
Abstract
Introduction
Bilateral herpes zoster ophthalmicus (HZO) is rare. We report a case of an immunocompetent patient with nonsimultaneous attacks of HZO in both eyes.
Case Description
A 71-year-old female patient complained of blurred vision in the left eye for 1 week, which was treated with topical antiglaucomatous drugs due to elevated intraocular pressure. She denied any systemic diseases, but HZO had manifested as a rash with a crust over the right forehead skin 3 months earlier. Slit-lamp examination revealed localized corneal edema with keratin precipitates and mild anterior chamber reaction. Suspecting corneal endotheliitis, we performed aqueous tapping for detecting viral DNA, including cytomegalovirus, herpes simplex virus, and varicella zoster virus (VZV) DNA, through polymerase chain reaction (PCR) testing, but the PCR results were negative for all viruses. The endotheliitis resolved well after treatment with topical prednisolone acetate. However, the patient's blurred vision recurred in the left eye 2 months later. A dendritiform lesion on the left cornea was detected, and corneal scraping for PCR testing revealed VZV DNA. The lesion disappeared with antiviral treatment.
Conclusions
Bilateral HZO is uncommon, particularly in immunocompetent patients. When in doubt, physicians should perform tests such as PCR testing to help establish a definite diagnosis.
Introduction
Herpes zoster ophthalmicus (HZO) is a viral disease characterized by a unilateral painful skin rash in the dermatome distribution innervated by the ophthalmic branch (V1) of the trigeminal nerve; the rash is caused by varicella zoster virus (VZV) reactivation. The ophthalmic manifestations of HZO are caused by direct viral invasion, secondary inflammation, nerve damage, and tissue scarring. 1 To prevent complications and progressive visual morbidity, physicians must ensure a timely diagnosis of HZO, recognize its complications, and provide prompt treatment. 2 Most cases of HZO are unilateral; bilateral HZO is an atypical presentation of herpes zoster (HZ), with the literature having few reported cases.3–5 Herein, we report a rare case involving an immunocompetent patient affected by nonconcomitant attacks of HZO in both eyes.
Case description
A 71-year-old female patient without a history of chronic systemic diseases visited our dermatology clinic with a classic presentation of HZ, most notably unilateral erythematous vesicular eruptions along the V1 dermatome over the right side of her forehead. Ophthalmic consultation did not reveal intraocular lesions in the right eye. The skin lesion resolved following famciclovir treatment. Three months later, she visited our ophthalmology clinic for blurred vision persisting for 1 week in the left eye. Initially, she had visited a local clinic, where elevated intraocular pressure (IOP) was noted; therefore, she was treated with brimonidine and carteolol twice per day. Upon examination, her left-eye vision was 20/40 and IOP was 18 mmHg. Slit-lamp examination revealed inferior localized corneal edema with keratic precipitates and mild anterior chamber reaction in the left eye (Figure 1). Suspecting corneal endotheliitis, we arranged aqueous humor sampling to detect the presence of viral DNA, including cytomegalovirus, herpes simplex virus (HSV), and VZV DNA, through polymerase chain reaction (PCR) testing. The PCR results were negative for the mentioned viral DNA. The endotheliitis resolved well after treatment with topical prednisolone acetate. However, 2 months later, the blurred vision recurred in the left eye. Slit-lamp examination revealed a dendritiform lesion over the left cornea (Figure 2), and HZO was strongly suspected. We performed corneal scraping and ran PCR testing for HSV and VZV DNA. The PCR results were positive for VZV DNA. After 1 week of treatment with acyclovir ointment, the dendritiform lesion subsided, but corneal edema developed. Thus, the treatment was changed to 500 mg of oral famciclovir taken three times per day and topical prednisolone acetate applied four times per day. Some faint scarring remained thereafter.
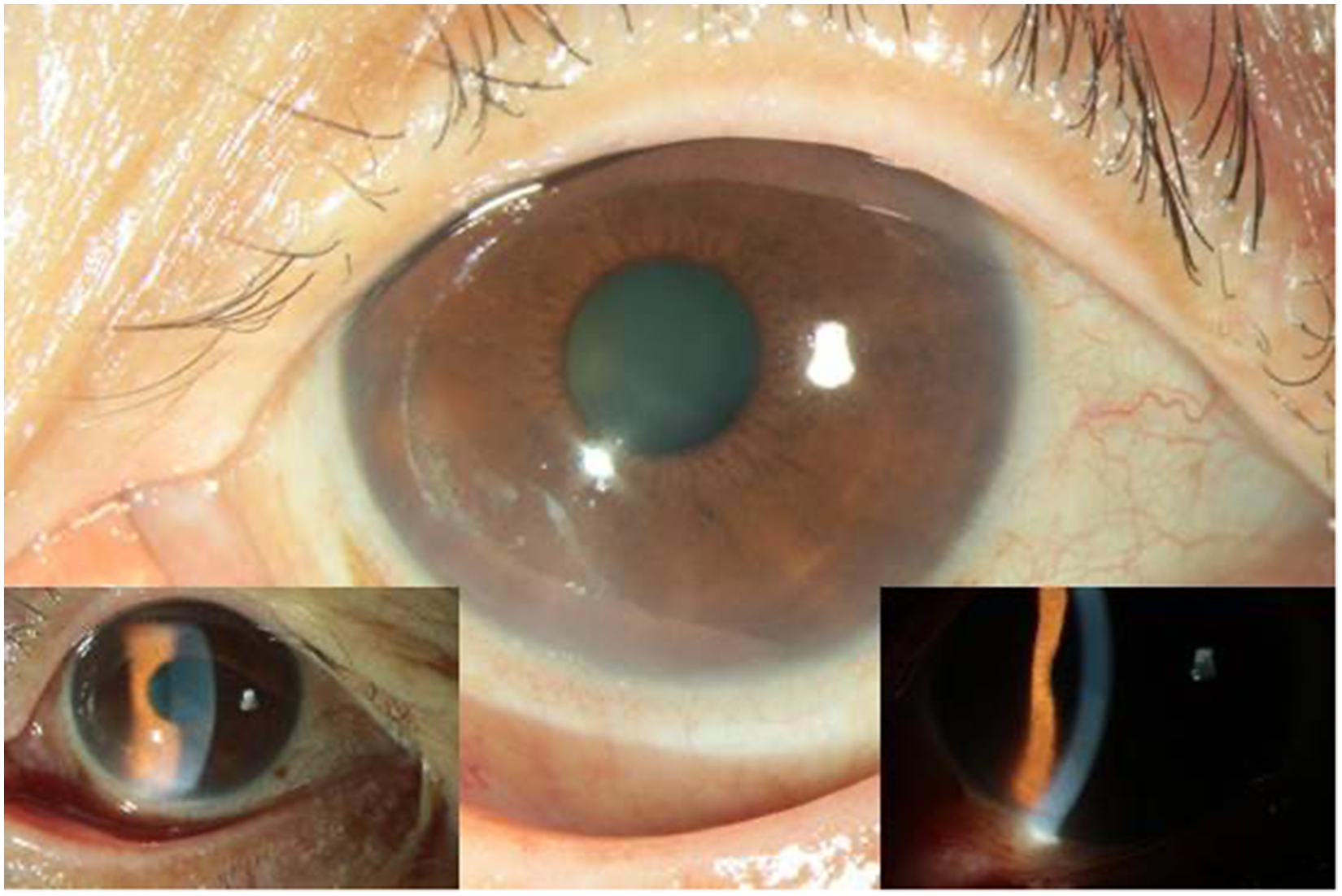
Slit-lamp photograph of the left eye showing inferior localized edema (left inset) with keratic precipitates (right inset).
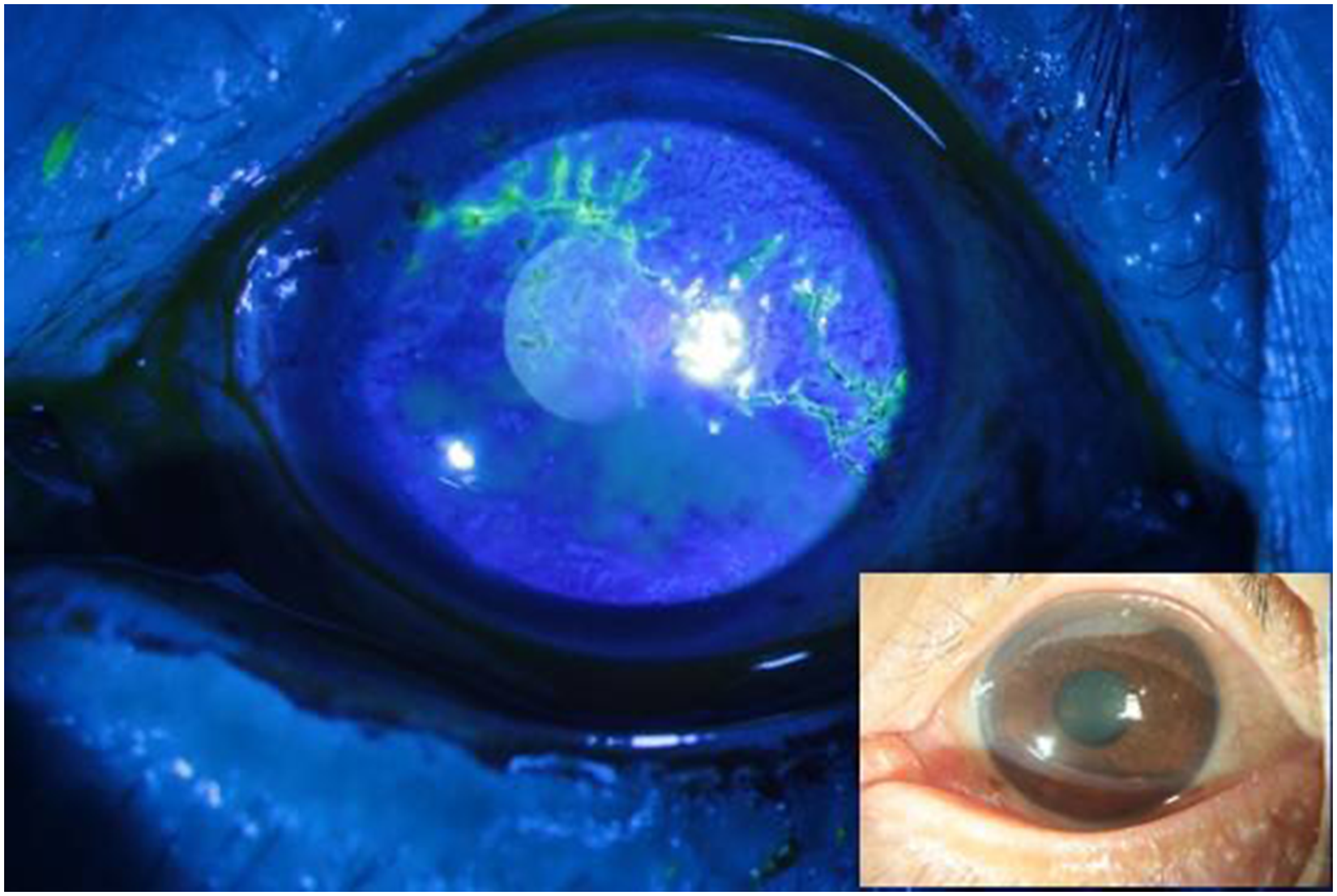
Slit-lamp photograph of the left eye showing a dendritiform lesion stained with fluorescein.
Conclusions
We report a case of an immunocompetent patient with nonsimultaneous HZO in both eyes. The diagnosis of HZO in her first eye (right eye) was based on the typical clinical presentation of vesicles and eruptions along the V1 dermatome. The first manifestation of HZO in the other eye (left eye) was corneal endotheliitis, but PCR testing of the aqueous humor was negative for viral DNA. The subsequent manifestation was a dendritiform lesion, a typical presentation of HZO, which was confirmed by PCR testing.
HZ occurs due to the reactivation of VZV residing in the dormant phase in the dorsal root or other sensory ganglia. Reactivation usually occurs due to a decline in the specific cell-mediated immunity caused by physiological aging or immunosuppression. HZ is characterized by unilateral erythema, blisters, and pain. The disease is usually limited to one side of the body. Bilateral HZ is an atypical presentation, usually found in immunocompromised or senile patients. Whether it occurs independently in two separate ganglia or is caused by viral evasion of cellular immunity and crossing over to the contralateral ganglion remains unconfirmed. 6
According to our review of current literature, three cases of bilateral HZO have been reported.3,4,5 Two of these cases involved immunocompromised patients, and the other involved a healthy young patient. All three patients had simultaneous bilateral V1 dermatome involvement but no intraocular involvement. However, in our patient, the episodes of HZO in both eyes did not occur concurrently, and no skin involvement was noted in the second eye, which rendered definite diagnosis challenging.
In our patient, it was difficult for us to make a diagnosis of bilateral HZO at the stage of corneal endotheliitis in the second eye. First, right-eye HZO had been diagnosed approximately 3 months before the left presented symptoms, which reduced the probability of concomitant bilateral HZO infection. Furthermore, the patient was immunocompetent, and her past history record was free of malignancy, immunosuppressive diseases or medication, organ failure, autoimmune disorders, or substance abuse. Second, the patient did not show dermatological presentations such as a vesicular rash or Ramsay Hunt syndrome that could indicate HZ over the contralateral V1 dermatome region. Third, the PCR testing of aqueous humor for viral DNA was negative. This result was a false negative owing to polymorphism, specimen degradation, or specimen scarcity. 7 Nevertheless, the subsequent dendritiform lesion helped us to make a diagnosis and provide appropriate treatment.
The management of HZO usually requires a multidisciplinary approach with the goal of reducing ophthalmic complications and morbidity. Timely diagnosis and aggressive management are imperative to reduce ocular damage and prevent vision loss. Although bilateral HZO is an uncommon disease, particularly in immunocompetent patients, when in doubt, physicians should collect samples through corneal scraping, aqueous humor tapping, and/or vitreous humor tapping for PCR testing to establish a definite diagnosis, especially when skin involvement is not present. We believe that the accumulation of more experience with cases similar to the presented case will contribute to the early diagnosis of and establishment of an optimal management protocol for patients with VZV reactivation and will enable the elucidation of the pathogenic mechanism underlying bilateral HZO.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.