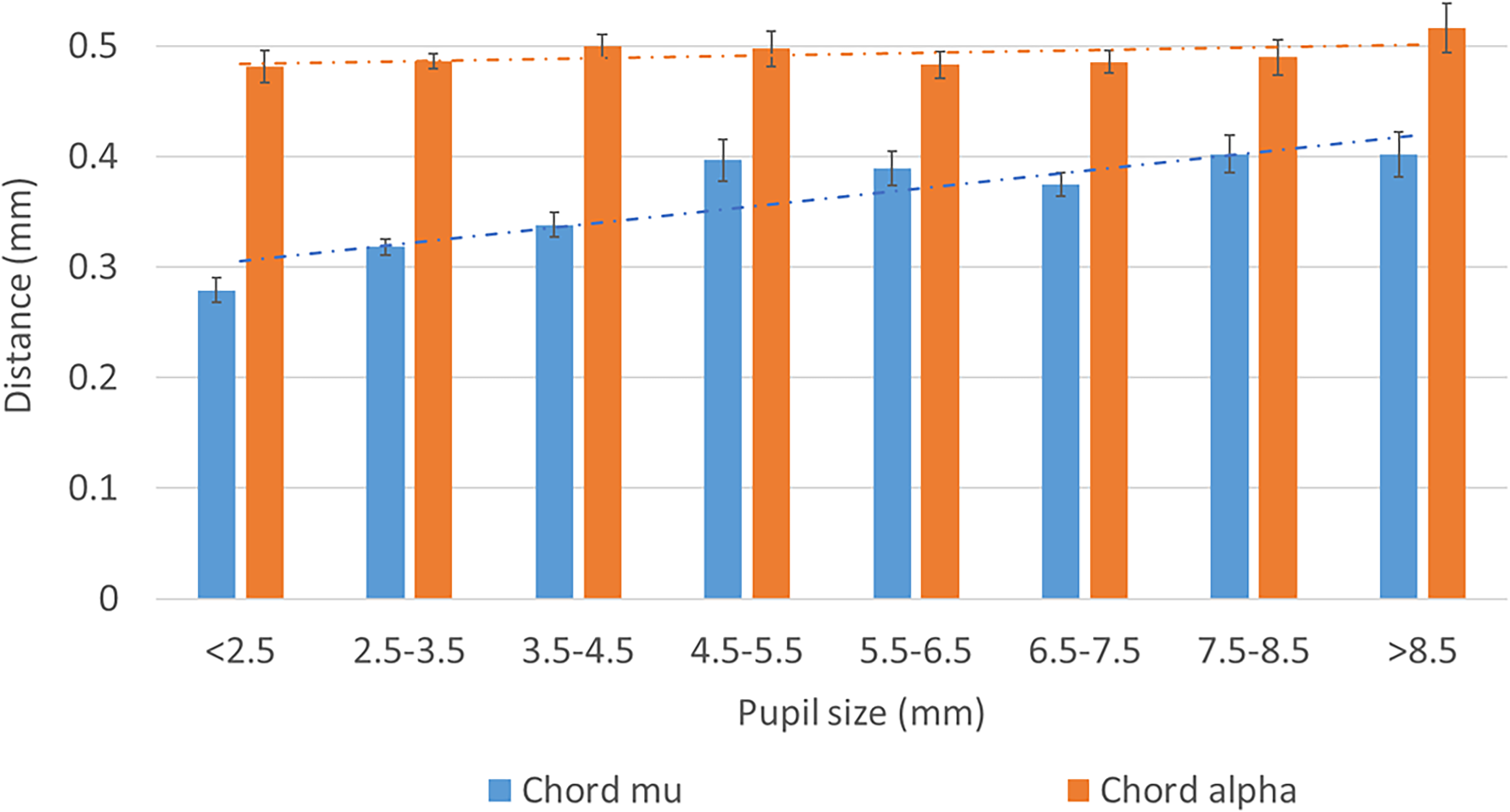
Comparison of chord mu and chord alpha by pupil size.
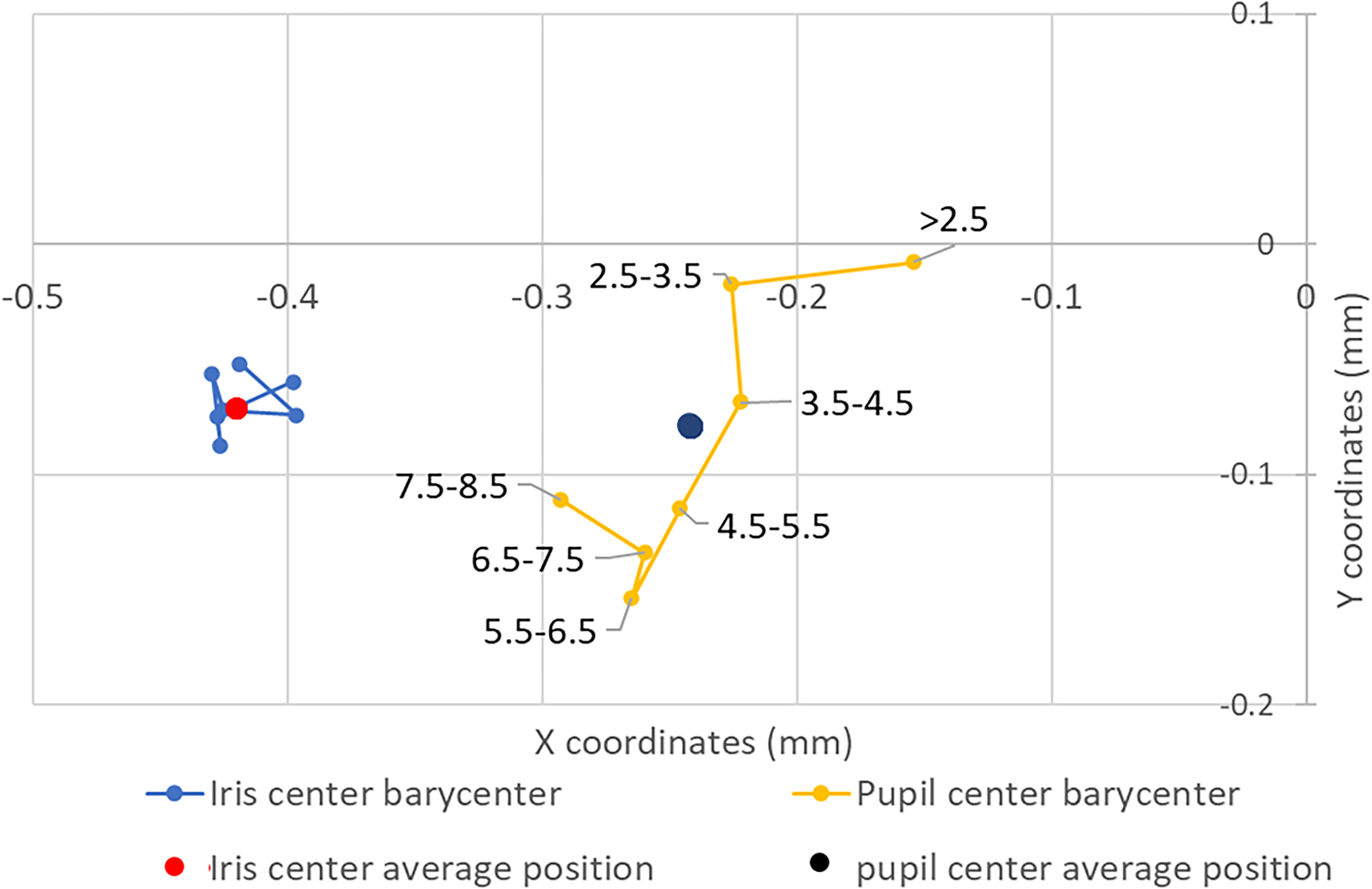
Iris and Pupil barycenters coordinates by pupil size sub-groups.
A linear regression analysis was applied to assess the impact of pupil size and axial length on chord mu value. In a univariate analysis, pupil size has a higher and positive effect on chord mu compared to AL (standardized beta = 0.16, −0.11; P < 0.001, respectively). While applying multivariate analysis and adjusting for possible confounders such as age and gender, the linear regression model still revealed that pupil size has a greater impact on chord mu level than AL (standardized beta = 0.18, −0.11; P < 0.001, respectively).
Pupil center shift with pupil size
An analysis of the mean coordinates of the pupil center and iris center for various pupil size groups was performed. The results indicate that the Px and Py significantly decreased with an increase in pupil size, while the Ix and Iy remained stable (Kruskall Wallis, p < 0.01). As shown in Figure 3, the pupil center barycenters of different groups shifted both temporally and inferiorly with an increase in pupil size, likely reflecting an asymmetric dilation of the pupil during mydriasis.
Discussion
In this retrospective study on a large adult population of cataract surgery candidates, we found that the chord mu varies significantly with the size of the pupil. These results highlight the importance of evaluating the pupil state under standardized lighting conditions, as recommended by Chang and Waring, for accurate interpretation of chord mu during the examination. 1 Recent retrospective studies on cataract candidates analyzing chord mu11,12 did not report the patient's pupil dilation status before biometry examination and did not consider lighting conditions during the examination. Our data suggest that considering pupil size in statistical analyses is crucial to prevent biased conclusions about chord mu values. Our results align with a recent prospective study on 87 eyes, which demonstrated an approximate 0.1 mm increase in chord mu following pharmacological pupillary dilation. 13
Previous studies have suggested that the major biometric parameters remain unaffected by pharmacologic dilation or lighting conditions.8,9,14 As a result, many ophthalmology centers conduct biometry exams after pharmacologic dilation of the pupils or in non-standardized lighting conditions. However, since Holladay defined a high chord mu cutoff value as greater than 0.6 mm and cautioned that high chord mu values could predict halos and glare after multifocal implantation, 10 surgeons have started to take chord mu value into consideration. Therefore, when assessing chord mu in patients prior to multifocal implantation, caution should be exercised, considering the patient's pupil state and environmental conditions during the examination. In fact, pharmacologic dilation and biometry examination under mesopic lighting conditions could result in artificially high chord mu values, leading to the exclusion of suitable candidates for MFIOL implantation.
In the current study, we also analyzed the location of the pupil and iris center (PC and IC) barycenters in different pupil size groups to suggest the cause of the increase in chord mu due to mydriasis. A displacement of the pupil center barycenter temporally and inferiorly relative to the visual axis was shown, while the iris center barycenter remained stable. This shift of the pupil center shift was previously observed in small prospective studies before and after pupil dilation. 9 and likely reflects the small temporal shift of the pupil center during physiologic mydriasis in mesopic conditions and during pharmacologic dilation because of asymmetric pupil dilation15,16 Erdem et al. also found that pupil movement has an inferotemporal direction, 16 as was observed in the current study.
Assessment of chord alpha could be useful in cases where the examination is conducted under dilated or unstandardized conditions. We found that chord mu and chord alpha are moderately related, but unlike chord mu, chord alpha is not affected by the pupil state and could be a good substitute for chord mu, especially when the biometry exam is performed under pharmacologic pupil dilation. High chord alpha is also associated with visual disturbances and dissatisfaction after MFIOL implantation 17 and seems to be more stable before and after cataract extraction than chord mu.7,18
This study had several limitations, primarily due to the retrospective study design. First, it was not possible to differentiate between pharmacologic and physiologic mydriasis due to a lack of documentation regarding light conditions during biometry measurements and the use of mydriatic drops before biometry exams. According to Erdem et al., pupil movement during pharmacologic and physiologic dilation is slightly different and may induce varying changes in chord mu. 16 Second, this study was a large sample size retrospective study that compared different groups of patients based on their pupil size in order to understand the impact of pupil state on chord mu. However, only a wide prospective study that compares biometry measurements of cataract candidates before and after dilation could demonstrate a real cause-effect link between pupil state and chord mu. Finally, another limitation is that the biometry measurements included in this study were successful biometry exams that had strict criteria for the proper measurement of each biometric parameter. We are aware that this may have caused a selection bias and excluded patients with advanced cataract since the IOL Master 700 has difficulty measuring lens thickness and axial length in such patients.
To conclude, chord mu significantly increases with pupil size. Therefore, it is of great importance to interpret chord mu in accordance with the pupils’ state of the patient and to perform biometric examinations under standardized lighting conditions in order to avoid the artificial exclusion of potentially good candidates for MFIOL implantation. Chord alpha, a value that is independent of pupil state, could be used as an alternative to chord mu measurement in patients who have been pharmacologically dilated prior to biometry.
Comparison of ocular biometric characteristics of different groups by pupil size.
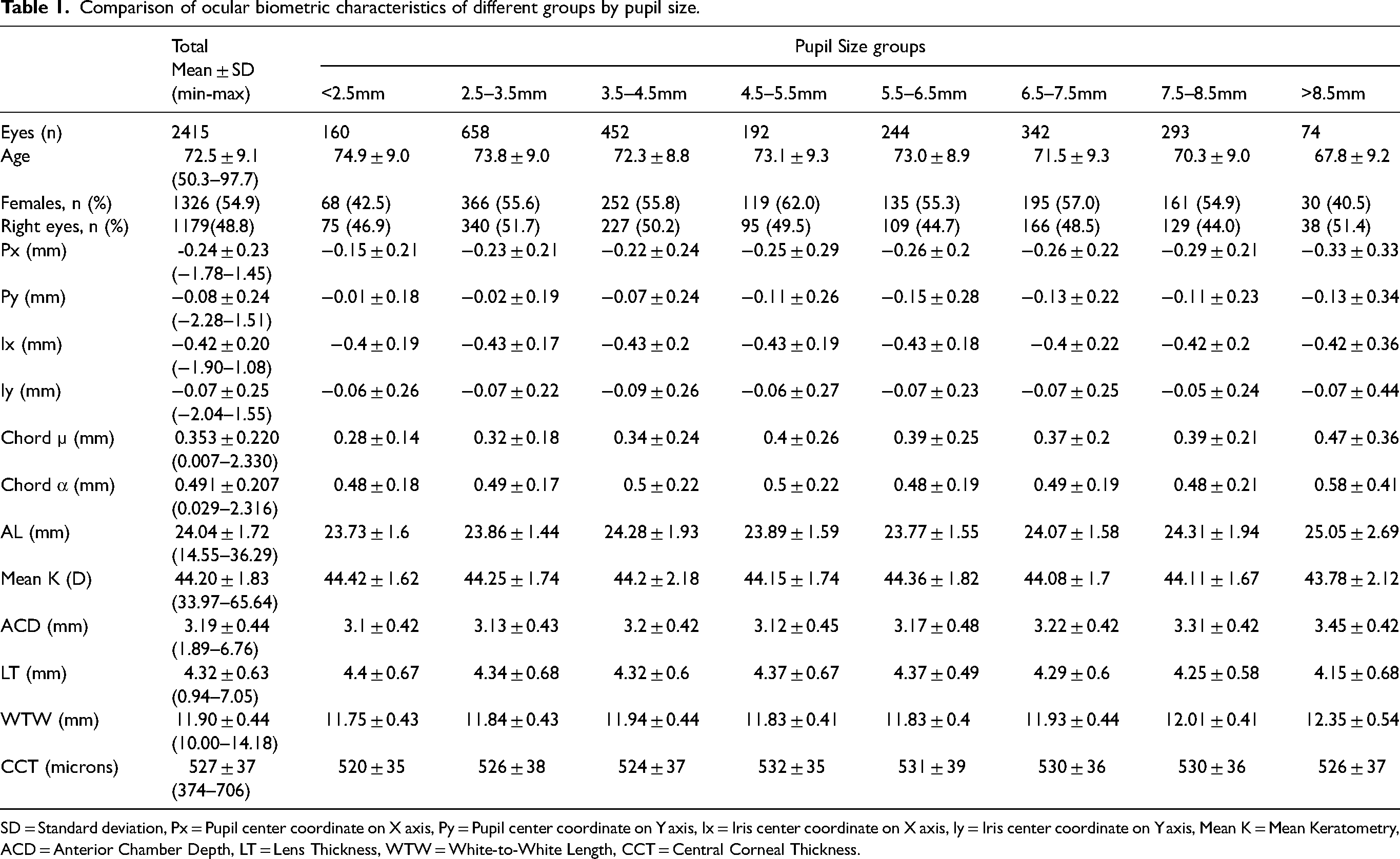
SD = Standard deviation, Px = Pupil center coordinate on X axis, Py = Pupil center coordinate on Y axis, Ix = Iris center coordinate on X axis, Iy = Iris center coordinate on Y axis, Mean K = Mean Keratometry, ACD = Anterior Chamber Depth, LT = Lens Thickness, WTW = White-to-White Length, CCT = Central Corneal Thickness.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.