
Abstract
Introduction
Bilateral acute iris transillumination (BAIT) is a relatively new syndrome whose etiopathogenesis is still not fully understood. It is characterized by acute bilateral onset of intense pigment dispersion in the anterior chamber, iris depigmentation with severe transillumination defects, accentuated pigment deposition in the angle, and elevated intraocular pressure (IOP). In literature, the first case was of bilateral acute iris depigmentation (BADI) reported in 2004 in a 77-year-old woman. In 2019, Perone et al. published a review about BAIT syndrome. They reported a total of 79 cases have been published up that date, mainly in Europe and especially in Turkey and Belgium. The majority of reported cases were of bilateral acute iris depigmentation (BADI). BAIT syndrome might be mainly confused with acute iridocyclitis, acute primary angle-closure (APAC) and pigment dispersion syndrome (PDS). In relation to BAIT, controversies still exist regarding the etiology being the differential diagnosis of paramount importance for adequate treatment.
Purpose
To report a case of BAIT syndrome associated to refractory glaucoma and to discuss the differential diagnosis based on clinical, OCT and UBM findings.
Methods
We present a case of BAIT syndrome in which clinical, OCT and UBM findings have pointed out the similarities and, mainly the diagnosis differences with other ocular diseases.
Conclusions
BAIT syndrome with accentuated IOP rise must be differentiated of other ocular diseases. It requires urgent clinical therapy and/or surgical management as occurred in the present case for avoiding structural damage in OCT and visual field loss. OCT and UBM are critical for early recognition, differential diagnosis and management.
Keywords
Case description
A 42-year-old man consulted one of the authors (CCC) in December 27th, 2019, claiming sudden redness, pain, photophobia and blurred vision in both eyes (OU).1–7 Best corrected visual acuity (BCVA) was 20/25 in right eye (OD) and 20/40 in left eye (OS). He had no previous history of any ocular disease but used moxifloxacin 800 mg once daily for ten days for treatment of an episode of sinusitis before the onset of ocular symptoms. Slit-lamp examination revealed symmetrical bilateral findings in OU of circumferential dusting of pigment on the surface of the anterior crystalline lens capsule (Figure 1, left), intense pigmented flare (4+) in the anterior chamber (Figure 1, center), extensive and circumferential iris transillumination defects along with fixed mid-dilated pupils related to a paralysis of the iris sphincter (Figure 1, rigth). Intraocular pressure (IOP) was 40 mmHg in OU. Gonioscopy revealed in OU an wide-open angle with intense pigment deposition in the trabecular meshwork. Posterior ocular segment examination has not presented vitreous cells. On that occasion, the attending ophthalmologist suspected of pigmentary glaucoma (PG) and prescribed a fixed combination of 0.5% timolol maleate, 2% dorzolamide hydrochloride and 2% pilocarpine twice a day, topical steroids t.i.d and oral valacyclovir 2000 mg per day for 2–8 weeks. The patient returned in the following day presenting IOP of 6 mmHg in OD and 20 mmHg in OS. Axial length equal to 24.6 mm in OU and central corneal thickness (CCT) of 558 µm in OD and 552 µm in OS.
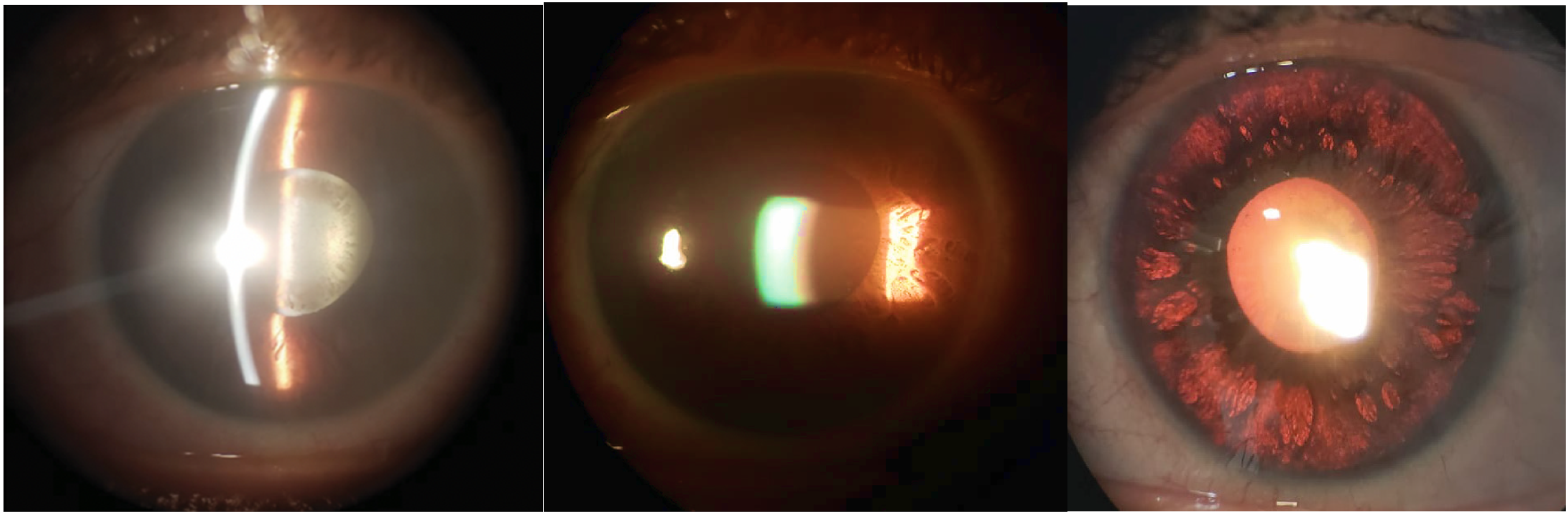
Both eyes illustration. Left: circumferential dusting of pigment on the anterior crystalline lens capsule; Center: intense pigmented flare; Right: circumferential iris transillumination defects and fixed mid-dilated pupil.
Ultrasound biomicroscopy (UBM)
Figure 2 shows through UBM the measurements of CCT, anterior chamber depth, angle and area of contact iris-crystalline lens. We found a deep anterior chamber, wide-open angle, reduced iris thickness and a large area of contact iris-crystalline lens.
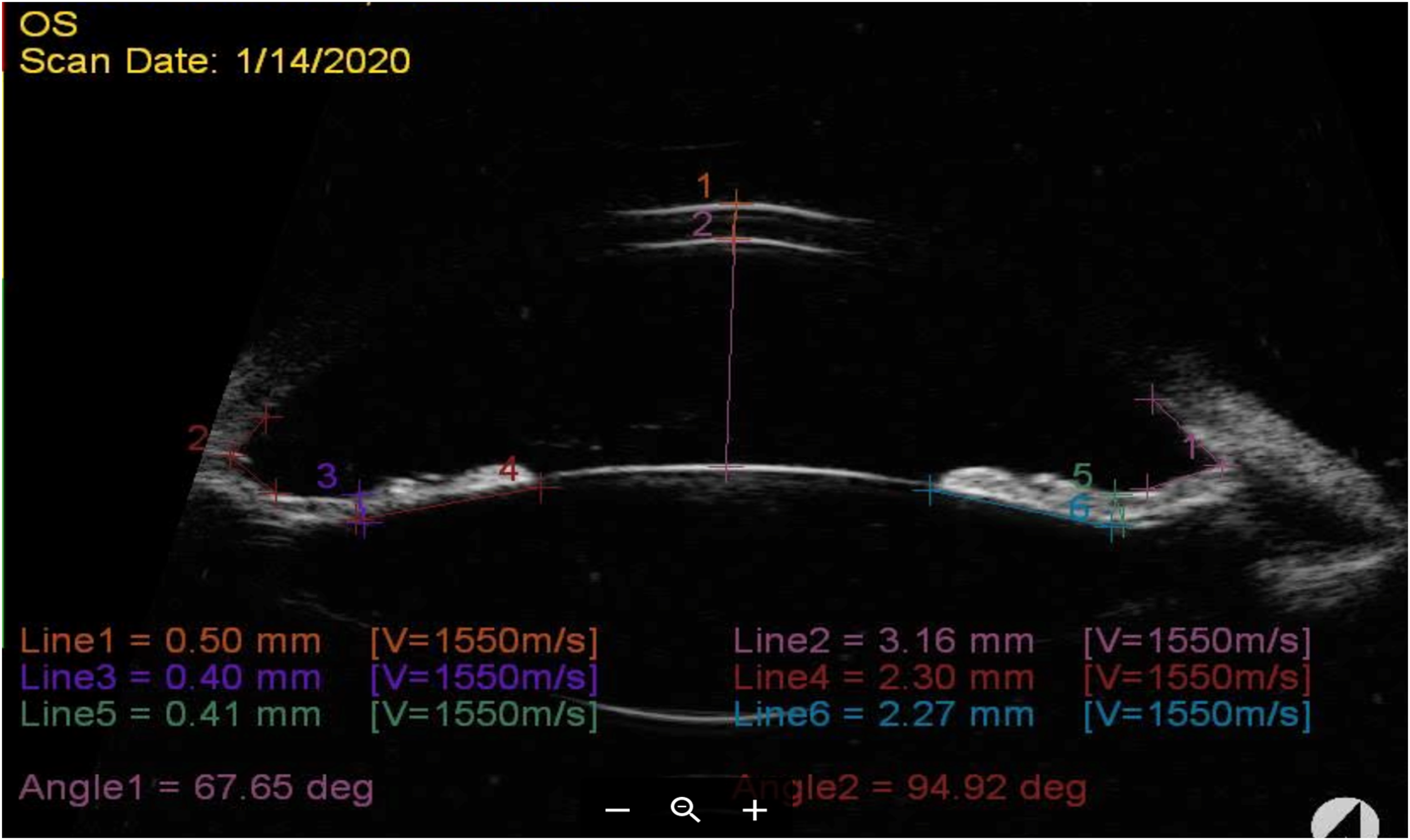
UBM image showing measurements of the central corneal thickness (0.50 mm), anterior chamber depth (3.16 mm), open angle distance (angle 1 = 67.65 degrees; angle 2 = 94.92 degrees), iris thickness (left = 0.40 mm and right = 0.41 mm) and area of contact iris-crystalline lens (left = 2.30 mm and right = 2.27 mm).
Visual field (VF) and optical coherence tomography (OCT)
Standard automated perimetry (SAP, 24-2 test) performed six weeks after presentation showed extensive involvement, especially of the upper hemifield, in OU (Figure 3(a), upper left).
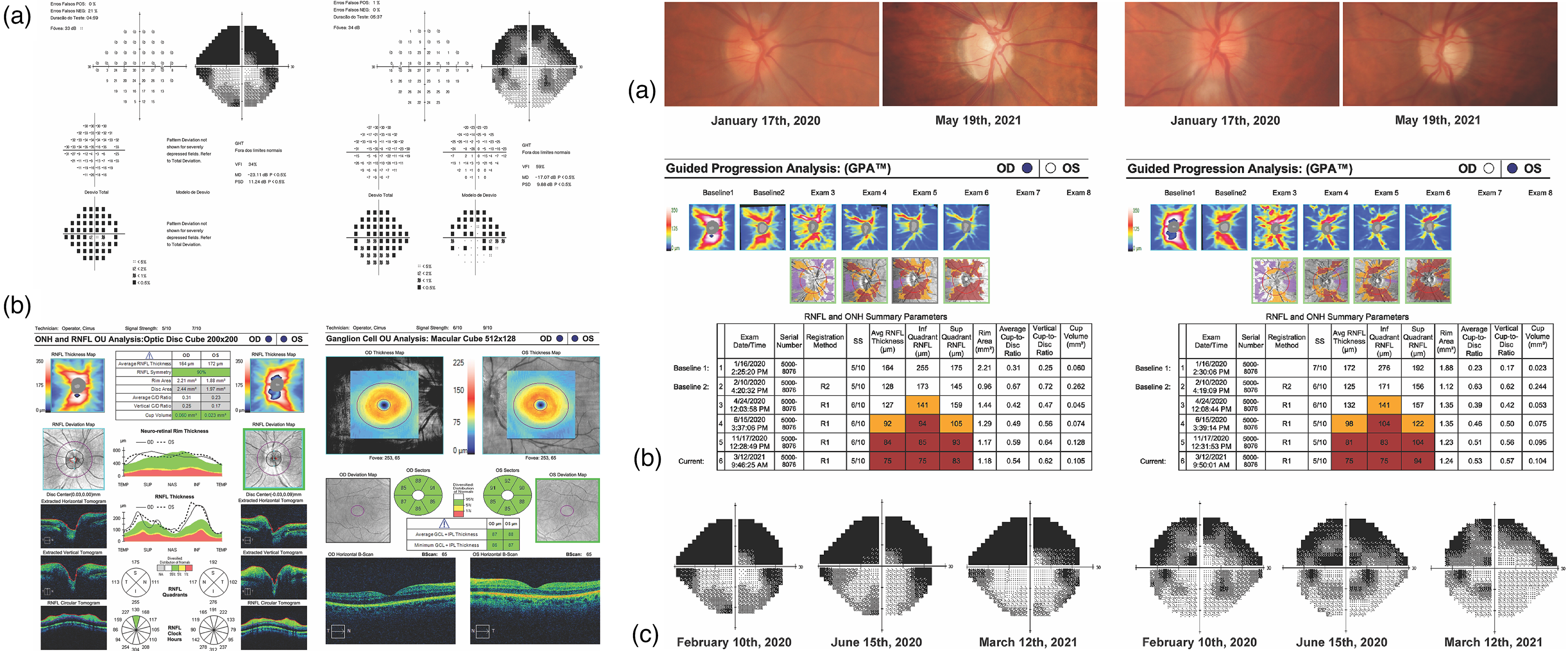
(a), upper left: SAP 24-2 test performed 6 weeks after presentation showed extensive involvement, especially of the upper hemifield, in OU; (a), upper right: retinographies over time: at January 17th 2020 the disc borders were blurred with peripapillary cotton wool spots, and poorly-defined cup/disc ratios. (b), bottom left: OCT showed increase in neuroretina rim and of RNFL thicknesses and preserved ganglion cell complex thickness; (c), bottom right: visual fields over time: the first exams presented major visual field loss mainly because of circumferential dusting of pigment on the anterior crystalline lens capsule.
Figure 3 depicts the follow-up of OCT from January 17th, 2020 to May 19th, 2021 and of the visual fields from February 10th, 2020 to March 12th, 2021.
OCT showed increase in neuroretina rim and peripapillary retinal nerve fiber layer (RNFL) thicknesses and preserved ganglion cell complex thickness in OU (Figure 3(a), bottom left). Fundus photography showed blurred disc borders, peripapillary cotton wool spots, and poorly-defined cup/disc ratios (Figure 3(a), upper right).
Two days after, the patient returned with intense ocular pain again associated with IOP of 40 mmHg in OU. Intravenous mannitol (20%) was then administered and patient was kept on 0.5% timolol maleate and 0.2% brimonidine tartrate and, 250 mg of acetazolamide orally every 6 h. Pilocarpine was discontinued and 0.005% latanoprost was initiated.
Despite therapy, IOP increased to 48 mmHg in OU and slit-lamp examination revealed persistent and symmetrical pigment dispersion in OU. At that point, ophthalmoscopy was unchanged in OD and was inviable in OS due to media opacity. The following day, worsening of intense flare was noticed in the anterior chamber of OU.
Review of systems was unremarkable apart from an upper respiratory tract infection 10 days before onset of ocular symptoms. The patient underwent laboratory evaluation, including complete blood count, erythrocyte sedimentation rate, liver enzymes, chest X-ray, anti-nuclear antibodies and rheumatoid factor, C-reactive protein, tuberculin skin test, blood and urinary calcium, angiotensin-converting enzyme, and lysozyme. Serological tests were negative for syphilis and for cytomegalovirus and positive (IgG antibodies with no IgM for toxoplasmosis, HSV and VZV). PCR of aqueous humor was not possible.
Since IOP was not controlled despite maximum ocular therapy, trabeculectomy with mitomycin C was performed in OS and, two weeks later, in OD. IOP gradually decreased throughout the second and third months, and postoperative medications were gradually tapered. Five months after surgery, IOP was 9 mmHg in OD and 10 mmHg in OS without medication, but with persistent photophobia. Because of evolving cataract in OU, BCVA was 20/80 in OD and 20/40 in OS. The patient underwent phacoemulsification with intraocular lens implantation with resultant BCVA of 20/25 in OD and 20/30 in OS. IOP was stable at 12 mmHg in OD and 8 mmHg in OS without medication.
Of note, during follow-up, progressive pallor of the optic discs with increased cup/disc ratio and neuroretina rim thinning in OU developed, especially in OD (Figure 3(a), second upper), corresponding to peripapillary RNFL thickness reduction in the inferior quadrant shown in OCT (Figure 3(b) bottom); SAP 24-2, however, remained stable (Figure 3(c) bottom) with reasonable topographic correlation between thinning of ganglion cell complex and SAP 10-2 in OU.
At the last examination in October 6th 2022 (almost 3th year follow-up), the patient presented in OU: BCVA equal 20/25; IOP equal to 12 mmHg without antiglaucoma medication; reduced photophobia, unchanged iris transillumination, VF and OCT findings.
Discussion
The last literature review about BAIT syndrome was published by Perone et al. 2 They reported a total of 79 cases have been published up that date, mainly in Europe and especially in Turkey and Belgium. 2 The majority of reported cases were of bilateral acute iris depigmentation (BADI).3–5 It was also reported that BAIT syndrome mainly affects young women between the ages of 30 and 50, and symptoms are often preceded by an upper airway infection.
Our case is the first BAIT syndrome reported in a young male in Brazil considering that the case reported by Maestrini et al. occurred in an old female and had the mistaken diagnosis of BADI. 8
Concerning the pigment discharge in BAIT, it comes from the iris pigment epithelium and stroma, whereas in BADI, the pigment discharge presumably comes from the iris stroma.3–5 In our case, we found transillumination defects and fixed mid-dilated pupils (Figure 1, right) which are not observed in patients with BADI.3–5 It is not yet clear whether both entities are distinct or subtypes/spectrum of the same disease. It is likely that some cases of BAIT syndrome may have been labeled as BADI before better recognition of a clear dichotomy between the two entities, as occurred with the case from Maestrini et al. 8 BAIT and BADI have recently been described in some patients and clinical signs of both syndromes can occur simultaneously in different eyes, confirming the probable etiopathogenic relationship between the two entities. 8 Indeed, the fact that both share many clinical features supports the hypothesis that they may represent parts of the same disease spectrum.
The main complications of BADI/BAIT are ocular redness, pain and elevated IOP. In BAIT syndrome, accentuated IOP rise, similar to APAC, might be refractory to medical therapy. There is persistent photophobia, causing discomfort in long-term, despite satisfactory BCVA as occurred in the present case. In cases of BADI, there is a gradual reduction of iris pigmentation over time. In addition, IOP elevation may respond to conventional antiglaucoma treatment associated with antiviral medications. However, in the present case of BAIT, glaucoma remained refractory to clinical treatment and trabeculectomy with mitomycin C was necessary for adequate IOP control in OU.
BAIT syndrome should be differentiated from inflammatory conditions such as viral iridocyclitis, Fuchs’ heterochromic iridocyclitis (unilateral uveitis), Vogt-Koyanagi-Harada disease and, other uveitis evolving with increased IOP and iris changes.5,7 Also, it should be differentiated of non-inflammatory conditions such as pigment dispersion syndrome (PDS) and PG, primarily in young, myopic and white individuals. We have ruled out PDS because in BAIT syndrome there is a diffuse and circumferential transillumination without sparing any pupillary portion of the iris (Figure 1, right), causing moderate to intense and persistent photophobia while in PDS, the iris transillumination is usually radial, mild and restricted to the ciliary portion, sparing the pupillary portion of the iris, resulting in no photophobia. In addition, in BAIT syndrome there is a heavy and circumferential dusting of pigment on the surface of the anterior crystalline lens capsule (Figure 1, left), intense pigmented flare (4+) in the anterior chamber, pigmentation on posterior surface of the cornea and angle while in PDS the Krukenberg spindle is slight and the Schlemm is black. In addition, there is redness and ocular pain in BAIT syndrome which are not present in PDS. The only similar finding in both entities is a concave iris. Lack of Krukenberg spindle often argues against PDS and PG. In PG, IOP increase is not sudden, although this might occur in some patients. Both PDS and PG have been linked to a wide range of genetic mutations.
In this present case, UBM showed that despite a large area of contact iris-crystalline lens, there was not posterior synechiae or pupillary seclusion causing iris bombée. This area large of contact iris-crystalline lens is totally contrary to that virtual area of contact iris-crystalline lens reported by Cronemberger et al. in APAC. 9 Even so, there was an acute bilateral IOP rise with a consequent increase of RNFL thickness on OCT (Figure 3(b), bottom left). The changes on peripapillary RNFL and macular ganglion cell complex by OCT as well as the VF losses are similar to those seen in eyes with acute primary angle closure (APAC), in which an early edematous phase is followed by progressive thinning of RNFL and ganglion cell complex. 10 The fundus findings were not incidental and they occurred as consequence of the sudden IOP elevation in BAIT syndrome (48 mmHg in OU). However, bilateral IOP elevation in BAIT is associated with mechanical obstruction of the angle by dense pigmentation deposition, whereas, in APAC, which rarely occurs simultaneously in OU, reversible apposition of the iris periphery in a narrow angle is the involved mechanism. Therefore, pilocarpine eye drops are contraindicated in BAIT syndrome where the angle is mechanically blocked while it is indicated in APAC, in which angle closure is appositional. Some similarities between BAIT syndrome and APAC are redness and ocular pain, fixed mid-dilated pupils due to a paralysis of the iris sphincter and, the initial and overtime changes in visual field and OCT.9,10
To the best of our knowledge this case report is the first to describe OCT and UBM findings and the importance of both workups in BAIT syndrome for the differential diagnosis.
Acute onset of bilateral anterior uveitis after an upper respiratory tract infection, with profound pigment dispersion in the anterior chamber and intense pigment deposition in the angle of a phakic patient with mid-dilated pupil poorly responsive to light and raised IOP is suggestive of BAIT. A viral etiology for BAIT has been postulated. In this present case, IgG antibodies were positive for toxoplasmosis, HSV and VZV, indicating chronic infection. Tugal-Tutkun et al. demonstrated that IgM antibodies were negative and IgG antibodies were present in 10 patients. 3 IgG seropositive for HSV-1 and EBV was 83% and 75%, respectively. 7 These authors reported 26 cases of BADI in 2009, with no conclusion on possible association with antibiotic use. 3 Nevertheless, use of oral moxifloxacin is found in the majority of cases described, and should not be overlooked as a possible etiopathogenic factor for this syndrome.
Etiology of BAIT syndrome remains to be determined. Several studies reported associations between BAIT syndrome and prior antibiotic therapy, particularly oral moxifloxacin. Upper respiratory tract infections were also described before onset of BAIT syndrome.
Conclusions
BAIT syndrome may present with accentuated IOP rise, refractory to clinical therapy and demanding surgical management as occurred in the present case. Its early recognition and differential diagnosis using OCT and UBM are critical for treatment. Etiopathogenesis of BAIT remains to be elucidated, but all clinicians should be aware of potential adverse effect of oral moxifloxacin.
Footnotes
Acknowledgements
None.
Authorship
All authors meet the current ICMJE criteria for authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Written and informed consent was obtained from the patient for the publication of this case report and all accompanying images.