
Abstract
Purpose
To determine the sensitive indices distinguishing forme-fruste keratoconus (FFKC) and early keratoconus (early KC) from thin normal corneas, and their cutoff values using Sirius topography.
Methods
156 eyes with normal thin corneas < 500 um (group 1), 99 eyes with early KC (group 2) and 41 eyes with FFKC (group 3), were assessed retrospectively for: corneal keratometric indices, pachymetry indices, corneal aberrations, elevation indices; thinnest corneal point elevation, Q value, root mean square (RMS) withRMS/ area (RMS/A); and KC summary indices of front and back surfaces; surface asymmetry index (SIf, SIb), elevation at KC vertex (KVf, KVb), Baiocchi-Calossi-Versaci index (BCVf, BCVb) and summation of its vector (BCV). Cutoff values were calculated.
Results
Keratometry indices were significantly different between early KC and thin normal cases (apex front curvature had the highest area-under-the-ROC-curve (AUROC) (0.926) in early KC, while only apex curvature and coordinates were significant in FFKC cases. Pachymetry indices did not show any significance in differentiating either early KC or FFKC from normal thin corneas. KC summary indices were highly significant among the 3 groups. The highest AUROC was observed with KVb in early KC (0.987) and with KVf in FFKC (0.831). Vertical coma and vertical trefoil showed the highest significance of all aberration parameters differentiating the 3 groups. Thinnest point elevation, RMS and RMS/A showed the highest AUROC in differentiating early KC and FFKC cases from thin normal corneas.
Conclusion
Comparing early KC and FFKC to thin normal corneas, Sirius provided high precision in prediction.
Introduction
Keratoconus (KC) is an ectatic dystrophy of cornea characterized by a progressive thinning and consequently steepening of the cornea, resulting in uncorrected irregular astigmatism. 1 Diagnosing KC in its earliest stage is one of the most important aspects of avoiding iatrogenic corneal ectasia during refractive surgery. 2
Forme fruste keratoconus (FFKC) was firstly proposed by Amsler 3 in 1961 and then adapted by Klyce 4 as “The fellow eye of a clinical manifest KC eye that has no clinical findings of any sort except for certain topographical changes. 2 Differentiating FFKC from early KC is mandatory as Xiaohui et al proved that approximately 50% of clinically normal fellow eyes will progress to KC within 16 years. 5
According to Gatinel, terms such as “subclinical KC,” “KC suspect,” and “forme fruste KC,” have been interchangeably used to describe early forms of KC, and he proposed generalizing the term “subclinical KC” to all corneas in which the phenotypic expression of KC is sufficiently minor to remain asymptomatic. 6
Published studies indicated that the central corneal thickness was a useful parameter to identify clinical KC.7,8 Although KC populations have significantly thinner corneas than healthy individuals, the thickness values of thin non- KC corneas partially overlap with the subclinical KC corneas,9,10 besides corneal thickness varies among eyes from different regions and ethnicities. 11 Accordingly, the non-keratoconic thin corneas (<500 μm) have special considerations in refractive surgery because as corneal thickness decreases, decision making for or against refractive surgery gets more crucial. 9
The aim of this study is to detect the most diagnostic indices to differentiate normal thin corneas from subclinical or FFKC and from early KC and to detect the cutoff values of the measured indices comparing the 3 groups.
Patients and methods
This is a retrospective cohort observational study that was carried out at the Eye World Hospital, in Dokki, Giza, Egypt. Medical records and topography scans using Sirius device (CSO, Costruzione Strumenti Oftalmici, Florence, Italy, version 3.2.1.60) of refractive surgery candidates were reviewed from Jan 2017 to June 2021. A total of 296 eyes of 296 cases were included, cases were categorized into 3 groups:
Before examination, all candidates removed their rigid contact lenses for 3 weeks and soft lenses for 2 weeks. We did not include any opacity visible in the Scheimpflug pictures, evident corneal scarring, obvious anterior segment disease on examination, or prior ocular trauma or procedures. All participants were required to sign informed consent forms before being included in the study as part of their preoperative refractive examination, which was conducted in accordance with the tenets of the Declaration of Helsinki and authorized by Cairo University's ethical committee.
Spherical equivalent and Best Corrected Visual Acuity (BCVA) were reported for each patient. As a routine, 4 reliable scans with highest quality were obtained by Sirius topographer and the one with best acquisition quality was taken in the study.
The investigated indices included
- At 3- and 5-mm circles, the anterior and posterior keratometric indices (K1, K2) were obtained. - Sim K1 and K2 values - Curvature and XY coordinates of the front and back corneal apices (representing the points with highest keratometric value).
- Central Corneal Thickness (CCT) - Thickness of the thinnest corneal point (TL) with its XY coordinates - Thickness at the point representing the apex of cornea.
- Best-fit sphere flat and steep radii (BFS) of aspherotoric reference surface - Q-value, representing the asphericity of the cornea. Elevation at the thinnest point. - Root Mean Square (RMS): - Root Mean Square per area. (RMS/A)
- - -

Analysis was performed on the front surface index (BCVf), back surface index (BCVb), and summation of both surfaces index (BCV).
Statistical analysis
All data were collected from Sirius machine as a .csv file and converted into .xlsx files by MS 356 Excel program (Redmond, Washington, USA). Then statistical analysis was done by MedCalc Statistical Software version 18.9.1 (MedCalc Software bvba, Ostend, Belgium).
All data were shown as mean ± SD and 95% confidence interval (95% CI) except for age and gender which were shown as frequency. Comparing age between groups was done using Kruskal-Wallis ANOVA test.
We have compared the two groups by unpaired t-test in which a statistically significant value was set if (p value < 0.05).
While comparing sensitivity and specificity of different values and the defining the value with best sensitivity and specificity cut off was done using DeLong method of area under the receiver operating characteristic curve (AUROC)
Results
Table 1 showed the demographic data of included subjects in 3 groups, with no statistically significant age difference between the three groups (P = 0.572). Table 2 showed the mean and standard deviation of keratometry, pachymetry, and KC summary indices together with corneal aberrations in the 3 groups and calculated the difference between the 3 groups and their AUROC values.
Demographic data of 3 groups

Showing the mean and standard deviation of keratometry, pachymetry and keratoconus summary indices together with corneal aberrations in the 3 groups and calculates the difference between the 3 groups and their AUROC values
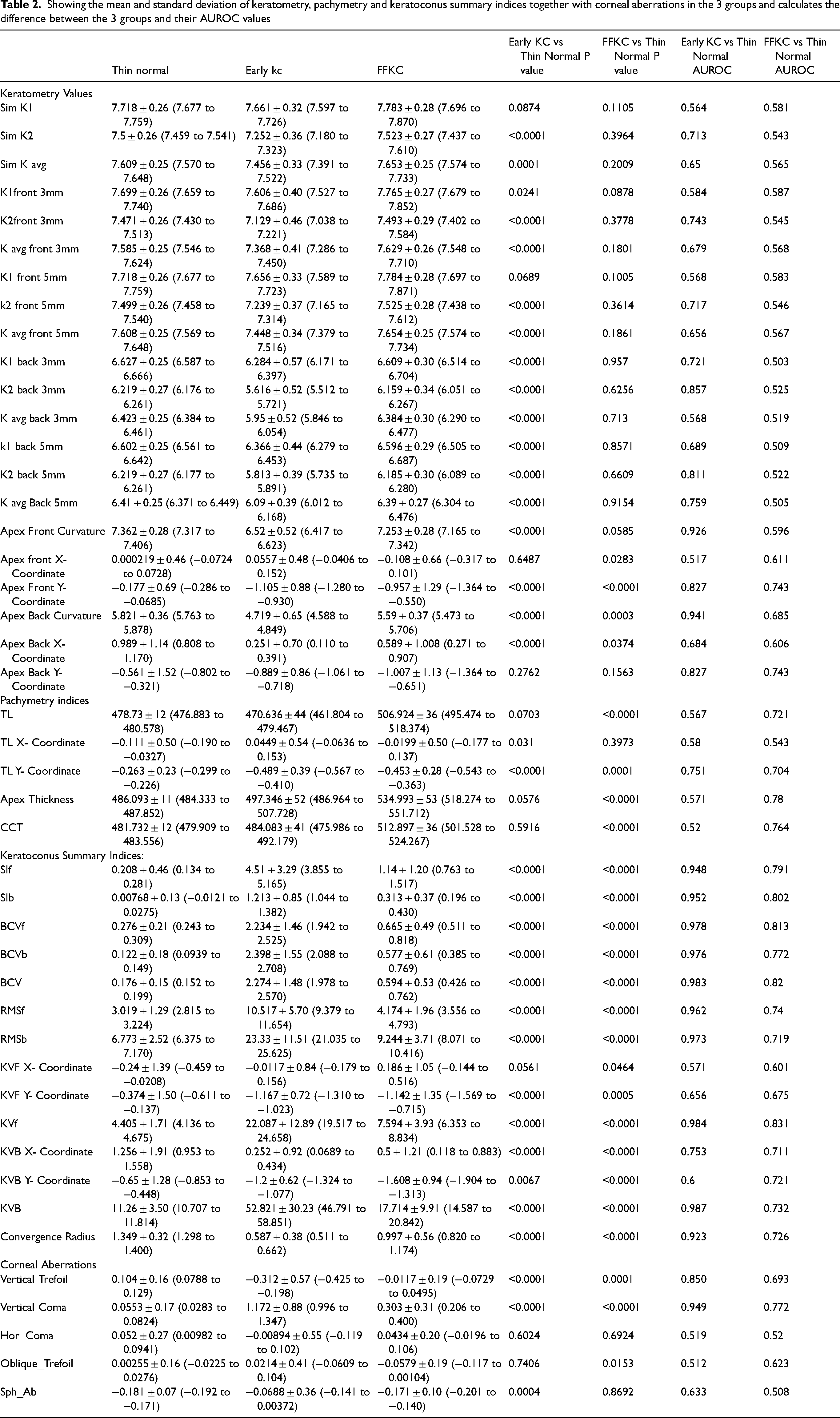
Many of the keratometry indices showed high significance in differentiating early KC from normal thin corneas, although only a few of them; including apex curvature and its coordinates, were significant comparing FFKC and normal thin corneas. Some of the
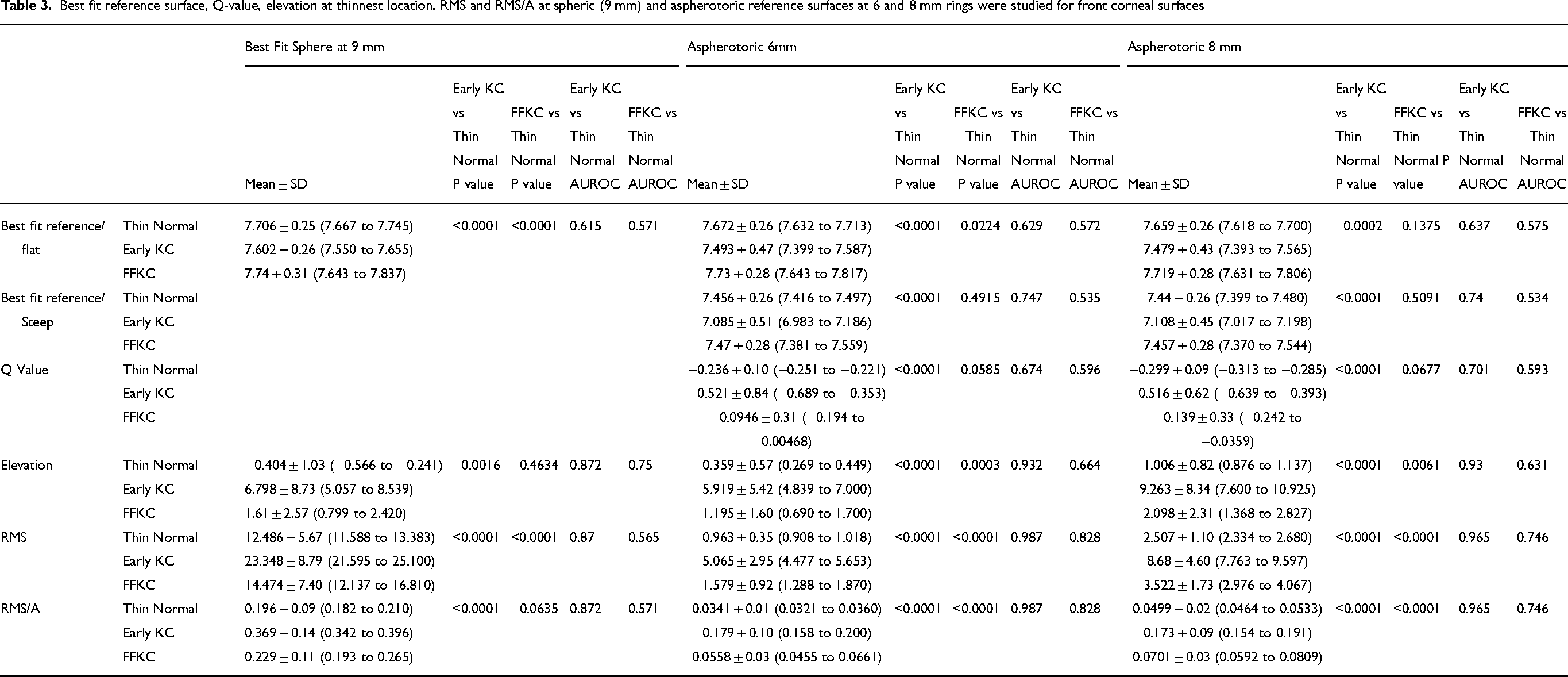
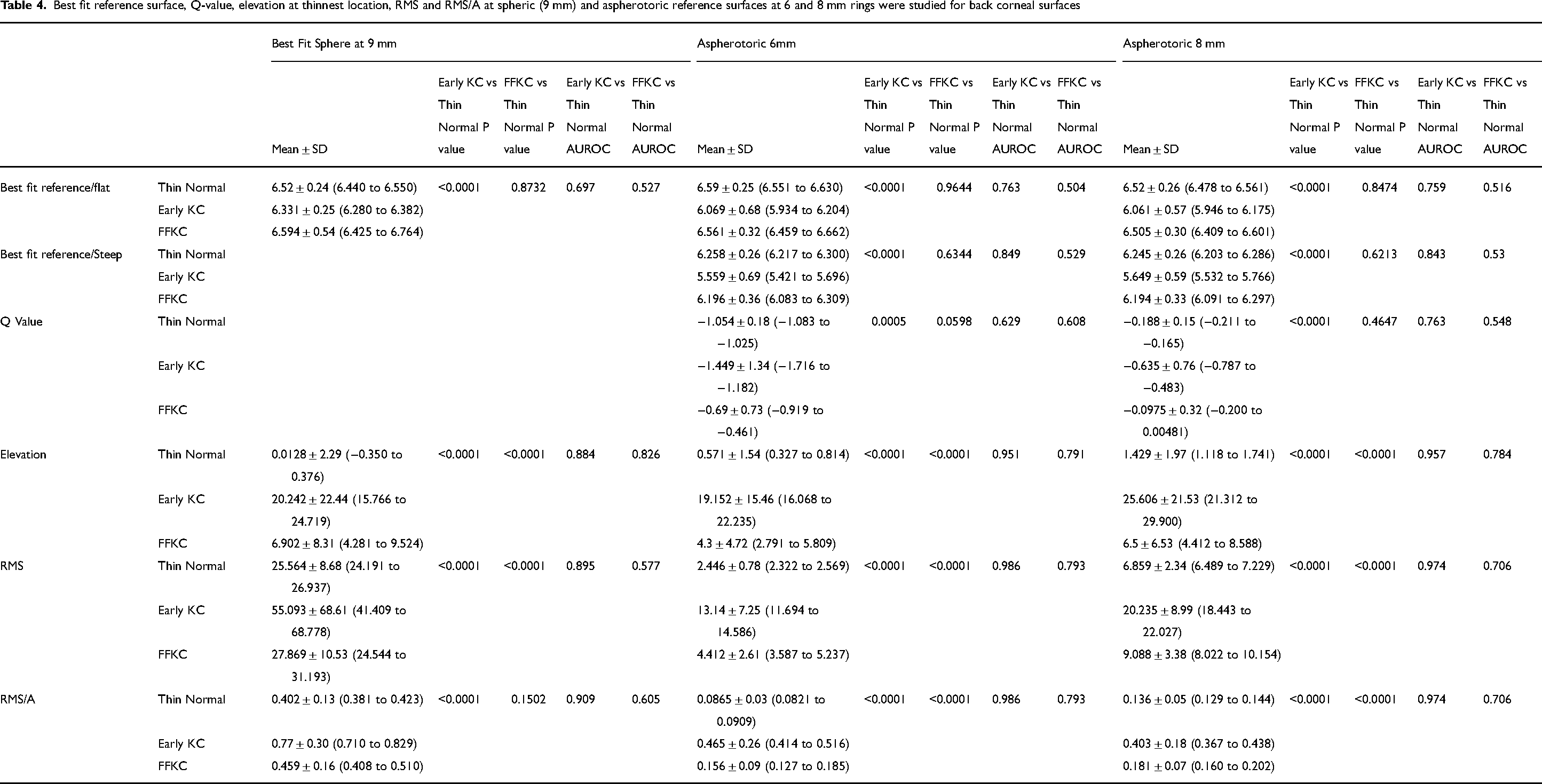
Best-fit reference surface, Q-value, elevation at the thinnest location, RMS and RMS/A at spheric (9 mm), and aspherotoric reference surfaces at 6- and 8-mm rings were studied for both front (Table 3) and back (Table 4) corneal surfaces. All the measured elevation indices showed a high statistically significant difference between early KC and normal thin corneas while the highest AUROC (> 0.9) was recorded in elevation indices at aspherotoric reference surface at 6- and 8-mm rings. Elevation at the thinnest point, RMS and RMS/A of the front and back surfaces were the most statistically significant elevation indices differentiating FFKC from normal thin corneas, especially at aspherotoric reference surface at 6- and 8-mm rings, although only RMS and RMS/A (front) at the 6 mm ring had a moderate AUROC (> 0.8).
Best fit reference surface, Q-value, elevation at thinnest location, RMS and RMS/A at spheric (9 mm) and aspherotoric reference surfaces at 6 and 8 mm rings were studied for front corneal surfaces
Best fit reference surface, Q-value, elevation at thinnest location, RMS and RMS/A at spheric (9 mm) and aspherotoric reference surfaces at 6 and 8 mm rings were studied for back corneal surfaces
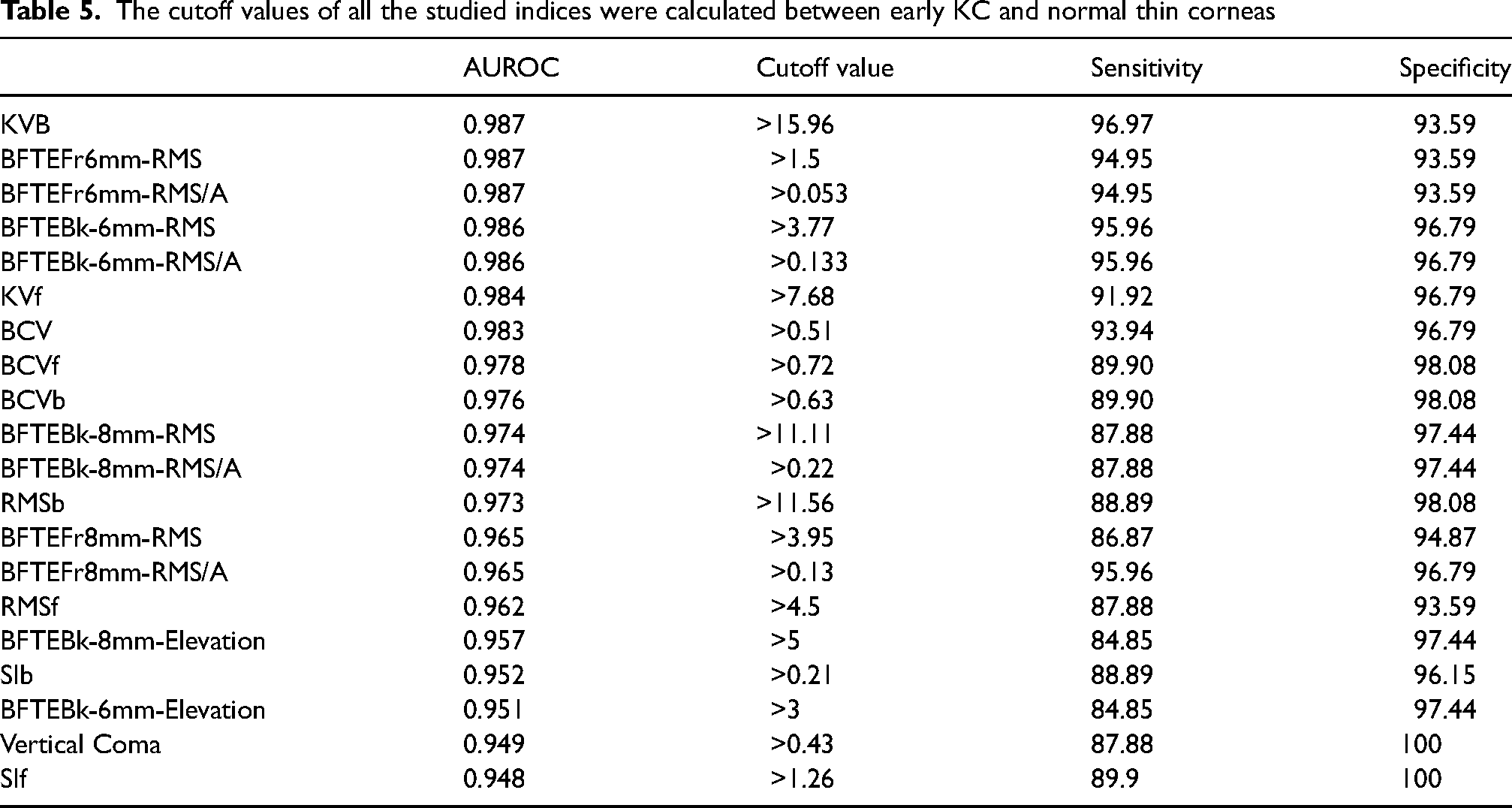
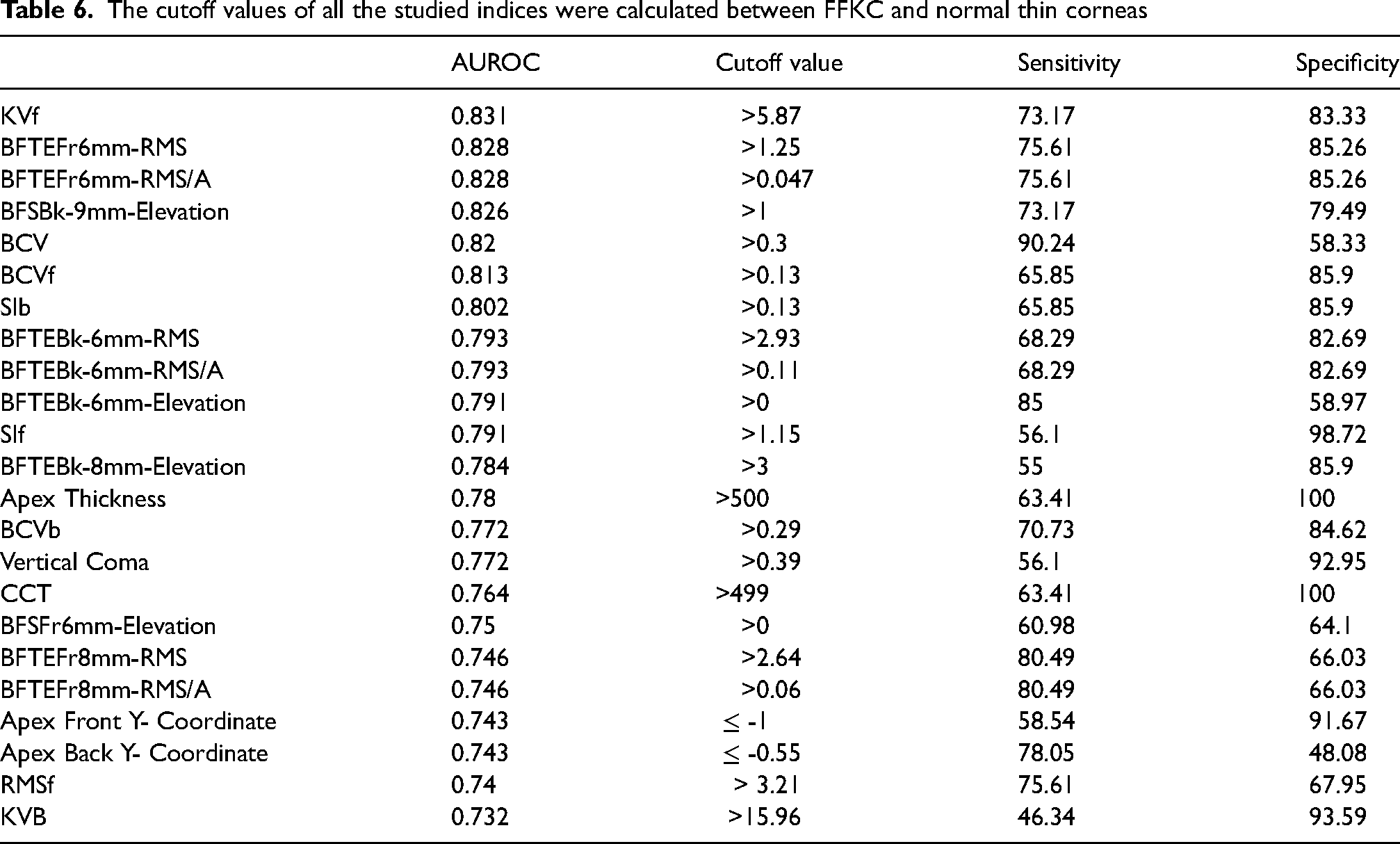
The sensitivity and specificity of the examined indices were used to derive the cutoff values between early KC and normal thin corneas (Table 5) and between FFKC and normal thin corneas (Table 6). None of the measured indices comparing the 3 groups showed 100% sensitivity, KVb showed the highest sensitivity (96.97%) comparing early KC and normal thin corneas with a cutoff value of 15.96, while BCV had the highest sensitivity (90.24%) comparing FFKC and normal thin corneas with cutoff value of 0.3. A 100% specificity was met with vertical coma and SIf comparing early KC and normal thin corneas. As corneal thickness was significantly higher in FFKC, CCT and apex thickness showed 100% specificity when comparing FFKC and normal thin corneas, despite low sensitivity (63.41% both).
The cutoff values of all the studied indices were calculated between early KC and normal thin corneas
The cutoff values of all the studied indices were calculated between FFKC and normal thin corneas
Discussion
Differentiating KC in its early stages is difficult. Corneal thickness used to be an important diagnostic tool for early detection of KC, although a group of normal population with thin corneas, < 500 um, would be a serious challenge for refractive surgery as proper patient selection is challenging in such cases, because preoperative thin corneas and thinner residual stromal bed after excimer laser ablation are widely described as risk factors for the development of postoperative ectasia. 14 Numerous studies have emphasized the value of many indices in early detection of KC as KC indices15–18 pachymetry progression9,19 elevations15,16 and aberrations, 20 but none of them investigated the full set of diagnostic indices form the combined Scheimpflug placido tomography (Sirius) in FFKC and early KC.
It was found that combination of different keratometric (power), thickness and elevation parameters would provide more accurate diagnosis of early KC cases. 21
KC cases included in this study were only in the early stage, this could be the reason only a few of the studied curvature indices had high predictability. The highest AUROC (> 0.9) was observed with anterior and posterior apex curvature (0.926, 0.941 respectively), and with front and back symmetry indices (0.948 and 0.952 respectively). SIf and SIb were the keratometry indices with highest predictability of FFKC (0.791, 0.802 respectively) with lower cutoff values (1.13, 0.13 respectively) than those for early KC. Our cutoff values were close to those estimated by
Elevation indices have shown excellent predictability for early stages of KC.13,22,23 We agree with
Knowing the cutoff values for different elevation indices using Sirius is mandatory, as it proved to have lower cutoff values than Pentacam and Orbscan topographers.
12
Elevation at the thinnest point of anterior and posterior surfaces differentiating either early or subclinical KC from normal thin corneas, showed much lower values than those recorded by
The highest sensitivity of all elevation indices (96.97%) comparing mild KC to thin normal cases was noticed with maximum posterior elevation (KVb) having excellent specificity (93.59%) at a cutoff value of 15.96 um, which was close to the cutoff value estimated by
Comparing FFKC with thin normal corneas showed lower cutoff values than comparing them with early KC cases in all studied elevation indices, which would provide higher accuracy in early detection of suspicious cases in such a confusing population (Table 5, 6)
Anterior corneal surface changes that occur in KC would increase the higher order aberrations, especially coma like aberrations due to cone decentration.20,24 Our study approved this hypothesis, as vertical coma in our study showed the highest predictability, either in early KC or FFKC, of all aberrations included.
BCV, which is an important KC screening index provided by Sirius, is obtained by combining data from different aberration coefficients including coma, trefoil and spherical aberrations at both anterior and posterior surfaces. In our study, BCVf, BCVb and their vectorial sum (BCV) showed statistically significant differences between early KC and FFKC cases compared to normal thin corneas, with high AUROC. It showed higher predictability differentiating normal thin corneas from early KC than from FFKC. This was confirmed by the higher values of coma, trefoil and spherical aberrations in early KC than in FFKC, which could be explained by the steeper cornea and higher surface irregularity seen in early KC. Our results agree with
The cutoff values of BCVf, BCVb and BCV were lower in FFKC (0.13, 0.29, 0.3) than in early KC (0.72, 0.63, 0.51) which would provide more precise and higher diagnostic ability of these indices, with excellent predictability (>0.9). Our cutoff values were closer to
In conclusion, differentiating normal thin corneas from subclinical KC and early KC is a real difficulty. This study proved that corneal thickness would be a misleading parameter in such conditions. The location of the thinnest point, elevation indices, particularly in reference to the aspherotoric surfaces, high-order aberrations specifically vertical coma, and KC summary indices provide excellent sensitivity and specificity for predicting either subclinical or early KC. As long as none of the studied indices had an AUROC of 1, and hence complete prediction, we believe that we should rely on a combination of all these indices to reach an accurate diagnosis of subclinical and early KC.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.