
Abstract
Introduction
Idiopathic retinal vasculitis, aneurysms, and neuroretinitis (IRVAN) syndrome is a rare clinical entity affecting young healthy individuals. Treatment primarily involves pan retinal photocoagulation (PRP) to capillary non perfusion areas. Intravitreal anti-VEGF or steroids are given in the presence of macula edema. Oral steroids do not alter the course of the disease. Arterial occlusions have been reported in IRVAN.
Methods
Retrospective case review.
Result
A twenty seven year old male presented to us with mild blurring of vision for one week. His BCVA was OU 20/20. Anterior segment examination was normal. Fundus examination showed bilateral disc aneurysm with OS arterial aneurysm along the inferior arcade. Fundhus fluorescein angiography and OCT angiography were confirmatory of the disc and retinal aneurysm. Capillary non perfusion (CNP) areas were noted in the periphery. Two days later he presented with paracentral scotoma in his left eye which was confirmed by Amsler chart. Fundus, OCT and OCTA were confirmatory of Paracentral Acute Middle Maculopathy (PAMM). The retinal aneurysm had increased in size from 333 micron diameter to 566 micron diameter. Panretinal photocoagulation to the CNP areas was done and intravitreal antiVEGF was given. At 6 months follow up, retinal aneurysm had disappeared.
Discussion
Our case describes a unique event with sudden increase in size of the aneurysm leading to acute blockage in the deep capillary plexus thus being the first report of PAMM in IRVAN. The patient was treated with PRP and intravitreal anti-VEGF for the enlarging aneurysm which reduced in size within a week.
Introduction
Idiopathic retinal vasculitis, aneurysms, and neuroretinitis (IRVAN) syndrome is a rare bilateral, insidious disease affecting young individuals leading to profound visual loss if not treated promptly. Chang et al put forth the acronym IRVAN- Idiopathic retinal vasculitis, aneurysms, and neuroretinitis, and presented the criteria for diagnosis. Major criteria include retinal vasculitis, arterial aneurysms and neuroretinitis. Minor criteria include capillary nonperfusion areas, retinal neovascularisation and retina exudates. 1
Here we describe a classic case of IRVAN with paracentral acute middle maculopathy.
Case report
Twenty seven year old male presented to us with mild blurring of vision for one week. His BCVA was OU 20/20. Anterior segment examination was within normal limits. Fundus examination) showed bilateral tortuous vessels over the disc and peripheral sheathing of vessels (Figure 1(a) and (b)). In the left eye there was a retinal arterial aneurysm along the inferior arcade with surrounding hard exudates inferior to fovea. Basic blood tests, serology & imaging (USG – Abdomen, MRI/MRA/MRV) showed no abnormalities. Fundus Fluorescein Angiography (FFA) (Figure 1(c) and 1(d)) showed bilateral capillary non-perfusion areas in all four quadrants and leakage from the disc. Leakage corresponding to the arteriolar aneurysm was noted in the left eye. OS SD OCT showed diffuse edema of inner retinal layers inferior to the fovea. OD SD OCT was unremarkable. OCTA of the disc showed aneurysms in both the eyes (Figure 1(e) and 1(f)).
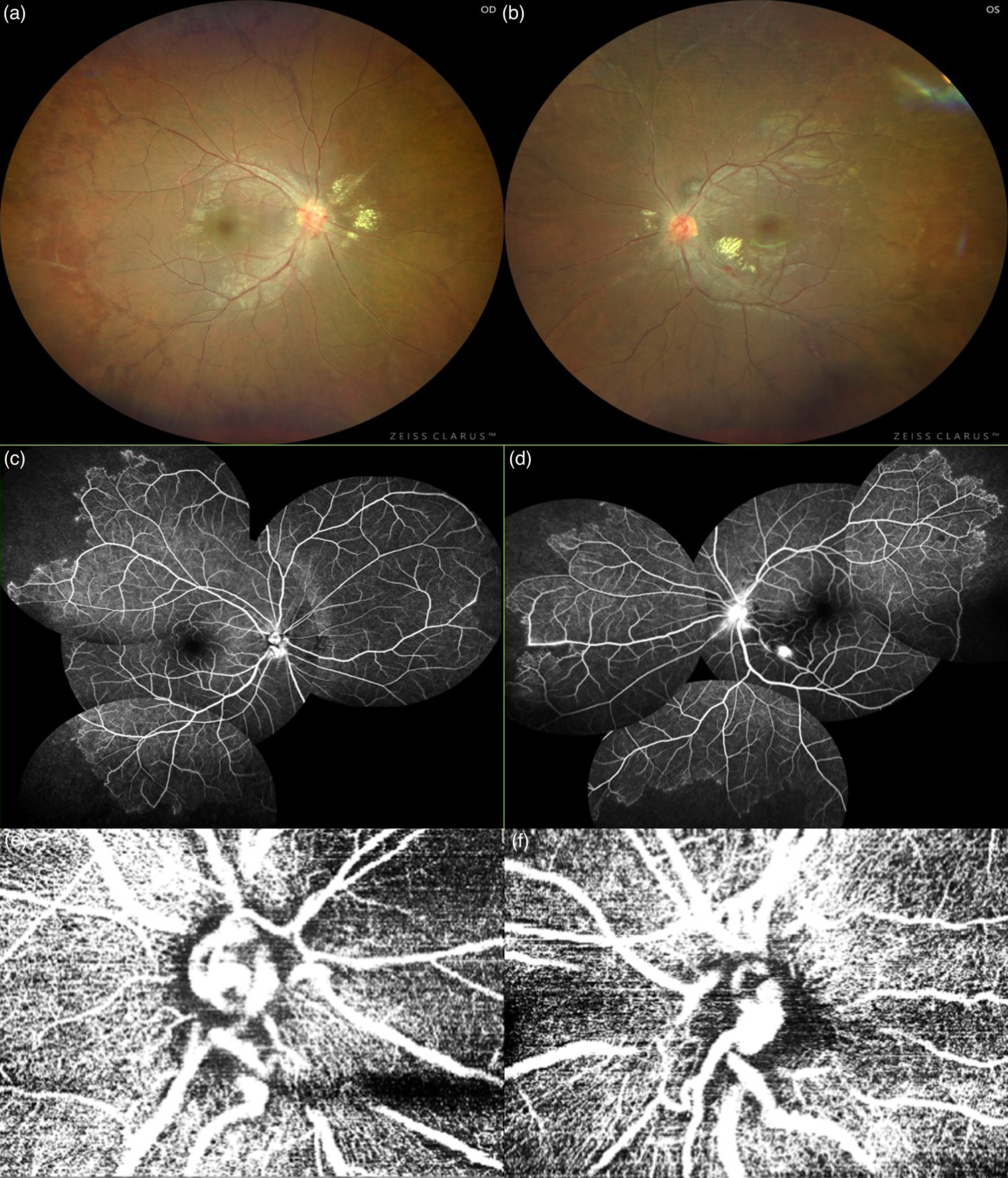
(a) Color Fundus photograph of right eye showing tortuous vessels over the disc, hard exudates around macula and peripheral sheathing of vessels. (b) Color Fundus photograph of left eye showing tortuous vessels over the disc, hard exudates around macula, peripheral sheathing of vessels with retinal aneurysm along the inferior arcade. (c) FFA showing capillary non perfusion areas in all four quadrants along with leakage from the disc. (d) FFA showing leaking retinal aneurysm in the para foveal region, capillary non perfusion areas in all four quadrants along with leakage from the disc. (e) SD OCTA of right eye optic disc showing dilated tortuous vessels. (f) SD OCTA of left eye optic disc showing dilated tortuous vessels.
Two days later he presented with paracentral scotoma in his left eye (Supplementary material). BCVA was OU 20/20. OS fundus showed increasing size of the retinal aneurysm associated with opacification of deep retinal layers in the inferior parafoveal region close to the aneurysm (Figure 2a) with corresponding capillary drop out areas in the deep vascular plexus in OCTA (Figure 2b). SD OCT of LE showed hyperreflectivity of middle layers near the parafoveal region suggestive of paracentral acute middle maculopathy (PAMM) (Figure 3c and 3d). In view of the increasing size of the aneurysm, he was given intravitreal anti-VEGF Ranibizumab. Pan retinal photocoagulation (PRP) was done to the capillary non-perfusion areas. After one week, his scotoma decreased, the retinal aneurysm had shrunk in size with reduction in hyper reflectivity of middle retinal layers (Figure 3e and 3f). At 3 months, BCVA was 6/6 and the size of the aneurysm remained the same. At 6 months follow up, BCVA was maintained at 6/6, retinal aneurysm had disappeared, with SD OCT showing thinned out middle retinal layers.
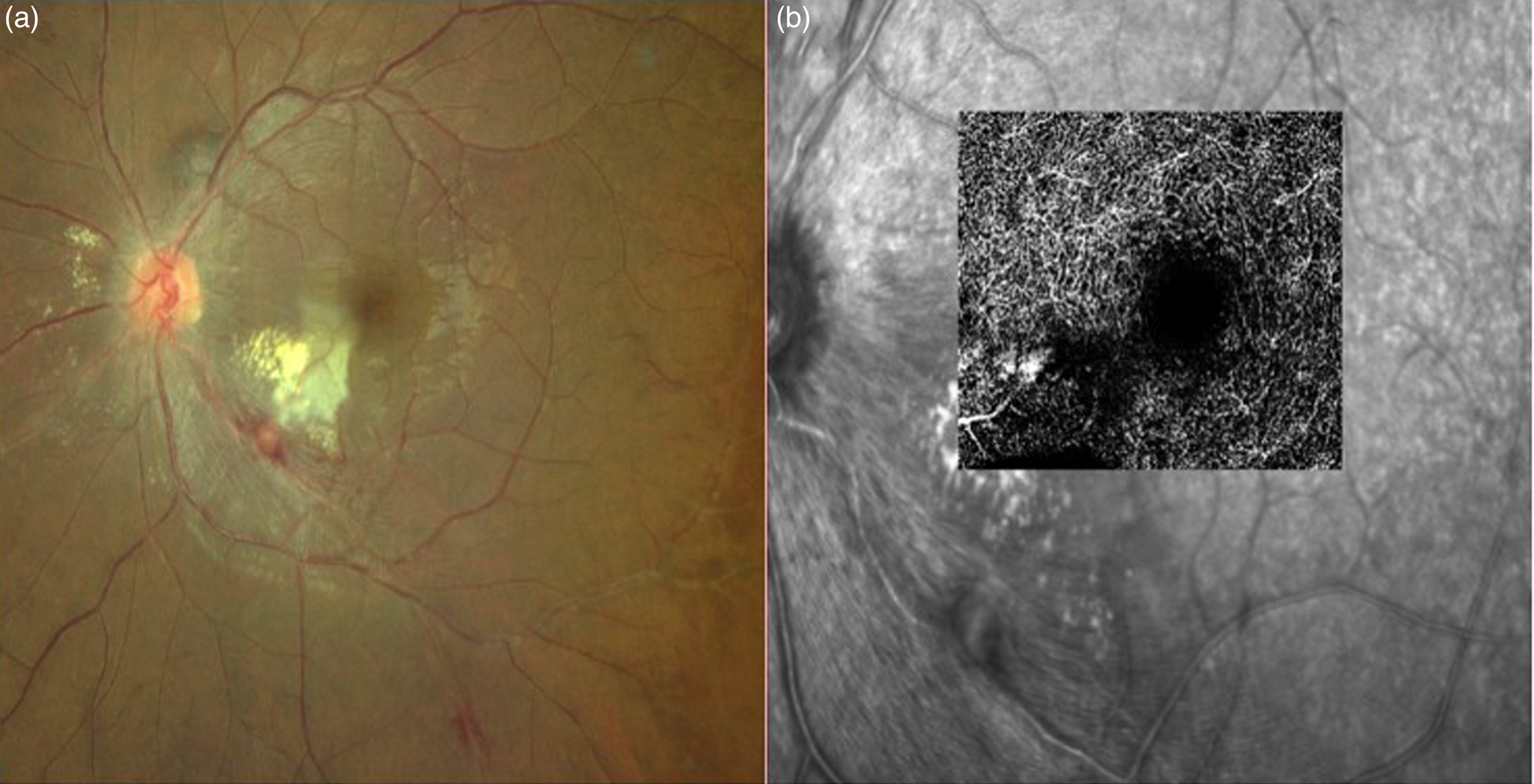
(a) OS color fundus photo showing opacification of the retina inferior to fovea with enlarging aneurysm. (b) OS SD OCTA of the deep capillary plexus showing corresponding capillary drop out areas.
Discussion
Samuel and Chang et al have published the largest case series of IRVAN.1,2 Diagnosis is clinical with the presence of characteristic signs namely disc aneurysms, multiple retinal arterial aneurysms, retinal exudates and presence of retinal vascular sheathing. Staging has been proposed by Samuel et al.
Stage 1 Macroaneurysms, exudation, neuroretinitis, retinal vasculitis
Stage 2 Capillary nonperfusion (angiographic evidence)
Stage 3 Posterior segment neovascularization of disc or elsewhere and/or
vitreous hemorrhage
Stage 4 Anterior segment neovascularization (rubeosis iridis)
Stage 5 Neovascular glaucoma. 2
Though they coined the term IRVAN, the neuroretinitis they describe in their cases refer to the peripapillary exudation seen clinically with disc leak on FFA. None of their cases presented with acute drop in vision with disc edema and hard exudates.1,2 Hence the term neuroretinitis is a misnomer and as Khairallah et al rightly suggested IRVARE may be the appropriate acronym and it stands for idiopathic retinal vasculitis, aneurysms and retinal exudates. 3 OCTA has been a valuable tool in demonstrating that the disc leak seen in FFA is in fact because of the aneurysmal dilatation of the disc vessels. 4 Our case has all the classic features of Stage 2 IRVAN with PAMM, which to the best of our knowledge has never been reported in IRVAN.
Multiple cases of retinal arterial occlusion occurring de novo have been reported in IRVAN. 4 The arterial occlusions occur either just distal to the aneurysm as in our case or may not be related to the location of the aneurysm. 4 Patients with IRVAN may thus be inherently at risk for arterial occlusion. A case of arterial occlusion following focal laser to the aneurysm was described in the series by Chang et al. 1 Our case describes a unique acute event with sudden increase in size of the aneurysm which could have caused a localized compression or a change in hemodynamics leading to acute blockage in the deep capillary plexus thus being the first report of PAMM in IRVAN. In view of potential risk of retinal vascular occlusion worsening with focal laser on the aneurysm and the enlarging size of the aneurysm, intravitreal anti-VEGF was given instead. Anti-VEGF agents play a significant role in reducing the macular edema in IRVAN. 5 It is also an adjuvant to PRP in the treatment of neovascularization. 5 In our case we have used anti-VEGF to reduce the sudden increase in the size of the aneurysm which caused a localized deep capillary plexus compression. The patient responded well to PRP and anti-VEGF treatment with the aneurysm disappearing at 6 months follow up.
The pathogenesis of IRVAN remains elusive. Balaratnasingam et al reported a case with previously documented evidence of normal fundus later progressing to IRVAN.
6
So they suggested that a congenital abnormality may not be possible. Cases of IRVAN being reported with tuberculosis and fungal sinusitis may suggest an immune reaction to the organism.7,8 In the case series by Massicotte E et al, out of the 5 cases, 2 were unilateral cases and 3 cases had noteworthy systemic associations namely multiple sclerosis, ischemic stroke and anti-phospholipid antibody syndrome.
9
Hence, all patients suspected to have IRVAN need a full systemic evaluation for vasculitis. The characteristic appearance of new aneurysms with disappearance of the old one suggest a migrating inflammatory process but lack of response to steroids does not support this theory.8,10 Most of the case reports describe vanishing aneurysms following PRP or oral steroids over a span of 4 to 6 months.
10
Whether the disappearance of aneurysm in our case is the natural course of the disease or as a result of PRP and anti-VEGF therapy is debatable
Conclusion
To the best of our knowledge, this is the first reported case of a patient with documented increase in the size of a retinal aneurysm associated with PAMM in IRVAN. Intravitreal antiVEGF may be considered in patients with vision threatening retinal aneurysms.
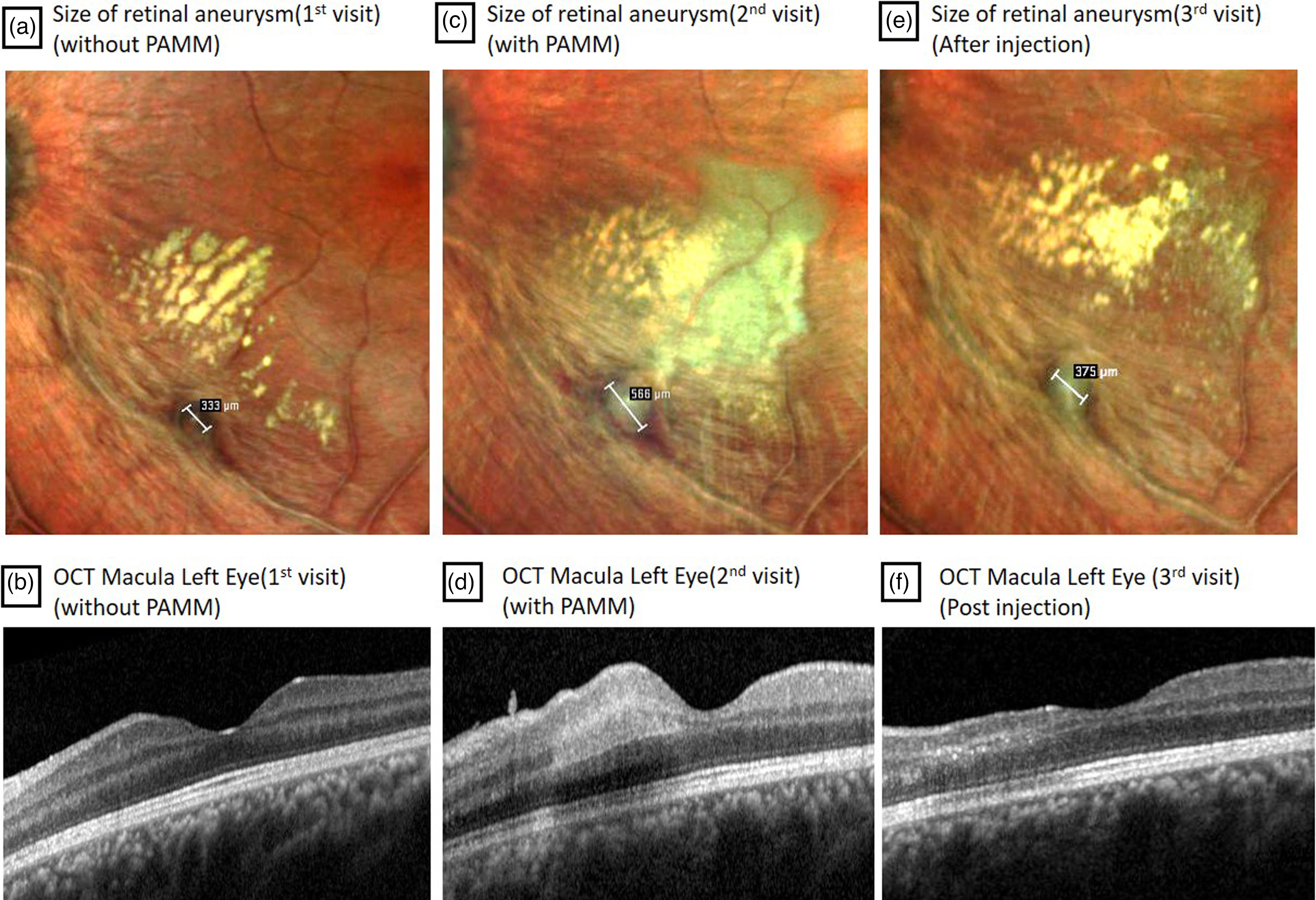
(a) Multicolor photo showing retinal aneurysm measuring 333 µm on presentation. (b) OS OCT showing normal foveal contour and layers. (c) Multicolor photo showing retinal aneurysm measuring 566 µm with opacification of retinal layers in the inferior para foveal region close to the aneurysm 2 days later. (d) OS OCT showing hyper reflectivity of middle layers suggestive of paracentral acute middle maculopathy (PAMM) near the para foveal region. (e) Multicolor photo showing retinal aneurysm measuring 375 µm one week after intravitreal Ranibizumab. (f) OS OCT showing thinning of middle retinal layers with loss of foveal architecture one week after intravitreal Ranibizumab.
Supplemental Material
sj-jpg-1-ejo-10.1177_11206721231174259 - Supplemental material for Enlarging aneurysm with paracentral acute middle maculopathy in idiopathic retinal vasculitis, aneurysms and neuroretinitis (IRVAN) – a case report
Supplemental material, sj-jpg-1-ejo-10.1177_11206721231174259 for Enlarging aneurysm with paracentral acute middle maculopathy in idiopathic retinal vasculitis, aneurysms and neuroretinitis (IRVAN) – a case report by Indu Govindaraj, Anju Kuriakose and Anand Rajendran in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721231174259 - Supplemental material for Enlarging aneurysm with paracentral acute middle maculopathy in idiopathic retinal vasculitis, aneurysms and neuroretinitis (IRVAN) – a case report
Supplemental material, sj-docx-2-ejo-10.1177_11206721231174259 for Enlarging aneurysm with paracentral acute middle maculopathy in idiopathic retinal vasculitis, aneurysms and neuroretinitis (IRVAN) – a case report by Indu Govindaraj, Anju Kuriakose and Anand Rajendran in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from the patient and the Institute Review Board approved the report for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.