
Abstract
Purpose
to underline the importance of optical coherence tomography angiography (OCT-A) in the diagnosis, assessment of final visual outcome and better understanding of the Purtscher like retinopathy, as well as to emphasize on performing an ophthalmologic evaluation in all patients with systemic lupus erythematosus, as eye involvement is closely related with disease activity.
Methods
case report. Ophthalmologic multimodal imaging assessment of a patient short after experiencing a systemic lupus erythematosus severe outset.
Results
fundus examination revealed multiple cotton-wool exudates and sharp defined intraretinal white flecken lesions, concentrated in the posterior pole, which along macular edema and the context of lupus disease led to the diagnosis of Purtscher like retinopathy, raising concern about underlying disease activity. OCT-A evidenced ischemic affront in the superficial and deep vascular plexuses but also at choroidal level, preconizing a poor visual outcome. Precapillary retinal vascular stops and choroid lobular ischemic images, with a honey comb configuration in the latter, were of note. Six months after initial consultation, previously displayed ischemic images gave rise to retinal and choroidal atrophy translated into counting fingers best corrected visual acuity with the posterior ensue of retina neovascularization.
Conclusions
This case proves ophthalmologic evaluation mandatory for all patients suffering from lupus and reveals OCT-A as an imaging tool of great value in the assessment of Purtscher retinopathy. To our knowledge, this would be the first report of a SLE Purtscher-like retinopathy characterized by OCT-A, matching graphically and unprecedently vascular micro-embolism stops and ischemic areas, seen as void signals, with the pathognomonic Purtscher flecken, and Paracentral Acute Middle Maculopathy (PAMM) lesions.
Keywords
Introduction
Purtscher retinopathy (PR) is characterized by acute arteriola and capillary occlusions following trauma, although these can also be secondary to underlying systemic conditions, in these cases, they are referred to as Purtscher-like retinopathy. Micro-embolism of precapillary arterioles and endothelial dysfunction are believed to play a central role, although the exact pathophysiologic basis is not fully elucidated. 1
While its diagnosis has traditionally been clinical, ancillary tests can help in defining the prognosis and in further understanding the condition. Although multimodal assessment is mandatory, optical coherence tomography angiography (OCT-A) remarkably success in these aspects. Among other modalities capable of analyzing retinal circulation, as Fundus Fluorescein Angiography (FFA) and Indocyanine Green Angiography (IGA), OCT-A is a non-invasive and faster technique, capable of rendering volumetric data. Therefore, helping in the individualized analysis of retinal plexuses and choriocapillaris, although it does not provide with dynamic information. The outer retinal layers, where photoreceptors are, receive their irrigation from the choriocapillaris, making the analysis of the blood flow status at this level crucial, because obvious potential implications in the final outcome. Analyzing this layer faces several challenges. Retinal Pigment Epithelium (RPE) scatters light, obscuring visualization bellow it. Dye-base angiograms, lack of enough lateral resolution, and even indocyanine leaks from capillaries making difficult to correctly study this layer. Even though lateral resolution stills a problem, OCT-A offers several advantages. Great axial resolution, essential for isolating the studied area. Swept source technology, when available, capable of better penetrating through the RPE. Counterintuitively, although acting as an optical barrier, RPE also prevents from projection artifacts from the above retinal vessels. 2 Finally, some comparative studies grant a greater sensitivity to the OCT-A in the detection of subtle ischemic changes. 3
We report a case of PR in a patient suffering from systemic lupus erythematous (SLE), developed short after its debut, rising concerns over a still active phase uncontrolled disease. To our knowledge this is would be the first report of a SLE Purtscher-like retinopathy characterized by OCT-A.
Case report
The A 31-years-old Pakistani woman was hospitalized due to a 4-month period of spiking fevers. A maculopapular rash involving hands, feet and thighs, palate ulcers and cervical inflammatory ganglia were observed. A thorough work up revealed proteinuria (341 mg/24-h urine protein) and microalbuminuria (34.1 mg 24 h-urine collection analysis), pancytopenia with hemolytic anemia (Hb: 6,4 g/dL, positive Coomb's test, LDH: 878 UI/L −230-480-, leukocytes: 3,5*103/mm3, lymphocytes: 0,55*103/mm3, platelets: 89 *103/mm3,) and hepatitis (GOT: 625 UI/L −32- and GPT: 242 UI/L −41-) along with interstitial lesions in the Thoracic CT scan.
Autoimmune serology, ANA >160 U/mL (<20), anti-DNAds 460 U/mL (0−200) and anti-Sm + , C3 32 mg/dL (82), C4 3,8 mg/dL (12), allowed diagnosis of systemic lupus erythematous (SLE). Noteworthy, antiphospholipid antibodies tested positive (positive lupus anticoagulant, IgM anticardiolipin antibodies: 42,6, IgG anticardiolipin antibodies: 60,05, IgM anti-B2 glycoprotein 1 antibodies: 24,54).
Systemic corticosteroids as 250 mg intravenous methylprednisolone pulse therapy per three consecutive days followed by oral 1 mg/kg/day prednisone were administered.
Once the systemic involvement was presumably under control, an ophthalmologic examination was requested prior to introducing hydroxychloroquine sulphate and hospital discharge. Although no symptoms were stated, her best corrected visual acuity (BCVA) was 20/100 OD and 20/20 OS. On Ishihara test no dyschromatopsia was found. Pupillary reflexes were preserved, as well as ductions and vergences. Anterior biomicroscopy was unremarkable and intraocular pressure was under 21 mm Hg. Right eye (OD) fundus examination revealed, sheathed peripheral vessels, multiple cotton wool exudates, mainly concentrated in the posterior pole, along with whitish intraretinal lesions, characterized by better defined boundaries, localized around the perimacular area, between arteriolar vessels, but always separated from them by clear retina. The left eye (OS) only exhibited an isolated cotton wool exudate in the infero-nasal quadrant. OD b-scan optical coherence tomography (OCT) demonstrated perifoveal areas of increased hyperreflectivity of the inner plexiform layer (IPL) and cystic macular edema (CMD) with foveal neurosensory retinal detachment (NSD). OD OCT-A exhibited flow devoid areas at the superficial and deep vascular plexus territories and at the choriocapillaris level drawing a honeycomb image. Occlusion of precapillary arterioles were also noted, all findings pointing towards an ischemic insult. FFA was not possible because of patient's denial. (Figure 1).
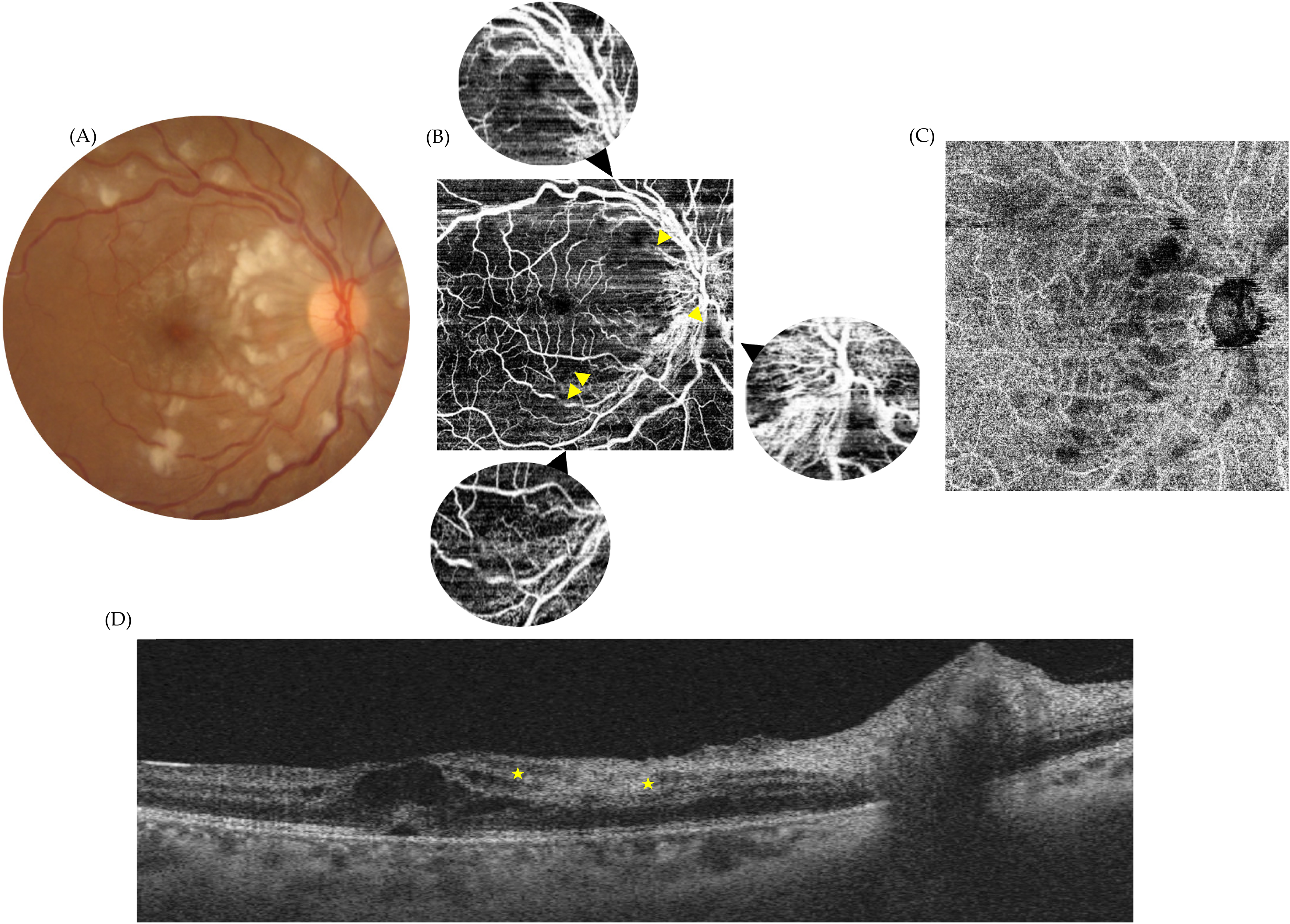
Purtscher-like retinopathy. Multimodal assessment of the affected eye at the initial presentation. Retinography (A) noting cotton wool exudates, whitening between small-sized vessels (Purtscher flecken) and macular edema. En-face OCT-A superficial and deep vascular plexuses segmentation (B) exposing possible partial vascular stops and ischemic areas seen as signal voids (yellow arrowheads) being ultimately responsible for Purtscher flecken and cotton wool exudates. En-face OCT-A choriocapillaris segmentation (D) evidencing ischemic compromise of the lobular irrigation of the choroid with signal voids adopting a honey comb image.B-Scan OCT (D) showing cystic macular edema with subfoveal neurosensory retinal detachment and inner nuclear layer hyperreflectivity (PAMM) (among yellow stars).
An intravitreal dexamethasone implant was used for the right eye. Hospital discharge was not recommended and further systemic immunosuppression was encouraged as retinopathy findings were most likely a reflection of a still active phase disease.
Effectively, analytic activity-related biomarkers were patent, 4 remarking still high transaminase values (GOT: 335 UI/L and GPT: 121 UI/L), low complement values (C3: 50 mg/dL and C4: 4,1 mg/dL) and elevated anti-DNSds titers (454 U/mL). Follow up visits were scheduled, brain MRI requested and the addition of six-monthly cycles of 750 mg/m2 cyclophosphamide or 1g cycles of rituximab was being under consideration, along with hydroxychloroquine 400 mg/day and anticoagulation with warfarin due to triple antiphospholipid antibody positivity plus an ophthalmologic ischemic event. However, the patient did not attend, appearing in clinical consultation five months later. On examination, BCVA was counting fingers in OD and 20/20 in OS. OD fundus inspection revealed: mild optic nerve pallor, narrowing vessels, copper-wiring and arteriovenous nipping, sclerotic avascular small arterioles all along the posterior pole and mid periphery without neovascularization, remaining cotton wool exudates in resolution, and generalized posterior pole atrophy. An isolated deep round small mid-peripheral hemorrhage was also present. Ancillary tests were used to further characterize funduscopic findings. OD OCT displayed marked atrophy of the inner retina, but also evidenced atrophy in the outer retina and the choroid. In the OCT-A, now in the absence of shadowing artifacts due to superficial lesions, a generalized hypoperfusion pattern with some more pronounced low signal areas were unveiled at all levels. Hence, in the choriocapillaris, the honeycomb appearance led to focal areas of marked hypoperfusion. (Figure 2). As compared with the former images, it seemed that the infarct zone did enlarge, forcing to close monitoring -monthly visits. Retinal neovascularization was detected on the next appointment, applying argon laser photocoagulation on the superior hemiretina.
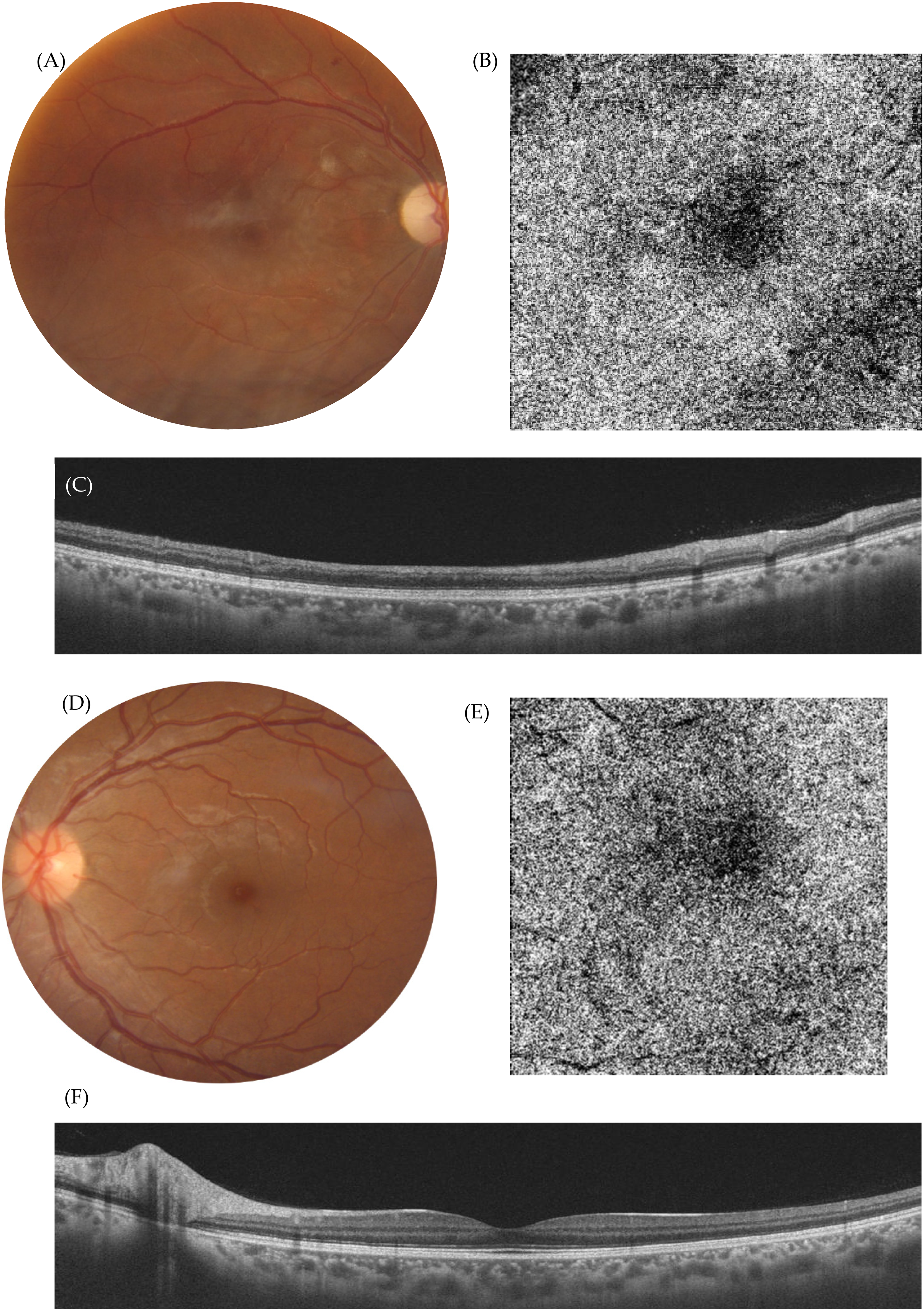
Purtscher like retinopathy. Multimodal assessment 5 months later from the initial presentation. OD retinography (A) showing subtle optic nerve pallor, sclerotic avascular vessels in the posterior pole and marked macular atrophy. OCT-A (B) demonstrating a shift from the honey comb image to an homogenous hypoperfused appearance with some more marked patches of signal voids as a representation of sequela from choroidal micro-infarctions during the acute stage. Comparison between left and right eye, evidencing atrophy at all layers (C) and (D).
Discussion
Systemic Lupus Erythematosus (SLE) is a systemic life-threatening condition, in which ophthalmologic manifestation takes place in one-third of cases. Manifestations that may imply severe sequela, but are in addition typically associated with an active phase disease. Therein, an ophthalmologic examination is imperative in all cases, as an early diagnosis is key for a good ophthalmologic but also systemic prognosis, as it is reflected from this case. 5
Retinal implications tend to be bilateral. Purtscher-like retinopathy although infrequent, should be kept in mind.1,5
Purtscher retinopathy (PR) diagnostic criteria are clinical, being necessary at least three of the following five points: Purtscher flecken, retinal hemorrhages, typically no more than ten, cotton wool exudates with a predisposition for the posterior pole, compatible etiology and ancillary test results matching with the condition. 1 Four of them patent at the initial presentation, with the occurring of hemorrhage later in time. Hypertensive retinopathy could mimic the condition, but no hypertension neither other typical signs such as macular star hard exudates configuration or disc swelling were found in our patient. 6
Among all clinical signs, two points makes Purtscher flecken remarkable, on the one hand they are considered pathognomonic; on the other, they tend to be overlooked by the usually much numerous cotton-wool exudates. However, they are described as well-defined white lesions comprised within 50 um from its surrounding arterioles, but always leaving healthy retina in between.
Regarding diagnosis, multimodal image assessing needs to be performed, as it offers diagnostic and prognostic clues.6–8 OCT normally evidences macular edema, less frequently becoming cystic and accompanied with NSD, as in our case. PAMM like lesions have recently been associated with the condition, 6 manifesting as hyperreflective bands in the INL, possibly being the OCT correlate of the Purtscher flecken lesions. OCT-A is a non-invasive tool helping in the diagnosis, assessment of prognostic factors and better understanding of the etiopathogenesis of the retinopathy. PR is likely to be caused by the occlusion of precapillary arterioles in the context of endothelial dysregulation. 1 Herein, ischemia plays an important role. Consequently, OCT-A is key, as it may be more sensible than FFA in the detection of subtle ischemia, microvascular occlusions and infarcts. In our patient, OCT-A demonstrated hypoperfusion in the inner and outer plexiform layers as flow-devoid patches bigger and better defined than the superior cotton-wool exudates, probably being a consequence of the ischemic affront. Furthermore, some of them remained in follow up exams. Vascular stops compatible with precapillary arteriole occlusions were also noted. The honeycomb appearance of the choriocapillaris implied damage of the lobular irrigation of the choroid. 6 Although not proved, those OCT-A signs, hypoperfusion of the retinal plexuses and choroid, has been suggested as prognostic factors, which proved true in our case, where a marked atrophy of retina and choroid developed and BCVA worsen to counting fingers.
Concerning treatment, it is not clear which the proper approach should be, as a benefit from the administration of corticosteroids has not been demonstrated. 1 This being the reason why some authors prefer to observe and limit treatment to the baseline pathology. Nonetheless, due to CME along with NSD, 0,7 mg dexamethasone intravitreal implant was injected in our patient. Unfortunately, our patient did not appear in consultations until five months from the injection, hampering a proper evaluation of the potential impact of the treatment. Finally, it seems to be clearer that follow up visits are vital, being recommended at one, two and six months from presentation. 1
To the best of our knowledge this would be the first case of a SLE Purtscher-like retinopathy in which OCT-A has been employed.
Conclusions
An ophthalmic examination should be carried out on each patient debuting with SLE, in which OCT-A, in the case of signs fitting with PR, can help in the diagnosis and the appraisal of final visual outcome.
Footnotes
Author contributions
Writing—original draft preparation, E.G.S. and C.M.R.; writing—review and editing, M.D.S. and P.U.; conceptualization, resources and supervision, D.S.A. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Informed consent statement
Informed consent was obtained from all subjects involved in the study.