
Abstract
Purpose
To compare the magnitude and duration of intraocular pressure (IOP) increase during the two principal Islamic prayer positions, Rukū (standing while bowing forward at a 90-degree angle), and Sujud (kneeling with the forehead touching the ground) in healthy subjects and patients with primary open-angle glaucoma (POAG).
Methods
Prospective, observational case series. Ninety-five eyes of 47 patients (27 with POAG and 68 without POAG) were included. Eligible candidates underwent IOP measurements in the sitting position and in two prayer positions using the Goldmann applanation tonometer and the Icare-Pro tonometer. IOP was measured at set intervals until it returned to baseline.
Results
Mean IOP increased from a sitting baseline value of 16.1 ± 2.9 mmHg (8.6-26) to 19.3 ± 4.2 mmHg (10.2-32.3) following 30 s of Rukū (p ≤ 0.0001) and from 16.1 ± 0.4 mmHg to 22.2 ± 3.1 mmHg (14.9-37) following Sujud (p ≤ 0.0001). IOP increased similarly in the POAG and non-POAG groups in both positions. Twenty-six eyes (27%) failed to normalize within 2mmHg of baseline, but all returned to baseline after another five minutes.
Conclusions
Performing traditional Muslim prayer positions increases IOP significantly. The increase did not resolve immediately in approximately a quarter of individuals. These findings may have a considerable impact on Muslim patients with glaucoma.
Introduction
Islam is the fastest-growing religion in the world. As of today, there are approximately 1.9 billion Muslims worldwide, making it the second largest religion in the world after Christianity. 1 The global prevalence of primary open-angle glaucoma (POAG) is estimated at 2.4% (95% CI 2.0 ∼ 2.8%), 2 which indicates that there are currently over 45 million Muslims with this diagnosis.
Glaucoma is the leading cause of preventable irreversible blindness in the world. 3 Body posture has a significant impact on intraocular pressure (IOP), the only modifiable risk-factor for disease progression.4,5 The mechanisms by which IOP changes in response to body position are not fully understood. Several studies have demonstrated that head-down postures can increase IOP considerably, attributed to elevated episcleral venous pressure (EVP). Alternatively, choroidal vascular engorgement caused by redistribution of body fluids may also contribute to this phenomenon.6–8
As part of Islamic prayer, Muslims kneel, prostrate, and perform head-down positions. The total amount of time spent in prayer positions throughout the day is estimated to be approximately 10 min. During these positions, IOP is likely to fluctuate greatly, potentially causing further damage to the optic nerve of patients with glaucoma. However, to our knowledge, no information exists concerning the impact of postural changes on the IOP caused by performing Muslim prayer positions.
This study was designed to examine the changes in IOP in healthy patients during the two principal Islamic prayer positions, the Rukū (bowing at a 90-degree angle, hands on knees, and feet shoulder-width apart) for 30 s and Sujud (kneeling and bowing, with the forehead touching the ground), and to compare the results with those of patients with POAG.
Material and methods
This prospective observational study was conducted according to the Declaration of Helsinki, following the approval of the Human Research Committee and in compliance with all applicable regulations regarding good clinical practice. Recruitment was conducted at a single investigational site (Meir Medical Center, Kfar Saba, Israel). Following an explanation of the nature and purpose of the study, written informed consent was obtained from each participant.
Eligible candidates were over 18 and physically able to perform the Rukū and Sujud positions. For the group with POAG, the diagnosis was made based on the presence of typical optic-disc damage and glaucomatous visual field defects detected by standard automated perimetry (Humphrey Field Analyzer, Zeiss, Dublin). Exclusion criteria were any previous IOP lowering procedures (excluding laser trabeculoplasty) or cataract surgery undertaken within the last three months, ocular pathologies other than glaucoma and any corneal abnormalities. Additional exclusion criteria were clinically significant systemic illnesses and conditions that may affect EVP, including superior vena cava syndrome, pregnancy, thyroid eye disease and orbital masses.
Eligible patients were located through a review of medical records. The participants were all Arab adults familiar with Islamic prayer.
The Icare-Pro tonometer (Icare, Tiolat Oy, Helsinki, Finland) was used to measure IOP in both sitting and praying positions, following a baseline IOP measurement performed using the Goldmann applanation tonometer (GAT). A topical anesthetic (Oxybuprocaine hydrochloride 0.4%) was instilled into both eyes prior to the measurements. IOPs were first measured while the patients were seated. Next, participants were asked to perform the Rukū position (Figure 1) for 30 s and then the IOP was measured from this position. Following this, subjects were instructed to sit for five minutes and then to perform Sujud for 30 s, and the IOP was recorded while they were in this position. The final IOP measurement was again recorded in the sitting position, immediately after completion of the Sujud. In the event that this second sitting IOP measurement was not equal to the first (within a range of 2 mmHg), a 5-min follow up measurement was performed in which the participant remained seated.
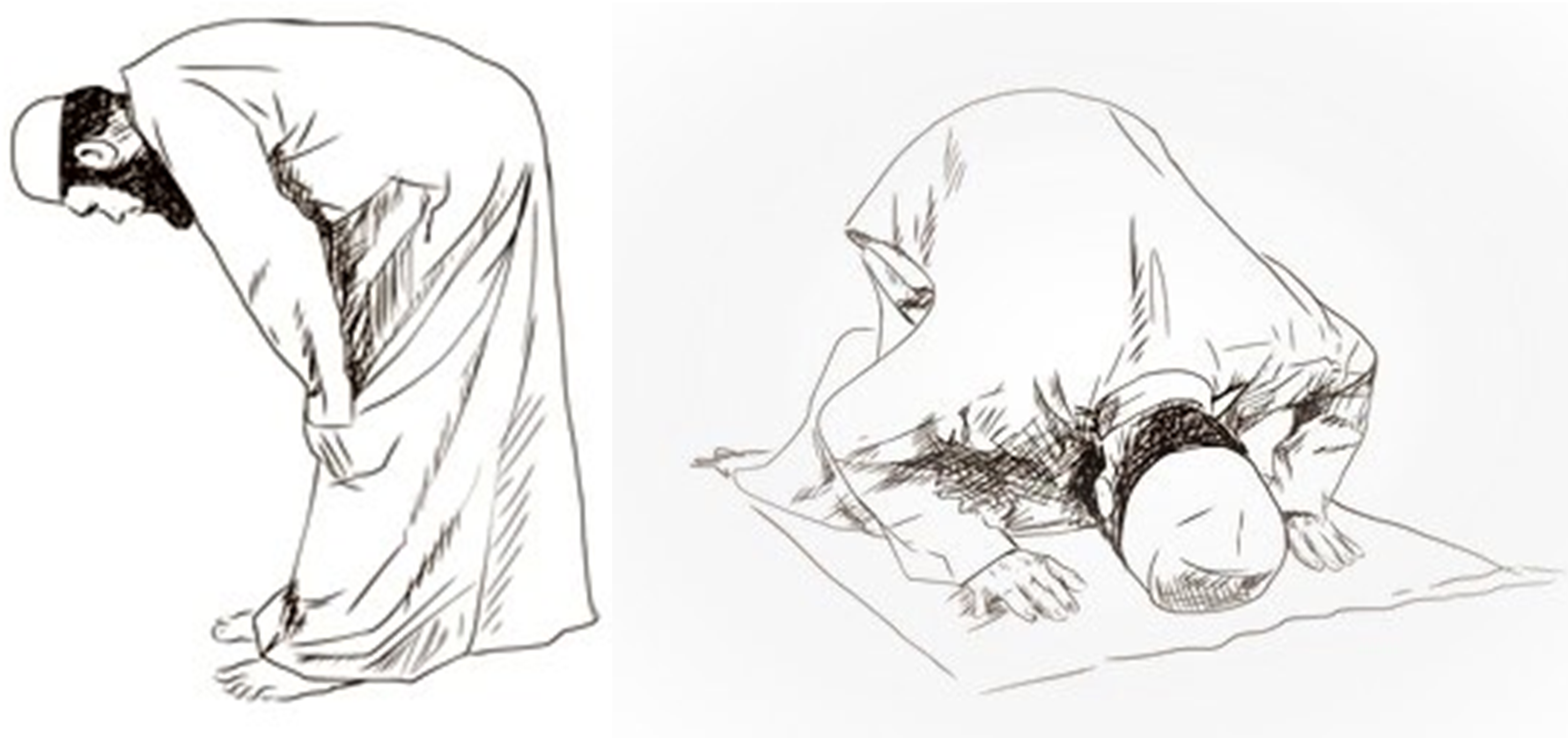
The “Rukū” and “Sujud” praying positions.
A single investigator who was knowledgeable in the correct technique for performing the praying positions conducted all measurements. If both eyes were to be studied, the right eye pressure was first measured. Each measurement involved the participant's head rotated 45 degrees in the direction of the eye being measured. The IOP was measured five times in each eye and the average score was recorded.
Statistical analysis
Data were recorded on an Excel spreadsheet (Excel 15.0, Microsoft Inc., Richmond, WA, USA) and analyzed with Graphpad prism 9 (GraphPad Software, La Jolla California USA). A χ2 test was used for categorical variables. Clinical parameter distributions were tested for normality with the Shapiro–Wilk. Independent and paired t tests were conducted for continuous variables with a normal distribution and Wilcoxon signed–rank test for variables with a non-normal distribution. A Cox stepwise regression survival analysis was conducted to determine the effects of the covariates on the IOP rise. Results are expressed as mean ± SD (median, range) and N (%). The mean differences between preoperative and postoperative values in same groups were compared by paired t test and the two-way ANOVA. A P. value of <0.05 was considered as statistically significant.
Results
Ninety-five eyes of 47 consecutive patients (27 eyes with POAG and 68 eyes without) were enrolled in the study. Demographic and clinical characteristics of the study participants are summarized in Table 1. Mean IOPs before and after the prayer positions for all study participants are outlined in Table 2. Mean IOP increased by 3.2 mmHg from a sitting baseline value of 16.1 ± 2.9 mmHg (8.6-26) to 19.3 ± 4.2 mmHg (10.2-32.3) following 30 s in the Rukū position, representing a 20% increase (p < 0.0001). An increase of 6.1 mmHg (37.1%) was observed between the sitting and the Sujud positions, from 16.1 ± 0.4 mmHg (8.6-26) to 22.2 ± 3.1 mmHg (14.9-37) (p < 0.0001). Three and fifteen patients (3% and 16%) had IOPs greater than 27 mmHg following the Rukū and Sujud positions, respectively. The mean IOP increase between the healthy subjects and the patients with glaucoma was the same as well as the percentage of patients with higher than 27 mmHg IOP after those two praying positions.
Demographics and clinical characteristics of study participants.
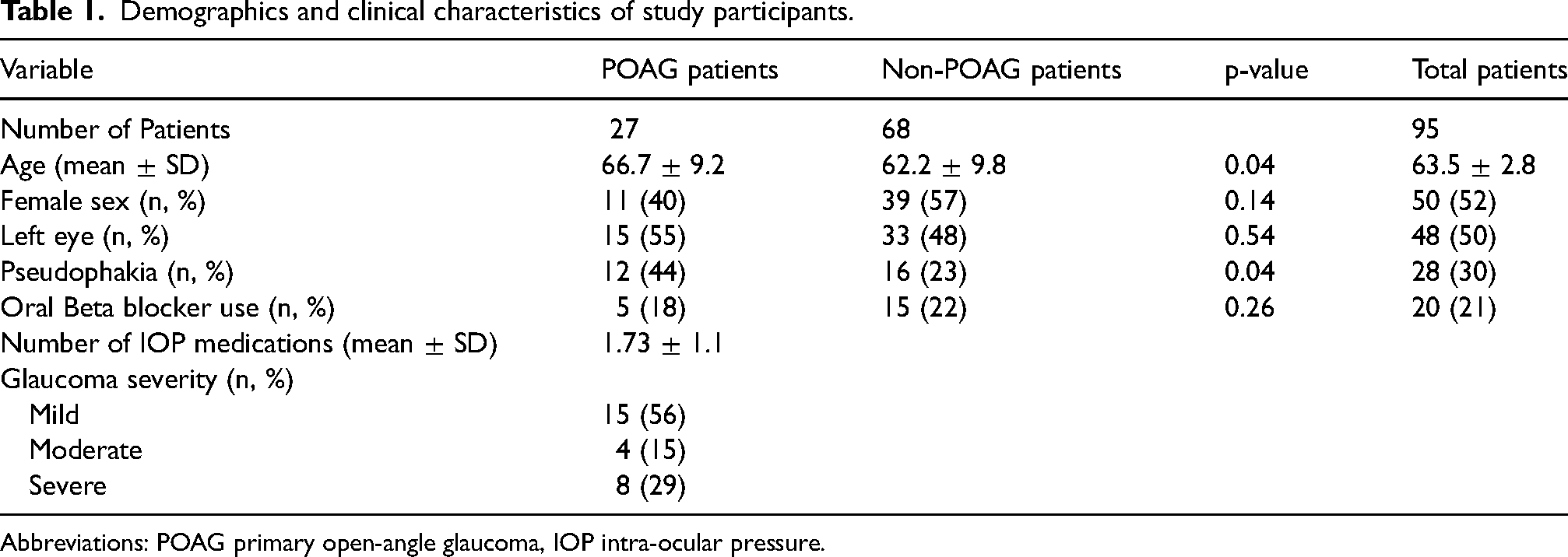
Abbreviations: POAG primary open-angle glaucoma, IOP intra-ocular pressure.
Mean IOP after sitting and prayer positions and the difference between participants with or without POAG, measured with Icare.
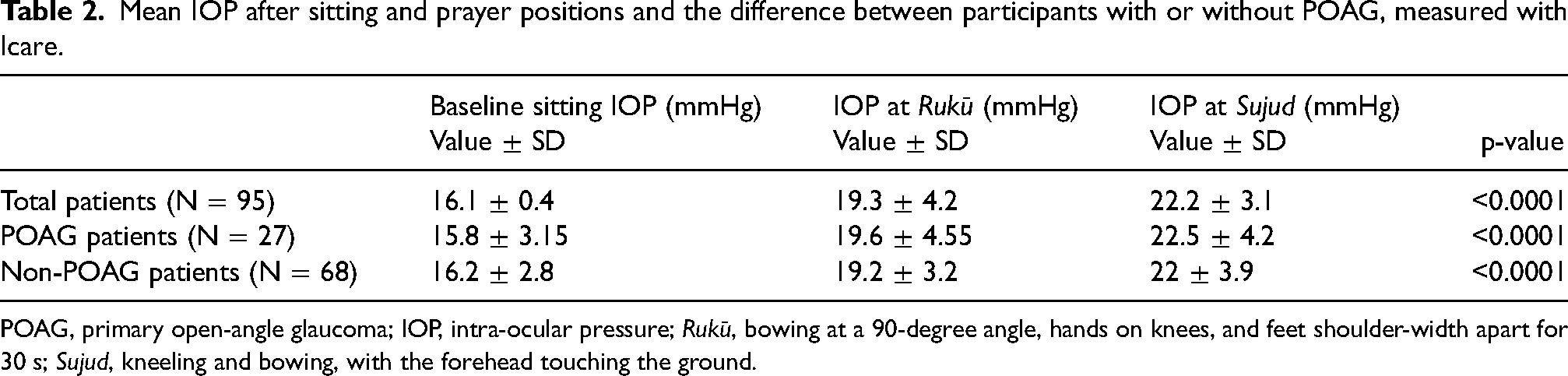
POAG, primary open-angle glaucoma; IOP, intra-ocular pressure; Rukū, bowing at a 90-degree angle, hands on knees, and feet shoulder-width apart for 30 s; Sujud, kneeling and bowing, with the forehead touching the ground.
Immediately after the IOP was measured in the Sujud position it was reassessed in the sitting position. If this second sitting measurement did not match the first baseline measurement (within a range of 2 mmHg), an additional 5-min follow-up measurement was made. Twenty-six patients (27.3%) required additional measurements due to this reason, 3 (11%) of which were POAG patients. IOPs returned to baseline values or lower in all twenty-six eyes at the first 5-min follow-up, and none required additional measurements. Cox stepwise regression survival analysis did demonstrate any correlation between the severity of the disease or the number of IOP lowering medications and the magnitude or duration of IOP increase during the two principal Islamic prayer positions.
Figure 2 illustrates the overall range and median IOPs, the first and third quartiles for the baseline sitting IOP measured using GAT and for the sitting and prayer positions. The median sitting IOP recorded by the Icare slightly exceeded that recorded by the GAT, as reported in other studies.9–11
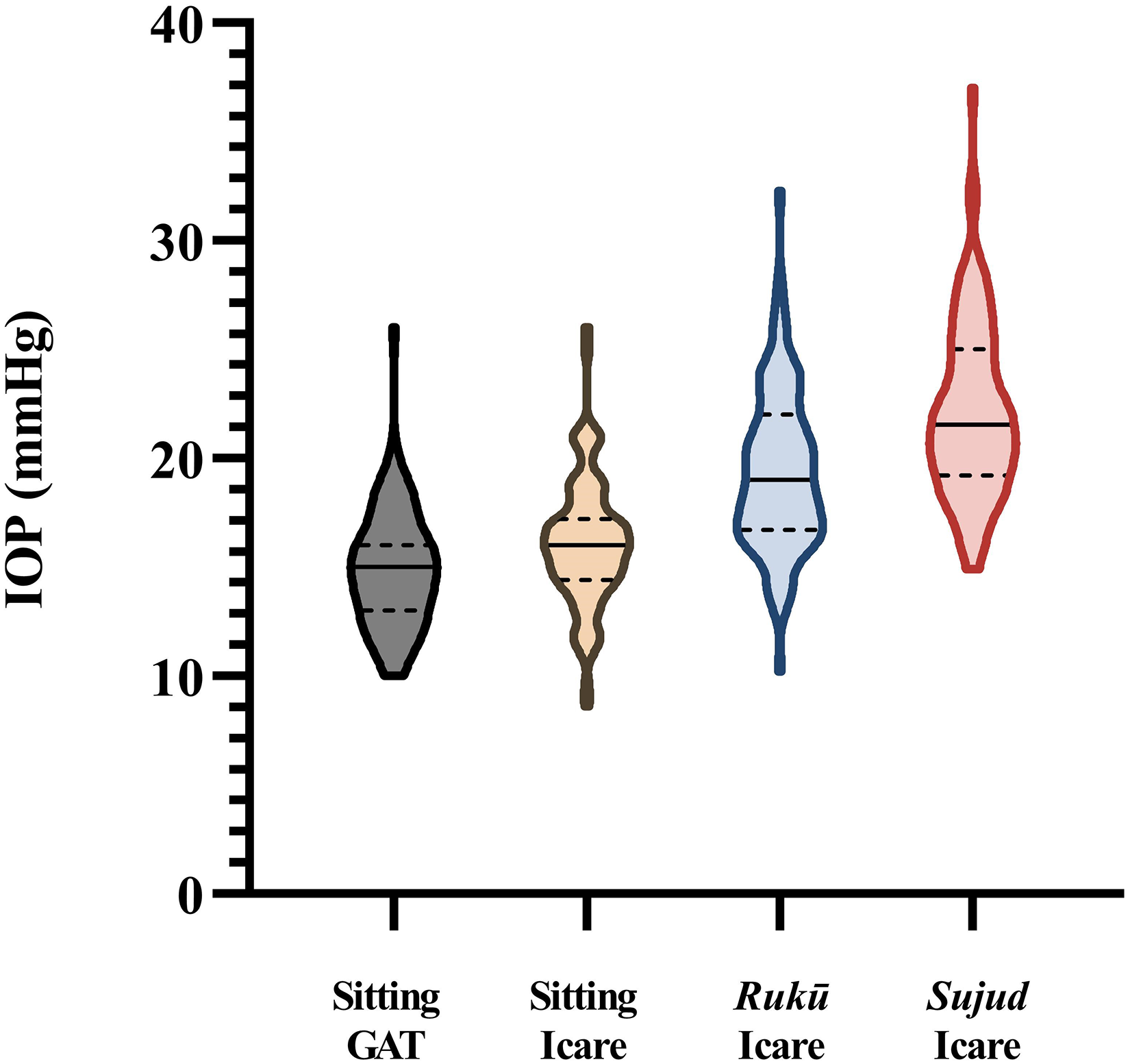
Comparison of sitting IOPs at rest using Goldmann applanation tonometer (GAT) and Icare, after performing 30 s at “Rukū” posture and after performing 30 s at “Sujud” posture. Solid line = median, dashed lines = 1st quartile and 3rd quartile.
Figure 3 depicts IOPs measured in the Sujud and sitting positions for the POAG and non-POAG patients. Notably, IOP increased in all eyes except one after moving to the Sujud position.
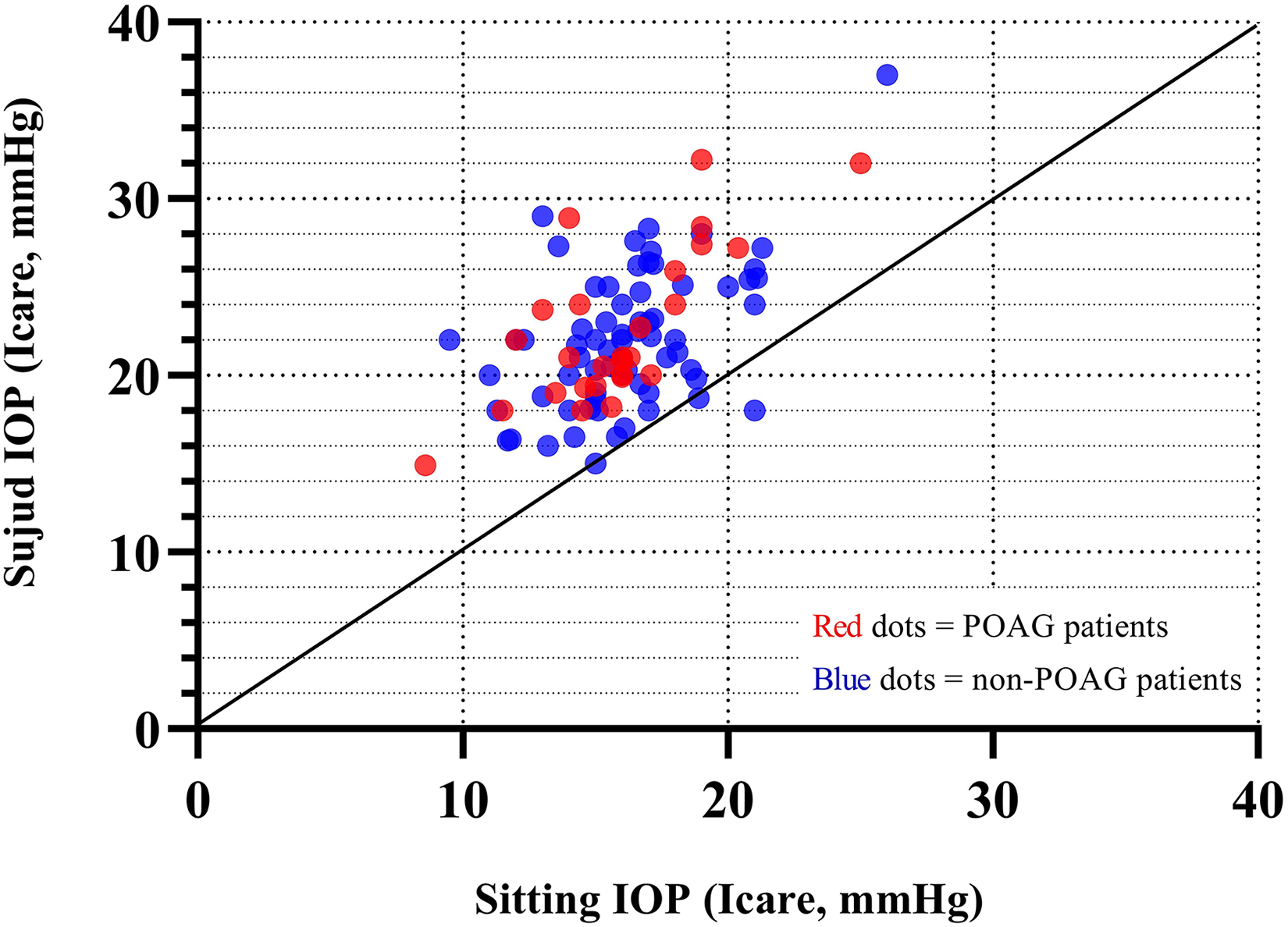
Correlation between measurements of IOP in the sitting and the “Sujud” postures.
Discussion
One quarter of the world's population adheres to Islam; the second largest religion in the world. In the Muslim faith, there are five daily prayer sessions that include a variety of body postures. As far as we are aware, no previous study has described changes in IOP among Muslims who perform these prayers.
The effects of different recumbent and head positions on IOP are well-established.12–14 Yoga positions are known to increase IOP, some of which resemble Muslim prayer postures.15,16 Case reports have described deterioration in glaucoma and acute angle closure attacks among yoga practitioners.17,18 Baskaran et al. 19 reported a 2-fold increase in IOP in 75 young patients in a headstand position.
One of the proposed mechanisms of increased IOP during a body position change is elevated EVP.20,21 Arora et al. 22 investigated the effects of different body postures on IOP and EVP and concluded that both are higher in the inclined position than in the sitting position.
The results of this study indicate that Muslim prayer positions lead to significant increases in IOP. This finding may have important implications for people diagnosed with glaucoma who perform daily Muslim prayers, during which time the IOP can increase by 30-40%, as found in the present study. A Muslim glaucoma patient who performs 5 daily ten-minute prayer sessions is subjected to over 60 h of elevated IOP over the course of a year. Additionally, we found that in slightly more than 25% of patients, the effects of the increase in IOP do not disappear immediately after completing the prayer pose. Interestingly, and contrary to our expectations, we did not find a higher proportion of glaucoma patients whose pressure did not normalize immediately after the pose. This intriguing finding may be explained by the relatively higher percentage of phakic individuals in the non-glaucoma group. In addition, the small number of glaucoma patients in the current study precludes definitive conclusions regarding this issue.
This study has several limitations. The IOP measurements were taken at different times throughout the day and important data such as central corneal thickness and the maximal IOP was not available. Moreover, there was also a heterogeneity in the severity of the disease among the glaucoma patients in the study”
In summary, IOP is significantly increased during traditional Muslim prayer positions, especially when kneeling with the forehead touching the ground. The lifelong exposure to this activity can put patients at risk of disease progression. Special care should be taken regarding recommendations, especially in those with advanced disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.