
Abstract
Background
To describe OCT-angiography features in a case of an optic disk pit (ODP) which underwent a pars plana vitrectomy with inverted ILM flap for macular detachment.
Case presentation
A 12 years old child with an ODP responsible for a macular detachment underwent 23G vitrectomy in the subacute phase of the disease with an inverted ILM flap used as a plug over the lateral dehiscence of the pit. Among the various retinal imaging examinations performed in the post-operative period, the OCT-angiography showed very interesting features characterized by a capillary drop-out in correspondence of the superficial and deep capillary plexus, a fine texture of the choroid capillary layer and star-shaped folds in correspondence of both the outer retina and the choroid capillary layer. OCT-A performed 24 months after surgery showed a normalization of the macular perfusion which correlated with a full recovery of the visual acuity of the young child.
Conclusions
OCT-A is an useful tool to monitor the subretinal fluid reabsorption after ILM inverted flap surgery for ODP-maculopathy and correlates with visual function. OCT-A may be useful in the follow-up of this rare condition as well as its response to therapeutic strategies.
Keywords
Background
Optic disk pit (ODP) was described for the first time by Wiethe in 1882. 1 Up to 75% of cases may have intraretinal schisis and macular detachment due to the passage of fluid from the pit to the fovea, which may cause a loss of vision secondary to a serous macular detachment. Sometimes a reduced visual acuity may be secondary to macular schisis, cystic degeneration, outer macular lamellar hole, degenerative pigment retinopathy, and epiretinal membrane formation. These semeiological entities have been included in the same nosological group: the optic disc maculopathy (ODP-M) which may benefit from delayed vitreo-retinal surgery. 2
Case description
In the present report we describe a case of a 12-year-old Caucasic female referred to our observation for a sudden decrease in visual acuity of her right eye. A diagnosis of “Morning Glory” disk anomaly in her fellow eye was made previously (Figure 1). General medical history and familiar medical history were negative. Anterior ocular segment was unremarkable bilaterally with an intraocular pressure of 13 mmHg in both eyes. Best Corrected Visual Acuity (BCVA) was 1.2 LogMar LogMAR in the right eye and 1.6 LogMar the left eye. Dilated fundus examination showed the presence of an infero-temporal ODP in the right eye; a retinal detachment involving the macula and the supero-temporal midperiphery extending to the temporal border of the optic nerve was found (Figure 1); a diagnosis of Morning Glory optic disk in her contralateral eye was confirmed. The patient underwent SD-OCT examination (Cirrus 5000, Zeiss, Meditec) that highlighted an hyperreflective strip going from the ODP to the fovea, causing a total macular schisis with splitting of all retinal layers (Figure 2). Edema measurement was performed by applying the ETDRS grid: the maximum thickness was 523 μm, located in the sector 5. Choroidal thickness at SD-OCT was 221 micrometers.

A. Fundus photography shows serous macular detachment departing from the optic disk temporal edge (showed by the arrow) and a yellowish round circumscribed depression in correspondence of the temporal sector of the optic nerve head (indicated by the star). B. Fundus photography indicates the Morning Glory Syndrome in the left eye. C. Late time fluorescein angiography presents a diffuse ovoidal leakage, confirming the serous macular detachment (pointed by the arrow). D. Late time fluorescein angiography displays ODP (showed by the arrow). E. OCT-A of the right disk shows a black round zone in the temporal edge of the optic nerve head (indicated by the arrow), a peripapillary dark halo, partially hiding superotemporal vessels emerging from the optic nerve, and a gathering of capillaries inferiorly to the ODP. F. OCT-A of the Morning Glory Anomaly shows a croissant-shaped papilla with no decorrelation signal (pointed by the arrow) and absence of vascular arcades. Diffuse capillary rarefaction is present.
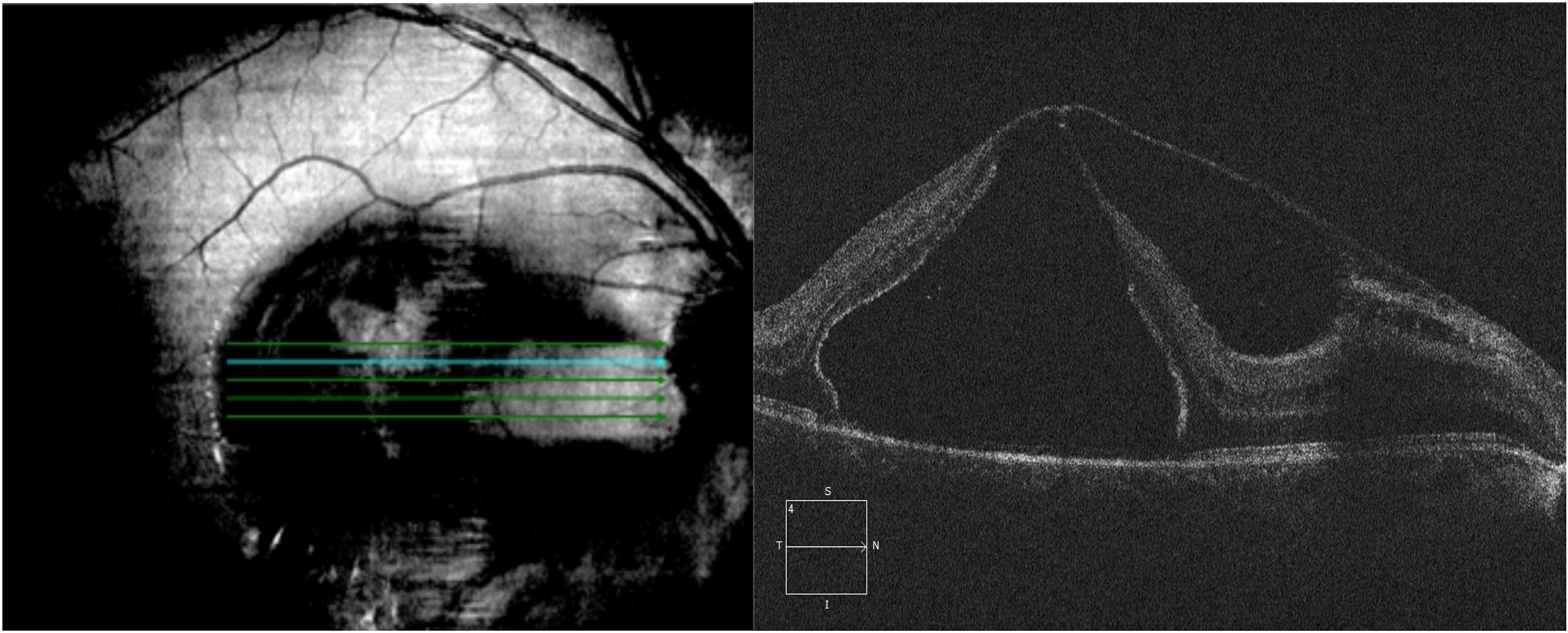
SD-OCT shows total thickness schisis with an outer lamellar macular hole, hyaloid adherence with points of cleavage in correspondence of nasal iuxtafoveal region and papillary area; ILM splitting is also visible.
Fluorescein angiography showed an hyperfluorescent round area in the temporal sector of the optic disc with a delayed leakage in the macular area responsible of the macular detachment (Figure 1). A diagnosis of ODP-M with foveo-schisis and neurosensory detachment was made.
For this reason, considering the low level of BCVA of the child, she was scheduled for surgery approximately 60 days after the diagnosis of ODP-M: a complete 23Gauge pars plana vitrectomy (PPV) was performed on her left eye (surgeon PMG) under general anesthesia with peeling of the inner limiting membrane (ILM) of the posterior pole after staining with MembraneBlue Dual® dye. During pars plana vitrectomy a posterior vitreous detachment was induced. Peeling started from fovea with sparing of the temporal hemi-macula after staining with membran blue dual. A vitreal traction from the edge of the pit was removed using a micro plier and the dehiscence of the optic pit was plugged using the inverted ILM flap which have been previously obtained. The optic pit was closed, by introducing the ‘inverted flap” inside. Preventive endolaser was made around sclerotomies and isovolemic mixture of SF6 was injected. A careful fluid-air exchange was made with particular attention to prevent ILM flap dislodgement. Sclerotomies were closed with Vycril 8.0 sutures. A face down position was maintained for 24 hours after the surgery. No complications occurred during and after the procedure.
Optical Coherence Tomography Angiography (OCT-A) (Optovue Device, XR Avanti, California) was performed at different times after surgery: time 0 (few days after surgery)- Figure 3-, time 1(approximately 2 months after surgery) – Figure 4- and time 2 (24 months after surgery)- Figure 5. Images with a signal strength below 6.0, with motion artifacts or with incorrect segmentation were excluded from our analysis. Projection resolved OCT-A (PR-OCTA) software for AngioVue device has been applied on OCT-A images.
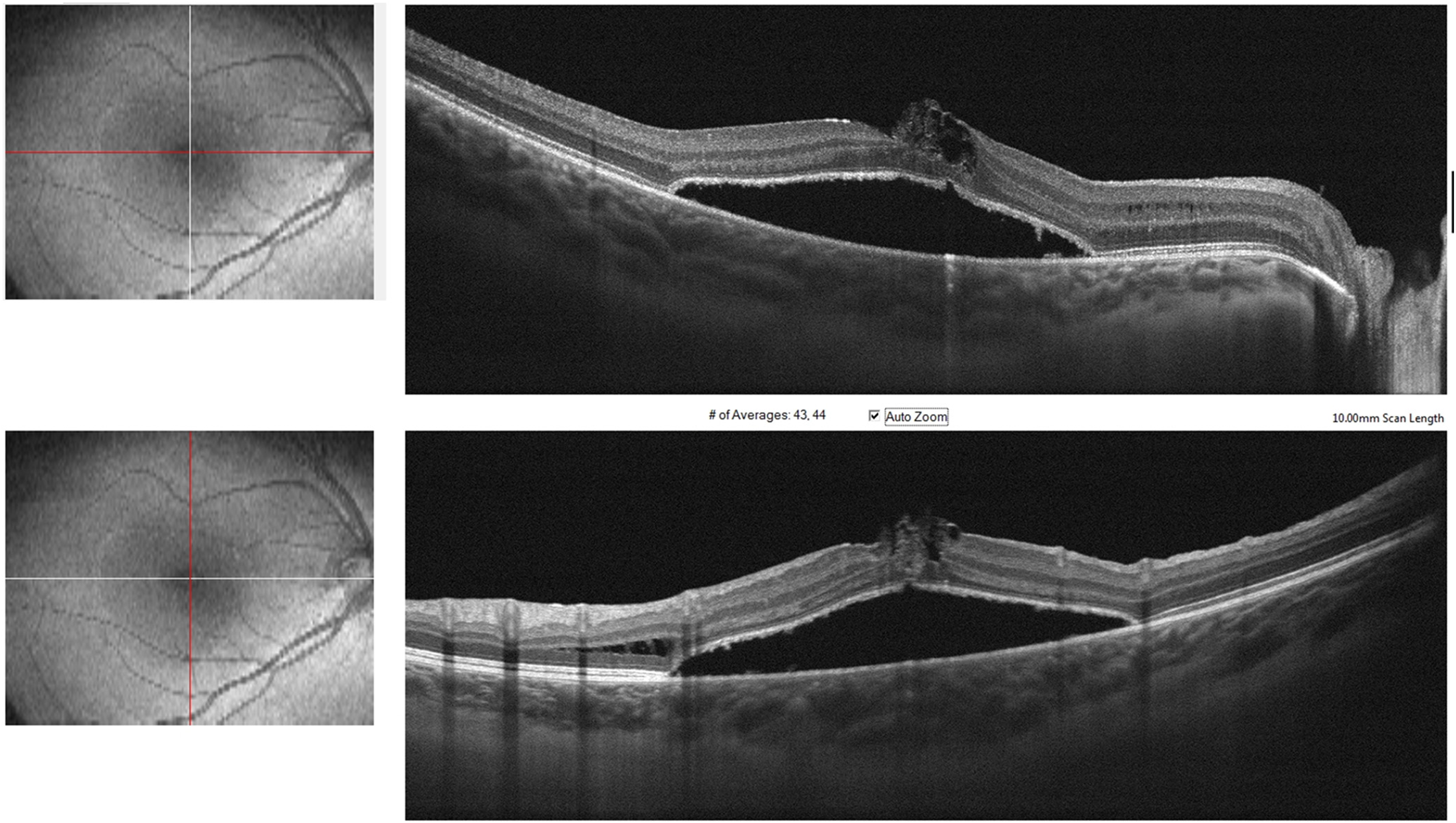
SD-OCT reveals complete reconstitution of retinal layers with schisis disappearance. Hyporeflective subretinal detachment is present.
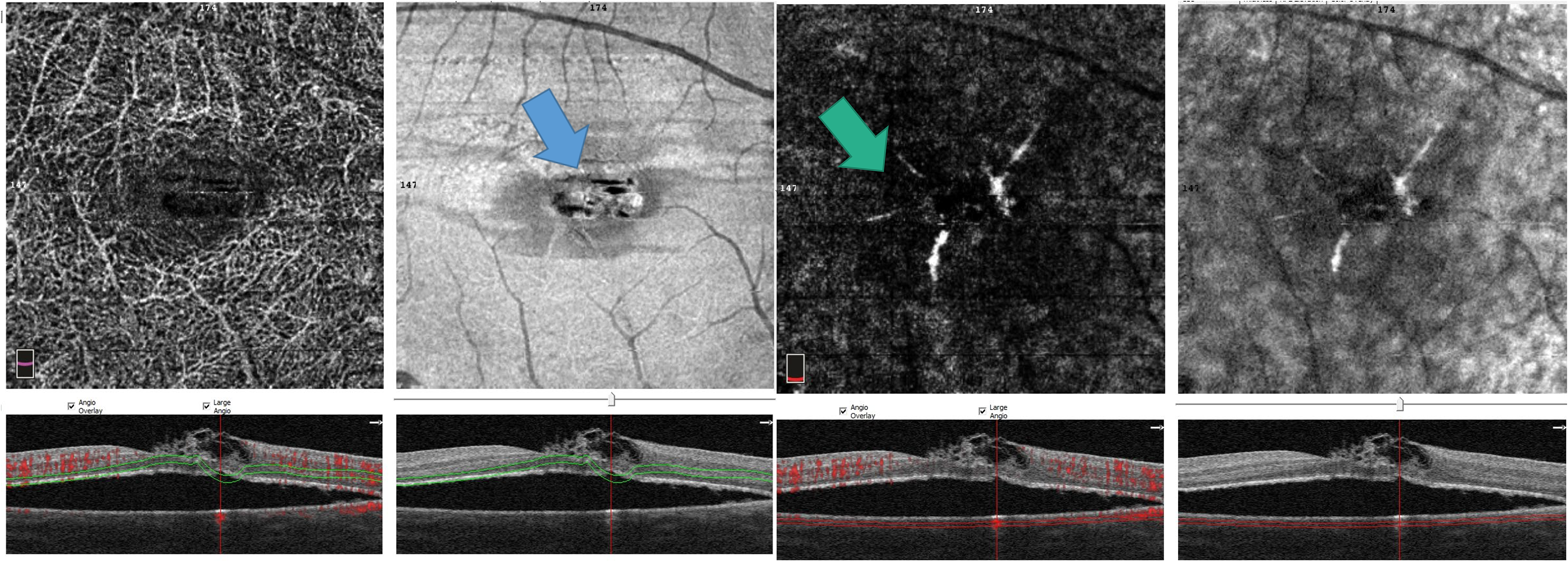
A. OCT-A and En-face OCT shows star-shaped straight lines in correspondence of the outer retina (indicated by the arrow). B. OCT-A and En-face OCT indicates radial lines in the choroid capillary layer (showed by the arrow).
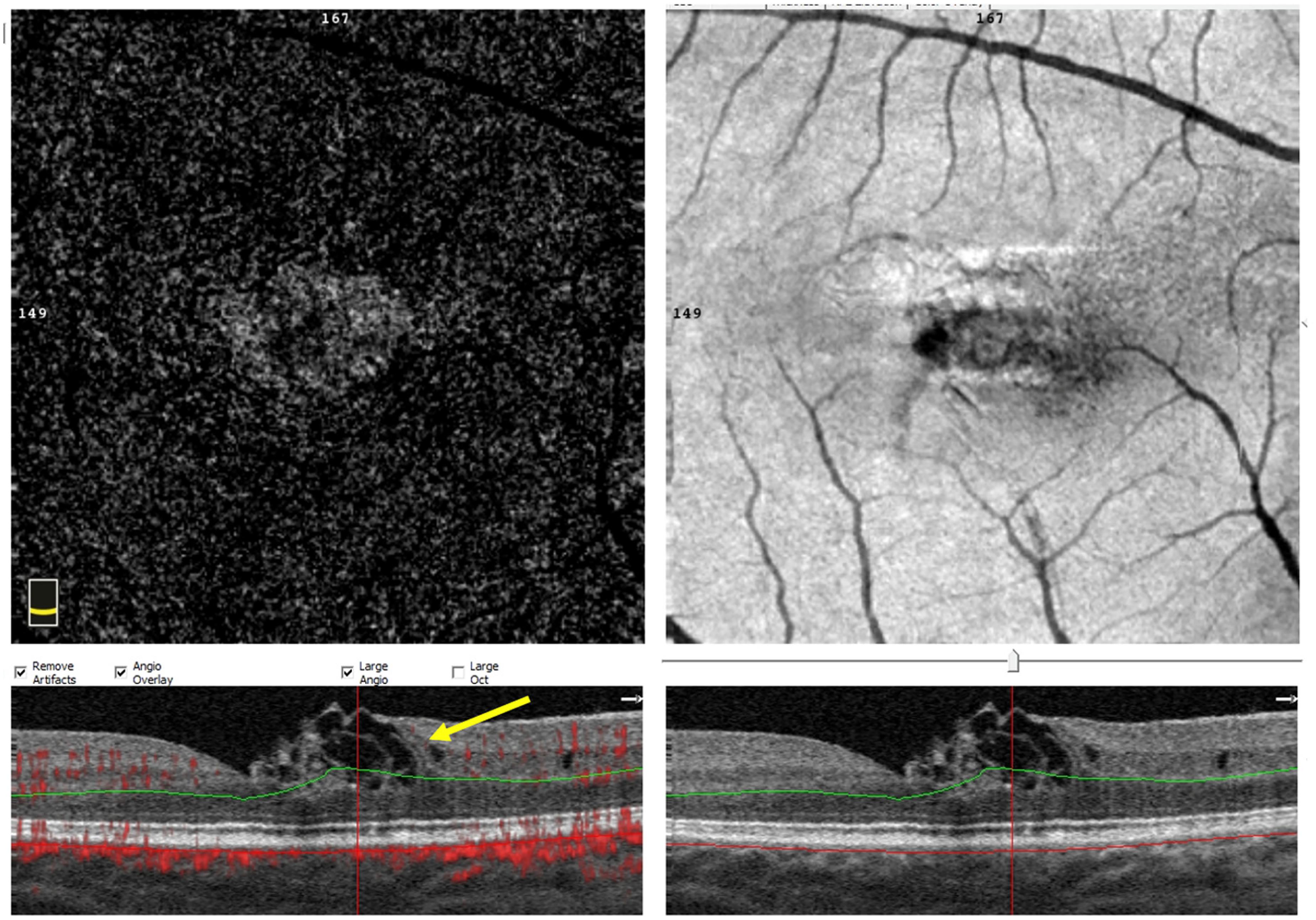
OCT-A shows a complete reabsorption of the subretinal liquid and a total reconstitution of the retinal issue. Parafoveal nasal hyporeflective cysts are visible in correspondence of the tissue that goes from the inner nuclear layer to the limiting membrane on B-scan (showed by the arrow).
OCT-A showed an overall rarefaction of mean vessels and capillaries in superficial and deep capillary plexus. In correspondence of the outer retina and choroid capillary layer, four straight lines departing from fovea with a star-shaped disposition were visible, also present in En-face OCT of the outer retina and choroid capillary layer (Figure 4). OCT-A showed an overall dropout of mean vessels and capillaries in superficial and deep capillary plexus.
The BCVA of the young child is actually (24 months later) 0.0 LogMAR and SD-OCT shows a complete recovery of retinal layers with normalization of the OCT-A features 3 (Figure 5).
OCT-A of optic disk showed a circular black area in the temporal sector extending to the choroidal capillary layer with a conical structure, inferiorly and nasally surrounded by a thick capillary network. 4 Optic disk was encircled by a dark halo, and superotemporal vessels seemed to be partially hidden by ODP. In correspondence to the outer retinal layer and choriocapillary layer, star-shaped folds were found (Figure 4).
AngioVue of optic disk of the contralateral eye indicated an ovoidal black structure dragging the surrounding capillaries. Vascular arcades were absent. Capillary rarefaction was present (Figure 1).
Discussion and conclusions
Multiple surgical techniques have been proposed and applied for ODP-M; argon laser, scleral buckle, optic nerve sheath fenestration, pneumoretinopexia, PPV with or without ILM peeling. The rarity and very low prevalence of the disease makes the choice very difficult, yet nowadays PPV is the standard of choice and is usually performed after the presence of a macular detachment.5,6 Nowadays there is a general agreement on an attendance interval of 3 months from the appearance of ODP-M before PPV, in order to ward photoreceptor layer disruption off after the launch of anaerobic pathway and the production of increased lactic acid, dextrose and phospholipids. 7 Regarding the intraoperative procedures that we can offer to these patients, the most recent comparative studies have demonstrated that juxtapapillary laser photocoagulation is not necessary as it has similar functional other than anatomical results compared to PPV without laser.5,8 Furthermore, among the intraoperative options that we can offer it seems that ILM plugs have a more lasting effect compared to other plugging techniques. 9
Post-operative SD-OCT of this case report patient complies with literature data about the persistence of subretinal liquid (mainly composed of hyaluronic acid) for 1–2 years after surgical operation. Visual acuity recovery of the patient was also concordant with the improvement of the visual function already described in some articles after OPD-M development. 10
OCT-A revealed the presence of a starlike pattern in the outer retina and choroid capillary layer. In 1981, Wolter described the presence of EPR reversed pits or folds during chronic edema, due to the detachment of the outer limiting membrane and of the central cones from the pigment epithelium, due to the pumping of the exceeding liquid by the EPR. 11 Radial chorioretinal folds have been also associated to retinal epithelium detachment in case of neovascularization. Retinal folds have been already studied by Aeko et al. in X-linked retinoschisis patients, highlighting their disappearance after acetazolamide inhibitors therapy. 12 Straight lines in outer retina and choriocapillary layer may be attributable to eye motion, projection or image processing artifacts albeit the same star-shaped pattern is found also in the matching En-Face OCT frame and no retinal structures are visible above our OCT-A finding.
In our case report, retinal and choroidal folds visible at En-face OCT and OCT-A were separated from the EPR by a very dense, chronic subretinal fluid, as an attempt to perpetually eliminate it. The peculiarity of this case consists in the concomitance of the optic disc pit and the Morning Glory Syndrome: OCT-A may represent a sensitive technique to monitor the evolution of this rare conditions rather than evaluating its response to different surgical approaches.
Footnotes
Availability of data and materials
The authors confirm that all data underlying the findings are fully available without restrictions. “Authors confirm that all data underlying the findings in the present study are freely available in the manuscript”.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The research protocols were conducted in accordance with the tenets of the Declaration of Helsinki. An informed consent for participation in the study was obtained where participants are children (under 16 years old) from their parent or guardian.
A written informed consent for publication was obtained.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.