
Abstract
Purpose
This study aimed to assess the possible effect of environmental factors and eating habits on patients with the exfoliation syndrome (XFS) and exfoliative glaucoma (XFG) in a Turkish population.
Methods
A questionnaire was applied to 1,000 individuals, including 290 patients with XFS, 210 patients with XFG, and 500 age- and sex-matched healthy control participants. Sociodemographic characteristics, home type and warming methods, living and working conditions (indoor–outdoor), dietary habits based on the the guidance of Turkey Dietary Guidelines, (Determination of Nutritional Status Report and Turkey National Nutrition and Health Survey) and using sunglasses were evaluated. The chi-square test, Student t test, and analysis of variance were used for the statistical analysis with SPSS v. 23.0 software.
Results
The case–control groups were matched during data collection, and age and sex distribution in groups was analyzed; however, no difference was found. The average years and hours spent outdoor were statistically different between case and control groups (P < 0.05). The disease risk among individuals wearing sunglasses was 2.74 times less than that among those who did not wear sunglasses. Individuals born in the city had 1.46 times lower risk. Also, living out of the city until the age of 12 years increased the risk of getting the disease 1.36 times. In addition, while living in an apartment decreased the risk of disease, using a stove increased. The control groups had more healthy eating habits than the case groups.
Conclusion
This case–control study showed that time spent outdoors, wearing sunglasses, home type, heating method, and eating habits might be associated with XFS and XFG.
Keywords
Introduction
Exfoliation syndrome (XFS) is the most common cause of secondary open-angle glaucoma, which presents with the accumulation of fibrillar extracellular matrix elements on various ocular tissues. 1 XFS can cause lens subluxation, angle-closure glaucoma, phacodonesis, and blood aqueous barrier breakdown, as well as severe, chronic open-angle glaucoma. It increases susceptibility to serious complications such as zonular dialysis, vitreous loss, early diffuse corneal endothelial decompensation, and rupture of the posterior capsule during cataract surgery. 2 This syndrome not only affects ocular tissues but also has been reported in association with vascular dysfunction, cerebral infarction, renal artery stenosis, neurosensory hearing loss, systemic hypertension, acute myocardial infarction, angina, stroke, and carotid stiffness.3–6 Therefore, the belief that XFS is an important systemic disease has been emphasized in recent years.
The involvement of genetic factors, such as lysyl oxidase-like1 (LOXL1) gene variants, has recently been stressed in the development of XFS. In a study of the Icelandic population, 99% of patients were found to be carrying the risk allele, while the rate was 85% in the control group. 7 This showed that LOXL1 risk alleles increased the risk but not necessarily led to the formation of the disease. LOXL1 variant ratios were found to be similar in the patient and control groups in areas with and without high disease prevalence, for example, in Finland and Australian populations. These findings suggested that other genetic causes or environmental factors might affect the etiology of XFS.8–11
Kang et al. reported in a large prospective study of individuals aged 20 + years in two US-based cohorts that living in the middle or southern tiers at the age of 15 years was most strongly associated with the risk of XFG and XFG suspect, but residence at birth and at age 25/30 was not independently associated . This prospective study showed that environmental and climatic factors played a role in the development of this disease. 10 Regarding environmental factors, the relationship between exposure to sunlight in particular and XFS has been researched.8,11–14 In an in vitro study of human Tenon capsule fibroblasts exposed to ultraviolet radiation (UVR), the basic elements of exfoliation material (elastin, fibulin, fibrillin-1, and LOXL1 components) were shown to be increased. 15 An increase in the number of sunny days per year increased the risk of XFS or exfoliation glaucoma (XFG) by 1.5%; 11 also, the time spent outdoors from 10 a.m. to 4 p.m. during summer was found to increase the risk of XFS by 4%. 13 Wearing sunglasses was reported to be associated with the reduction of the risk. 13 Contrary to these studies, some others suggested that the time spent outdoors, exposure to high solar radiation, and the behaviour of wearing sunglasses were not related to XFS.8,9
The food consumption of patients with XFS/XFG is thought to be another factor impacting the disease. Heavy coffee consumption, ≥ 3 cups of coffee per day, was related to an increased risk of XFS/XFG. 16 The intake of vitamin B6 and vitamin B12 has not been found to be associated with the disease, but supplemental folate intake, not dietary, has been reported as a risk-reducing factor. 17
XFS is a common disease in a Turkish population. Its incidence was reported to be 16.4% among patients scheduled for cataract surgery in a study. 5 Despite the high frequency of XFS in a Turkish population, information on the association between environmental factors and XFS/XFG is insufficient. Therefore, this study aimed to investigate the role of environmental factors and eating habits in the development of XFS and XFG in a Turkish population.
Methods
This case–control epidemiological study was carried out in Department of Ophthalmology in Hacettepe University Medical School. This medical department is a reference clinic where patients from many different regions of Turkey visit. The application of the questionnaire and the collection of data continued between March 2016 and January 2021. The tenets of the Declaration of Helsinki were observed throughout the study. Written consent forms were obtained from all patients, and the study was approved by the Institutional Review Board (Hacettepe University Noninvasive Clinical Research Ethics Committee, GO16 /51-35.).
A total of 1,000 people (290 patients with XFS, 210 patients with XFG were in the case group and 500 patients who applied same clinic with other reasons except XFS and XFG were in the control group, case and control groups matched by gender and age), who visited the Department of Ophthalmology in Hacettepe University Hospital, were included in the study. The participants in the case and control groups were selected at the ratio of 1:1. All the participants underwent routine ophthalmic examinations, including visual acuity, slit lamp biomicroscopic examination, intraocular pressure measurement with Goldman applanation tonometry, and dilated fundus examination. XFS was defined as a white, grayish material on the anterior capsule or pupillary margin of the iris or anterior-chamber angle but with no glaucomatous optic nerve damage or intraocular pressure (IOP ≥21 mm Hg) elevation. 2 The diagnosis of XFG goes beyond the symptoms of classical exfoliation material, with characteristic glaucomatous optic nerve damage, for example, neuroretinal rim thinning, focal area and polar notching or bayoneting sign, and visual field defects with at least two reliable standard automated perimetry [24-2 Swedish Interactive Threshold Algorithm (Humphrey Visual Field Analyzer; Carl Zeiss Meditec, Dublin, Ireland)]. The participants in the control group had no history of ocular disease, exfoliation findings, signs of optic nerve damage, and IOP ≥21 mm Hg.2–3
The questionnaire was created by the ophthalmologist, epidemiologist and nutritionist. While preparing the questionnaire, descriptive findings and factors affecting glaucoma reported in previous studies, daily habits and food consumption frequency questions were considered. The pre-trial of the questionnaire was applied in a different department of the same hospital, and the prepared questions were tested to see whether they could be replied effectively or needed to be amended or removed. The questionnaire consisted of sections examining the sociodemographic characteristics of the participants, their eating habits (with food frequency), anthropometric measurements, and home, living, and working conditions (indoor–outdoor). The questions were also about the type of house in which the participants had lived for most of their lives (>30 years), the type of heating methods they had used for most of their lives (>30 years), and whether they lived in a village, town, or city at birth, up to 12 years of age and after the age of 12 years. The house types were evaluated as apartments and others (slum dwelling or village house) and heating methods as a stove or a central heating system. The indoor and outdoor hours of daily work and total working years at the age of 20–50 years were also questioned.
Further, the eating habits of the participants and the consumption and frequency of bread, cereals, red meat, white meat, fish, olive oil, butter, milk, yogurt and cheese, eggs, vegetables, fruits, tea, and coffee were questioned, with response options of every day, 4–7 times/week, 2–3 times/week, 1–2 times/2 weeks, and less than once a month (including rarely and never). The individuals were evaluated according to the recommendations of the Turkey Dietary Guidelines (2016), which defined the daily consumption of different food groups and balanced meal routines required for a healthy diet. 18 The participants’ frequency of food consumption was assessed based on the recommendations of World Health Organization and the European Food Safety Authority to ensure unity and make comparisons.19–21 The food frequency was also assessed considering the Determination of Nutritional Status Report, which is an official publication of the Turkish Ministry of Health. 22 Data for the eating habits were analyzed according to the Turkey Nutrition Guideline (TUBER) 2016. Further, the statistical analyses of healthy and unhealthy eating habits were performed. The question regarding the frequency of wearing sunglasses was answered as “always”, “only on sunny days”, “during the summer holidays”, and “never.”
The questionnaire was added as supplementary material.
Statistical analysis
The data were collected, cleaned, and analyzed using SPSS v. 23.0 software (C3BA73A4-2A45-4036-8541-4F5F8146078B). The data set followed normal distribution. The chi-square test, Student t test, and analysis of variance were used for statistical analyses. The cut-off point of the study was taken as type 1 error α: 0.05. Risk [odds ratio and confidence interval (CI)] calculations were performed to evaluate the effect of the variables on the disease. All statistical analyses were double checked using the same software.
Results
The data collection and cleaning were completed, and the patients in the XFG and XFS groups were analyzed as case groups. The case group included 290 patients with XFG and 210 patients with XFS. The control group, without exfoliation material and glaucoma, included 500 normal individuals. Participants over 50 years of age were included in the study. The mean age of individuals in the case and control groups was 69.2 ± 7.6 and 68.8 ± 7.4 years, respectively. No statistically significant difference in age and sex was found between the groups (P = 0.259 and P = 0.880, respectively). The demographic characteristics and distribution of Body mass index (BMI) in the groups are shown in Table 1.
Demographic characteristic distribution in the case and control groups.
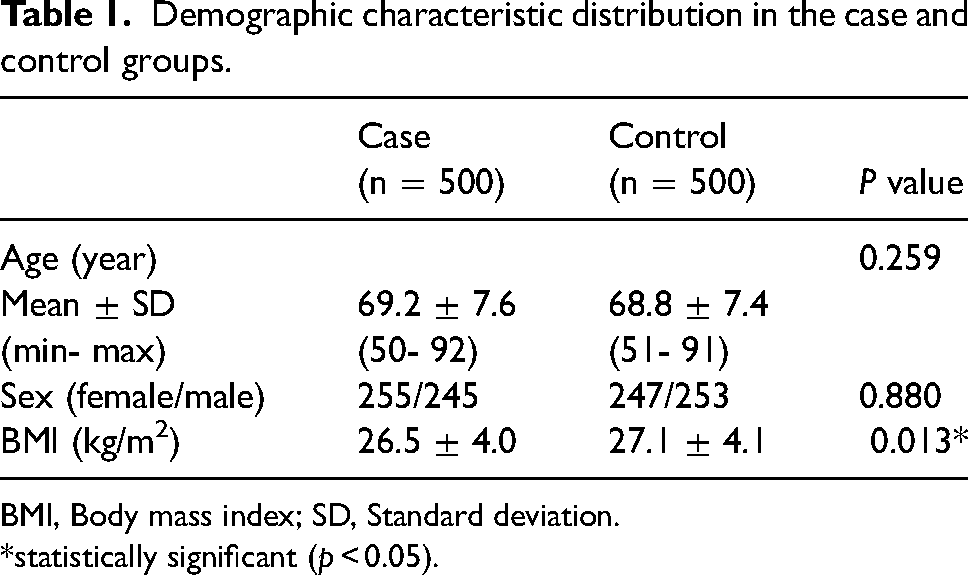
BMI, Body mass index; SD, Standard deviation. *statistically significant (p < 0.05).
The total number of years working outdoors or indoors and the average daily working hours were different between the groups (Table 2). The number of outdoor activities were significantly higher in the case group than in the control group: the mean working years outdoors (26.0 ± 8.96 vs 19.6 ± 7.51 years, P < 0.001) and average daily working hours outdoors (8.6 ± 1.94 vs 7.8 ± 1.72 h, P = 0.012). The mean working years indoors between case and control group (27.8 ± 7.58 vs 26.0 ± 7.10 years, P = 0.006) was found to be significant and average daily working hours indoors between case and control (8.1 ± 2.19 vs 7.8 ± 1.55 h, P = 0.121, respectively) were not significant statistically.
Distribution of the average working years and daily hours indoor and outdoor between case and control groups.
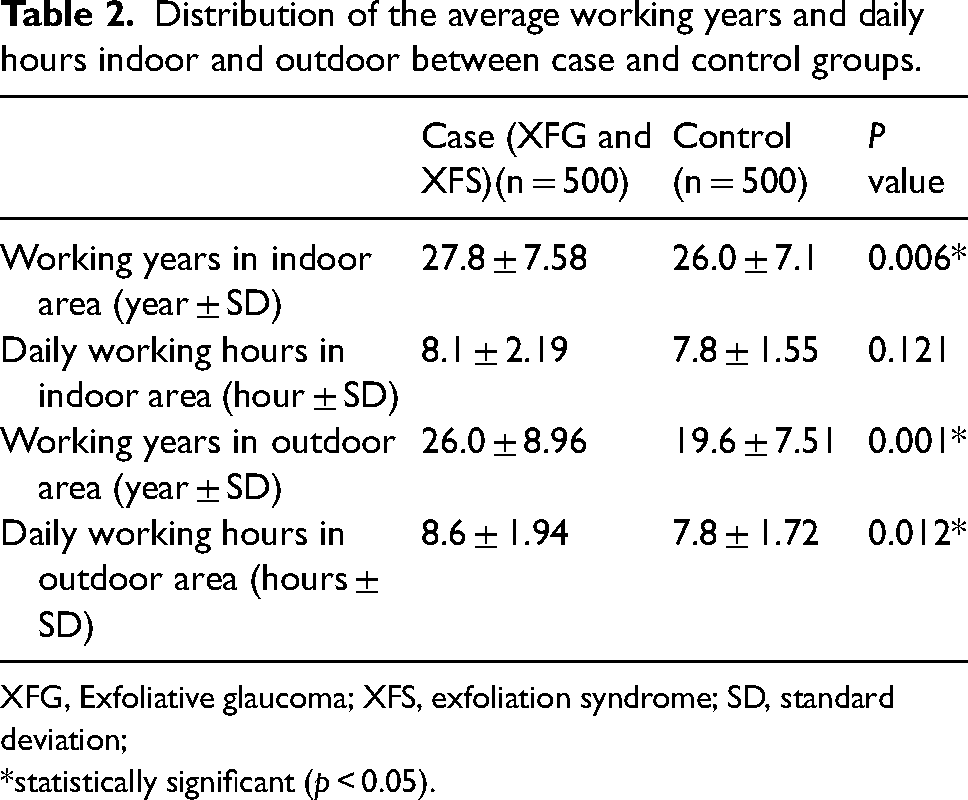
XFG, Exfoliative glaucoma; XFS, exfoliation syndrome; SD, standard deviation; *statistically significant (p < 0.05).
When individuals born in a village or town were taken as a group compared with those born in the city, the risk was found to be 1.46 times lower in those born in a city (95% CI: 0.49–0.95). Further, 64.8% of individuals in the case group lived in a village or town and 35.2% lived in a city, and it was seen that living in a village or town from birth to age 12 years increased the risk 1.36 times (95% CI: 0.55–0.94). No statistically significant difference was found with respect to where the participants lived the most from the age of 12 years to the present (Table 3).
Some lifestyle risk analyses between case and control groups.
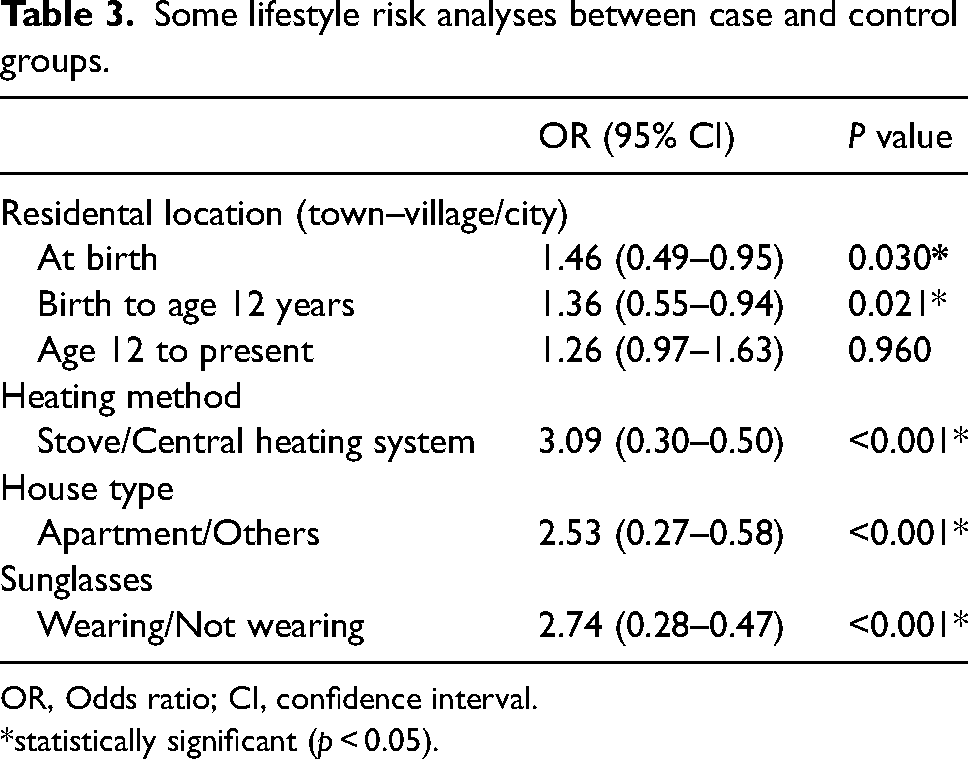
OR, Odds ratio; CI, confidence interval. *statistically significant (p < 0.05).
Using a wood- or coal-burning stove for heating was found to increase the risk of disease3.09 times (95% CI: 0.30–0.50) compared with the central heating system. In terms of type of housing, 91.4% of the control group and 80.8% of the case group had lived in an apartment for many years. Living in an apartment was found to be 2.53 (95% CI: 0.27–0.58) times more protective than living in other types of housing (Table 3).
Differences were found between the three groups (XFS, XFG and control) in terms of wearing sunglasses (P = 0.001). Wearing sunglasses (always, only on sunny days, or during the summer holidays) was noted in 34.2% of the case group and 58.8% of the control group. Further 65.8% of cases and 41.2% of control groups’ participants stated that they never wore sunglasses. Wearing sunglasses protected 2.74 (95% CI: 0.28–0.47) times than not wearing sunglasses.
According to the healthy nutrition criteria determined by TUBER, the groups were compared. A difference was found between the case and control groups in terms of healthy nutrition; participants in the control group had a healthier diet than those in the case group (P = 0.006). (Figure 1) The risk of disease in the unhealthy diet group was 1.46 (95% CI: 0.52–0.87) times higher than that in the healthy diet group. No difference was found between the case and control groups in terms of vegetables consumed regularly (P = 0.218), but regular fruit consumption was found to be 2.84 (95% CI: 1.63–4.96) times more protective against XFS/XFG. Drinking tea everyday was common between the two groups; 70.8% of the participants in the case groups and 75.6% of the participants in the control group consumed tea everyday and also 41.8% of XFS/XFG patients and 44.2% of the participants in the control group drank coffee every day. No statistical difference was observed between the groups in terms of tea (P = 0.05) and coffee consumption (P = 0.482) everyday.
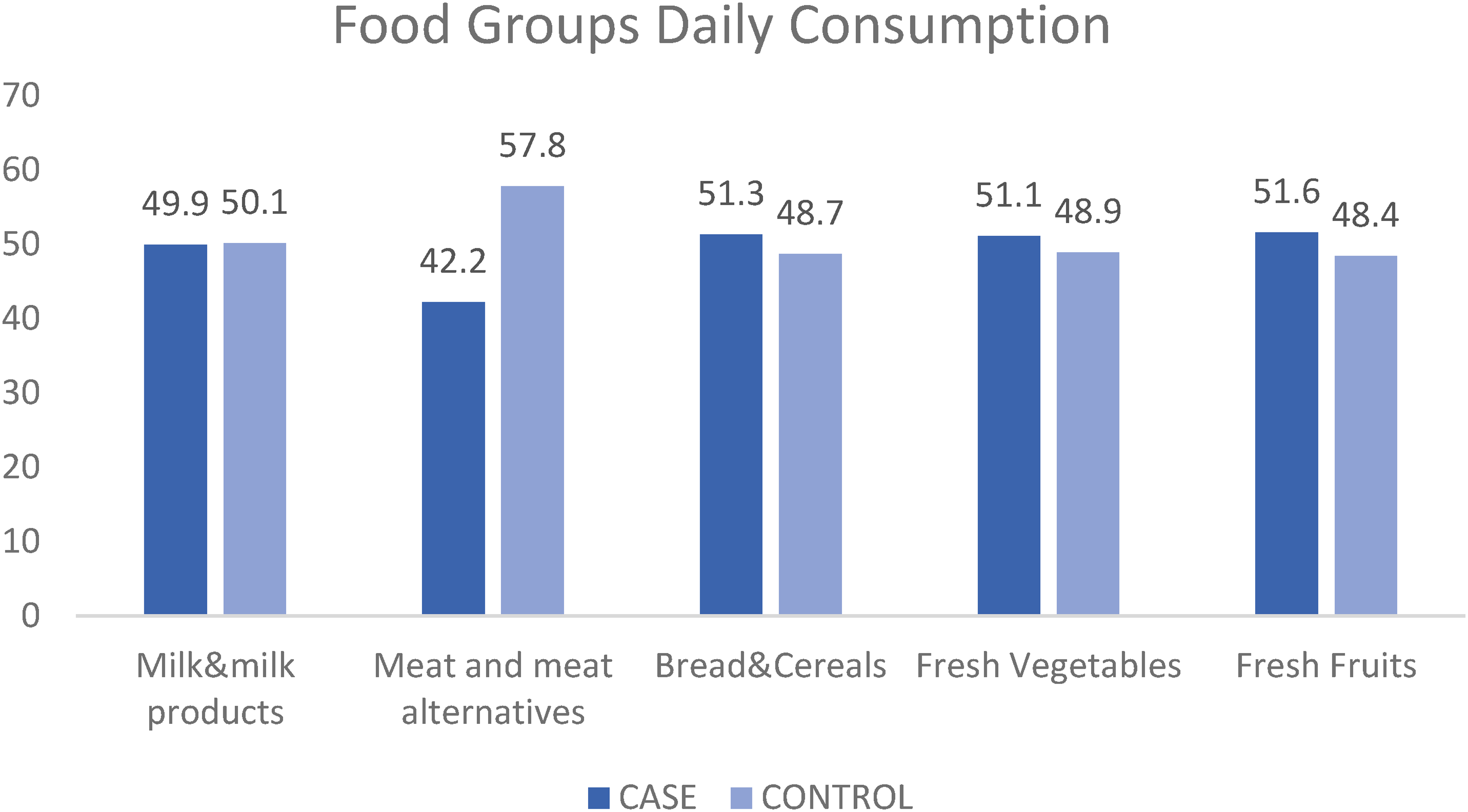
Distribution of daily food consumption between groups.
Discussion
The results of this case–control study of 1,000 participants demonstrated that some environmental factors might have a relationship with XFS/XFG. The time spent outdoors, wearing sunglasses, place of living and their characteristics such as heating methods or house type, and healthy eating habits were found to be associated with XFS/XFG in a Turkish population, which had a high frequency of exfoliation. The time spent outdoor and not wearing sunglasses were found to be related with increased risk of XFS/XFG. While the village or town life might be related XFS/XFG, living in apartment and not using stove were detected as protective factors. Higher fruit consumption and healthy eating habits were associated with a reduced risk of disease.
One of the most common environmental factor associated with XFS and XFG development in the literature is solar exposure. UVA (Ultraviolet A) and UVB (Ultraviolet B) radiation can reach the anterior uveal tract and lens passing through the cornea and UVR is also known to cause solar radiation–related diseases such as climatic droplet and pterygium in the anterior segment of the eye. 23 Some studies examining the presence of XFS with solar eye pathologies showed that UVR played an important role in the development of XFS.24,25 In vitro studies on Tenon's capsule fibroblasts were important in providing some evidence of the development of XFS through the effect of UVR. With UVR exposure, the expression of LOXL1, fibrillin-1, fibulin, and elastin, which are the basic elements of XFS was upregulated and these proteins were transformed into microfibrillar aggregates in the extracellular space. 15 A high prevalence of XFS in populations with high exposure to sunlight, such as Australian Aborigines, has been frequently observed, 26 besides reports that the risk of XFS/XFG increased by 1.5% with the increase in the number of sunny days per year. 11 Another study recorded the time spent outdoors for each decade of life from 10 to 60 years and found that every hour outdoors between 10 a.m. and 4 p.m. during the summer increased the risk of XFS by 4% averaged over the lifetime, and wearing sunglasses was related to a 2% reduced risk for XFS in the United States population, but not in Israel. 13 The present study determined that the increased risk of XFS/XFG was associated with spending more time outdoors and also not wearing sunglasses regularly. In the XFS and XFG groups, the mean working years and mean daily working hours were outdoor for longer periods of time, furthermore sunglasses were rarely or never used. Sunglasses were also found to be protective against XFS/XFG 2.74 times (95% CI: 0.28–0.47). In a Turkish population, solar radiation was found to be associated with XFS/XFG, in accordance with the majority of the literature.
Kang et al. surveyed the average time spent at different ages in a United States population; high school to age 24 years, age 25–35 years, and age 36–59 years. The multivariate analysis showed that the risk of suspected XFG/XFG increased twofold in participants who spent ≥11 h/week outdoors from high school to age 24 years, compared with participants who spent ≤5 h/week outdoors in the middle of the day (95% CI: 1.30–3.08; P = 0.001 for a linear trend). 12 Another prospective study of Kang et al. showed that at the age of 15 years, living in the middle or southern tier of the United States was the most important risk-reducing factor. The reason why place of residence at age 15 was so important that more time could be spent outdoors during adolescence. 10 In the early decade of life, more solar radiation may reach the eye and play an important role in the development of XFS due to more time spent outdoors and the large diameter of the pupils. 13 In the present study, the exposure to sunlight was examined only during a certain period, not throughout the whole lifetime. As the 20–50 years age range covers the young adult and adult periods, it is not possible to comment on the period in which the solar effect is more effective.
Many previous studies about residence reported a higher risk of XFS/XFG with increased latitude away from the equator.10,11,13 In this study, distinct from latitude or tier of cities, the emphases were on the place of birth, residential location up to the age of 12 years and current, and house type and heating method. Being born in a city or living in a city until the age of 12 years reduced the risk of XFS/XFG. Village or town life might have an impact on the development of XFS/XFG, although how this occurs is not known. It may be argued that those living in a village or town spend more time outside than city dwellers. In addition, the genetic transfer from parents may have an effect from birth onward, and the younger lifetime may play a much more critical role in body changes caused by the exposure factors.
Apart from the latitude, ocular sun exposure may also change with ground reflectivity. The reflection from surfaces such as snow or water is more than that from asphalt or grass. Depending on the position of the sun, ocular exposure may occur with direct or indirect sunlight. When the solar altitude is intermediate, about 40 degrees, 9–11 a.m. or 2–4 p.m., direct and indirect reflection to eye occurs, which may also be the strongest for high ground reflectivity. 27 This may allow the places with high reflectivity regardless of latitude to be designated as ‘hotspots’ for XFS development. 28 The effect of city and town life on the disease found in this study was perhaps for this reason. However, a detailed study is needed due to the lack of enough information.
When house types were examined in this study, living in an apartment was found to be more protective than living in slum dwellings and village houses. The materials used in construction or failure to provide adequate insulation in terms of external and internal ambient temperature might be responsible for this situation. Although the insulation is not valid for all, it may be generalized that this is better in the apartment compared with other house types. It is believed that the ambient temperature plays a role in the emergence of XFS. Stein et al. reported that the precipitation of the exfoliative material increased when the ambient temperature decreased and collapsed due to lower ocular temperature. 11 This study also evaluated heating methods and found an increased risk when a wood- or coal-burning stove was used for heating. This could be because the ambient temperature could not be kept adequately stable by the stove. In addition, the chemical factors in the fuels used, such as coal and wood, caused air pollution, which damaged DNA and might genetically effect the development of XFS.29–30 This study was novel in examining the residential history, such as city, town, village and house type, and the heating method used. The present study found that being born in the city and living until the age of 12 years was protective compared with living in the village or town. Also, using the stove as a heating method increased the risk, and living in the apartment for many years seemed to be a protective factor for the disease.
The Reykjavik Eye Study reported less XFS in participants who consumed dietary fiber-rich and yellow-green vegetables. 8 In addition, more frequent fruit consumption (1–2 times/2 weeks) results in lower rates of XFS compared with fruit consumption of less than once a month. 31 In the present study, no difference was detected in terms of vegetable consumption, but fruit consumption was found to be a protective factor against XFS, compatible with the literature. When the frequency of consumption of all the questioned food items was classified as healthy or unhealthy according to the TUBER 2015 data, healthy eating habits were found to be protective against XFS/XFG. In the study evaluating dietary intake by Kang et al., 17 it was found that a low serum level of folate was associated with XFS, but not B6 or B12 vitamins. Folic acid is an essential enzyme during the conversion of homocysteine into methionine. In the case of insufficient folate, increasing homocysteine level plays a role in the development of exfoliation by creating oxidative stress. 32 Due to the high levels of folic acid in vegetables and fruits, their consumption may be important in preventing the development of the disease.
A previous study observed that the risk of XFS/XFG increased in those who consumed three or more cups of coffee a day, but not with consumption of caffeinated tea, soda, or chocolate consumption. 16 This could be explained by the increased serum level of homocysteine after coffee consumption, 33 but in this study, no significant relationship was detected between tea and coffee consumption and XFS/XFG.
Overall this study had some limitations. The height and weight were taken with the declaration of the individuals, but they were not considered in the statistical evaluation about the disease. This study had selective bias, but a case–control study cannot be representative without nested case–control study. Although lifetime residence and individual solar exposure were examined, it was not possible to evaluate each decade of life from 10 to 60 years. Also, since it was questioned retrospectively, this could be the cause of the recall bias.
In conclusion, this study showed that environmental factors and eating habits had effects on patients with XFS and XFG who were admitted to Hacettepe University Hospital Ophthalmology Outpatient clinic. This was the first study on the effects of the type of residence and heating methods on XFS and XFG. The fact that environmental factors, besides genetics, have an impact on the disease, which causes serious ocular morbidity indicates that successful results can be achieved by eliminating preventable factors in the development of this disease. The future nested case–control study will provide more details on the Turkish population.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231178055 - Supplemental material for Evaluation of the effects of environmental factors and eating habits on exfoliation syndrome and glaucoma in a Turkish population
Supplemental material, sj-docx-1-ejo-10.1177_11206721231178055 for Evaluation of the effects of environmental factors and eating habits on exfoliation syndrome and glaucoma in a Turkish population by Figen Bezci Aygun, Ayse Tulay Bagci Bosi, Sibel Kocabeyoglu and Murat Irkec in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.