
Abstract
Purpose
To describe a rare presentation of torpedo maculopathy (TM).
Case description
A 25-year-old male was examined in the retina clinic for a macular scar in the left eye. His visual acuity was 20/20, N6 in both eyes and no past history of ocular trauma or any medical or ocular history. The anterior segment was quiet and intraocular pressure was normal.
Results
The patient's left eye on 78D slit lamp biomicroscopy revealed a flat, diffusely hyperpigmented fusiform torpedo-like lesion with sharp margins and surrounding hypopigmentation located predominantly temporal to the fovea, with its tip pointing towards it and just crossing the vertical foveal midline. Dilated fundus examination with binocular indirect ophthalmoscopy revealed no peripheral chorioretinal lesions or vitritis in both eyes. OCT scan through the lesion revealed gross damage to the outer retinal layers, as well as thickening of the retinal pigment epithelium and underlying shadowing, as well as a hyporeflective subretinal cleft involving the lesion. OCT also revealed outer retinal layer damage with an intact retinal pigment epithelium through the lesion's hypopigmented margins. Fundus autofluorescence image revealed a globally hypoautofluorescent lesion in the left eye, with surrounding patchy hyperautofluoroscent areas. Based on the patient history, clinical and imaging findings, other differential diagnoses such as atypical congenital hypertrophy of retinal pigment epithelium (RPE), choroidal nevus, RPE hamartoma, trauma and inflammatory conditions were ruled out. The diagnosis of TM was confirmed based on the typical lesion shape and location.
Conclusion
A torpedo lesion with diffuse hyperpigmentation is an unusually rare presentation.
Introduction
In 1992, Roseman and Gass were the first to describe a case of torpedo maculopathy (TM) in a 12-year-old boy, while Daily coined the term “torpedo maculopathy” to describe the characteristic torpedo-like tip that points towards the fovea.1,2 Cases of TM that have been traditionally reported in the literature have certain consistent features such as temporal location to the fovea, horizontally ovoid shape, hypopigmentation, and usually no visual symptoms.3,4 However, there have been reports of TM with variable features such as intraretinal cavitation, hyperpigmentation, fundus excavation, scotoma and choroidal neovascular membrane.5–7 Additionally, there have been reports of TM with various multimodal imaging findings, including adaptive optics.5,6,8,9 According to Golchet et al., pigmentation can be variable, with some lesions exhibiting significant hyperpigmentation within the hypopigmented lesion. 10 A globally hyperpigmented TM lesion has been reported infrequently in the literature.11,12
We present a rare case of a diffusely hyperpigmented torpedo-shaped lesion, illustrate the imaging findings with multimodal techniques, and discuss the common differential diagnosis commonly associated with this entity in this report.
Case description
A 25-year-old male was seen by a general ophthalmologist for routine eye examination. The patient was later referred to a retina specialist with a diagnosis of macular scar in the patient's left eye. His visual acuity was 20/20, N6 in both eyes with a refraction of −4.50DS in the right eye and −3.50DS/−1.00DC×170° in the left eye respectively. There was no significant past history of ocular trauma or any medical or ocular history, including infectious diseases or long-term exposure to retinotoxic substances. The anterior segment was quiet and unremarkable upon examination. The Goldman applanation tonometry result was 16 mmHg in both eyes. In the left eye, 78D slit lamp biomicroscopy revealed a flat globally hyperpigmented fusiform lesion with sharp margins and surrounding hypopigmentation. It was predominantly temporal to the fovea, with its tip pointing at it and just crossing the vertical foveal midline (Figure 1A). Dilated fundus examination with binocular indirect ophthalmoscopy revealed no peripheral chorioretinal lesions or vitritis in both eyes. Examination of the right eye was unremarkable. The Spectralis OCT device (Heidelberg Engineering, Germany) was used to perform optical coherence tomography (OCT) through the lesion. OCT revealed gross damage to the outer retinal layers, as well as thickening of the retinal pigment epithelium and underlying shadowing, as well as a hyporeflective subretinal cleft involving the lesion (Figure 1B). OCT also revealed outer retinal layer damage with an intact retinal pigment epithelium through the torpedo lesion's hypopigmented margins (Figure 1C). The fundus autofluorescence image revealed a globally hypoautofluorescent torpedo-like lesion in the left eye, with surrounding patchy hyperautofluoroscent areas (Figure 1D). The right eye showed normal fundus autofluorescence (Figure 1E).
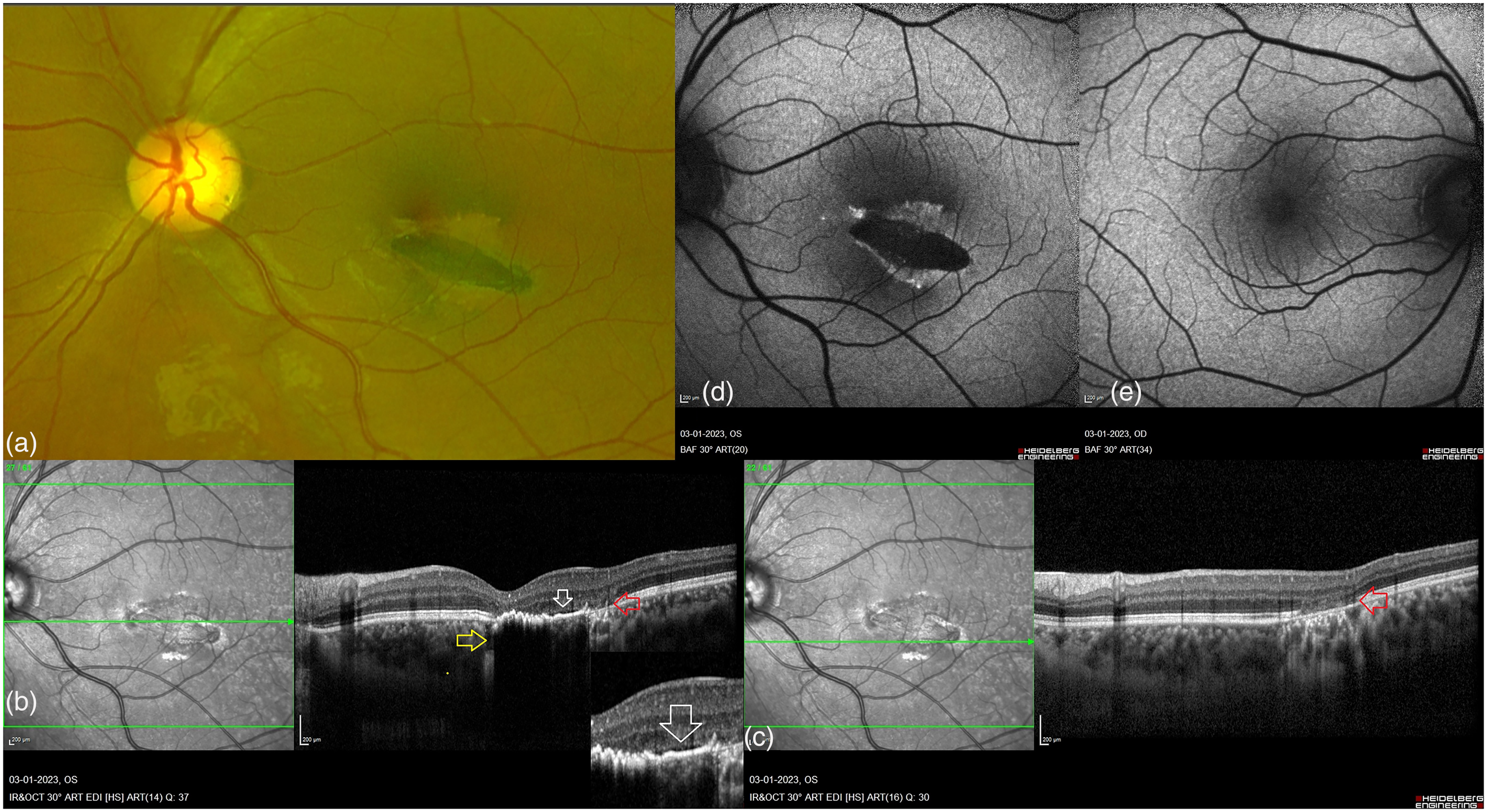
Imaging findings in a case of hyperpigmented torpedo maculopathy. (a): Cropped Optos® image (Optos, Daytona, UK) of the left eye shows a flat diffusely pigmented horizontally ovoid fusiform lesion on the temporal side of the fovea, with sharp margins and surrounding hypopigmentation, just crossing the vertical foveal midline. (b and c): A spectral domain optical coherence tomography (OCT) scan through the torpedo lesion revealed damage to the outer retinal layers (red arrow), thickening of the retinal pigment epithelium and underlying shadowing (yellow arrow), and a hyporeflective subretinal cleft (white arrow and zoomed inset image). An OCT scan of the hypopigmented margins of the torpedo lesion revealed outer retinal layer damage with intact retinal pigment epithelium (red arrow). (d and e): Autofluorescence image of the left eye fundus revealed a globally hypoautofluorescent torpedo-like lesion surrounded by patchy hyperautofluoroscent areas. The fundus autofluorescence in the right eye was normal.
Discussion
Based on clinical characteristics such as shape, location, unilaterality, and absence of visual symptoms, as well as OCT findings such as thinning of the outer retinal layers, uninvolved inner retinal layer structure, and subretinal cleft, this is a true TM lesion.
The appearance of this lesion raised the possibility of other diagnoses such as atypical congenital hypertrophy of retinal pigment epithelium (CHRPE), choroidal nevus, retinal pigment epithelial hamartoma, traumatic maculopathy, choroidal rupture, healed choroidal neovascular membrane and inflammatory conditions (toxoplasmosis). Based on the appearance of the lesion, the closest differential diagnosis was atypical CHRPE. Atypical CHRPE lesions are typically multiple and smaller in size than typical CHRPE lesions, which are generally solitary and round. They are usually bilateral and are linked to familial adenomatous polyposis. 13 Clinically, they appear as haphazardly distributed oval, spindle, comma, or fishtail-shaped lesions across the fundus. Depigmented lacunae can also be found in atypical lesions. The lesion in our case lacked hypopigmented lacunae and displayed characteristics more typical of TM. Furthermore, based on the patient history, clinical and OCT findings, the remaining differential diagnoses were ruled out.
A typical TM lesion is a localized congenital abnormality of RPE hypopigmentation which leads to outer retinal and inner choroidal degeneration and an uninvolved inner retinal layers.4,14 In our case, the torpedo lesion's global hyperpigmentation was unusual. A literature search revealed only two other cases with similar appearing fundus lesions that have been reported to date.11,12 The case presented by Rohl and Vanace demonstrated a hyperpigmented torpedo lesion with pseudo lacunae that progressed over a 5-year period, whereas the case presented by Ranjith and Giridhar demonstrated a hyperpigmented torpedo lesion without lacunae. The clinical and imaging findings in our case were comparable to that reported by Ranjith and Giridhar expect for the nasal tip of the lesion just crossing the vertical foveal midline.
This unique case describes a rare presentation of TM well supported by multimodal imaging features.
Footnotes
Authors’ contributions
RV, JC – conceptualising the study, data acquisition, analysing the data, statistics and results, interpreting the findings, writing & reviewing the manuscript
SP, RB, AH – Data acquisition and analysing the data
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.