
Abstract
Introduction
Granulomatous uveitis is mainly defined by the nature of keratic precipitates and iris nodules. Anterior chamber (AC) granulomas, also known as Berlin nodules (BN), are circumscribed granulomatous nodules that form in the iridocorneal angle (ICA) in response to intraocular inflammation.
Cases description
We present three representative cases of anterior uveitis with berlin nodules to insist on the clinical features of this entity. Case 1: A female adult was referred to our department for bilateral redness and gradual blurry vision. Slit-lamp examination of both eyes (OU) found a yellow-white nodular mass at 6 o’clock on the peripheral iris with irido-crystalline synechiae, vitreous haze and blurred fundus. Purified protein derivative skin test revealed an induration of 20 mm. A diagnosis of presumed ocular tuberculosis was made. The patient received antituberculosis drugs and steroids with good evolution. Case 2: An 11-year-old girl presented for redness and pain OU. Anterior segment examination showed circumciliary congestion, epithelial microcystic edema OU and pearly vascularized lesion against the cornea in the right eye. Fundus examination was unremarkable. A diagnosis of definite ocular sarcoidosis was made based on accessory salivary glands biopsy. The patient was treated with teroids and controlled twice a week. Case 3: A 26-year-old male presented with a redness and pain of the left eye. The slit-lamp examination showed fine keratic precipitates with pearly white nodules within the AC. Fundus examination showed a chorioretinal lesion and occlusive vasculitis. Chest CT was consistent with milliary tuberculosis. Adequate therapy was initiated with favorable outcome
Conclusion
BN can be associated with various ocular manifestations of several diseases. They may be the first manifestation of systemic conditions and seem to be well managed with topical steroids.
Introduction
Anterior Uveitis is the most frequent form of uveitis. 1 The characteristics of keratic precipitates and iris nodules define its granulomatous nature. Koeppe and Busacca nodules are observed around the pupillary area and in the iris stroma, respectively. Anterior chamber (AC) granulomas, also known as Berlin nodules (BN), are circumscribed granulomatous nodules that form in the anterior chamber angle in response to intraocular inflammation. They may be observed in various conditions including malignancies, tuberculosis, and sarcoidosis. 2 Data on BN are scarce. Herein, we report 3 cases of uveitis with a rare presentation of BN to insist on the clinical features of this entity.
Case 1
An 18-year-old female adult was referred to our department with a 1-month history of bilateral redness and gradual blurry vision, self-medicated with topical steroids. Best corrected visual acuity (BCVA) was 20/100 in both eyes. Slit-lamp examination of both eyes found hyperemic conjunctiva, medium-sized inferior corneal precipitates and 1+ cells in the anterior chamber. In the left eye (LE), a yellow-white nodular mass at 6 o’clock on the peripheral iris was noted with irido-crystalline synechiae at 2, 5 and 7 o’clock (Figure 1(A and B)). Gonioscopy showed a yellowish deposit in the iridocorneal angle (ICA). Moreover, the ICA was open with tent-shaped synechiae. In the right eye (RE), we found an iris nodule at 10 o'clock. Intraocular pressure (IOP) was normal in both eyes. A vitreous haze and disc hyperemia were observed in the RE. Fundus examination of the LE was blurred but we could distinguish snowballs with a superior juxta-papillary vascular sheathing. Chest computed tomography (CT) was normal and the purified protein derivative (PPD) skin test revealed an induration of 20 mm. A diagnosis of presumed ocular tuberculosis without systemic involvement was made and the patient received anti TB drugs and systemic steroids. The fundus of both eyes became clear after one week of general medication and BCVA raised to 20/53 and 20/80 respectively in the RE and LE because of uveitic cystoid macular edema confirmed on optical coherence tomography (OCT). The nodules gradually decreased in size to disappear after one month with restitution ad integrum within two months.
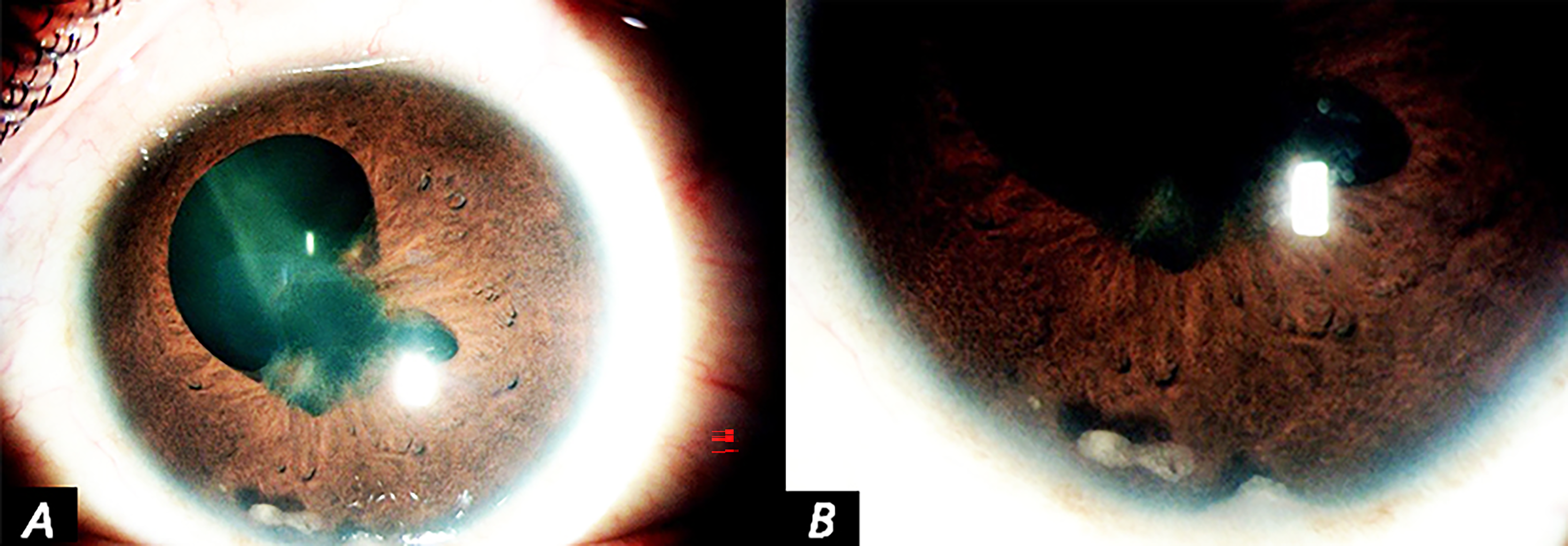
(A,B) Left eye: A yellow-white nodular mass at 6 o’clock on the Irido Corneal Angle, with irido-lens synechiae at 2, 5 and 7 o’clock.
Case 2
An 11-year-old girl presented with a one-month history of redness and pain in both eyes. BCVA was limited to 20/100 in the RE and counting fingers in the LE. Anterior segment examination of the RE showed circumciliary congestion, epithelial microcystic edema, and pearly white vascularized lesion against the cornea that extended over 180° temporally with a hazy appearance of the anterior chamber (Figure 2(A and B)). These findings were well defined by gonioscopy (Figure 2(C)). In the LE, we noted a few endothelial granulomatous precipitates and 2+ cells in the anterior chamber. IOP was 34 mmHg and 25 mmHg respectively in the right and left eyes. Results of fundus examination were unremarkable in both eyes. The general physical exam was otherwise normal. Imaging and laboratory tests including count blood cells, chest (CT) scan, TPHA/VDRL, and tuberculin test were all negative except for serum ACE levels that were elevated. Accessory salivary glands biopsy showed epthelioid granuloma without necrosis. A diagnosis of definite ocular sarcoidosis was made based on clinical and histologic findings. The patient was treated with topical and general steroids and controlled twice a week. At two months follow up, IOP was within normal limits and BCVA was 20/100 in both eyes. The nodules decreased in size but the patient was lost to follow-up.
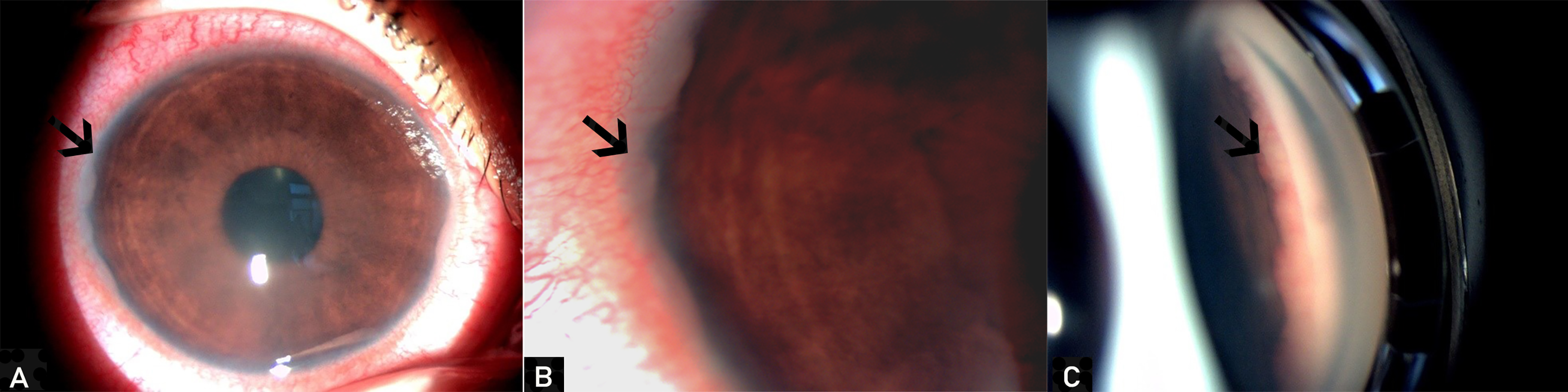
left eye: (A) circumciliary congestion, corneal edema and pearly white vascularized lesion against the temporal cornea that extended over 180° better visualized in (B) . (C) Gonioscopy of the left eye showing Berlin nodules as an extended pearly-white and slightly vascularized closed temporally.
Case 3
A 26-year-old male presented with a 2-week history of redness and pain in the LE. BCVA was 20/20 in the RE and 20/100 in the LE. The slit-lamp examination showed white conjunctiva, fine keratic precipitates with 2+ cells in the AC, broad-based posterior synechiae at 6 o’clock, and three pearly white, nonvascularized, sessile, emerging nodules in the anterior chamber at 4, 6 and 10 O’clock. Gonioscopy showed the angle nodules and revealed peripheral anterior synechiae (Figure 3(A)). Fundus examination showed 1+ vitreous haze, a macular star with a circular white-yellowish lesion of 1 disc diameter, and occlusive vasculitis (Figure 3(B)), better objectified on fluorescein angiography (Figure 3(C)). Examination of the RE was unremarkable. IOP was normal in both eyes. A diagnosis of unilateral acute panuveitis of the LE was made. Anterior Segment Optical coherence tomography (AS-OCT) showed a homogenous hyporeflective lesion covered by a hyperreflective margin at the angle (Figure 3(D)). General examination revealed cervical lymphadenopathy with necrotic ultrasound aspect but blood tests were unremarkable. Chest CT revealed mediastinal lymphadenitis with interstitial pulmonary syndrome, which was consistent with milliary tuberculosis. Antituberculosis quadritherapy, local, and generalsteroid therapy were initiated. The nodular lesions disappeared clinically and on AS-OCT with no anterior chamber reaction within the first month of treatment.
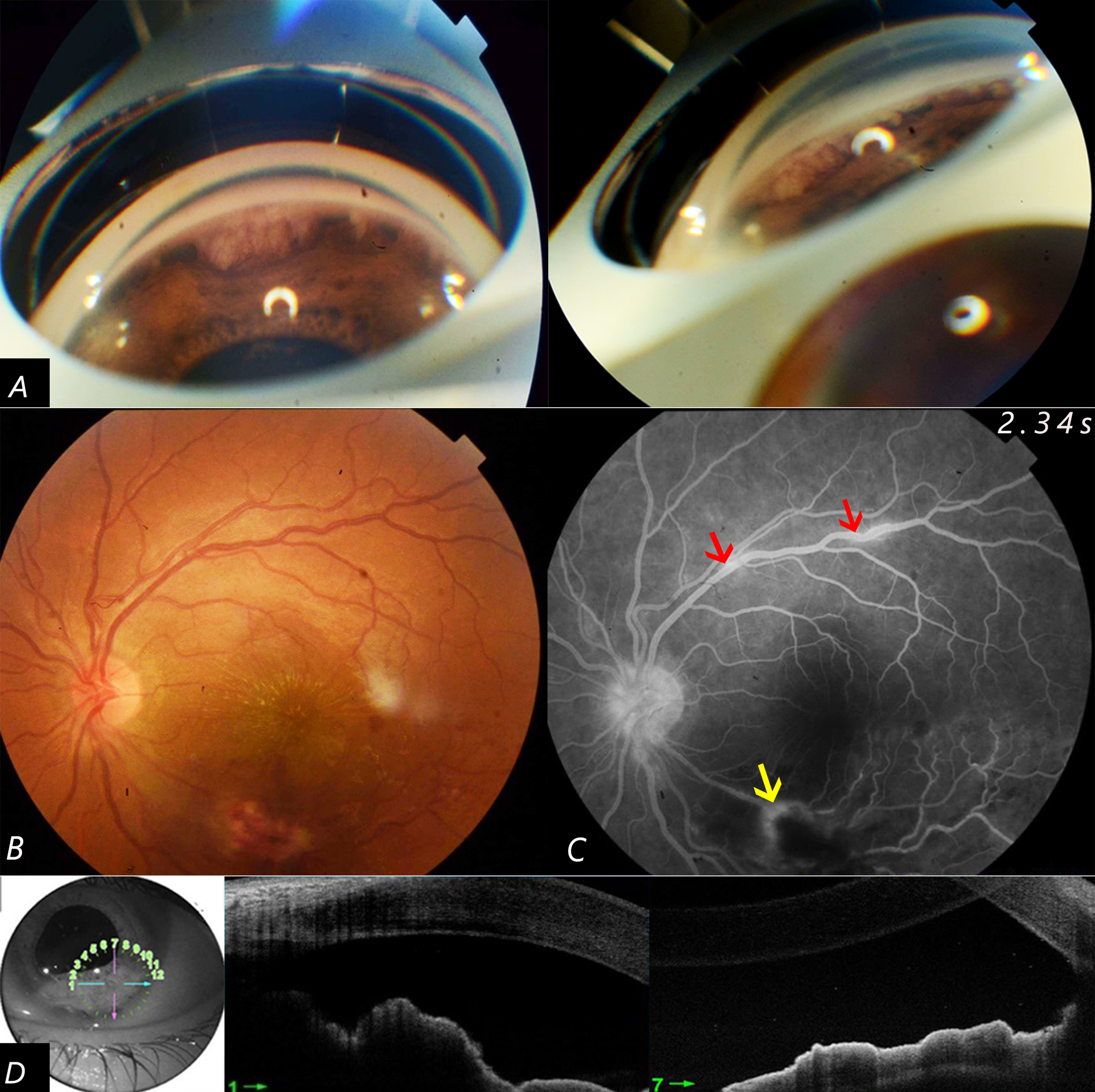
(A) Gonioscopy of the left eye showing pearly white, finely-vascularized, sessile, emerging nodule in the anterior chamber with peripheral anterior synechiae. (B) Fundus of the left eye: Circular white yellowish lesion of 1 disc diameter with occlusive vasculitis and a macular star.(C) Fluorescein Angiography of the left eye: occlusive vasculitis within an infero temporal chorio retinal lesion with superficial retinal hemorrhage (yellow arrow). Supero temporal Perivasculitis with segmental venous sheating (red arrow) (D) Anterior Segment Optical Coherence Tomography of the angle: homogenous hyporeflective lesion surrounded by hyperreflective border.
Discussion
AC granulomas, also known as BN, are inflammatory unilateral or bilateral iris nodules described within the trabeculum of iridocorneal angle (ICA). 3 They are generally pearled, covered by vessels, and mostly associated with anterior synechiae drawing a « tent pattern » in the ICA. 3 In our patients, anterior synechiae with IC angle nodules were easily individualized in gonioscopy. Gonioscopy is essential to assess the nodule aspect, and volume and to report associated lesions such as angle-closure due to synechia. To better appreciate the extent and localization of these nodules, imaging of structural details of the anterior ocular segment using Ultrasound Biomicroscopy (UBM) has been described. 4 UBM showed homogenous hyperreflective lesions with an occluded angle due to peripheral anterior synechia. We performed an AS-OCT instead of UBM as it also enables qualitative assessment of the anterior segment structures. It helped identify nodules and follow their evolution, thereby facilitated the diagnosis and management of the iris nodules in the third case.
Histologically, the components of the granuloma would depend on the main associated etiology. Biopsy of the lesion shows a non-caseating epithelioid cell granuloma or epithelioid cells with caseation necrosis respectively in cases of sarcoidosis and tuberculosis. 2 If practiced, Ziehl–Neelsen stain would objective tubercular acid-fast bacilli if mycobacterium tuberculosis is the causative agent. 5 BN aren’t isolated and are generally associated with anterior uveitis. They are usually a clinical feature of sarcoidosis as a main diagnosis. 3 Nearly two-thirds of patients with sarcoidosis present bilateral granulomatous uveitis. BN are considered by the International Workshop on Ocular Sarcoidosis as a suggestive manifestation of the pathology although they are not frequently described. 3 Saricaouglu et al reported that iris nodules have been associated with severe anterior uveitis with important corneal changes in contrast to anterior segment findings in our three cases. 6 That may be due to prior prescription of topical steroid drops and corneal edema related to elevated IOP that prevented the visualization of anterior chamber details, in the first and second patient respectively. Infectious etiologies such as syphilis, tuberculosis, and parasitosis should be as well considered. 2 The diagnosis of tuberculosis must be considered when BN are detected. It is often presumptive and the treatment should be attempted based on clinical, imaging, and laboratory findings. 7 In our cases, the diagnosis was made based only on the PPD test and Tubercular Posterior Uveitis associated with the miliary aspect on the chest CT scan. PPD test has low sensitivity and specificity since the large coverage rate of tuberculosis vaccination. 8 A skin reaction under 10 mm is usually correlated to previous immunization status but its sensitivity increases with a history of exposure. 6 In our first patient, the significant positive induration of 20 mm allowed a diagnosis of presumed tuberculosis to be made. Interferon-Gamma Release Asays (IGRA) test (QuantiFERON test) is more sensitive and specific for the diagnosis of latent tuberculosis as it is not affected by prior BCG vaccine. 9 However, it is relatively expensive with a risk of false-positive results after a tuberculin skin test which prevented its realization in our patient. The presence of angle granuloma has been also associated with malignant etiology. Pseudo uveitis must be considered as a differential diagnosis of iris nodules. In fact, inflammatory granulomas are often vascularized and should be differentiated from tumoral nodules or metastatic lesions such as lymphomas, leukemias or other malignancies. 2 None of our patients reported anorexia, asthenia, a sudden weight loss, or suffered from another complaint that might have raised the diagnosis of malignancies. In the second case, the necrotic aspect of the cervical lymph node on the ultrasound scan without any other general manifestation suggested an infection related to Mycobacteria Tuberculosis at the first line. Increased IOP is commonly associated with BN. In fact, nodules may obstruct Schlemm's canal resulting in IOP elevation and secondary glaucoma. 10 In the second case, higher IOP was observed in the LE. It would be related to trabecular nodules in addition to the inflammatory cascade that leads to trabeculitis and synechiae in sarcoid uveitis. 2 Ocular hypertension was well managed by hypotensive drugs and returned to normal limits after the disappearance of angle nodules
The treatment of the nodules is mainly medical. It is based on topical and general steroids associated with anti-infectious drugs in case of infectious etiology. Surgical granuloma excision was suggested in the literature. It may lead to a more rapid resolution of inflammation compared to conservative treatment. 4 In our patients, the medical approach was first attempted as the context and etiology were different. There was no need for surgical intervention given the favorable outcome under topical dexamethasone drops.
Conclusion
BN can be associated with various ocular manifestations of several diseases. They can be an isolated manifestation or the first clinical sign of a systemic condition that requires general treatment. Sarcoidosis and tuberculosis should be considered in the context of ICA granuloma even in the absence of associated severe anterior chamber inflammation or granulomatous precipitates. Topical steroids seem to be an effective mean to manage BN.
Footnotes
Acknowledgments
The author(s) declare that there is no conflict of interest. All the authors participated either in the follow-up of the patients or in the drafting and the revision of the article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
A written informed consent form was obtained from the patients and from the legal guardian of the minor patient to publish their data and images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.