
Abstract
Purpose
To evaluate the safety and efficacy of the surgery of intracorneal ring segment implantation with 320° of arc (320-ICRS) in patients with advanced keratoconus stage IV and maximum keratometry (Kmax) above 60 D.
Methods
A prospective, interventional case series study evaluating 25 eyes of 19 patients with keratoconus stage IV and Kmax > 60D in which 320-ICRS were implanted using VisuMax® femtosecond. Uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), keratometric values (mean - mean-K, flat - K1, and steep - K2), maximum keratometry (Kmax), tomographic astigmatism, refractive astigmatism and asphericity (Q) were assessed preoperatively and at 3, 6 and 12 months after the procedure.
Results
The UDVA improved from 1.03 ± 0.28 LogMAR (20/200) to 0.54 ± 0.21 LogMAR (20/60), (p < 0.001), the CDVA (with glasses) improved from 0.63 ± 0.29 LogMAR (20/80) to 0.31 ± 0.16 LogMAR (20/40),(p = 0.004), K1 reduced from 54.41 ± 4.46 D to 49.36 ± 4.11 D (p < 0.001), K2 reduced from 61.15 ± 4.37 D to 53.715 ± 4.05 D, (p < 0.001), mean-K reduced from 57.55 ± 4,17 D to 51.44 ± 3,94 D (p < 0.001), Kmax reduced from 69.80 ± 8.20 D to 63.43 ± 6.31 D (p < 0.001) and asphericity (Q) changed from −1.57 ± 0.35 to −0.77 ± 0.56 (p < 0.001). A total of 89.9% patients reached BCVA wearing scleral contact lens 0.2 LogMAR(20/25).
Conclusion
320-ICRS to treat advanced keratoconus appears to be an efficacious and safe procedure, being a surgical alternative to delay or even prevent corneal transplantation.
Keywords
Introduction
Keratoconus is a chronic, progressive, bilateral, non-inflammatory, typically asymmetric corneal condition with progressive curvature, protrusion and thinning of the corneal stroma. 1 The approach to the treatment of keratoconus has greatly evolved in recent decades, and research has been conducted in search of methods to promote stabilization of the condition in order to avoid or delay corneal transplantation. 2
Typically, the treatment for advanced keratoconus is based on deep anterior lamellar keratoplasty or penetrating keratoplasty. However, both options may be associated with eventual intraoperative and postoperative complications, often severe. 3 For this reason, safe therapeutic alternatives have been studied in an attempt to avoid or even delay the need for corneal transplantation. 4
The benefits of ICRS have been established in the literature for the treatment of keratoconus, with much less risk involved, showing to be an effective and safe alternative for the treatment of the condition.5–9 However, the intracorneal ring has been limited to eyes with Kmax (maximum keratometry) values less than 58 D, as larger curvatures could be associated with worse visual outcomes and more complications, such as extrusion. 10
Despite the existing studies on ring implants addressing the outcomes of intracorneal ring implantation in advanced keratoconus, these studies are limited to patients with maximum curvatures lower than 60D.8,11,12 This is the first study to show the results of the Ferrara ring of 320° of arc (AJL, Vitoria, Spain) as an alternative therapy in patients with advanced keratoconus, grade IV, with Kmax > 60D, intolerant to contact lens, and with indication for corneal transplantation.
Patients and methods
This prospective, interventional case series study evaluates a total of 25 eyes of 19 patients with keratoconus stage IV, according to the ABCD Keratoconus Staging ranking 13 and Kmax > 60D, implanted with 320-ICRS. Uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), keratometric values (mean - mean-K, flat - K1, and steep - K2), maximum keratometry (Kmax), tomographic astigmatism, refractive astigmatism and asphericity (Q) were assessed preoperatively and at the final follow-up visit 12 months after the procedure.
The survey was conducted, with the approval of the ethical committee, in Ver Hospital de Olhos, Goiania, Brazil. All research adhered to the tenets of the Declaration of Helsinki and all patients gave their informed consent prior to the study.
Preoperatively, all patients had corrected distance visual acuity (CDVA) of 0.3 logMAR (20/40) or worse, and inability to wear corneal or scleral contact lens, with previous indication of corneal transplantation. All patients underwent surgery in October 2019, performed by the same surgeon, using VisuMax® femtosecond laser. Patients with central keratoconus, and thickness in ring track > or equal to 400 microns were included in the study. Patients with corneal opacities, those who had undergone previous surgeries, patients with cataracts, strabismus or any fundus condition that could damage the surgical outcome were excluded.
The ring implanted was the ICRS Ferrara ring® (AJL, Ophthalmics, Vitoria, Spain), with 320° of arc in a 5 mm optical zone. In patients with a ring track thickness of 400 to 500 microns, 1 segment of 320/20 was implanted, and in patients with a track thickness > 500 microns, 1 segment of 320/25 was implanted.
Examination protocol
Preoperative and postoperative evaluation included a comprehensive ophthalmologic examination with uncorrected distance visual acuity (UDVA) and CDVA, spheric refraction, and manifest refractive astigmatism (MRA). Slip-lamp examination, Goldmann tonometry, fundus examined 12 months action, corneal tomography (Pentacam, Oculus, Optikgerate, Wetzlar, Germany).
The following corneal tomography data between preoperatively and 1, 3, 6, 9 a 12 months postoperatively were evaluated: flat and steep corneal keratometry, dK and respective axis, mean keratometry, maximum keratometry and average corneal asphericity as 30 angle (Q 30).
Surgical techniques
All surgical procedures were performed under topical anesthesia with 2 anesthetic drops, 1 min before the procedure of proxymetacaine hydrochloride 0,5% (Anestalcon, Alcon Laboratories, Inc., Fort Worth, TX),. Incision and stromal tunnel were both created by using a femtosecond laser VisuMax® (Carl Zeiss Meditec, Oberkochen, Germany). As it was a 320° arch ring, and all patients had central nipple type keratoconus, we implanted all the rings in the 90° axis. Laser parameters included: (1) incision placed at 90 degree in all patients, (2) incision and tunnel depth of 70% of corneal thickness at the thinnest point in the ring track, (3) inner diameter of 4.6 mm, (4) outer diameter of 6.0 mm, (5) entry cut length of 1.2 mm, (6) entry cut thickness of 1 um, (7) ring energy of 1.3 mJ, and (8) entry cut energy of 1.3 mJ.
After incision and tunnel creation, the ICRS was inserted into the circular tunnel using an implantation forceps. The postoperative regimen included moxifloxacin 0.5% and dexamethasone 0.1% eye drop (Vigadexa®, Alcon Laboratories, Inc.) four times a day for 10 days and topical lubrificant with Polyethylene Glycol 400 0.4% also four times a day (Systane UL®, Alcon Laboratories, Inc.) No intraoperative complications occurred.
Follow-up evaluation
Postoperative visits were schedule for 1 day, and 1,3,6,9 and 12 months. On the sixth postoperative month, the Zenlens™ (Solótica) scleral contact lens test was performed on all patients.
Vector analysis
Vector analysis of MRA and dK changes between preoperatively and the final follow-up visit at 12 months were performed using Alpins vector analysis. 14
All vector calculations for the Alphins method were performed using VECTrAK (version 2.4.6; ASSORT Pty. Ltd., Cheltenham, Australia). The followings vectors were determined and evaluated: Target induced astigmatism (TIA), which is the vector of the proposed change in the cylinder for each treatment, surgically induced astigmatism (SIA), which is the vector of the actual change achieved.
The tomographic and refractive vector astigmatism obtained with the implantation of intracorneal ring with 320° of arch in eyes with advanced keratoconus was analyzed. In view of that, representative graphs were generated. In this analytical process, the closer the points are to the blue line, the greater the proximity to the target. The points above the blue line represent eyes with overcorrection of astigmatism, while the points below the blue line represent eyes with undercorrection of astigmatism. The black line represents the trend line: the steeper it is, the higher the correlation between surgical induced (SIA) and target induced astigmatism (TIA).
Statistical analysis
Statistical analyses were performed supported by the statistical package SPSS, version 26.0 (SPSS Inc, Chicago, IL). The sample profile was characterized by absolute frequency (n) and relative frequency (%) for categorical variables, as well as mean and standard deviation for continuous variables. A P value of less than 0.05 was considered statistically significant.
Calculation of the sample size
Sample size was calculated for each variable assessed using the software G.Power® 3.1 (Franz Faul, Universitat Kiel, Germany). It found a minimum estimate of 19 eyes (95% CI: 11 to 26) at a 5% significance level, 95% confidence interval and 99% sampling power to detect statistically significant differences.
The parameter used in the calculation of the sample size was the mean difference of all parameters presented in Table 1, using the same G.Power® 3.1 method. In this way, an ‘n’ was obtained for each parameter. Based on the simple calculations of the confidence interval for these ‘n’ samples, the minimum estimate with the lower and upper limit was obtained. Therefore, it was demonstrated that the ‘n’ sample estimate was adequate for all parameters
Visual acuity, refraction and tomography outcomes
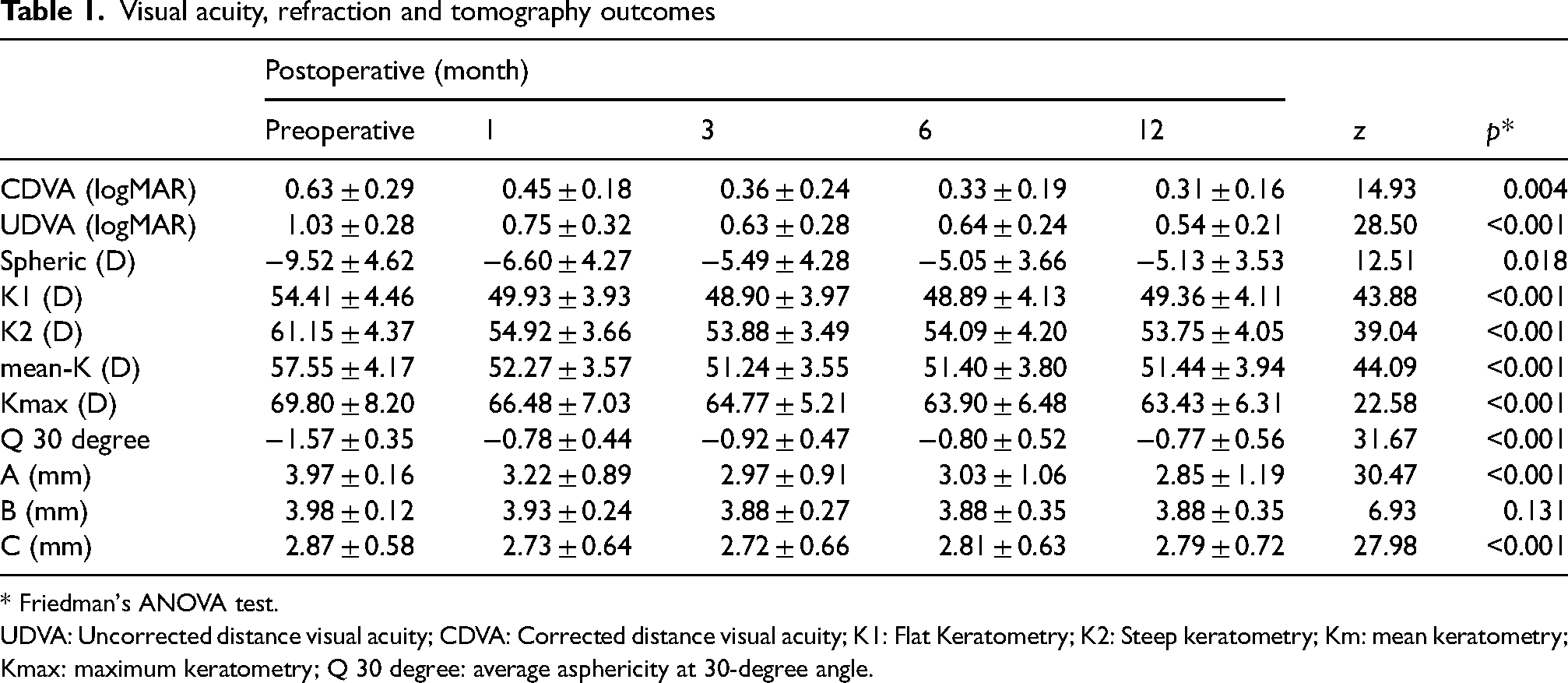
* Friedman's ANOVA test.
UDVA: Uncorrected distance visual acuity; CDVA: Corrected distance visual acuity; K1: Flat Keratometry; K2: Steep keratometry; Km: mean keratometry; Kmax: maximum keratometry; Q 30 degree: average asphericity at 30-degree angle.
Based on this, the mean difference and standard deviation of the preoperative and postoperative periods were verified, and the mean difference of all other parameters reviewed were used together for the sample estimate. Based on these parameters, the more significant the difference between the pre and postoperative periods, the smaller the “n” needed to achieve a 99% sample power. Since the “p” value was highly significant between the pre and postoperative analysis, the “n” needed to achieve a 95% sample power, considering this significance level of 5% and confidence interval of 99%, was 19 eyes.
Safety and efficacy criteria of the proposed treatment
One criterion to evaluate the safety of the treatment was the mean postoperative CDVA higher than the mean preoperative CDVA. Another criterion was based on observed loss of more than one line of sight in the corrected visual acuity at the end of the follow-up. The procedure would be considered safe if less than 10% of the patients lost more than one line of sight. An additional safety criterion considered was the rate of complications: if there were less than 10% of complications inherent to the surgery, the procedure would be considered safe.
The mean postoperative UDVA higher than the mean preoperative CDVA was the criteria to examine the effectiveness of the proposed treatment. It was considered the distribution of corrected distance visual acuity, comparing pre- and post-operative - here, vision corrected with glasses was another parameter of treatment efficacy. Surgery would be considered effective in this regard if the majority of patients reached a visual acuity corrected with glasses better than or equal to 20/40.
Another parameter considered to evaluate treatment efficacy was the number of patients who had their VA restored with the use of scleral contact lens after 320-ICRS implantation. The procedure would be considered effective if the majority achieved VA wearing lens better than or equal to 20/25.
Results
A Total of 25 eyes of 19 patients were included. The mean age was 22.8 ± 7.9 years (range: 15 to 31 years). In 19 eyes was implanted a 320/200 ring and in 6 eyes was implanted a 320/250 ring. One eye was excluded of the analysis because we had to explant the ring after 15 postoperative days.
The table below discloses the pre and postoperative values of the main variables analyzes, showing the preoperative progress on the 12th postoperative month (Table 1).
Spherical equivalent
Figure 1 Shows the stability of SE refraction between preoperative and postoperative intervals
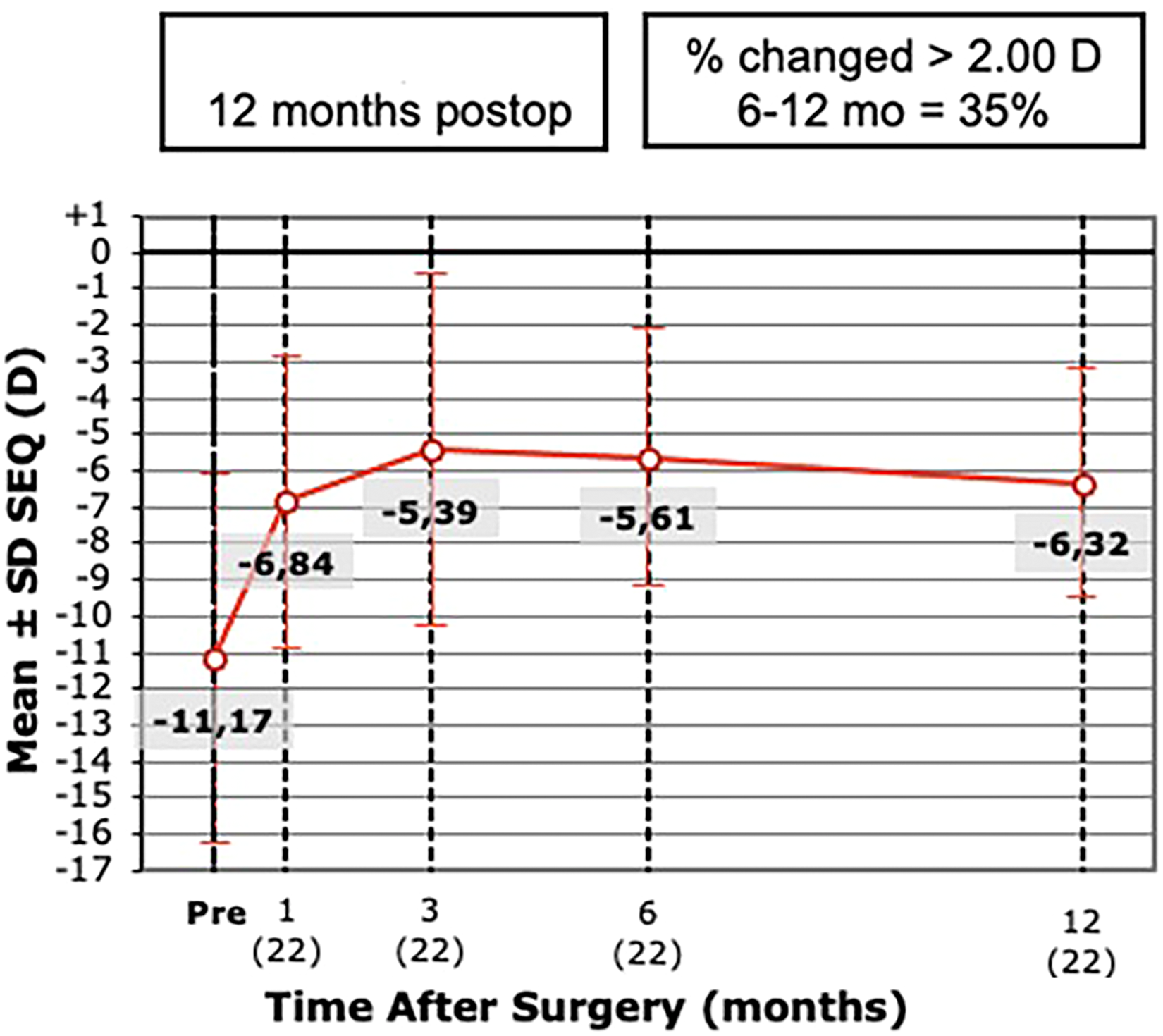
Stability of spherical equivalent refraction during postoperative intervals.
Vector astigmatism
Vector analysis of corneal astigmatism changes
Figure 2 illustrates the relationship of the target induced astigmatism (TIA); surgically induced astigmatism(SIA). The correction index is the ratio SIA / TIA. The correction index is preferably 1.00; it is higher than 1.00 if an overcorrection occurs and less than 1.00 if there is an undercorrection. In this case the correction index was 0.53, meaning an undercorrection of the tomographic astigmatism.
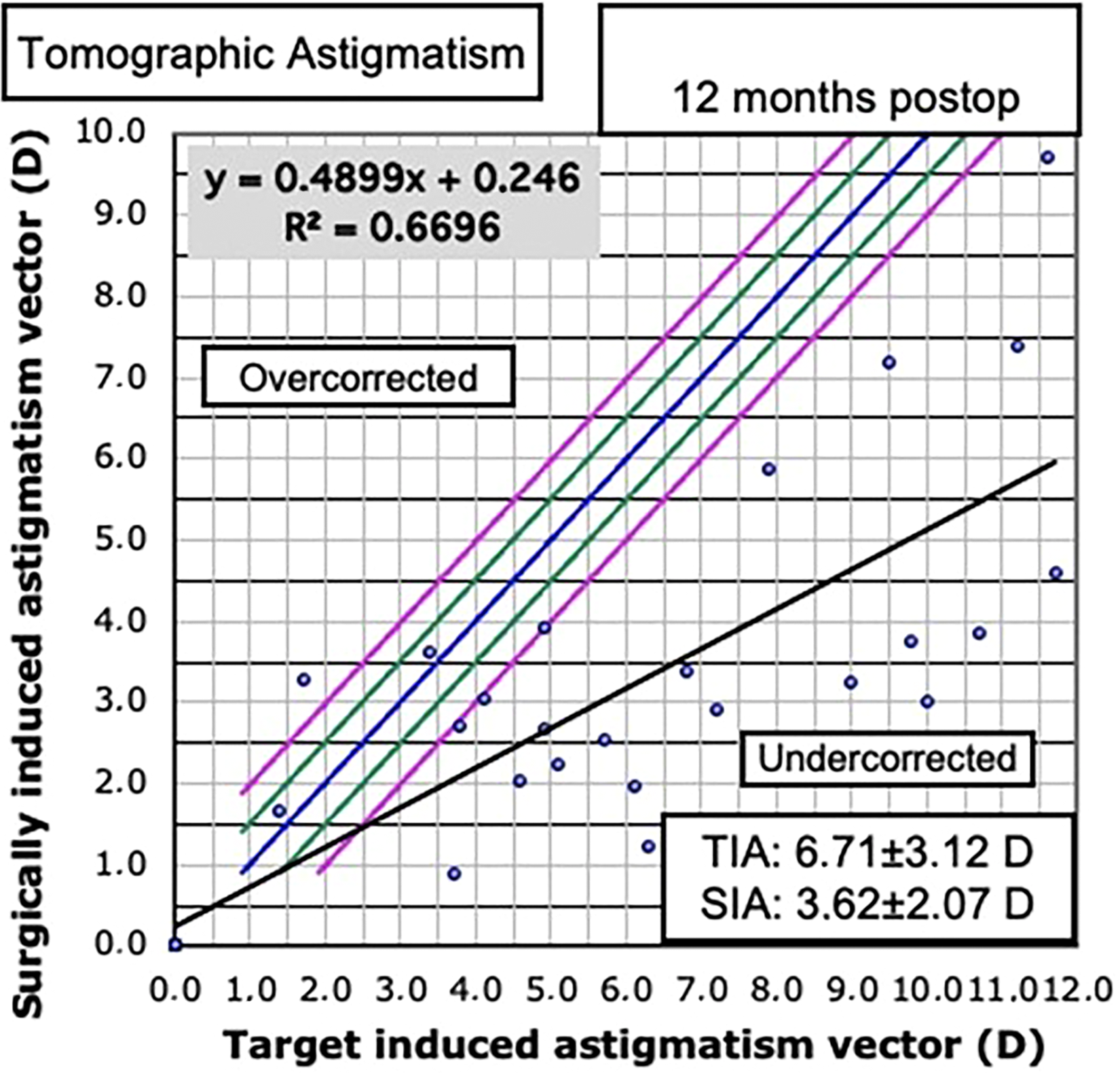
Target induced astigmatism (TIA) vs. surgically induced astigmatism (SIA) with implantation of the 320-degree arc intracorneal ring in eyes with advanced keratoconus.
Figure 3 discloses the distribution of tomographic vector astigmatism before and after the implantation of intracorneal ring with 320 degrees of arch in eyes with advanced keratoconus.
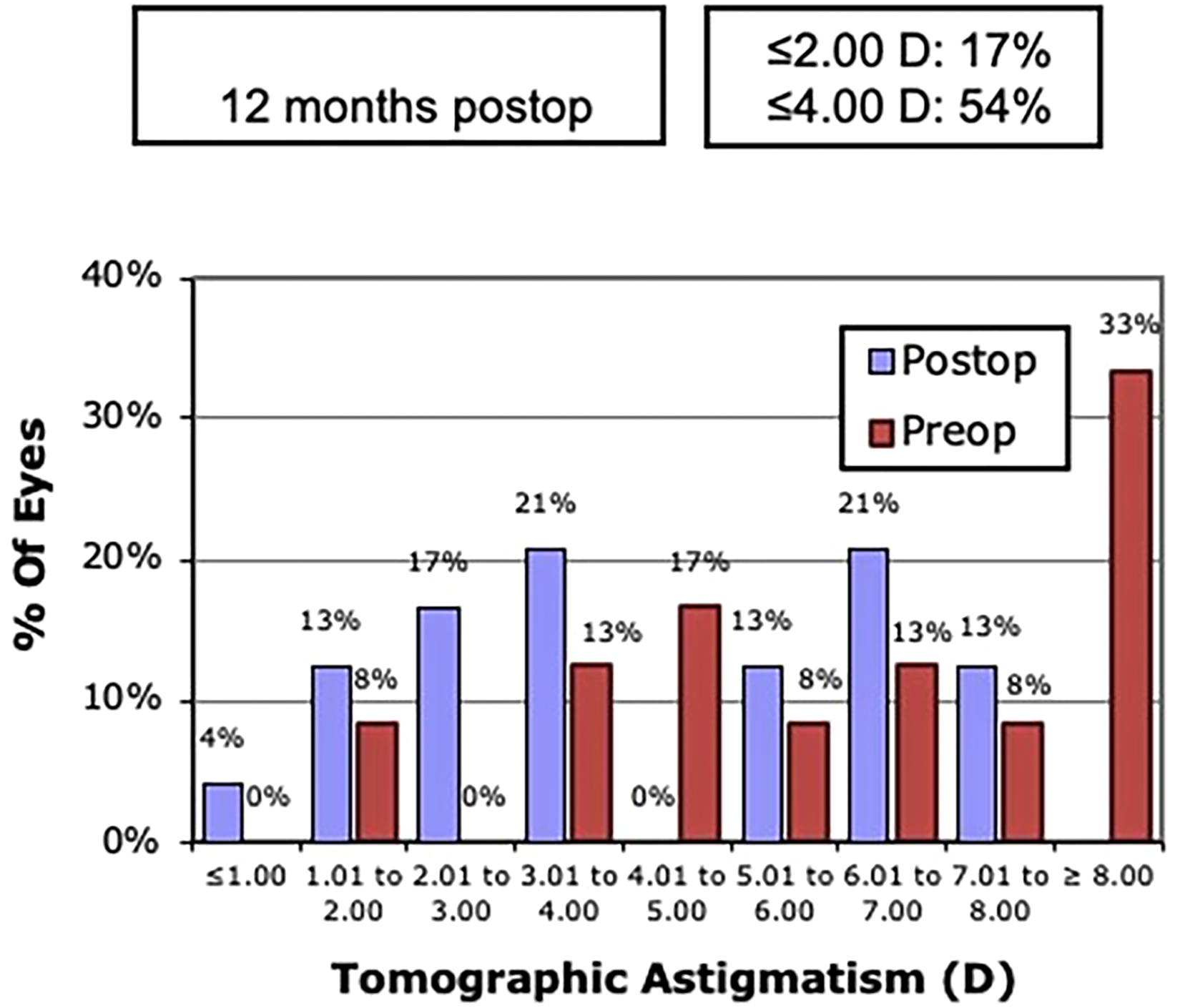
Distribution of tomographic astigmatism before and after implantation of intracorneal ring with 320 degrees of arch.
Safety, treatment failure, and complications
Among the 25 eyes evaluated, one (1) eye lost two lines of sight (4.5%), one (1) eye lost one line of sight (5%), three (3) eyes maintained the same visual acuity (14%), two (2) eyes gained two lines of sight (9%), and 18 eyes gained three (3) or more lines of sight (68%).
One of the safety criteria was the mean postoperative CDVA greater than the mean preoperative CDVA. The mean postoperative CDVA was 20/40 (0.31 ± 0.16 LogMAR), better than the mean preoperative CDVA (20/80 or 0.63 ± 0.29 LogMAR).
The procedure was considered safe, in that 9.5% of patients lost one or more lines of sight (<10%) and only 4% of patients undergoing ring implantation with 320 degree of arch (one patient) had a complication inherent to the procedure (Figure 4). No intraoperative complications were observed. One patient's eye developed an infectious stromal infiltrate on the ring track day 7 of the postoperative period, and was prescribed with Vigamox antibiotic eye drops every two hours. However, as the patient had no improvement, the therapy was changed to fortified antibiotic eye drops (ceftazidime and gentamicin) and, as there was no improvement either, it was necessary to explant the ring. There was no sequel. No cases of ring extrusion, perforation or migration were observed.
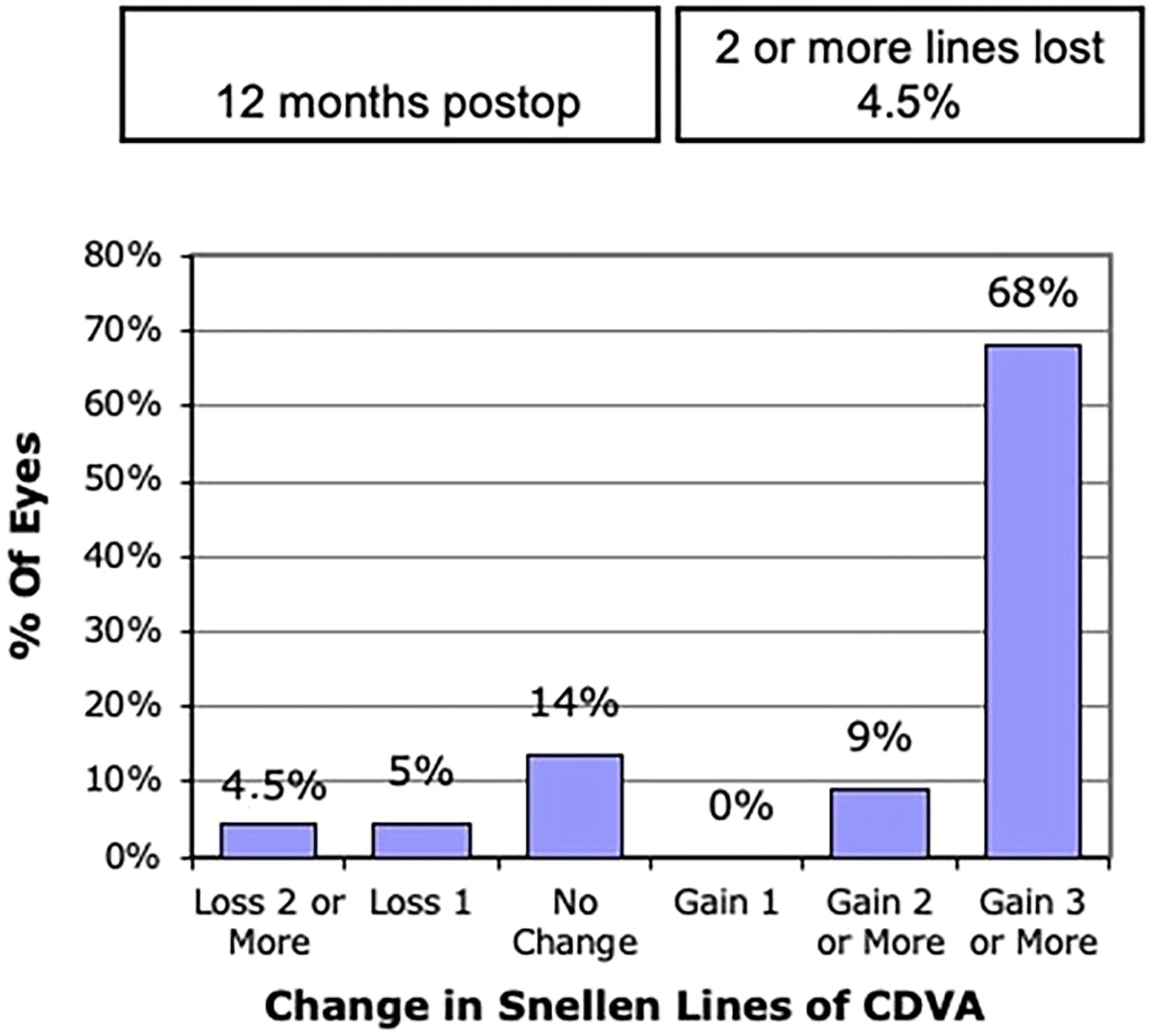
Safety graph illustrating the changes in the snellen lines according to corrected distance visual acuity after 12 months postoperatively.
Treatment efficacy
Figure 5 illustrates the distribution of the percentage of patients with corrected distance visual acuity in preoperative and the postoperative uncorrected distance visual acuity. Postoperatively, 70% of the patients had corrected distance visual acuity better than or equal to 20/40 (Figure 6). All patients underwent scleral contact lens testing six months after surgery. Figure 7 shows that 80.9% of patients had visual acuity better than or equal to 20/25 after 12 months of the scleral contact lens surgery. The mean postoperative UDVA was 20/60 (0.54 ± 0.21 LogMAR), higher than the mean preoperative CDVA which was 20/80 (0.63 ± 0.29 LogMAR). All these points confirm the efficacy of the proposed treatment.
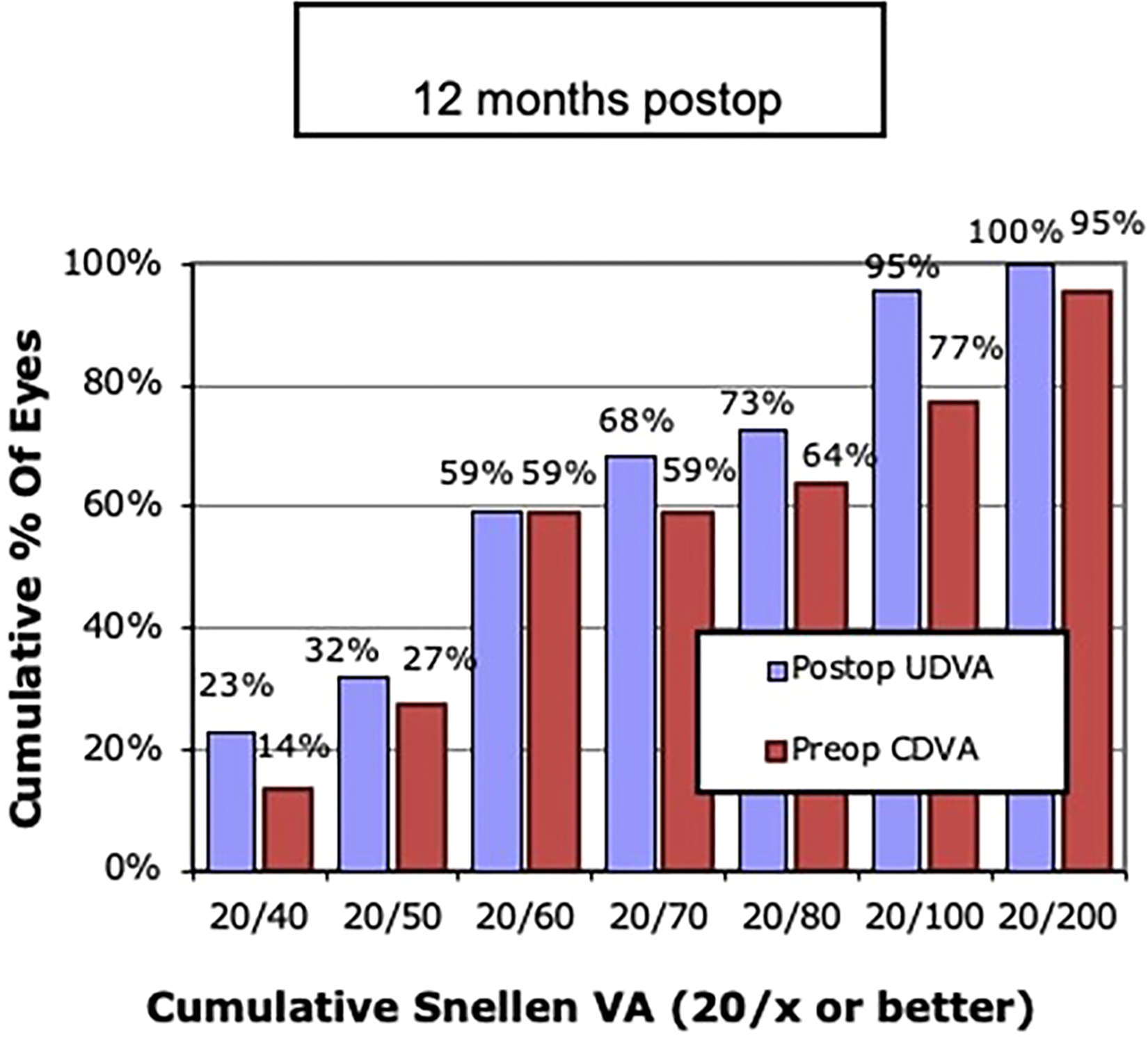
Effectiveness of intracorneal ring implantation surgery illustrating the percentage distribution of postoperative uncorrected distance visual acuity (UDVA) and preoperative corrected distance visual acuity (CDVA).
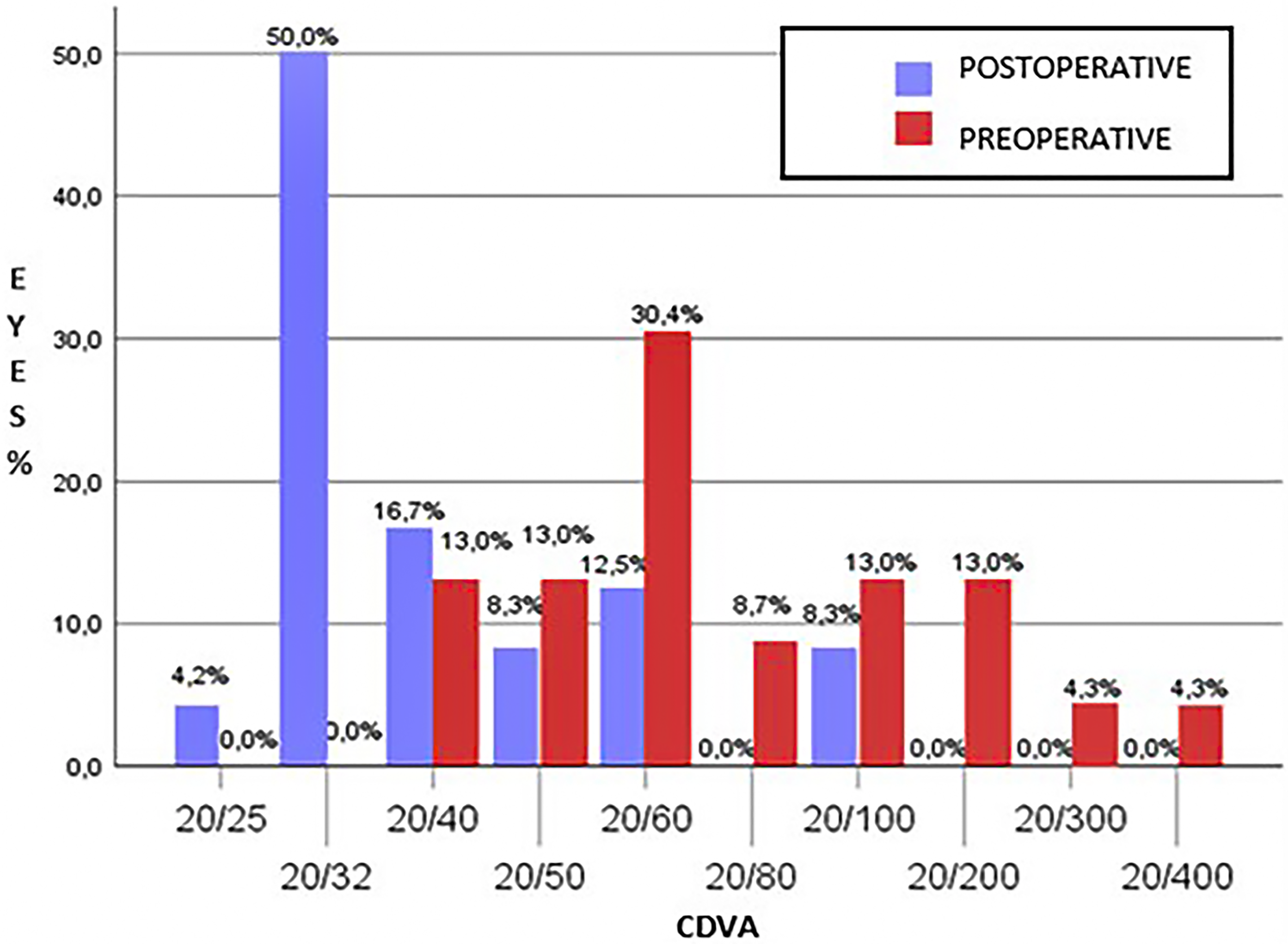
Percentage distribution of patients according to the visual acuity achieved postoperatively wearing glasses (CDVA) comparing pre- and post-surgery.
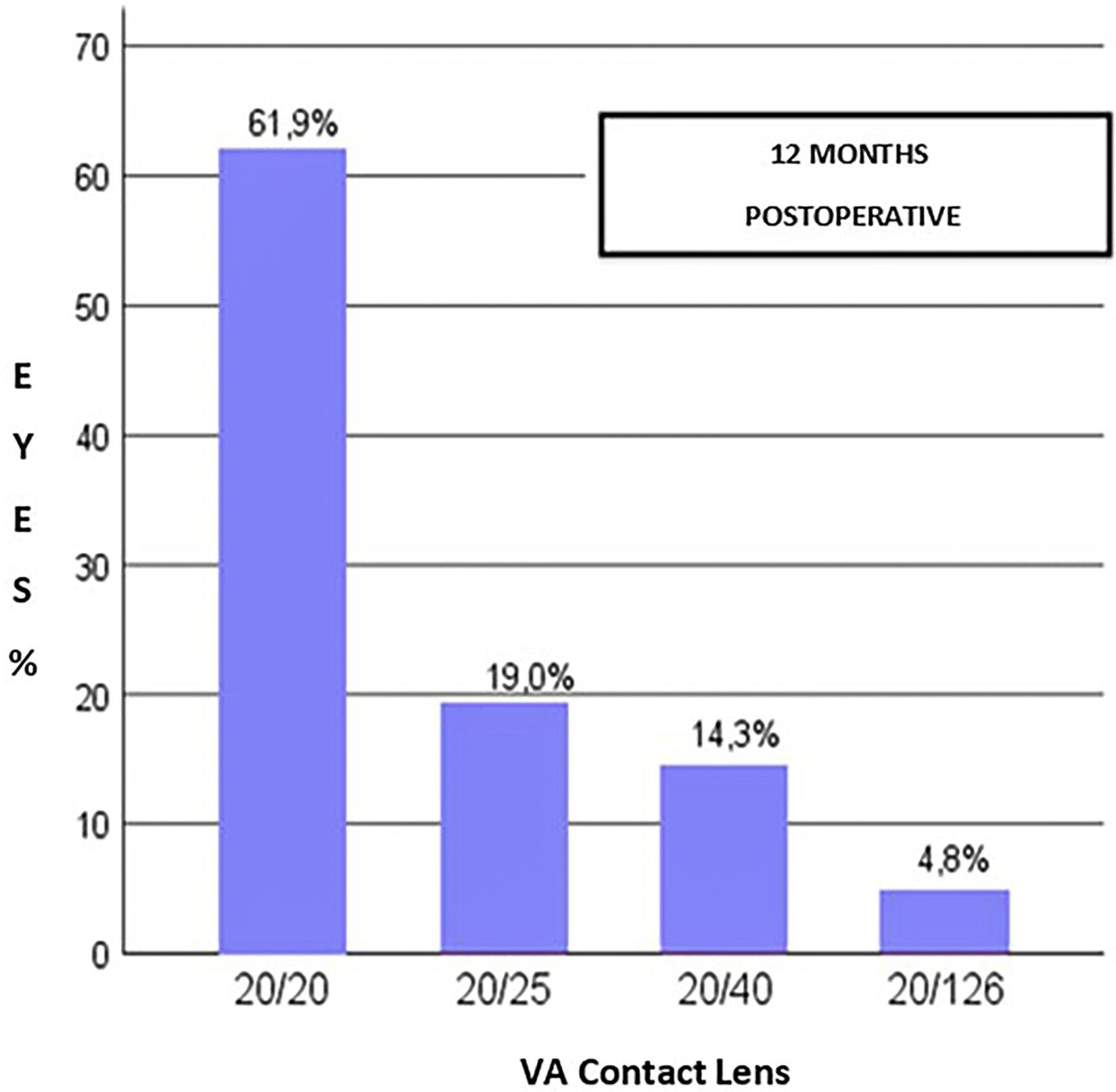
Percentage distribution of patients according to the visual acuity achieved postoperatively wearing contact t lens (CDVA).
Discussion
Corneal transplantation has been considered to be the best option of treatment for visual rehabilitation in patients with advanced keratoconus.15,16 large sample cohort studies shows that the rate of need of graft procedure in keratoconus patients can vay from 12 to 21.6%.17,18 However, visual rehabilitation in transplant patients can be slow and unsatisfactory, especially due to high post-transplant astigmatism, corneal irregularity, anisometropia, and risk of rejection. 19
Many studies adopted as exclusion criteria for intracorneal ring implantation, patients with corneal curvatures greater than 60D, showing low effectiveness for the treatment of more advanced cases of the condition.10,20 Other studies have shown high rate of complications, such as persistent epithelial defects, anterior and posterior corneal perforations, extension of the incision to the visual axis, superficialization and extrusion of the ring.21,22
The progress of intracorneal ring implantation surgery resulting from the advent of the femtosecond laser has considerably changed this scenario, making the surgery safe and efficient even in very advanced cases. In the current study, in which rings were also implanted with the aid of the femtosecond laser, there was no extrusion. This supports the descriptions that laser-assisted intracorneal ring implantation is more predictable and safer. Another factor that has contributed to this new scenery is the advent of new designs of corneal ring segments, such as long-arch rings with smaller diameters capable of flattening the cornea in a more significant way, thus proving to be more suitable for more advanced cases.23,24 Previous studies on intracorneal ring implantation in advanced keratoconus did not include eyes with keratometry greater than 65 D.11,12,24,25 This is an important differential in this study, since one of the inclusion criteria was Kmax greater than 60 D (ranging from 60 D to 87.4 D). Thus, it allowed assessing the behavior of the intracorneal ring in eyes with such high keratometry for the very first time.
The rate of complications in the present study was low (only one case) and no case of extrusion or superficialization of the ring was observed. This is a frequent concern in extreme cases, and proved this is a safe procedure. The current study allowed us to observe that in central keratoconus with extreme curvatures (Kmax 83D), the major thinning was located outside the ring track. Therefore, all eyes included had a thickness greater than 400 microns in the track, making the ICRS implantation safe.
A previous study compared visual and refractive outcomes in eyes with advanced keratoconus that underwent deep anterior lamellar keratoplasty (DALK) with those undergoing intracorneal ring implantation. The results showed statistically significant visual improvement in both groups, with greater gain in vision in the DALK group. However, although DALK involves lower risks of rejection compared to penetrating transplantation, intracorneal ring surgery has been suggested as an alternative treatment with satisfactory results, considering the greater ease of ring implantation technique, associated with fast postoperative recovery and low complication rates involved when compared to transplantation. All these suggest it is a good alternative prior to transplantation. 25
A recent study comparing different treatment approaches for advanced keratoconus also considers that, although in some aspects DALK shows more satisfactory results than intracorneal ring implantation, patients should go through each stage of treatment, respecting the proper indications and observing potential complications inherent to each procedure. According to Rocha et al, 14.28% of patients who underwent DALK presented postoperative complications, and 17.86% were unable to wear contact lenses to complement visual improvement. On the other hand, no complication was observed in the group that had the ring implant. 26 Only one case of complication was observed in this study; 70% of patients achieved corrected distance visual acuity better than or equal to 20/40 (0.3 logMAR), and 80% of patients achieved visual acuity better than or equal to 20/25 (0.1 logMAR) with the use of scleral contact lenses, reporting comfort with use.
It is worth mentioning that the intracorneal ring implantation, especially in advanced cases, is not a refractive procedure, since the main objective is not to reach the best uncorrected distance visual acuity, but to reestablish the patient's corrected vision, wearing either glasses or contact lenses. 27
A study that evaluated the results of INTACS in advanced keratoconus defined the procedure as effective when most patients achieved a CDVA better than or equal to 20/40 (0.3 logMAR). Another parameter used as a criterion of effectiveness would be the mean postoperative uncorrected distance vision better than the mean preoperative corrected distance vision. 11 Although criterion is more valuable for refractive procedures, since the ring surgery does not aim at obtaining good uncorrected distance visual acuity, observing the results found in this present study, most patients (70%) reached CDVA wearing glasses better than or equal to 20/40, and the average preoperative CDVA was 0.63 logMAR (20/80), worse than the average UDVA postoperatively that was 0.54 logMAR (20/60).
According to the safety criteria proposed by this study, intracorneal ring implantation would be considered safe if the mean postoperative CDVA was greater than the mean preoperative CDVA, if the loss of lines of sight was less than 10%, and if complication rate was below 10%. The results show that mean pre-op CDVA was 0.6 logMAR (20/80) and the post-op CDVA was 0.31 logMAR (20/40), only 9.5% of patients lost lines of sight, and the complication rate was only 4% (1 case). Therefore, we can consider the procedure safe.
This study showed that patients with keratoconus in advanced stages may benefit from the intracorneal ring implantation, which proved to be an effective and suggests to be a safe technique with low risks of complications. Therefore, considering its feasibility, it should be a procedure to be considered before indicating corneal transplantation.
Higher keratometric values alone, announced as predictors of unsatisfactory results, are not limiting factors for the indication of intracorneal ring implantation.
One of the limitations of the present study was the absence of a control group of patients submitted to corneal transplantation, both lamellar and penetrating, a treatment traditionally recommended for cases of advanced keratoconus, to allow a comparison with the results of the intracorneal ring implantation with 320° of arch for advanced keratoconus. Since this was a preliminary case series study, will be needed studies with larger sample sizes and longer follow up time to support the results disclosed in the present study.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs. P. Ferrara, G. Ferrara, have a financial interest in the Ferrara intrastromal cornea ring. The remaining authors have no financial or proprietary interest in the materials presented herein.