
Abstract
Purpose
To investigate the influence of post-operative eye patching on corneal thickness, endothelial cells’ loss and visual acuity in patients diagnosed Fuchs’ endothelial corneal dystrophy (FECD).
Setting
Public healthcare centre, Shamir Medical Centre, Israel.
Methods
This randomized controlled trial included patients with FECD undergoing routine cataract surgery in a public medical centre. Patients were randomly assigned to 2 groups: the eye undergoing surgery was covered with a patch for 24 h in the first group (patched group), and a plastic shield was used in the second (non-patched group). Both groups received a unique dose of a local steroid and antibiotic post-operatively. The eyes were examined pre-operatively, and on days 1, 7 and 30 post-surgery . Examination included: best corrected visual acuity (BCVA), comeplete slit lamp examination, intra ocular pressure (IOP), anterior chamber depth (ACD), central corneal thickness (CCT) using the IOL Master 700 (Zeiss, Germany) and endothelial cell density (ECD) using Specular microscopy. Cumulative dissipated energy (CDE) and operation time were recorded for all cases.
Results
The study included 46 eyes of 46 patients diagnosed with FECD. Twenty-three eyes in the patched group, and 23 eyes in the non-patched group . Thirty days post-operatively the CCT in the patched group decreased by 60 ± 38 mµ (9%) compared to 92 ± 80 mµ (13.5%) in the non- patched group (p = 0.04). Seven days post-operatively the CCT in the patched group decreased by 31 ± 35 mµ (5%) compared to 58 ± 76 (8%) in the non-patched group, but this difference did not reach statistical significance (p = 0.081). There was no statistically significant difference in endothelial cells loss as well as BCVA at 1, 7 and 30 days post-operatively between the study groups.
Conclusions
Avoiding eye patch post-operatively after cataract surgery in patients with FECD results in better corneal clarity recovery and reduced corneal edema one month post-operatively. Visual acuity and endothelial cell's loss were not influenced by patching.
Keywords
Post-operative eye patching after routine cataract surgery results in slower visual recovery and increased corneal edema in patients without FECD as compared to non-patched controls. Avoiding eye patching in FECD results in better corneal recovery and reduced corneal edema one month post-operatively. Avoiding eye patching post-operatively after cataract surgery in patients with FECD doesn’t affect endothelial cells loss.
Introduction
Fuchs’ endothelial corneal dystrophy (FECD) is a bilateral dominantly inherited disease, affecting corneal endothelial cells and causing progressive loss of them and secretion of an abnormally thickened basement membrane.1–2 FECD can present in variable expressivity, is often asymmetric, and in some cases, incomplete penetrance.1–2
FECD patients are more prone than the general population to endothelial cells damage in all intraocular surgeries including phacoemulsification cataract surgery. 3
Phacoemulsification has been shown to decrease the number of corneal endothelial cells in the general population by 8.5% and in patients with FECD by 11.5–19.5%.4–8
Loss of endothelial cells might lead to corneal decompensation and corneal edema, ultimately leading to corneal bolus keratopathy and need for posterior lamella keratoplasty. 3
Different intra-operative measures are employed to protect corneal endothelium and prevent endothelial cell loss in patients with FECD including coating of the endothelium with visco-surgical devices (also known as the soft-shell technique), phaco-power modulations and corneal-protective chopping techniques, and recently the use of femtosecond laser assisted cataract surgery (FLACS).5–9
Our study group recently conducted a study that showed that post-operative patching results in slower visual recovery and increased corneal edema in patients without FECD as compared to non-patched controls. 10
The goal of this current study was to evaluate the influence of post-operative eye patching on corneal thickness, endothelial cells’ function, and visual acuity in patients with FECD.
Methods
A randomized controlled trial including patients with a diagnosis of FECD who underwent a routine cataract surgery by two senior cataract surgeons in one medical centre between 2020 to 2021. The diagnosis of FECD was made by a cornea specialist and confirmed by specular microscopy. In all patients the presence of corneal guttata, polymegatism and pleomorphism was confirmed and in the vast majority of patients the endothelial cell density (ECD) was lower than the average in the general population for their age. 11 All patients were diagnosed with asymptomatic and sub-clinical FECD. Non-of the patients had clinically significant corneal edema nor symptoms related to FECD. All patients signed an informed consent and the study was approved by the Institutional Review Board and followed the tenets of the Declaration of Helsinki. IRB registry number 0287-19-ASF.
The exclusion criteria included: history of previous ocular surgery or trauma; history of uveitis; corneal scar and opacity; postoperative descemet membrane detachment, and any complication during surgical course.
All the patients underwent a standard phacoemulsification cataract surgery with intraocular lens implantation. The CENTURION® (Alcon, USA) phacoemulsification machine was used for all surgeries and the endothelium was protected using the soft-shell technique in all cases with the use of the same Ophthalmic Viscosurgical Devices (OVD) for all surgeries: Viscoat® and Biolon®. 12 All patients received topical anethesia with Oxybuprocaine drops and intracameral adrenaline+ lidocaine. In the end of surgery intracameral cefamezine or moxifloxacin in case of allergy was injected to all patients. In all patients in this study Alcon Acrisof SA60AT were implanted, and the power was calculated using the Barret II Universal formula. Patients were randomly assigned to 2 groups using Microsoft Excel 365 randomization function. In the patched group, the eye was patched for 24 h immediately after surgery and in the non-patched group, a plastic shield alone was used. A single dose of a topical steroid and antibiotic drops immediately after surgery was given to all patients in both groups. Postoperative local therapy included antibiotic as well as steroidal agents: Ofloxacin ophthalmic solution drops q4h and Dexamethasone eye drops q3h, starting 1 day post-operatively.
Preoperative examination included: Best corrected visual acuity (BCVA), the presence of corneal edema, intra ocular pressure (IOP) and cataract grading. Central corneal thickness (CCT) and anterior chamber depth (ACD) was obtained using the IOL Master 700 (Zeiss, Germany). Specular microscopy using Noncon Robo NSP-7700 (Konan Medical Inc) to evaluate ECD, coefficient of variation (CoV), mean cell size, and hexagonality.
Cumulative dissipated energy (CDE) and operating time were recorded intra-operatively.
Post-operative ocular examination at 1 day, 1 week and 1 month included: BCVA, the presence of corneal edema, IOP, CCT, using the IOL Master 700 (Zeiss, Germany). Specular microscopy using Noncon Robo NSP-7700 (Konan Medical Inc) to evaluate ECD, coefficient of variation (CoV), mean cell size, and hexagonality. Endothelial cell count was performed manually on the specular microscopy software by marking the cells in a chosen area and the software performed extrapolation to the entire cornea. Primary outcome was CCT decrease after 7 and 30 days post-operatively, measured by IOL Master 700 (Zeiss, Germany) compared to CCT on the first post-operative day. Secondary outcomes were ECD measured by Specular microscopy using Noncon Robo NSP-7700 (Konan Medical Inc) and BCVA tested using a Snellen Visual Acuity chart.
Sample size
The study was designed to have at least 80% power and statistical significance was set at < 5%. Given an expected postoperative CCT of 690 mµ among patched patients with FED 13 and CCT of 650 mµ among non-patched patients with a standard deviation of 30 mµ. Exposed to controls (non-patched to patched) ratio was planned to be 1: 1 in this study. Thus, the minimal sample size required for an 80% power and 5% significance assumption is 40 patients, 20 patients in each group.
WinPepi software, version 11.65, 2016 was used for sample size calculation.
Statistical analysis
The students’ t test, the Mann–Whitney U test and the chi-square test, were used as appropriate to compare the baseline and outcomes variables between the two groups. The students’ t-test or the Mann–Whitney U test were used for the analysis of continuous variables according to their distribution. Normal distribution was checked with Q–Q plot, the Shapiro–Wilk test and histogram chart with a normal distribution curve. P-value < 0.05 in a two-sided test was considered significant.
All analyses were performed using IBM SPSS Statistics for Windows version 24.0 (IBM Corp., Armonk, NY, USA).
Results
Forty-six eyes of 46 patients diagnosed with FECD were included in the study. Twenty-three eyes were patched for 24 h after surgery, and 23 eyes were not patched, protected with only plastic shield.
The demographic, preoperative and intraoperative characteristics according to patients’ patching status are presented in table 1. There was no significant difference between the groups in age, gender, diabetes mellitus status, degree of cataract, ACD, preoperative CCT and ECD, as well as operation time and CDE.
Demographic, clinical and surgical characteristics of study groups.
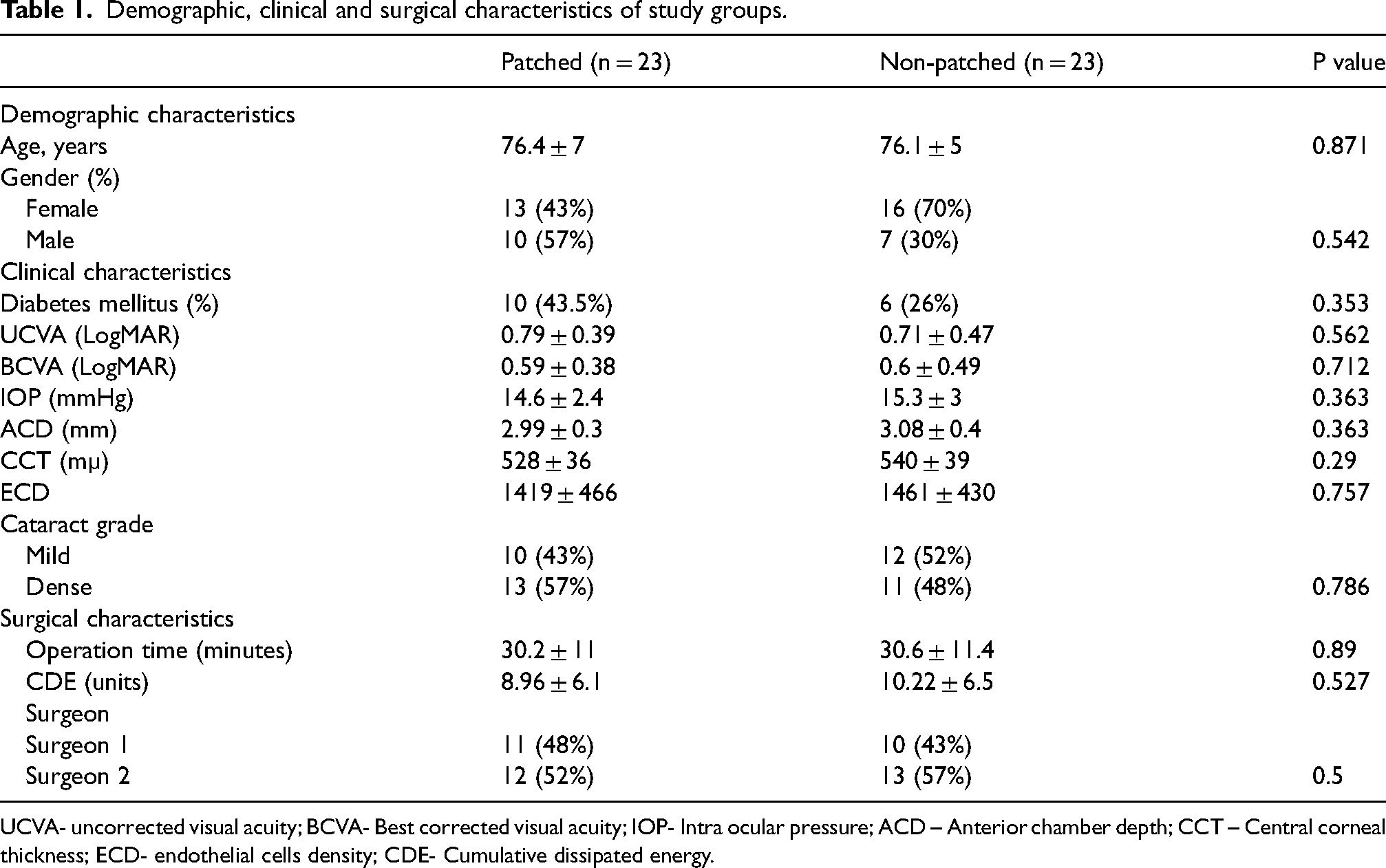
UCVA- uncorrected visual acuity; BCVA- Best corrected visual acuity; IOP- Intra ocular pressure; ACD – Anterior chamber depth; CCT – Central corneal thickness; ECD- endothelial cells density; CDE- Cumulative dissipated energy.
Table 2 shows the outcomes of UCVA, BCVA, CCT and ECD at 1, 7 and 30 days post-operatively in both groups.
Post-operative outcomes in study groups.
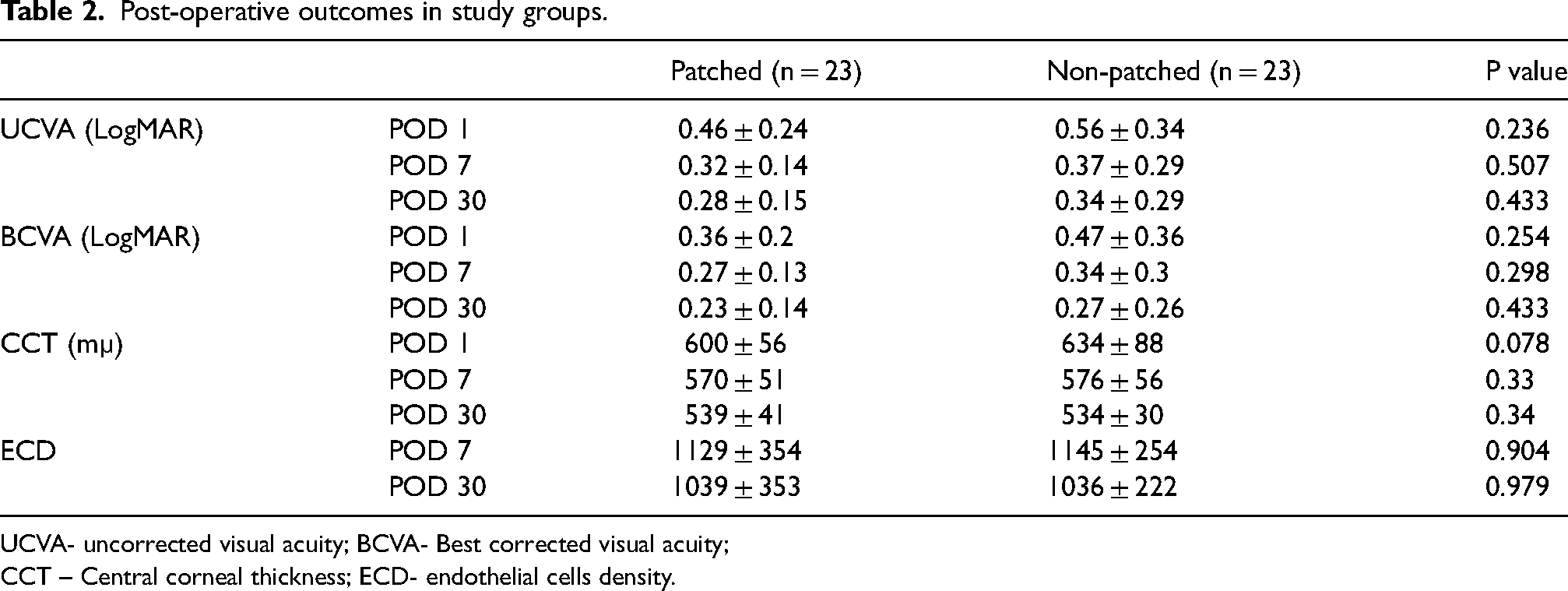
UCVA- uncorrected visual acuity; BCVA- Best corrected visual acuity;
CCT – Central corneal thickness; ECD- endothelial cells density.
CCT
Thirty days post-operatively the CCT in the patched group and non-patched group decreased by 60 ± 38 mµ (9%) and 92 ± 80 mµ (13.5%) respectively (p = 0.04), compared to the CCT measured one day after surgery. A similar trend was found seven days post-operatively, CCT decrease in the patched group of 31 ± 35 mµ (5%) compared to 58 ± 76 (8%) in the non-patched group, but this difference did not reach statistical significance (p = 0.081). Table 3 and Figure 1 show the CCT decrease at days 7 and 30 post-operatively.
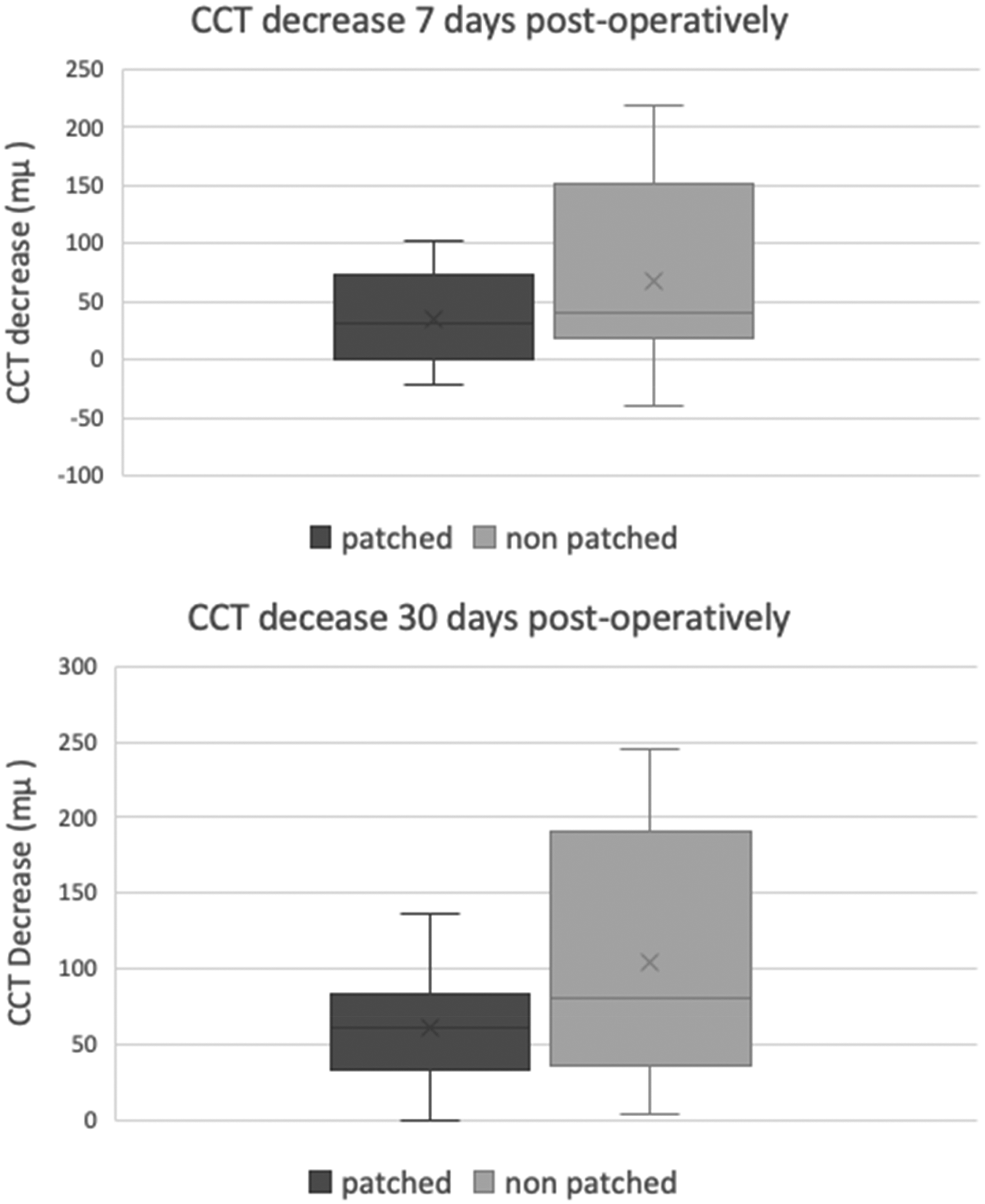
Central corneal thickness decrease (improvement) in the study groups 7 and 30 days post-operatively compared to the 1st post-operative day.
CCT and ECD decrease in the study groups 7 and 30 days post-operatively.

CCT – Central corneal thickness; ECD- endothelial cells density.
Three patients in the patched group (13%) and 2 patients in the non-patched group (9%) remained with clinically significant corneal edema (CCT > 600 mµ) and will likely need to undergo endothelial keratoplasty (EK).
BCVA
There was no statistically significant difference between the groups in the pre-operative BCVA as well as in the post-operative BCVA at 1, 7 and 30 days. Figure 2 shows the BCVA in the study groups in each of the above-mentioned time points. In each group there was statistically significant improvement in BCVA 7 and 30 days post-operatively compared to pre-operative BCVA.
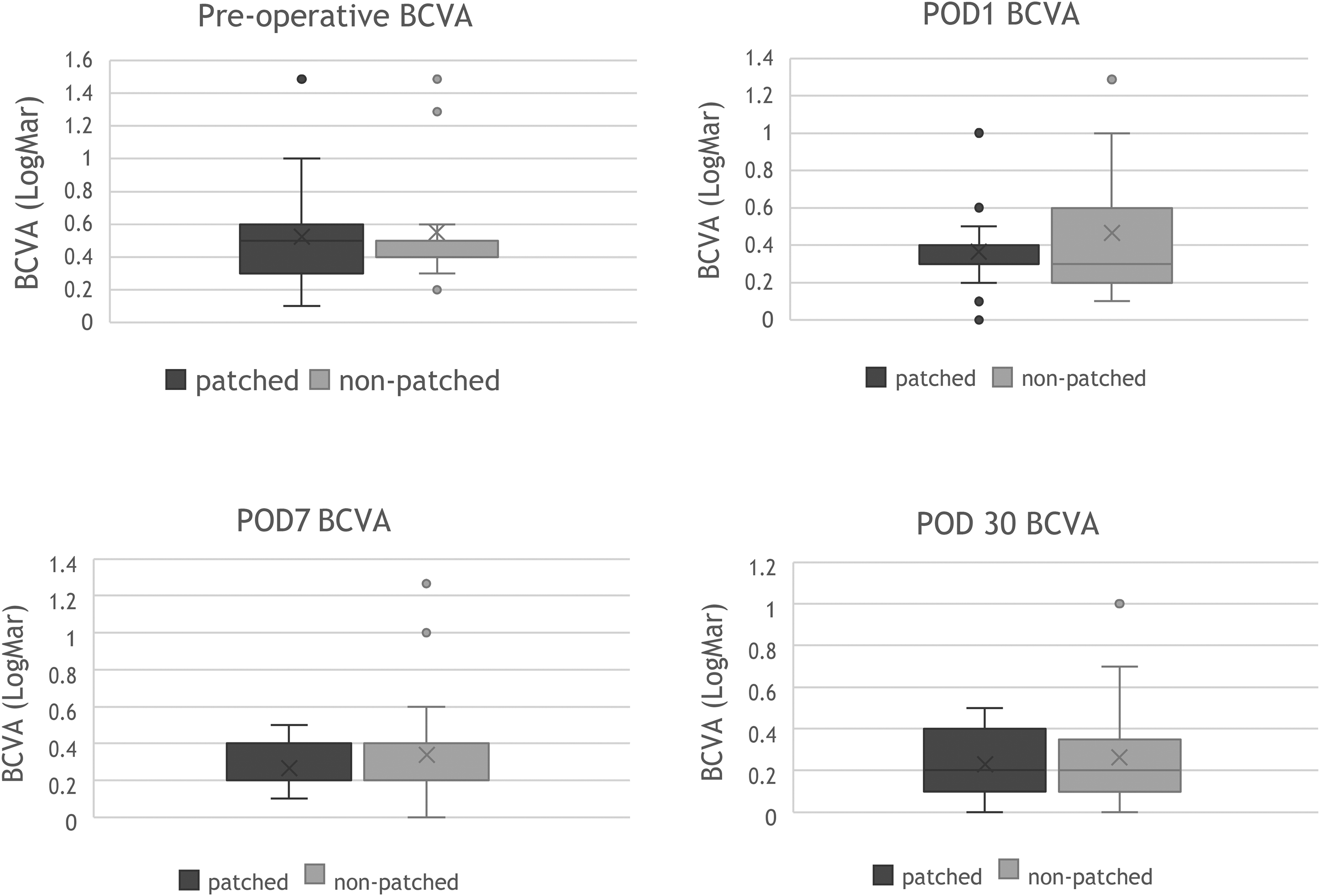
Best corrected visual acuity 1, 7 and 30 days post-operatively in the study groups.
ECD
In each group there was a statistically significant decrease in ECD At 30 days post-operatively from baseline. There was no statistically significant difference in endothelial cells loss between the study groups. Endothelial cells loss 7 days post operatively was 20% and 23% in the patched and non-patched groups respectively (p = 0.26), and 25% and 28% in the patched and non-patched groups respectively (0.52) 30 days post-operatively. (Table 3) Figure 3 shows specular microscopy of patches and non-patched patients.
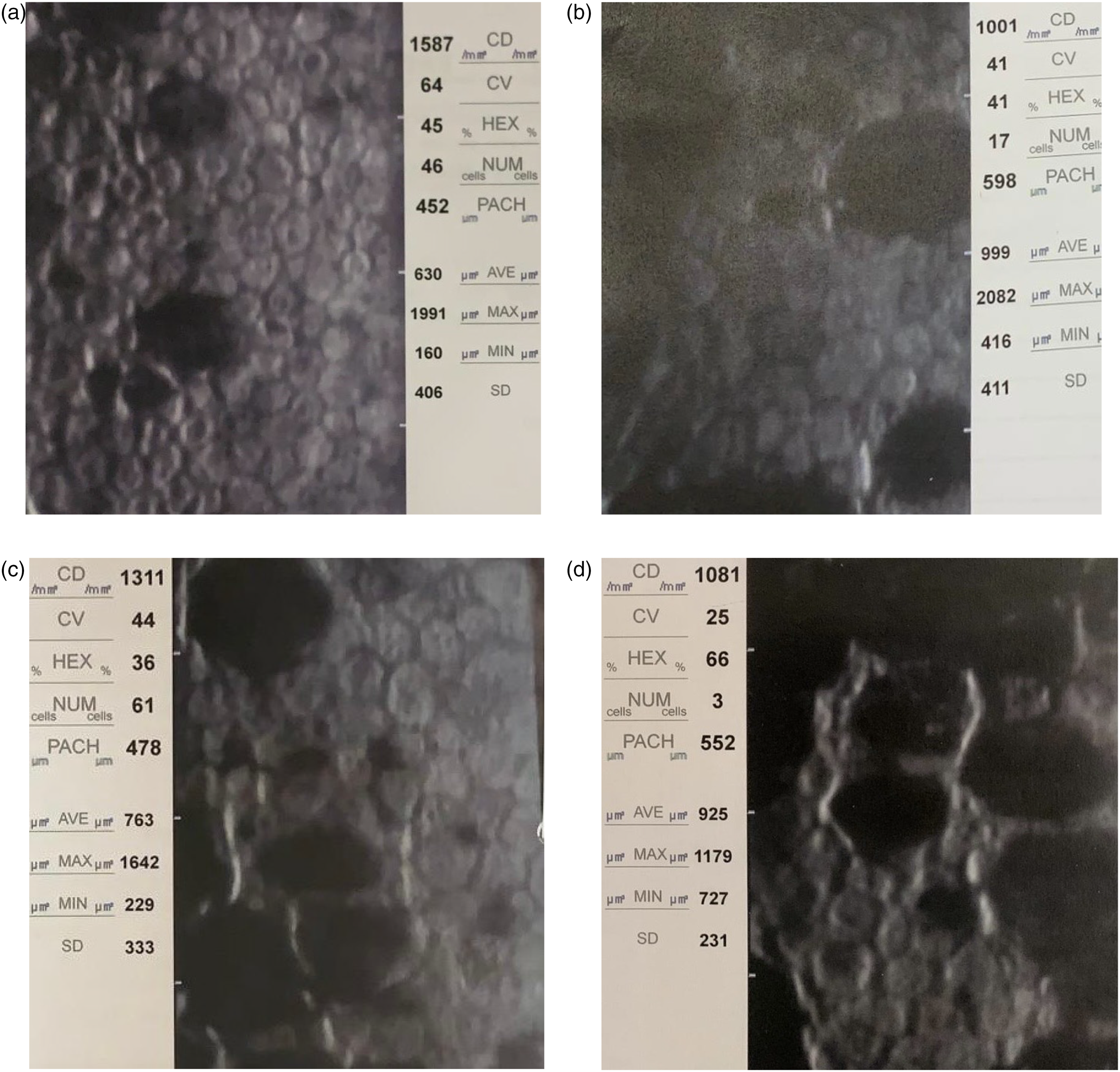
Specular microscopy of patched and non-patched patients before cataract surgery and 30 days post-operatively. a and b - patched patient (a- before; b- 30 days post-operatively); c and d - non-patched patient (c- before; d- 30 days post-operatively).
Discussion
Cataract surgery in patients with FECD holds a higher risk for corneal endothelial injury and corneal decompensation leading eventually to EK. There are three possible surgical approaches for patients with FECD and cataract: staged initial cataract surgery followed by EK if needed, EK followed by cataract surgery or a triple procedure- combined EK and cataract. 13
Endothelial cell count of less than 1000 cells/mm2, corneal pachymetry above 640 mµ or clinical evidence of corneal edema with visual symptoms, have been suggested as thresholds criteria for considering a triple procedure.3,14–15
In our study none of the patients had preoperative pachymetry above 640 mµ or clinical evidence of corneal edema, thus a staged approach of initial cataract surgery was chosen.
In this study we showed a significant difference in CCT one month post-operatively compared to CCT on the first post-operative day between the study groups – there was higher decrease in CCT in the non-patched group compared to the patched group. Similar trend was found at one week post-operatively but was not statistically significant.
Our group's previous study in patients without FECD showed that eye patching results in worse BCVA and increased corneal edema 24 h post-operatively. 10 Possible explanation of these results might be that the oxygen used by endothelial cell ATPase pump function arrives from atmospheric oxygen in trans–corneal diffusion.16–17 Our assumption was that deprivation of ambient oxygen by eye patching post-operatively would result in decreased endothelial pump function and corneal edema, since the endothelium uses atmospheric oxygen. 4 The results in this current study demonstrate that post- operative patching also in patients with FECD might slow down and harm the recovery process of the endothelium. The eyes in the non-patched group experienced a better recovery and greater decreased in CCT one month post-operatively.
The fact that in this current study, in contrast to our previous study, 10 the difference in CCT one day post-operatively between the study groups was not statistically significant and becomes significant only one week and one month postoperatively, suggests that since the endothelial cells in patients with FECD have lower function compared to non FECD patients, it takes them longer time to re-gain proper function after cataract surgery. The early exposure to greater amount of oxygen, in the non-patched group, might help in the recovery of the endothelial cells.
The fact that endothelial cells’ recovery is slower in patients with FECD was already shown before. In a study comparing phacoemulsification cataract surgery to femto-laser assisted cataract surgery -the corneal recovery time in patients with FECD, expressed as the CCT return to baseline, lasts 6 months post-operatively. 13 For this reason we believe that oxygen deprivation on the first 24 h after cataract surgery in FECD patients might cause greater damage to those cells hence slow down their recovery period as well as lower their function.
There was no significant difference in endothelial cells loss one week and one month postoperatively between patched and non-patched groups. This suggests that a higher oxygen supply in the non-patched eye immediately after surgery does not prevent endothelial cells loss but only improves cell's function, improves ATPase pump's function and decreases corneal edema. The overall endothelial cell loss in this study was 26%, slightly higher than previously reported in studies on FECD patients as 11.5–19.5%.4,8
Overall, 5 patients (10.8%) – 3 patients in the patched group (13%) and 2 patients in the non-patched group (9%) remained with clinically significant corneal edema (CCT > 600 mµ) one month post-operatively and will likely need EK. This finding correlates with previous studies that reported 10–15% EK post cataract surgery in patients with FECD.7–8 This emphasizes the benefit in a stepwise approach in patients with FECD, and against the initial triple procedure in patients with baseline CCT of less than 640 mµ. Nine patients had pre-operative ECD of less than 1000 cells/mm2, out of which 2 patients (22%) remained with clinically significant corneal edema (CCT > 600 mµ) one month post-operatively, one was in the patched group and one in the non-patched group.
Even though there was significant difference in CCT decrease (improvement) between the study groups one month post-operatively, there was no significant difference in BCVA between the groups. This may be explained by the fact that thickened Descemet membrane and guttae in patients with FECD were shown to reduce quality of vision more than visual acuity. 18
To the best of our knowledge, this is the first study to report the influence of postoperative eye patching after phacoemulsification cataract surgery in patients with FECD. The study's main strength is its prospective, randomized controlled design. The study has several limitations. First, the small sample size, due to the fact FECD is not a very common disease. Second the relatively short follow up period of one month. This can influence in both directions- first the patients with significant corneal edema one month post-operatively may improve over a longer period but also bullous keratopathy can occur many years after cataract surgery. Third, BCVA may be confounded by unmeasured variables such as patching induced transient astigmatism. The fact there was no difference between the groups suggests that overall, the effect of these factors is not meaningful.
In summary, cataract surgery alone provides a safe and favourable approach in patients with FECD with pre-operative CCT of less than 640 mµ and avoiding eye patching post operatively results in better corneal recovery and reduced corneal edema one month after surgery in these patients. Further studies are needed to investigate long-term effects of this phenomenon in bigger cohorts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.