
Abstract
Purpose
To describe a case of ocular Lichen Planus, successfully managed using a multimodal evaulation, including Anterior Segment OCT (AS-OCT).
Observations
A female patient in her forties with a history of cutaneous Lichen Planus presents with blurred vision and burning eye sensation. Anterior segment evaluation revealed bilateral punctate keratitis, stromal haze and subepithelial pigmented dots. AS-OCT was pivotal for diagnosis, showing anterior stromal hyperreflective dots. A diagnosis of ocular Lichen Planus was estabilished and the patient was treated with topical hydrocortisone, with complete subsidence of the complaints.
Conclusions and Importance
Ocular Lichen Planus can present as isolated corneal involvement independent from severe cicatrizing conjunctivitis. Appropriate and timely treatment can prevent irreversible ocular surface disease. Ophthalmologists should be aware of Lichenoid Tissue Reaction (LTR) disorders, especially in patients with relentless blepharitis and/or ocular surface disease.
Keywords
Introduction
Lichen Planus (LP) is a chronic inflammatory mucocutaneous disease presumably T-cell mediated, characterized by disruption of the epithelial anchoring system due to keratinocyte apoptosis and hemidesmosome destruction. 1 LP is often overlooked, in part due to its clinical diversity and waxing-waning disease activity. It can be subdivided according to its disease location: cutaneous LP manifests as pruritic violaceous papules and plaques on the extremities and mucosal LP which is characterized by sores and erosions frequently on the oral mucosa, followed by genitalia and, rarely, ocular surface. Although LP usually manifests as mild, self-limiting, recurrent episodes of cutaneous/mucosal inflammation, in some cases, scarring and hyperpigmentation eventually develops. 2
Ocular involvement from LP is rare and usually presents with concomitant mucous/cutaneous manifestations. 3 Hence, the diagnosis is frequently delayed and usually made by the dermatologist, rheumatologist or oral surgeon, not by the ophthalmologist. Nevertheless, LP may cause significant and irreversible changes in the integrity of the ocular surface such as symblepharon, corneal neovascularization and lacrimal drainage stenosis. 3
Corneal epithelial lesions, although rare, are often accompanied by conjunctival cicatrization. Therefore, it was not clear whether keratitis is a primary or secondary manifestation of the disease.2,3
We present a case of ocular LP in which timely diagnosis was made with multimodal imaging with Anterior Segment Optical Coherence Tomography (AS-OCT) with successful management of disease activity.
Case description
A female patient in her forties presented in the ER with burning eye sensation, photophobia and decreased vision bilaterally for 2 days. She denied ocular discharge, epiphora, other systemic symptoms or any similar previous episodes. The patient had been diagnosed LP for the last 5 years, with ocasional (once a year), self-limiting episodes of pruritic violaceous plaques in the wrists and abdomen, the last of which ocurred in the previous week to her visual complaints. Systems revision and past medical history were noncotributory.
At presentation, the Best Corrected Visual Acuity (BCVA) was 20/30 in both the right eye (RE) and left eye (LE). Mild scarring on the wrists and lower abdomen were observed. Slit-lamp examination showed central anterior stromal haze and multiple subepithelial pigmented dots bilaterally. On fluorescein staining, there were multiple small, round epithelial defects, some of which coalesced, but no dendritic/pseudodendritic fluorescein positive lesions (Figure 1 and 2). There was no conjunctival hyperemia, no significant papillar/follicle reaction, no scarring on both bulbar and tarsal conjunctiva and the cilia were normally implanted and dark. Fundus examination was unremarkable.
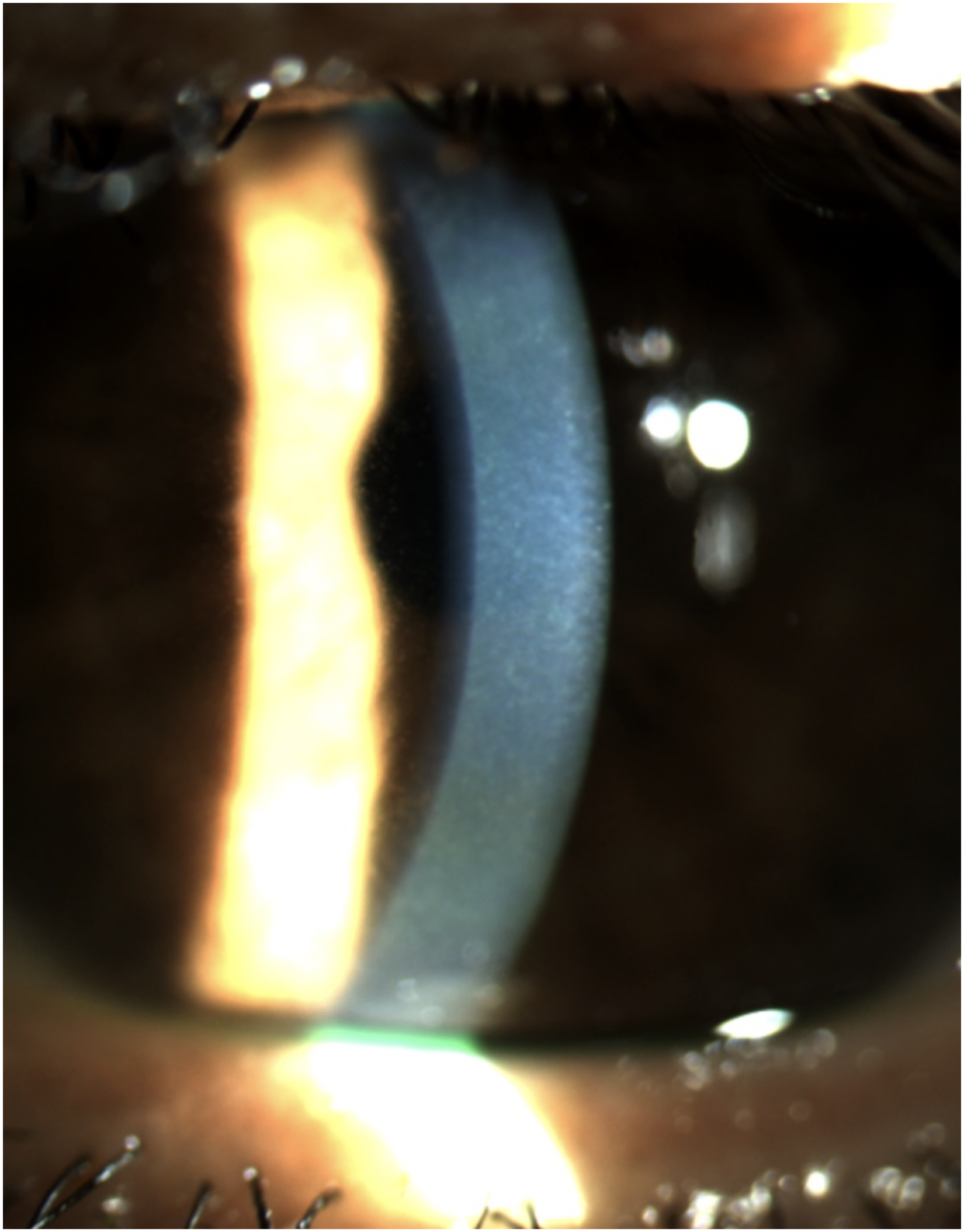
Central anterior stromal haze.
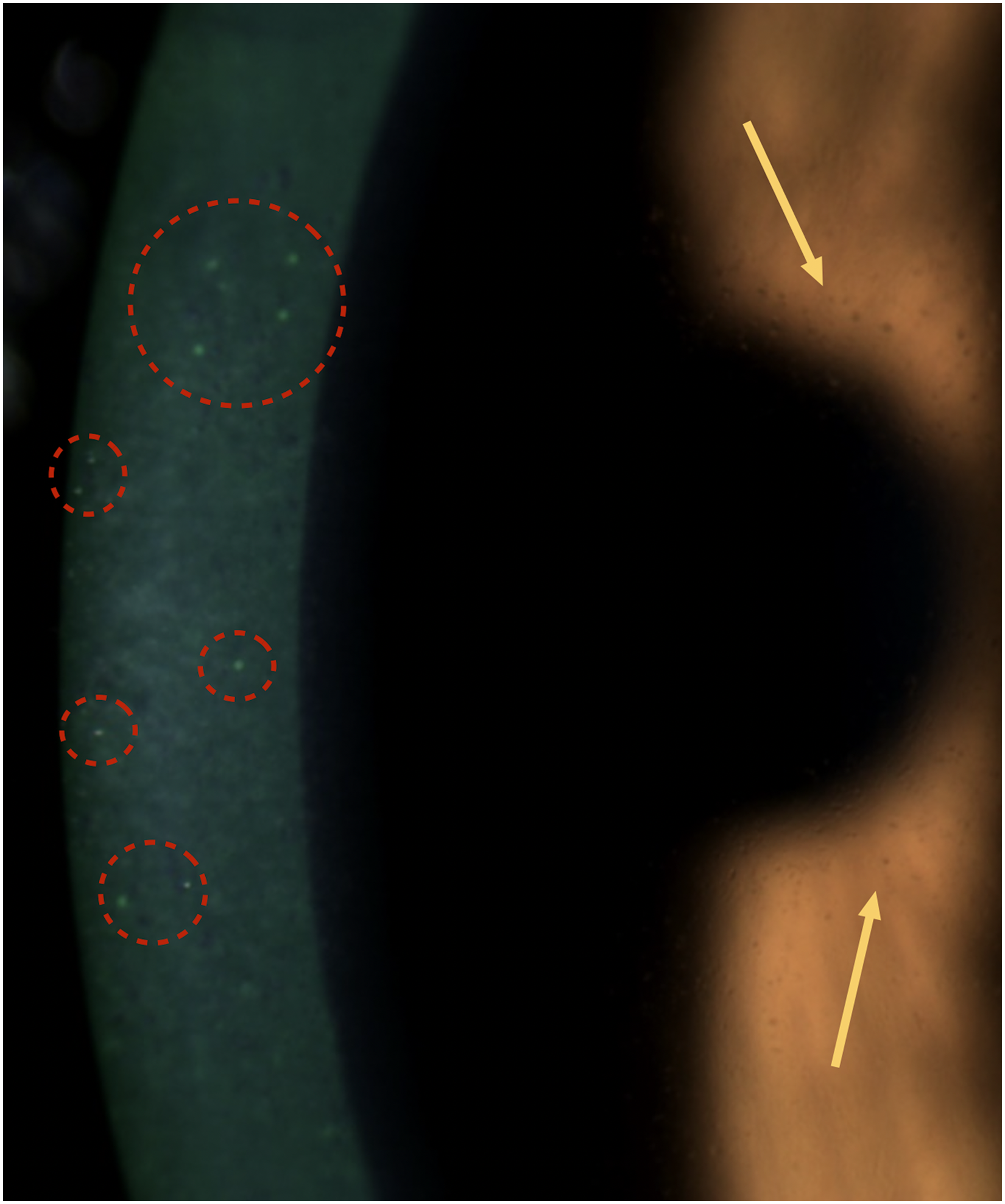
Multiple small, round fluorescein-positive epithelial lesions (circles) and multiple subepithelial pigmented dots (arrows).
Intraocular pressure (IOP), measured using Goldman's applanation tonometry, was 20 and 22 mmHg, in the RE and LE, respectively.
Complete multi-modal approach was undertaken.
Pachymetry for central corneal thickness was 573 µm in the RE and 579 µm in the LE and Specular Microscopy revealed no abnormalities of the Descemet/Endothelium Complex, with an endothelial cell count of 2205 and 2337 in the RE and LE, respectively.
AS-OCT revealed bilaterally epithelial irregularity and scattered, granular hiperreflectivity in the central anterior stroma. There were no abnormalities in the posterior stroma or the Descemet membrane/Endothelium complex (Figure 3).
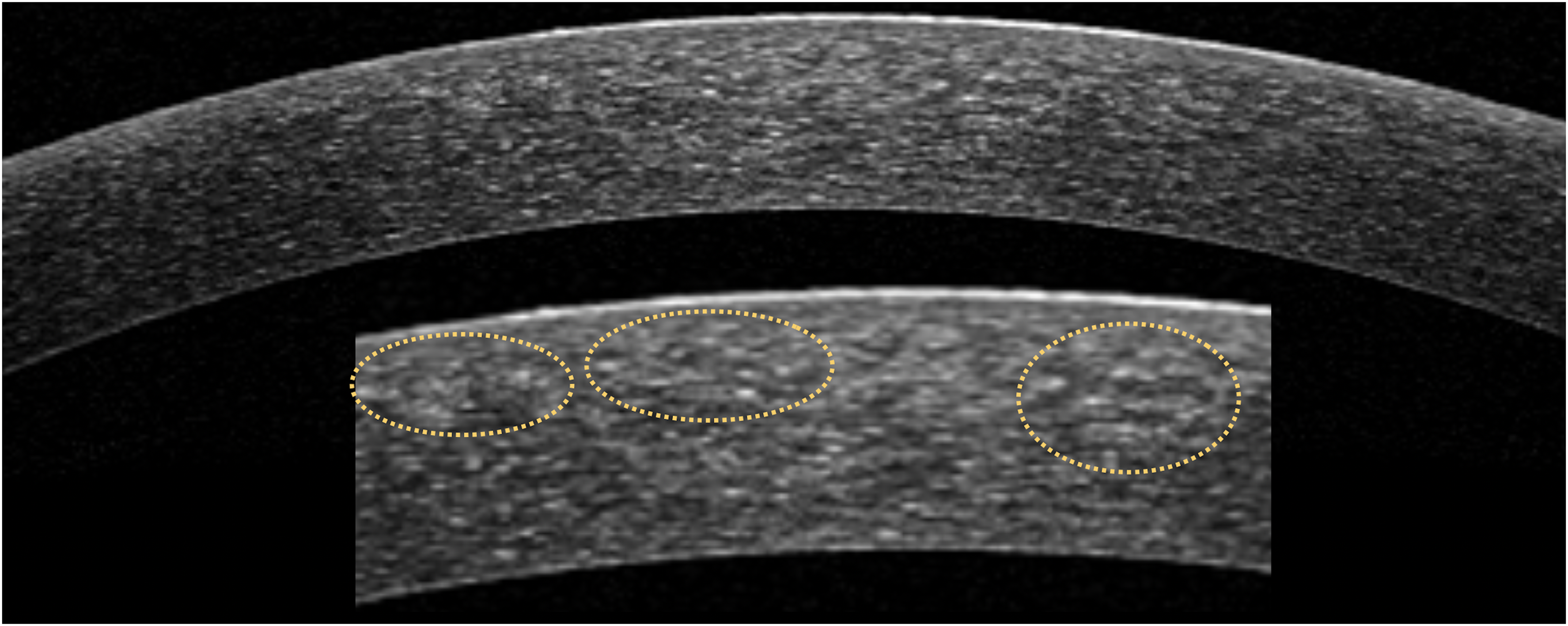
AS-OCT: epithelial irregularity and scattered, granular hyperreflectivity, specially in the central anterior stroma (circles on close-up below).
Differential diagnosis included conditions causing bilateral epithelial punctate keratopahty and stromal haze.
Adenoviral keratoconjunctivitis usually presents unilaterally but affects both eyes in up to 70% of cases. It usually presents with conjunctival hyperemia, chemosis, follicular reaction, which were not present in our patient. In more severe cases, diffuse epithelial keratitis may precede the development of multifocal subepithelial infiltrates, regarded as pathognomonic. 4 In contrast, we did not find clusters of subepithelial infiltrates surrounding epithelial punctate lesions, but rather diffuse haze of the anterior central stroma.
Herpes simplex/zoster epithelial keratitis manifests in the first 12-24 h as punctate epithelial keratopathy, eventually leading to the characteristic dendritic ulceration or pseudodentritic lesion, respectively. In some cases, the punctate epithelial keratopahty persists with recurrent epithelial erosions and/or granularity, with underlying anterior stromal haze. Although bilateral disease is possible, such presentation seemed unlikely in our patient without prior history of herpetic eye disease, without any dendritic or pseudodentric lesion ever noted, and with significant clinical improvement with only topical corticosteroids (and no anti-viral). In addition, for Herpes Zoster Ophthalmicus, there were no typical prodrome signs such as fever, malaise or headache prior to skin rash (papules, macules, vesicles, pustules and/or crusting along the distribution of the trigeminal nerve). 5
In Thygeson's superficial punctate keratitis, most patients (62.7%) present with recurrent, bilateral disease, with very few having only unilateral disease, usually beginning in the third or fourth decade of life with slight female predominance. During the active keratitis phase, the characteristic intra-epithelial lesions are multiple, coarse, oval-shaped and slightly raised white/grey lesions, which stain minimally with fluorescein, without conjunctival hyperemia and no to minimal subepithelial edema. During the inactive, chronic phase however, these granular lesions flatten, appearing as gray subepithelial opacities that stain negatively with fluorescein. 6 In contrast, our patient did not show such slightly raised typical white lesions. In fact, there were multiple punctate, fluorescein positive lesions with underlying anterior stroma edema.
Fintelmann et al reported AS-OCT features of Thygeson's, showing increased reflectivity of the anterior stroma just beneath the hyperreflective intraepithelial lesion, suggesting scarring form chronic inflammation associated with prolonged disease activity. 7 In contrast, our patient showed in the AS-OCT no hyperreflective intra-epithelial lesion and a rather scattered, granular anterior stroma edema, predominantly in the central cornea, which resolved with corticosteroid therapy, suggesting acute inflammation instead of scarring formation.
The patient was started on topical hydrocortisone sodium phosphate 0.335% four times daily.
Three weeks later, the patient revealed gradual and progressive improvement of photophobia and burning eye sensation. BCVA improved to 20/25 in the RE and 20/20 in the LE. Slit-lamp examination showed a reduction in the number and size of the fluorescein positive epithelial lesions, resolution of pigmented subepithelial dots and minimal anterior stromal edema in the RE. Topical hydrocortisone was slowly tappered in the following 3 weeks.
Final evaluation was made 6 weeks after presentation, with total resolution of symptoms and BCVA of 20/20 in both eyes. At slit-lamp examination there were no fluorescein positive lesions and no residual anterior stromal edema (Figure 4). Pachimetry, Specular Microscopy and IOP were similar to the initial presentation and AS-OCT imaging revealed no residual corneal abnormalities in both eyes. We decided to tapper hydrocortisone drops to 1 time daily for another week. Subsequently, the patient was mantained on eye lubricant without relapsing episodes to date.
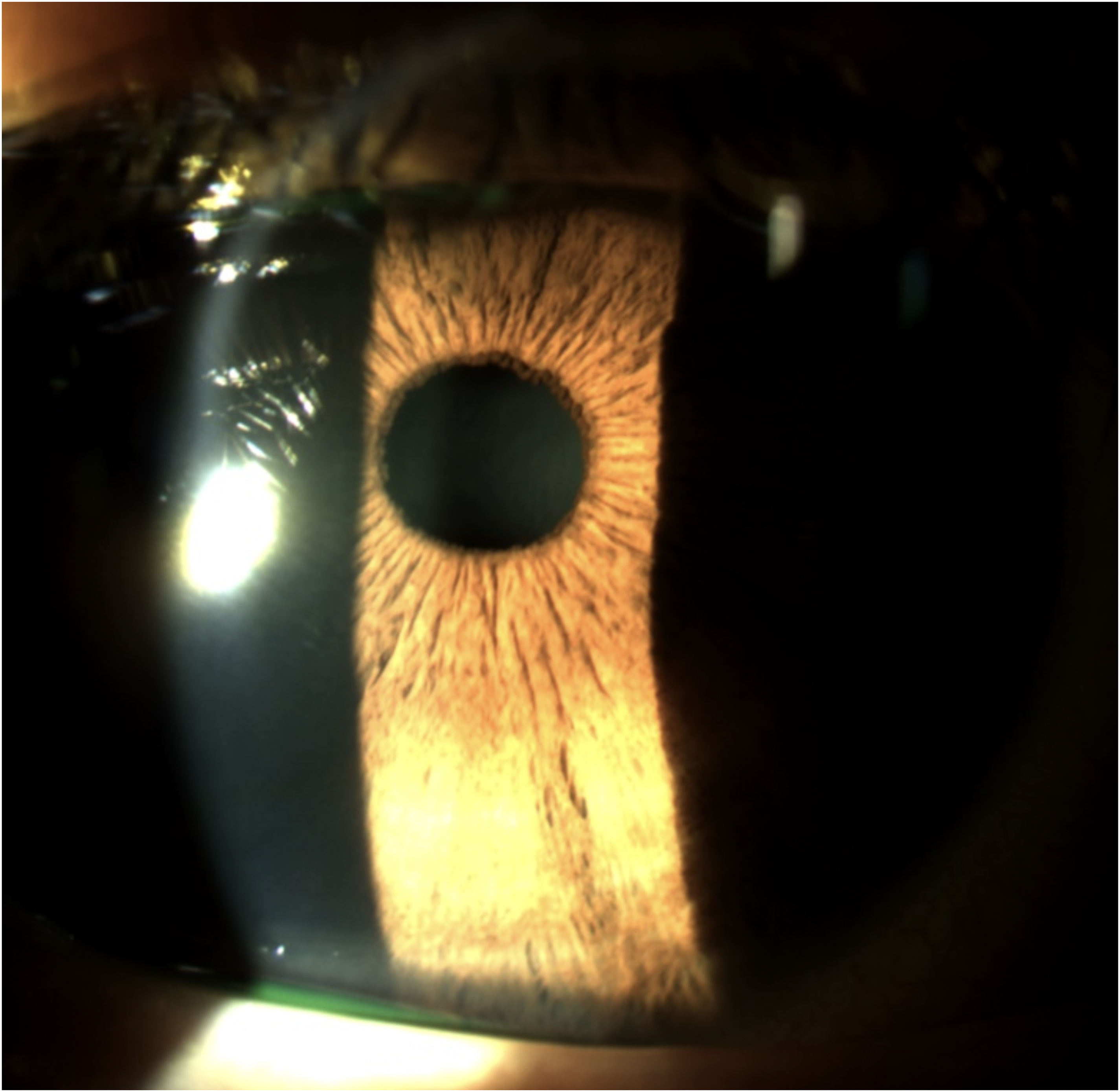
Complete resolution of both stromal haze and subepithelial pigmented dots.
Conclusions
With this case report, we describe a novel multimodal approach for ocular LP using AS-OCT to localize and characterize corneal inflammatory pigmented lesions. In addition, to our knowledge, this is the first reported case in the English literature with isolated corneal disease from LP that was treated solely with topical steroid.
Ocular involvement from LP is rare and usually preceded by oral/cutaneous manifestations. The most common findings include cicatrizing conjunctivitis, followed by lacrimal drainage stenosis, and rarely corneal involvement. Chronic cicatricial conjunctivitis leads to fornix shortening and symblepharon. Lacrimal drainage stenosis usually presents as severe, bilateral and proximal obstruction of punctata, with patients complaining of epiphora.2,3
Despite using oral corticosteroids, topical cyclosporine and/or amniotic membrane transplant, the prognosis of ocular surface disease from LP is usually poor.2,3
However, there may be literature selection bias, as usually only patients with more severe ocular surface disease are investigated thoroughly for concomitant inflammatory mucocutaneous disease. Hence, more subtle presentations of ocular LP may be unrecognized and therefore not reported in the literature. 2
Our patient was previously diagnosed with mild LP, for which there was no need for chronic oral or topical corticosteroid therapy. She mentioned infrequent (once a year), self-limited episodes of cutaneous pruritic papules in the lower abdomen. The concomitant timing of the cutaneous inflammatory flare and the ocular complaints lead us to consider the possibility of ocular involvement by LP. The bilateral, symmetric ocular involvement, with widespread, coalescent, fluorescein-positive lesions, subepithelial pigmented dots and central anterior stromal edema were suggestive of an underlying widespread inflammatory process such as LP.
Corneal involvement from LP, albeit rare, is accompanied by conjunctival cicatrization in most cases. Therefore, previously it was not clear whether keratitis is a primary manifestation or secondary to conjunctival involvement of the disease.2,3
Our patient did not show cicatrizing conjunctivitis that would otherwise justify the punctate keratitis and anterior stromal haze. Hence, there was primary corneal disease from ocular LP.
Similar to our patient, Soleimani et al reported direct corneal involvement from LP Pigmentosus, with an accumulation of pigment in the corneal epithelium (confirmed by Confocal Microscopy), treated with topical fluorometholone 0.1% every 6 h and topical cyclosporine 2% two times a day. 8 In contrast to our patient however, they identified multiple pigmented dots scattered on the bulbar conjunctiva and lid margins and punctate epithelial erosions from severe dry eye disease.
In our patient, there was only inflammation in the anterior corneal stroma, confirmed by AS-OCT, for which a topical corticosteroid with high intraocular penetration such as dexamethasone or prednisolone would be unnecessary with undesirable side effects.
Topical hydrocortisone at 0.335% is a low-potency corticosteroid that is frequently used for chronic dry eye disease, improving Ocular Surface Disease Index (OSDI), conjunctival hyperemia and increasing tear film thickness, while not increasing IOP due to its low intraocular penetration. Hence, topical hydrocortisone at 0.335% is an effective steroid for ocular surface inflammation with a good safety profile, 9 therefore being an excellent option for the T-cell infiltrative response and vacuolar epithelial changes, typical from LP histological studies, before the development of irreversible fibrotic changes.
In fact, our patient had a prompt and full response to this topical steroid, completely resolving the anterior stromal edema, epithelial punctante keratitis and subepithelial pigmented deposits.
AS-OCT has been increasingly used to evaluate ocular surface and corneal diseases such as keratitis, corneal dystrophies and degenerations. Although these diagnosis are clinical, AS-OCT is particularly helpful in quantifying corneal disease, grading its severity and monitor progression. In addition, AS-OCT can provide valuable information regarding the extent and location of subtle corneal changes, which can be difficult to ascertain at the slit-lamp. 10 For instance, in Thygeson's keratitis, AS-OCT is currently an important aid in differential diagnosis, demonstrating characteristic intra-epithelial lesions, guiding its proper management, which is distinct from initially identical diseases such as infectious keratitis. Our case suggests a similar value of the AS-OCT for ocular LP which is usually diagnosed once irreversible ocular surface disease have developed, presumably due to unrecognized progression of mild ocular surface signs.
In ocular LP, AS-OCT identified distinct hyperreflective subepithelial and anterior stromal lesions, which guided the selection of the appropriate topical corticosteroid, preventing disease progression and halting comorbidities. In addition, AS-OCT can be important for disease monitoring, revealing progressive resolution of those characteristic finding with topical corticosteroid. To date, the reported patient did not experience any relapse. Hence, it is still uncertain whether AS-OCT has diagnostic value for identification of subclinical inflammatory activity.
In conclusion, ocular complaints from muco-cutaneous inflammatory conditions such as LP are often overlooked by the ophthalmologists or misdiagnosed as primary dry eye disease with failed treatment response. In patients with relentless blepharitis and unexplained conjunctival inflammation, specially when considering refractive surgery, LTR disorders should be investigated, in conjunction with Dermatology and/or Rheumatology. Even mild ocular symptoms due to LP may preclude LASIK or other corneal refractive surgery, due to the risk of subsequent severe dry eye, corneal melt and potentially corneal perforation. Accordingly, in the pre-operative period, refractive surgeons should be aware of coexisting autoimmune conditions, mucosal/cutaneous symptoms and medications that cause LTR. 11
This article provides new insights on primary corneal involvement from LP without significant conjunctival abnormalities. Furthermore, this is the first case report in the English literature showing typical corneal changes of ocular LP on AS-OCT and successful treatment with only topical steroid.
Footnotes
Authorship
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author's statements
We confirm that Ethical Committee approval was sought and that international guidelines on patient consent have been met.
We confirm that there are no conflict of interest or external funding to be disclosed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This publication complied with the World Medical Association Declaration of Helsinki and conformed to the ICMJE Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals.
Funding
No funding to disclose.
Statement of authorship
Category 1:
Conception and design: M. Leitão, D. Cabral; Acquisition of data: M. Leitão, D. Cabral; Analysis and interpretation of data: M. Leitão, D. Cabral; Drafting the manuscript: M. Leitão, D. Cabral; Revising it for intellectual content: M. Leitão, D. Cabral; Final approval of the completed manuscript: M. Leitão, D. Cabral;
Category 2:
Category 3:
Publication originality statement
This publication is original.