
Abstract
Objective
To determine the preference for dacryocystorhinostomy (DCR), patient selection criteria for endoscopic DCR, endoscopic DCR technique, and barriers to adoption of endoscopic DCR.
Method
Cross-sectional study conducted from May-December 2021. A survey was sent to oculoplastic surgeons. Questions on demographic characteristics, type of clinical practice, technique preferences, barriers and facilitators to adoption of endoscopic DCR were included.
Results
245 participants completed the survey. Most respondents were located at an urban site (84%), were in private practice (66%), and had been in practice for more than 10 years (58.9%). Sixty one percent perform external DCR as the first line procedure for treating primary nasolacrimal duct obstruction. The most common factor influencing the surgeon's decision to perform endoscopic DCR was the patient's request (37%) followed by endonasal exam (32%). The most common barrier for not performing endoscopic DCR was the lack of experience and lack of training during fellowship (42%). The most worrisome complication for most respondents was failure of the procedure (48%), followed by bleeding (30.3%). Eighty one percent believe surgical mentorship and supervision during initial cases would facilitate endoscopic DCR learning.
Conclusions
External Dacryocystorhinostomy is the preferred technique for treating primary acquired nasolacrimal duct obstruction. Learning endoscopic DCR early during fellowship training and high surgical volume to improve the learning curve dramatically impacts the adoption of the procedure.
Introduction
It is well established that the gold standard treatment of epiphora due to primary acquired nasolacrimal duct obstruction is dacryocystorhinostomy (DCR). Success rates documented for this procedure range between 80–95%. 1 The external approach is performed by a cutaneous incision to access the lacrimal sac.1–3 This procedure became widely accepted due to its efficacy and minimal complication rates.1–3 The endonasal technique was impractical when first introduced in 1893 by Caldwell, until 1989 with the advent of endoscopes and illuminators allowing visualization of endonasal anatomy.1–3 Endoscopic endonasal DCR (EE-DCR) has slowly gained acceptance due to the comparable success rates, absence of skin scarring and shorter recovery periods. 1
The challenge with EE-DCR however is learning and mastering this technique while operating on unfamiliar topography using monocular endoscopic views that ophthalmologists are unaccustomed to. 4 This is compounded by the initial steep learning curve and the need for expensive instrumentation.1–4
Both approaches have been modified several times over the years. 5 The aim of this study is to build on current literature by surveying a sample of oculoplastic surgeons to determine their preference for DCR, patient selection criteria for EE-DCR, EE-DCR technique as well as barriers to adoption of EE-DCR.
Material and methods
This cross-sectional study was conducted from May-December 2021. The Institutional Review Board at King Khalid Eye Specialist Hospital approved this study, and study procedures followed the tenets of the Declaration of Helsinki.
The survey was developed by the study investigators. It included 38 questions mainly on demographic characteristics such as age, geographic location, duration in practice (years), and type of clinical practice (academic university, academic non-university, private multispecialty group, private single-specialty group, private solo) (see Appendix 1).
The sampling method was a convenient sampling employing the snowball technique; therefore, estimated response rate could not be generated. The aim was to reach a large number of participants. We used multiple platforms, including data from the global educational forum from King Khalid Eye Hospital, and we contacted each society through a representative from the co-authors, namely, the Saudi Oculoplastic and Orbit Group SOOG through (HS), American Society of Oculoplastic and Reconstructive Surgery ASOPRS (RA), European Society of Plastic and Reconstructive Surgery ESOPRS (DS), Brazilian Oculoplastic Surgery Society BOSS (SS), Asia Pacific Society of Ophthalmic Reconstructive Surgery APSOPRS and Hong Kong Society of Ophthalmic Plastic and Reconstructive Surgery HKSOPRS (HY).
The technique preferences were correlated with type of training (formal training in oculoplastic vs. non formal training), duration of training (2 years or less), period of training (70 s,80 s,90 s,2000 and after), exposure to DCR cases during training (external, endoscopic endonasal, non-endoscopic endonasal DCR) and the volume of cases.
Low volume was defined as less than 2 cases/week, moderate as 3–5 cases/week and high volume as more than 6 cases/ week. Respondents were classified as new in practice (10 years or less) or established in practice (>10 years).
We inquired about oculoplastic surgeons’ preferences for dacryocystorhinostomy (DCR) including the use of stent, duration of stent retention, use of antimetabolites, and patient selection criteria. Finally, barriers and facilitators to the adoption of endoscopic DCR were reviewed.
Statistical analysis
Chi-squared and Fisher exact tests, as deemed appropriate, were used to summarize categorical data. Statistical analysis was performed using paired t tests, with threshold for significance set at p < 0.05. All analyses were performed using Stata statistical software (version 14, StataCorp, College Station, TX).
Results
Demographics
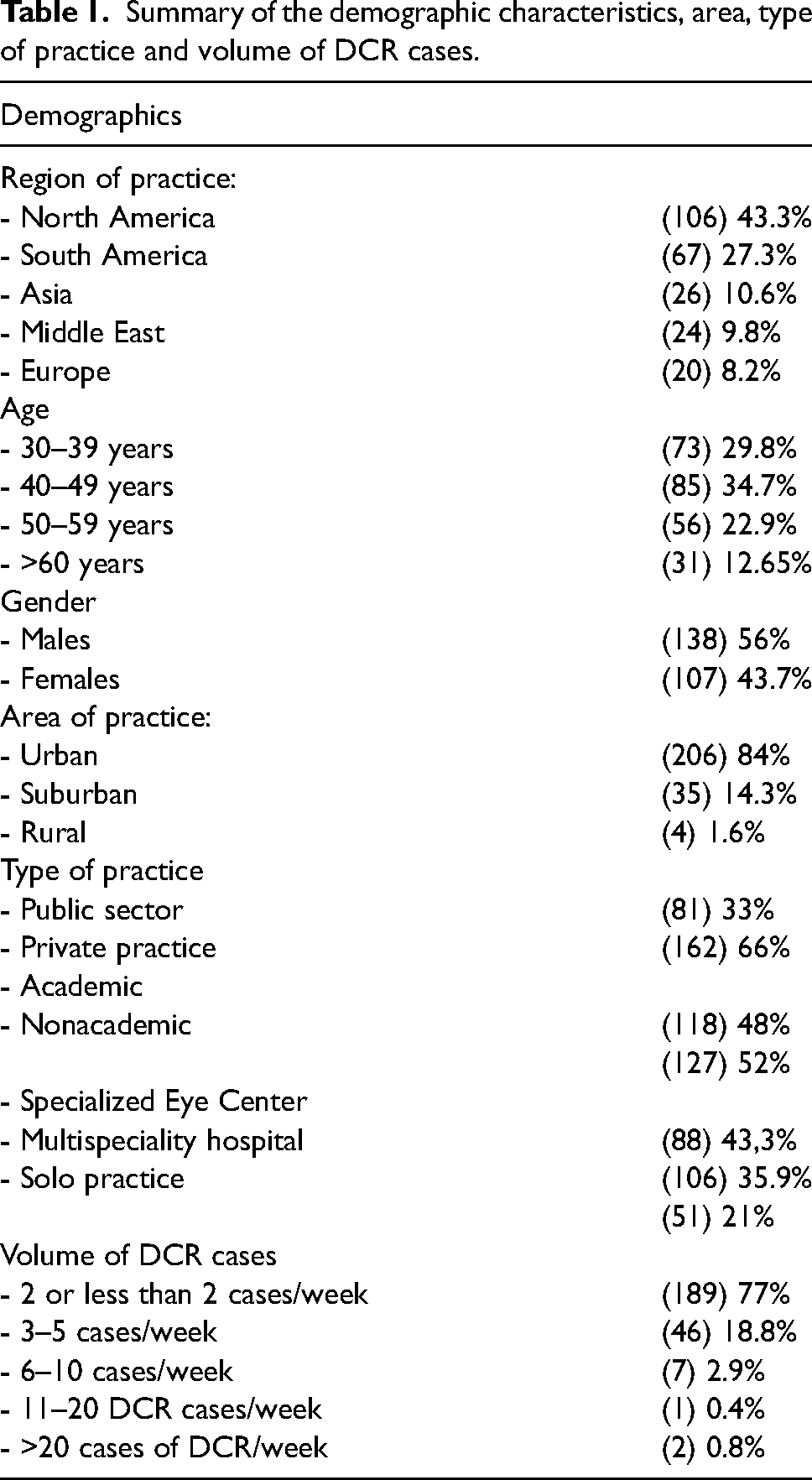
A total of 245 respondents completed the online survey. Demographic characteristics, including age, gender, region, area, and type of practice, are summarized in table 1.
Summary of the demographic characteristics, area, type of practice and volume of DCR cases.
training
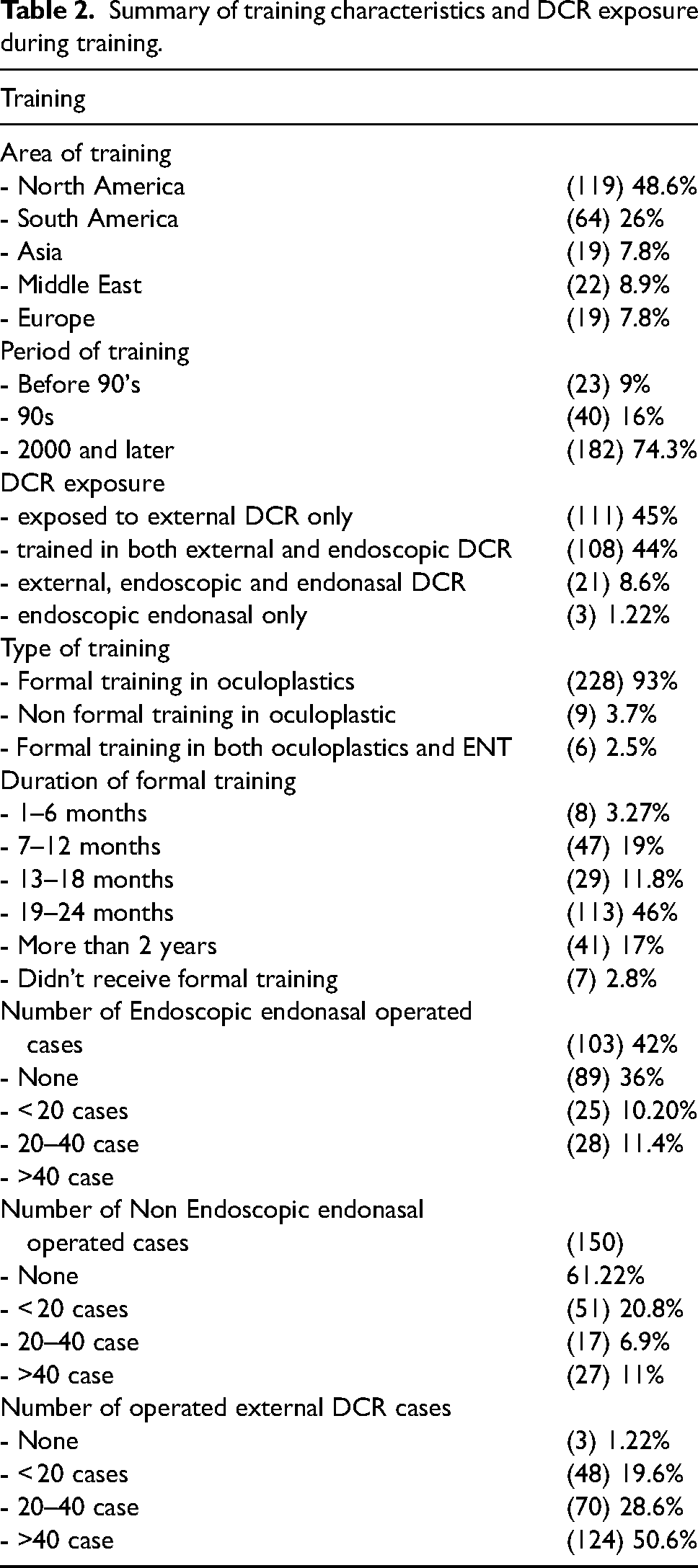
Table 2 summarizes characteristics of training, including the country where the training was performed, type of training, duration, period of training, techniques exposed, and the number of cases performed during training.
Summary of training characteristics and DCR exposure during training.
Practice
The pattern of practice, preferences and factors influencing the decision to perform endoscopic DCR are summarized in table 3.
Patterns of practice and factors influencing the decision to perform endosopic DCR.
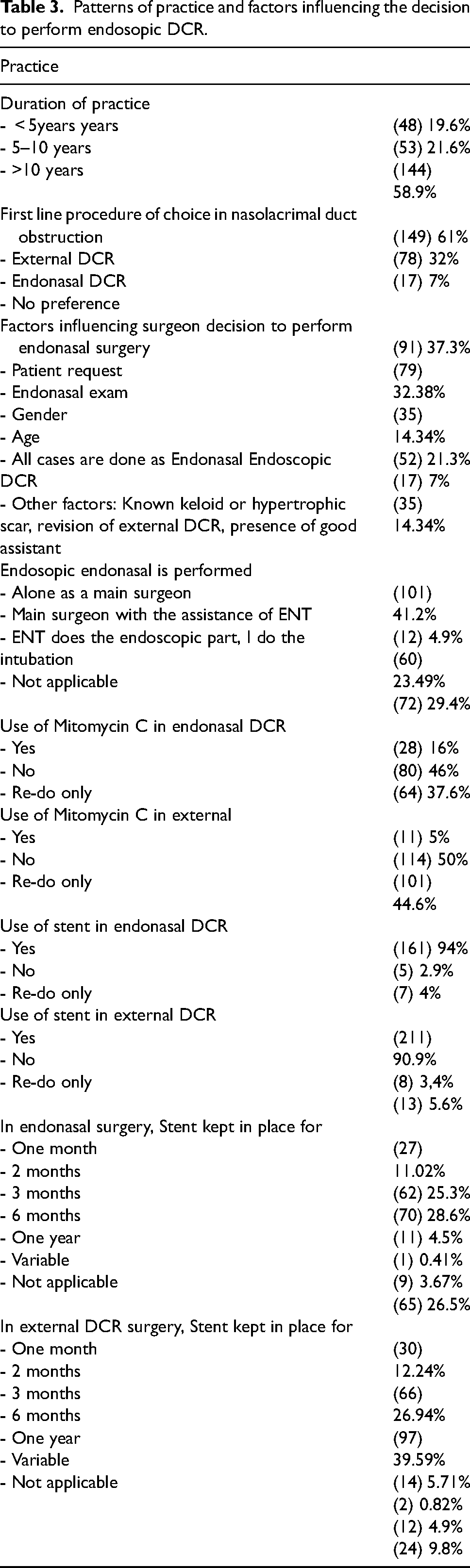
According to the respondents, the most common factor to affect their decision to operate was patient's request followed by endonasal exam. Other factors are summarized in table (3).
Barriers and potential facilitators for endoscopic DCR adoption:
Most respondents (45%) reported lack of experience as a barrier to not performing endoscopic endonasal DCR. 42% were not trained during the fellowship. The following factors also influenced the respondents’ decision: investment to acquire instruments for surgery is very high for a small number of procedures available (31%), steep learning curve (29.9%), concern about the surgical outcome (27%), limited visibility of endoscopic DCR (25.4%) and lack of resources (25.3%). 52% consider endoscopic DCR to have a similar success rate to external DCR. 44% find that endoscopic DCR is more challenging to perform.
The most worrisome complication for most of our respondents was failure of the procedure (48%), followed by bleeding (30.3%) and Injury to the skull base (7.8%). 22.5% are satisfied with their results in external DCR and not interested in learning endoscopic DCR
81% believe surgical mentorship and supervision during initial cases would facilitate endoscopic DCR learning. Other facilitators include high surgical volume to improve the learning curve (62.4%), initial training with an ENT surgeon to become familiar with nasal anatomy and the endoscope (44.9%), wet lab experience (44.5%) and surgical simulators to improve endoscopic maneuvering skills (40%).
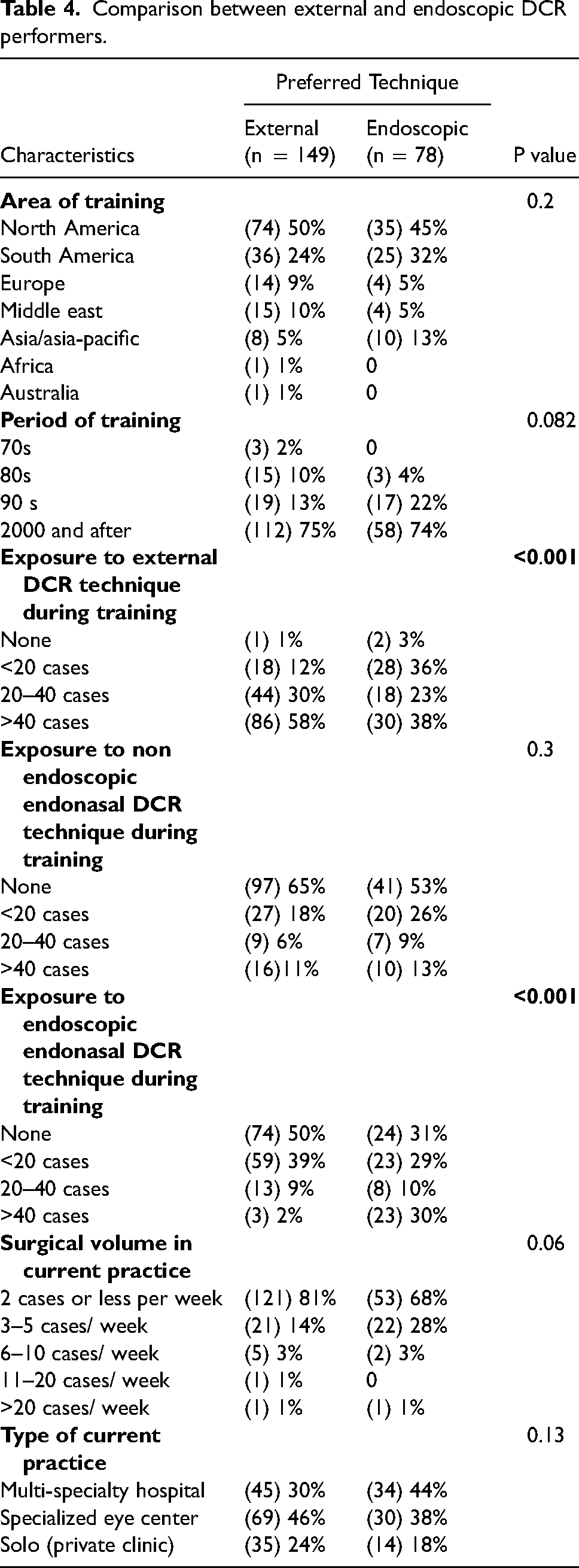
We observed that participants who were trained in 1990 onwards had preference for EE-DCR over external procedure. However, this was not statistically significant (P = 0.082)
Working in a multidisciplinary hospital where ENT could be involved, did not have an impact on the type of procedure or the decision to perform endonasal surgery P = 0.129
EE-DCR is found to be the first choice of treatment among those who operated more than 40 cases of endoscopic DCR during their training (P < 0.001).
We found an association between moderate to high surgical volume (>3 cases/week) and the tendency to perform EE-DCR Table 4.
Comparison between external and endoscopic DCR performers.
Discussion
External DCR was first described in 1904 by Adeo Toti. 5 It underwent several modifications until it reached the final external DCR known today. Caldwell described the first intranasal DCR in 1893. 6 However, it was considered impractical due to the difficult visualization of the endonasal anatomy with the instrumentation at that time. After the introduction of rigid nasal endoscopes, endoscopic endonasal DCR was described by McDonogh and Meiring in 1989. 7 Both external and endoscopic DCR have a good prognosis. However, endoscopic DCR has several advantages over external DCR, including the absence of an external scar and better visualization as a result of the development of the endoscopic monitor system.
In this survey, more than half of the respondents perform external DCR as a first-line procedure for primary nasolacrimal duct obstruction. Previous surveys about DCR preferences also reported a higher preference for external DCR.8,9 We also observed that those who preferred external DCR were trained to perform only this technique during their training. This could explain why they are more comfortable performing external DCR. The majority of endonasal DCR performers were trained in the 90 s. Also, a higher percentage of endonasal DCR performers have been in practice less than 10 years, indicating that endonasal DCR performers (both endoscopic and non-endoscopic) are relatively new practitioners. There is an increased interest in learning endonasal DCR. This is consistent with previous studies.8–10
Exposure to endoscopic endonasal DCR during training positively affected practitioners adopting this technique. More than half of participants who preferred this technique reported they received training on endonasal surgeries and two-thirds performed more than 20 cases during their fellowship. Furthermore, about 40% of participants received training on non-endoscopic endonasal DCR. However, no difference was noticed in their preferred technique, external vs endonasal. We found no statistically significant difference in the preferred technique based on where the surgeon work (academic vs. non-academic). However, there is a trend that more endonasal cases are performed in the academic sector (p-value = 0.07)
Endonasal DCR surgery requires a thorough knowledge of the intranasal anatomy since anatomical variations inside the nasal cavity are likely to affect the outcome of the EE-DCR surgery. 11 The presence of ENT specialist back up in the hospital would increase the number of surgeons performing EE-DCR as this might be useful to refer difficult patients with nasal pathologies and to manage post operative complications if present. However, our data showed that working in a multidisciplinary hospital with ENT backup available did not affect the decision to perform endonasal surgery.
Many factors influence the success rate of endoscopic DCR including age and presence of nasal pathology12,13 . In this survey, the decision to proceed with endoscopic DCR was mainly influenced by the patients’ request, followed by the endonasal exam. Gender of the patient did not affect the decision to perform endonasal surgery as stated by almost 85% of respondents. Barmettler et al also reported the patient's preference as the highest-ranked reason to perform EE-DCR. 8
21% consider the age of the patient before performing endonasal surgery. This consideration may be based on the concern for a noticeable scar in younger patients. Another consideration is that older age has been associated with a higher failure rate with external DCR. It has been postulated that this higher failure rate in older patients is due to a weak orbicularis muscle affecting the lacrimal pump 12 .Recent studies have demonstrated compromise of the facial nerve with external DCR incisions, which may further affect the lacrimal pump. 14 An advantage of an endoscopic DCR is the potential decreased risk to these branches of the facial nerve.
Regarding surgeon's preferences in DCR, 46% of participants do not use mitomycin C in first-time endoscopic DCR. This is in agreement with multiple level-1 evidence studies that demonstrate no benefit of MMC in terms of symptomatology and ostial patency for primary EE-DCR. 13 A small percentage of respondents use MMC in primary external DCR. MMC has been shown to be safe and effective in increasing surgical success rate in primary external DCR 15 . Gonzalvo et al studied the effects of intraoperative MMC on the clinical evolution and osteotomy size following an external DCR with helical computed tomography and reported that intraoperative MMC may increase the success rates over the traditional DCR. 16 Furthermore, a meta-analysis published in 2014 supported these studies. It concluded that intraoperative application of MMC increases the success rate in primary External DCR and revision EE-DCR, but does not provide any significant benefit in primary EE-DCR. 17
A stent helps keep the osteotomy site patent in the initial stages of healing and thus decreases the chance of early failure. Vishwakarma et al performed a prospective study on 272 patients to assess the effect of silicone stenting on the outcome of endoscopic dacryocystorhinostomy and found a higher success rate using a silicone stent.18,19 However, several studies have found no significant difference in surgical success between DCR done with stents and those done without.18,20–22 Even with the evidence that stent-free surgery results in good outcomes in DCR surgery, most of the performers of EE-DCR prefer placing a stent. An Indian survey showed that practitioners with less than 10 years of experience were more likely to place stents. 9 This could be due to the feared risk of mucosal adhesions or lack of awareness of these recent studies. Malhorta 2015 suggested that stenting during the early adoption period of endoscopic DCR may be of value as mucosal adhesions are anticipated. 21
Regarding barriers and potential facilitators for endoscopic DCR adoption, the lack of experience was the most common barrier to not performing endoscopic DCR. 42% of participants were not trained to perform endonasal surgery during their fellowship. Other barriers were limited visibility of the endonasal endoscope and difficulty manoeuvring instruments in a confined space. Giving more surgical training time to trainees and familiarizing them with nasal anatomy may help overcome these barriers.
Almost a quarter of participants reported that the lack of support and backup from an experienced oculoplastic surgeon or ENT specialist is a barrier to performing endoscopic DCR. Complications can be encountered during surgery, and thorough knowledge and experience are required.
Although surgeons with lower surgical volumes and limited technical proctorship might have concerns about being able to overcome the learning curve of endoscopic DCR, previous research shows that the initial learning curve may be overcome relatively easily after 30 cases of experience of endoscopic surgeries3,23 . This is consistent with our study which showed that those who performed 40 cases of EE-DCR during fellowship were more likely to perform this procedure after training.
Previous studies reported good success rates with a safety profile and efficacy equivalent to the traditional external approach. 24 The endoscopic DCR is also known to have a shorter operative time and a relatively lower complication rate. 24 However, concern for complications is one of the main obstacles encountered in the adoption of endoscopic DCR. Among the difficulties, the most problematic was risk of failure. This is followed by the risk of bleeding, injury to intraorbital structures, and injury to the skull base. Improving trainees’ awareness of these complications and providing guidance in the OR may help overcome this.
Most respondents agreed that mentorship and supervision are important facilitators for the adoption of endoscopic DCR. This was followed by initial training with ENT. Our study showed that those who were not trained to do endoscopic DCR during their fellowship were unlikely to perform endonasal surgery later. Kamal et al. recommended a structured training program through knowledge of nasal anatomy, clear demonstration of surgical steps, and supervision by experienced surgeons to result in efficient skills transfer. 4 The use of virtual reality simulators can create a computerized environment in which the anatomy is reproduced and interaction with endoscopic handling and realistic haptic feedback is possible. Moreover, scenarios can be presented that improve trainees’ skills and confidence. Wais et al found that the trainee pretrained on the cadaveric endoscopic sinus surgery (ESS) tasks performed better than the nonintervention (no pretraining) group. 25
Almost a quarter of participants believe video-based performance assessment would facilitate endoscopic DCR learning. Video-based coaching is an educational modality that is known to be beneficial as it targets intraoperative judgment, technique, and teaching. 26 Reviewing surgery footage can be useful in identifying areas of difficulty and minimizing repeating the same mistakes. Posture training, instrument handling, avoiding multiple entries, and paying special attention to the superiorly placed bone overhanging the ostium are some of the feedback points that Malhotra et al. have enumerated in their list of tips for the trainee and trainer in En-DCR. 21
Limitations and future studies
Survey-based studies have inherent limitations. The cross-sectional study design is also a limitation. The length of the survey might have affected the response rate. Poor participation from the Eastern countries might been due to language barrier. Future studies using simulators among oculoplastic surgeons and the efficacy of video-based teaching may be beneficial.
Conclusions
Exposure to and learning endoscopic DCR early during fellowship training dramatically impacts the adoption of the procedure. Thorough knowledge of the nasal anatomy and supervision by an experienced surgeon is essential in learning the technique and overcoming the learning curve. Implementing video-assisted training and simulators may have a positive role in learning the procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
DCR preferences among Oculoplastic Surgeons
We appreciate the time you are taking out of your busy schedule to fill out this questionnaire.
*Required
Do you agree to participate in this study? * Mark only one oval.
Yes No 1- Age: *
30–39 40–49 50–59 60 and plus 2- Gender: *
Male Female 3- Region of practice: * Mark only one oval.
North America South America Europe Africa Middle East Asia/ Asia-Pacific Australia Other: ……………………………Please Specify the country: * 4- Area of practice: * Mark only one oval.
Urban Suburban Rural 5- Type pf practice: * Mark only one oval.
Governmental hospital Public Private hospital/ Clinic Charity Hospital 6- You are working in. ……… * Mark only one oval.
Academic sector Non-academic sector 7- Where are you practicing oculoplastic* Mark only one oval.
Multi-speciality hospital or clinic (general hospital) Specialized eye centre Solo (private clinic) 8- How do you describe the surgical volume in your hospital? * Mark only one oval.
2 or less than 2 cases of DCR/week 3–5 DCR cases/week 6–10 DCR cases/week 11–20 DCR cases/week >20 DCR cases/week 9- Type of training after residency: * Mark only one oval.
Formal training (fellowship in Oculoplastics) Formal training in Rhinology Formal training both (Oculoplastic and Rhinology) Non-formal training in Oculoplastics Non-formal training in Rhinology Non-formal training in both (Oculoplastic and Rhinology) Other: 10- Area of training: * Mark only one oval.
North America South America Europe Africa Middle East Asia/ Asia-Pacific Australia 11- Duration of training: * Mark only one oval.
1–6 months 7–12 months 13–18 months 19- 24 months more than 24 month Didn't receive formal training 12- Period of training: * Mark only one oval.
70's 80's 90's 2000 and later 13- Exposure to DCR cases during training: * Mark only one oval.
External DCR only Endoscopic Endonasal DCR only Non-Endoscopic Endonasal DCR Both External and Endoscopic External, Endoscopic and Non-Endoscopic endonasal No DCR exposure 14- During your training, how many cases of Endoscopic Endonasal DCR did you perform? (total) *
<20 cases 20- 40 cases >40 cases none 15- During your training, how many cases of Non-Endoscopic Endonasal DCR did you perform? (total) *
<20 cases 20- 40 cases >40 cases none 16- During your training, how many cases of External DCR did you perform? (total) *
<20 cases 20- 40 cases >40 cases none 17- Since when are you practicing Oculoplastic(years after residency) * Mark only one oval.
<5y 5–10y >10y 18- In your practice, which technique do you consider as first line procedure to manage nasolacrimal obstructions? * Mark only one oval.
External DCR Non-Endoscopic Endonasal DCR Endoscopic Endonasal DCR No preference I don't perform DCR 19- Among all DCR cases, what is the percentage of endonasal DCR surgeries performedMark only one oval.
1–25% 26–50% 51–75% 76–100% I don't perform endonasal surgeries 20- Since when are you performing External DCR? * Mark only one oval.
<10 years 10 years and more I don't perform external DCR 21- Since when are you performing Endoscopic Endonasal DCR? * Mark only one oval.
< 10 years 10 years and more I don't perform endoscopic DCR 22- Since when are you performing Non-Endoscopic Endonasal DCR? * Mark only one oval.
< 10 years 10 years and more I don't perform non-endoscopic endonasal DCR 23- Your decision to perform Endoscopic DCR is based on: * Tick all that apply.
Gender of patient Age of the patient Patient request Endonasal exam I don't perform endoscopic DCR Other: ……………. 24- Do you perform endonasal surgeries: * Mark only one oval.
Alone as a main surgeon I am the main surgeon with the assistance of the ENT The ENT does the endoscopic part and I do the lacrimal probing and intubation Not applicable 25- Do you use mitomycin when performing endonasal DCR? * Mark only one oval.
Yes No Only in re-do cases Not applicable 26- Do you use mitomycin when performing external DCR? * Mark only one oval.
Yes No Only in re-do cases Not applicable 27- Do you use stent when you perform an endonasal DCR surgery? * Mark only one oval.
Yes No Only in re-do cases Not applicable 28- Do you use stent when you perform an external DCR surgery? * Mark only one oval.
• No • Only in re-do cases Not applicable 29- If your answer to the previous question was “yes, I use stent in endonasal DCR,” how lon after surgery the stent is removed? * Mark only one oval.
One month Two months Three months Six months One year Variable Not applicable 30- If your answer to the previous question was “yes, I use stent in external DCR,” how long after surgery the stent is removed? * Mark only one oval.
One month Two months Three months Six months One year Variable Not applicable 31- If you routinely use both techniques, which one do you feel results in a better outcome? Mark only one oval.
External Endoscopic Both similar Not applicable 32- If you are performing External and Endonasal DCR, with which one do you feel you face more complications? * Mark only one oval.
External Endoscopic Both similar Not applicable 33- Are the facilities for performing Endonasal DCR available at your hospital? * Mark only one oval.
Yes No 34- In your opinion, which one of the following is considered as a barrier for not performing endonasal DCR? (Tick all that apply) *
Insufficient time to learn Insufficient resources/support Lack of experience Steep learning curve Worried about complications Limited visibility of endoscopic DCR Worried about the surgical outcome Was not trained during fellowship No courses in my region Investment to acquire instruments for surgery very high for a small number of procedures availab Facilities for performing endoscopic DCR are not available in my place Lack of experienced back up Difficulty achieving dexterity and instruments maneuvering within the confined space of nasal cavity. I am not interested in endoscopic DCR because my results with external are good. Other: ……………………….. 35- In your opinion, the surgical success rate of endoscopic DCR compared to external DCR Mark only one oval.
higher lower equal 36- Compared to external DCR, I find endoscopic DCR: * Mark only one oval.
easier than external DCR more difficult same not applicable 37- What are the complications you are worried about when performing Endoscopic DCR? Mark only one oval.
Bleeding Failure / non patent lacrimal system Silicon tube displacement Injury to the orbital structures Injury to skull base Other: …………………. 38- In your opinion, which of the following facilitate endonasal DCR training? (Tick all that apply) *
Surgical mentorship/ supervision during initial cases High surgical volume to improve the learning curve Initial training with an ENT (ear, nose, and throat) surgeon to familiarize with nasal anatomy and endoscope Additional data to highlight non-inferiority of endoscopic compared to external DCR Surgical simulation for improving endoscopic DCR skills Wet lab / Cadaveric session Video-based performance assessment (self assessment or by experts) I have no interest in endoscopic surgery Other: …………………………..