
Abstract
Purpose
To investigate the impact of the delay in patient appointments caused by the COVID-19 pandemic and the triage system on the glaucomatous disease of patients in a London tertiary hospital.
Methods
Observational retrospective study that randomly selected 200 glaucoma patients with more than 3 months of unintended delay for their post-COVID visit and other inclusion and exclusion criteria. Demographic information, clinical data, number of drugs, best-corrected visual acuity (BCVA), intraocular pressure (IOP), visual field (VF) mean deviation (MD), and global peripapillary retinal nerve fibre layer (pRNFL) thickness were obtained from the pre- and post-COVID visit. At the post-COVID visit, the clinical outcomes subjective clinical concern and change of treatment or need for surgery were also annotated. The variables were stratified by glaucoma severity (according to the MD into early, moderate and advanced) and by delay time (more and less than 12 months) and analysed using SPSS.
Results
We included 121 eyes (from 71 patients). The median patient age was 74 years (interquartile range -IQR- 15), 54% were males and 52% Caucasians. Different glaucoma types and all glaucoma severities were included. When data was stratified for glaucoma severity, at the pre-COVID visit, significant differences in BCVA, CCT and IOP were observed and there were significantly higher values in the early glaucoma group. The median follow-up delay was 11 months (IQR 8), did not differ between the glaucoma severity groups and did not correlate to the glaucoma severity. At the post-COVID visit, significant differences in BCVA, IOP, and Global pRNFL thickness were observed between the glaucoma severity groups, as lower BCVA and higher IOP and pRNFL thickness were observed in the early glaucoma group. At the post-COVID visit there was cause for concern in 40 eyes: 5 were followed more closely, 22 had a change of treatment and 13 were booked for surgery (3 for cataract and 10 for glaucoma surgery). However, the number of eyes with causes for concern were similar between the glaucoma severity groups and there was no correlation between these clinical outcomes and the delay of the post-COVID visit. The number of topical hypotensive medications increased significantly after the post-COVID visit, higher number of medications were observed in the advanced glaucoma group. When differences of IOP, MD and pRNFL thickness between the pre and post-COVID visit, only the MD difference was significantly different between the glaucoma severity groups because it was higher in the severe group. When data was stratified for delay longer or shorter than 12 months, no differences were observed between the groups except at the pre-COVID visit, when the numbers of patients with MD deviation >−6 dB had longer delay time. When differences in IOP, MD and RNFL thickness were calculated, only the pRNFL thickness showed significant differences between the delay groups, because it was higher in the longer delay group. Finally, when paired analysis of the variables at the pre- and post-COVID visits, stratified by glaucoma severity and delay were conducted, although there were no significant differences in IOP in any group, the BCVA decreased significantly in the overall group and in the longer delay groups, the number of hypotensive drugs increased significantly overall and in the moderate and advanced glaucoma, the MD of the VF worsened significantly in the overall group and in the early glaucoma and longer delay groups and the pRNFL thickness decreased significantly in all groups.
Conclusions
We document that delayed care impacts negatively on the glaucomatous disease of our patients because at the post-COVID visit there were reasons for clinical concern in a third of eyes that resulted in change of treatment or surgery. However, these clinical consequences were not related to IOP, glaucoma severity or delay time and reflect that the triage methods implemented worked adequately. The most sensitive parameter to indicate progression in our sample was the pRNFL thickness.
Keywords
Introduction
Since the declaration by the World Health Organization of the coronavirus pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on 11th March 2020, multiple measures were implemented worldwide to try to decelerate the spread of the virus and minimize its impact on healthcare systems. In the United Kingdom (UK), the first lockdown began on the 23rd of March 2020 and ended on June 30th 2020. By August 2020, COVID-19 cases and deaths were 313,798 and 46,706 respectively (472 cases and 70 deaths per 100,000 population), with London being the most affected city in the UK. 1 As in other countries, initially all face-to-face clinic appointments and elective surgeries were cancelled.
Ophthalmology is one of the medical specialties that requires most face-to-face contact with patients, where social distancing is not possible, the use of reusable equipment is necessary and there are many “high-risk high-touch” surfaces.2,3 In addition, transmission can occur from airborne particles onto the conjunctiva, with conjunctivitis being in some cases the presenting symptom.4,5 Contact with ocular secretions can contaminate reusable equipment and infect clinicians, which can in turn increase community transmission.6–9 In consequence, ophthalmologists were urged to discontinue non-urgent care. 10 Since ophthalmic visits and surgeries are usually for non-life-threatening conditions, 11 ophthalmology consultations decreased worldwide during the pandemic. 12
Glaucoma is the leading cause of irreversible vision loss worldwide13,14 and the asymptomatic nature of the disease may represent a particular disadvantage during COVID. Other medical specialties have turned to telemedicine applications, but tele-ophthalmology is at present unsuitable to evaluate glaucoma progression.8,15 Also, while phone consultations may be useful for screening in some ophthalmic subspecialties such as medical retina or cornea, self-reported glaucoma symptoms are often unreliable and related to the adverse effects of topical treatment. 15 However, phone consultations may even be useful in glaucoma because they increase understanding of the glaucoma condition, discussion of compliance and advice on optimizing treatment application.
The Western Eye Hospital is one of the busiest outpatient clinics in London, and the glaucoma department is a tertiary referral centre. During lockdown and for some time afterwards, the risk of COVID-19 transmission was deemed unacceptable for routine, low-risk attendances that were cancelled. However, a strategy was developed to reduce global outpatient attendance, but at the same time, provide care for patients in need. Thus, new protocols were implemented to enable COVID19 workflows in the glaucoma clinic. 8 Stratification became of the utmost importance. Patients were triaged to be able to provide adequate care for high-risk glaucoma patients, who were scheduled for face-to-face appointments and surgical interventions when necessary. 8 Clinical prioritization according to the medical records was hence used in our centre but also in many centres worldwide.16,17
The aim of this study was to estimate the impact of delayed care secondary to COVID-19 in the glaucomatous disease of our patients in the Western Eye Hospital (WEH) in London (UK). It is hoped that these analyses will provide a valuable insight into the understanding of delayed face to face glaucoma care and the management of patients in possible future situations of difficult access to medical care.
Methods
This is an observational retrospective study. The selection of the patients was as follows (Figure 1):
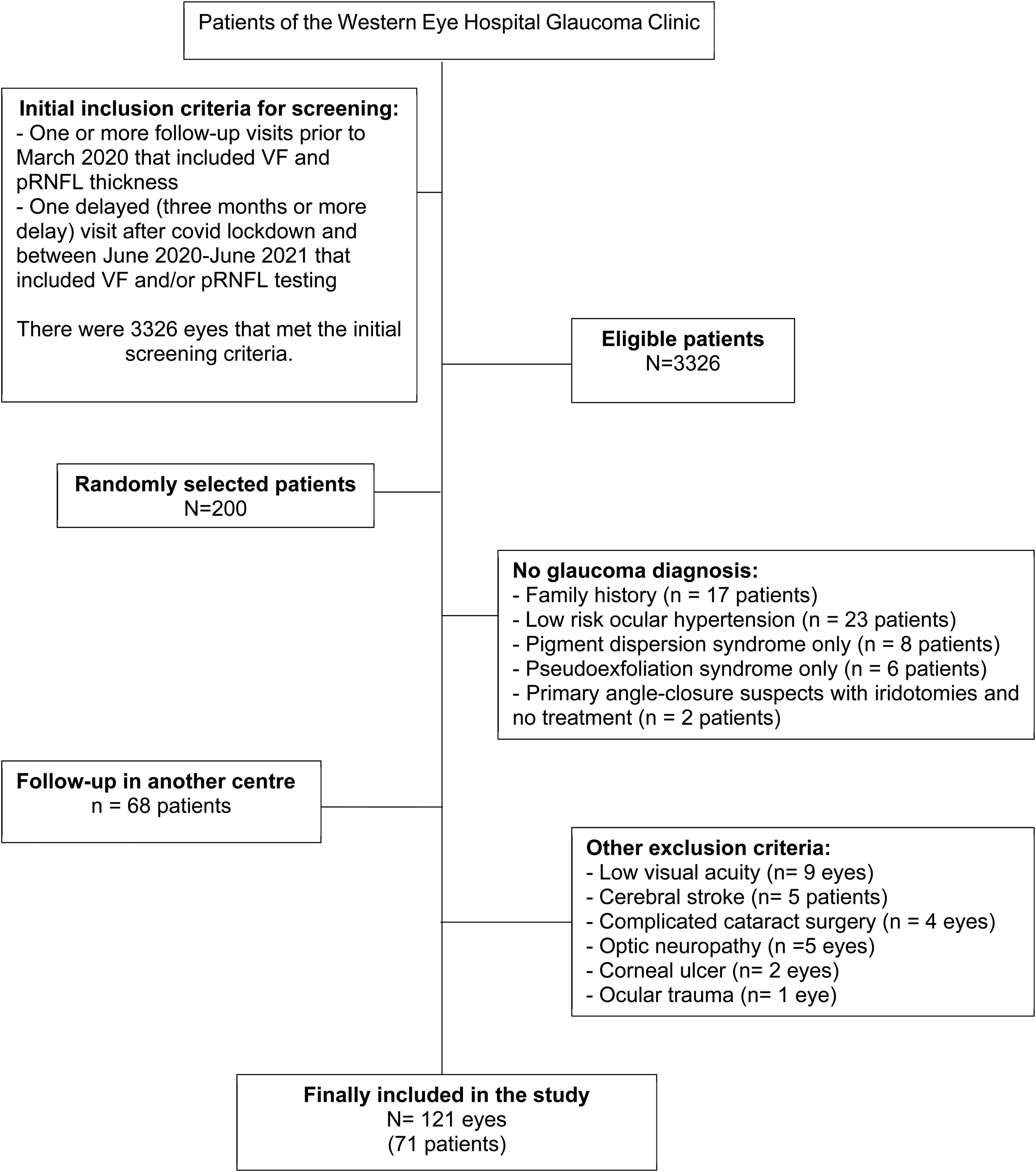
Consort diagram of patients in the study.
Initial inclusion criteria for screening
Patients from the Glaucoma Unit at the WEH were identified using the electronic medical record system (Medisoft Ophthalmology, Medisoft Limited, Leeds, UK).
We selected the patients that had visits that included 30-2 or 24-2 visual field (VF) testing (Humphrey and/or Octopus) and peripapillary retinal nerve fibre layer (pRNFL) thickness evaluation with the optic disc circle protocol of the Optic Coherence Tomography (OCT; Spectralis, Heidelberg), at least in three visits before the pandemic, and one delayed (three or more months) after the COVID lockdown, this last one between June 2020 and June 2021.
The delay of the post-COVID visit was determined by the triage system that followed the Joint Royal College of Ophthalmologists and United Kingdom Éire Glaucoma Society GLAUC-STRAT-Fast risk stratification tool that takes into account various demographic and disease variables to orient patient management. 18
Random selection of patients
There were 3326 patients that met the initial screening criteria. To obtain a representative sample, 200 patients were randomly selected using the Excel RAND function.
Inclusion and exclusion criteria
The medical records of the 200 patients selected were screened for the following inclusion and exclusion criteria:
Inclusion criteria were: [1] glaucoma diagnosis prior to the pre-COVID visit; [2] complete medical records that included all variables necessary for the study (see below, Figure 1).
Exclusion criteria were: [1] diagnosis other than glaucoma (i.e., family history of glaucoma, ocular hypertension, pigment dispersion syndrome, pseudoexfoliation syndrome; [2] follow-up in another centre between the pre- and post-COVID visits; [3] BCVA > 1 logMAR; [4] other ocular or systemic pathologies that could influence VF testing or the pRNFL thickness (i.e., optic neuropathies, corneal or retinal diseases); [5] complicated cataract surgery.
The medical records of the patients were evaluated independently by two researchers (BBB, BVV). The following demographic and clinical data were obtained: age, sex, race, arterial hypertension, diabetic status and dyslipidaemia.
From the pre-COVID visit, the following variables were registered: type of glaucoma, topical hypotensive medication, previous cataract or glaucoma surgery, central corneal thickness (CCT), refractive error (spherical equivalent), BCVA according to the logMAR scale, mean time between the previous recorded pre-COVID visits, mean deviation (MD) of the VF, IOP, global pRNFL thickness and cup to disc ratio.
From the delayed post-COVID visit, we annotated: the delay in follow-up (difference in months between the appointed and the rescheduled post-COVID visit), BCVA, IOP, MD of the VF and global pRNFL thickness. At this visit, three types of clinical outcomes were evaluated: subjective clinical concern, need for change of topical treatment and need for glaucoma or cataract surgery. Subjective clinical concern was evaluated in accordance with the NICE guideline for glaucoma 19 and included the other two clinical outcomes because in most patients with clinical concern treatment was changed or surgery indicated. At this post-COVID visit, the number of topical hypotensive drugs after the visit and change of treatment was annotated.
Statistical calculations and comparisons were performed using Statistical Package for Social Sciences (version 25.0, SPSS Inc., Chicago, IL, USA). Analysis of the data was performed altogether and by stratification of the eyes by glaucoma severity (according to the MD of the VF and the Hodapp-Parrish-Anderson classification 20 into: early MD ≥ −6 dB, moderate −6 to −12 dB or advanced MD ≤ −12 dB glaucoma. Qualitative data are expressed as their frequency distributions. Quantitative data are provided as the median and interquartile range (IQR). The statistical significance of the differences between the continuous values of the stratified data were compared using the Mann-Whitney U-test or a Kruskal-Wallis test. The statistical significance of the differences between qualitative variables was assessed using Chi-square test. Paired analysis of pre- and post-COVID variables was also performed using a Wilcoxon matched-pair signed-rank test. Relationships between variables were also assessed using Spearman's Rho correlation. p < 0.05 was considered statistically significant.
Results
From the 200 randomly selected patients, only 121 eyes of 71 glaucoma patients met all the inclusion and exclusion criteria and were finally included in the study (Figure 1). The following patients and/or eyes excluded from the study and the reasons for exclusion were: diagnosis other than glaucoma (n = 56 patients), follow-up in another centre (n = 68 patients), low visual acuity (n = 9 eyes), cerebral stroke (n = 5 patients), complicated cataract surgery (n = 4 eyes), optic neuropathy (n = 5 eyes), corneal ulcer (n = 2 eyes) and ocular trauma (n = 1 eye).
Of the 71 patients included in the study, 38 (54%) were males, and 33 (46%) females. The median age of the patients was 74 years (IQR 15). As for race, 37 patients (52%) were Caucasian, 10 (14%) Asian, 5 (7%) Caribbean, 13 (18%) African, and in 6 (8%) race was not stated. Thirty-four patients (48%) had arterial hypertension, 18 (25%) had diabetes mellitus and 30 (42%) had dyslipidaemia.
The pre- and post-COVID characteristics of all patients, stratified by glaucoma severity and their comparisons are depicted in Table 1. From the 121 eyes included, 63 had early glaucoma, 23 moderate glaucoma and 35 advanced glaucoma and various types of glaucoma were included, but no significant differences of these types were found between the severity groups. There were significant differences between groups on the number of patients that had undergone cataract or glaucoma surgery because the advanced glaucoma group had a higher number of these surgeries (45.7%). The time between the pre-COVID visits differed significantly between the groups, as it was shorter in the severe and moderate glaucoma groups when compared to the early glaucoma group.
Clinical pre- and post-COVID characteristics of all patients and stratified by the pre-COVID mean deviation of the visual field.
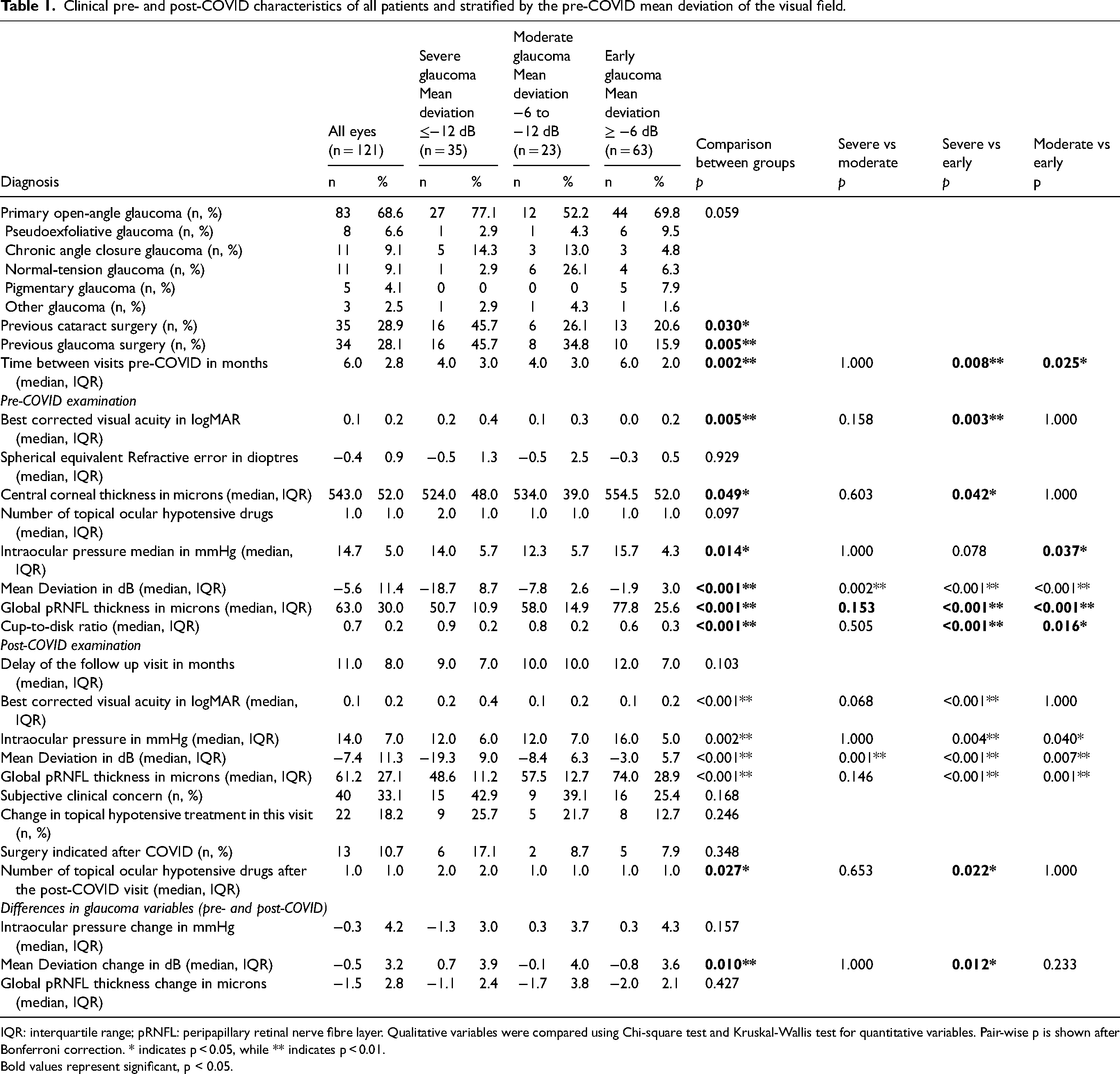
IQR: interquartile range; pRNFL: peripapillary retinal nerve fibre layer. Qualitative variables were compared using Chi-square test and Kruskal-Wallis test for quantitative variables. Pair-wise p is shown after Bonferroni correction. * indicates p < 0.05, while ** indicates p < 0.01. Bold values represent significant, p < 0.05.
At the pre-COVID visit, the median BCVA was 0.1 (IQR 0.2) and there were significant differences of this parameter between groups, as it was higher in the early glaucoma group when compared to the severe glaucoma group. Central corneal thickness was significantly different between groups; it was higher in the early glaucoma group when compared to the severe glaucoma group. The median number of topical hypotensive medications was 1 (IQR 1) and there were no significant differences between groups. The median IOP was 14.7 (IQR 5) and there were significant differences between the groups, as it was higher in the early glaucoma group when compared to the moderate group. At this visit, there were also significant differences in the VF MD, the pRNFL and the cup to disc ratio between groups.
The median delay of the post-COVID appointment was 11 months (IQR 8) and there were no significant differences of this time between groups. This follow-up delay time did not correlate with the MD of the VF (Spearman's Rho correlation; p > 0.05).
At the post-COVID visit, significant differences between the three glaucoma severity groups were observed in the following variables: BCVA (lower in the severe glaucoma group when compared to the early glaucoma group), number of topical ocular hypotensive drugs (higher in the early glaucoma group), IOP (higher in the early glaucoma group) and global pRNFL thickness (higher in the early glaucoma group).
At the post-COVID visit, there was cause for clinical concern in 40 eyes (33%). The causes for clinical concern were: IOP above target pressure (21 eyes), definite VF progression (4 eyes), structural progression (5 eyes), peripapillary haemorrhage (3 eyes), allergy to topical treatment (2 eyes), non-compliance (4 eyes) and IOP above target pressure (1 eye). Thus, at the post-COVID visit, a change of treatment was indicated in 22 eyes (18%), 13 eyes (11%) were appointed for surgery (3 cataract, 3 iStents®, 1 Preserflo™ implant, 1 trabeculectomy, and 6 selective laser trabeculoplasties) and 5 eyes were only followed more closely. We did not observe significant differences in the number of patients with clinical concern, treatment change or indication of surgery between the glaucoma severity groups.
Differences between the pre- and post-COVID visits were calculated for IOP, VF MD and pRNFL thickness and compared between the glaucoma severity groups. Overall, there were small decreases of the IOP, MD and pRNFL thickness, but only the MD showed significant differences between the severe and the early glaucoma groups.
Next, we analysed the data stratified by appointment delay lower or higher than 12 months (Table 2). Similar baseline characteristics were observed in both groups. However, when we analysed the pre-COVID VF MD (higher or lower than 6 Db), the patients with VF MD worse than −6 dB were more frequently seen earlier than 12 months. At the post-COVID visit we did not find differences in the different variables (IOP, MD, clinical concern, change of treatment or need for surgery) between the two delay times groups. However, when analysing the calculated differences between the pre- and post-COVID variables in the two delay times groups, the patients with longer than 12 months delay showed a significantly greater decrease only in global pRNFL thickness.
Clinical pre- and post-COVID characteristics of the patients stratified according to visit delay.
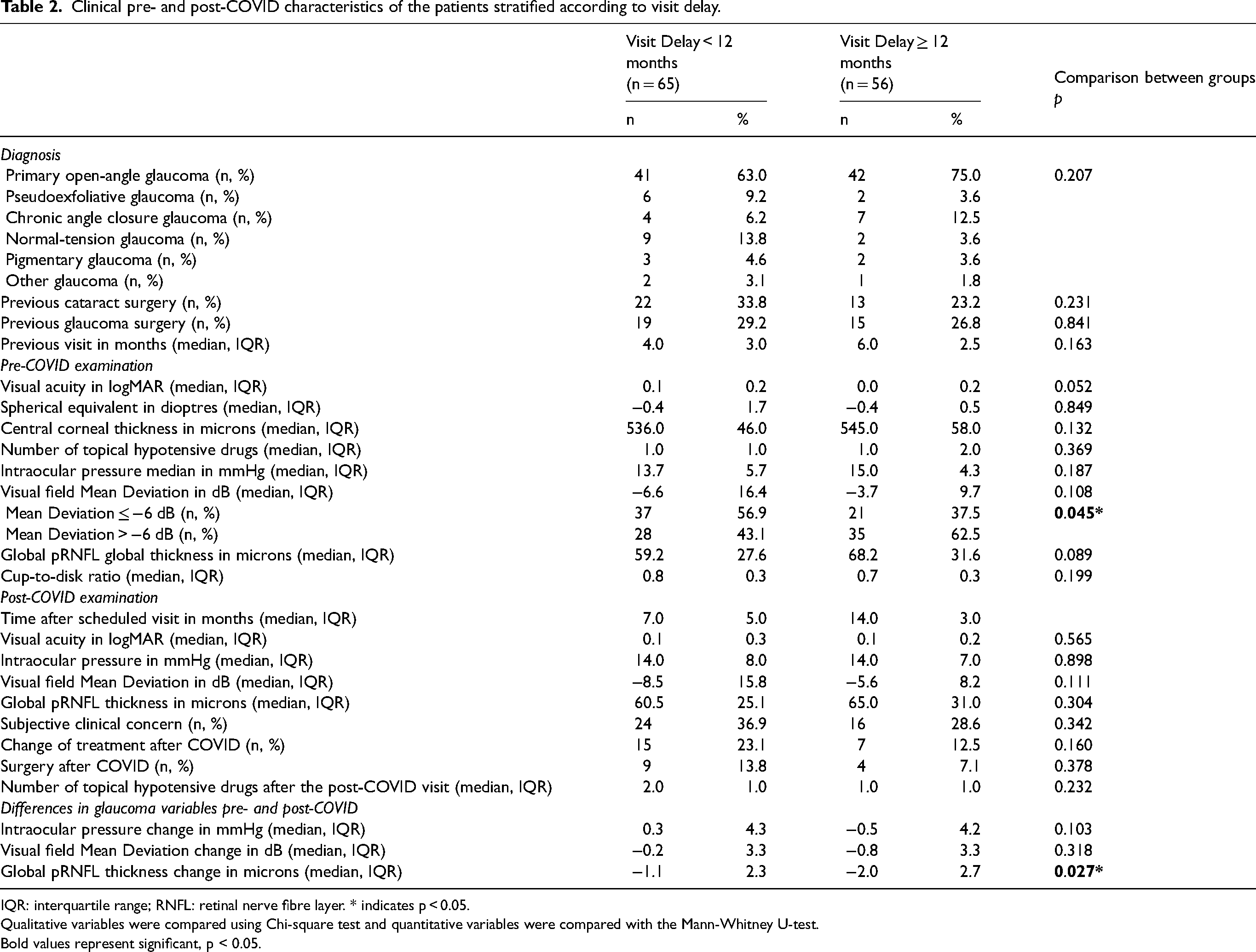
IQR: interquartile range; RNFL: retinal nerve fibre layer. * indicates p < 0.05.
Qualitative variables were compared using Chi-square test and quantitative variables were compared with the Mann-Whitney U-test. Bold values represent significant, p < 0.05.
Finally, we carried out a paired analysis of the variables between the pre- and post-COVID visits, stratified by glaucoma severity and delay lower or higher than 12 months (Table 3). We found that the BCVA worsened significantly in the overall group and in the group with delay longer than 12 months. Overall and in the patients with moderate and advanced glaucoma, the number of hypotensive drugs increased significantly after the post-COVID visit. Although no significant changes in IOP were detected between the pre- and post-COVID visits in any group, the VF MD worsened significantly in the overall group, in patients with early glaucoma and in the group with delay longer than 12 months. Also, the global pRNFL thickness decreased significantly in all glaucoma severity and delay time groups.
Paired analysis of pre- and post-COVID visual acuity and glaucoma variables
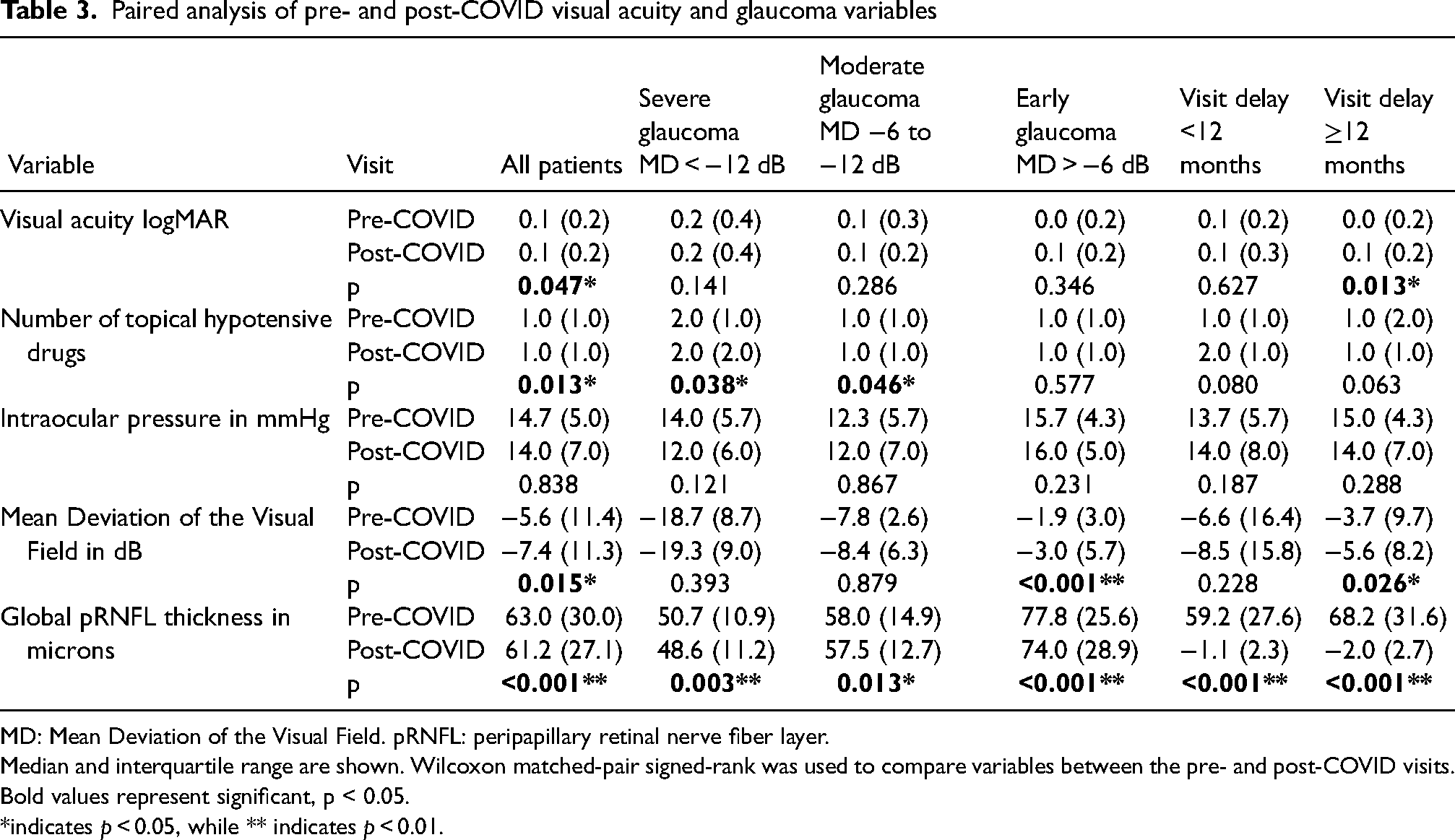
MD: Mean Deviation of the Visual Field. pRNFL: peripapillary retinal nerve fiber layer.
Median and interquartile range are shown. Wilcoxon matched-pair signed-rank was used to compare variables between the pre- and post-COVID visits. Bold values represent significant, p < 0.05. *indicates p < 0.05, while ** indicates p < 0.01.
Discussion
Since COVID-19 outbreak, health care systems have been under enormous stress and ophthalmology practices have been significantly affected. Once the first wave of the pandemic subsided and outpatients started to attend hospital appointments, health care was prioritised, usually determined by ophthalmologists on review of patients’ records. 21 Electronic medical records have greatly assisted in this task, as compared to a paper record.
In glaucoma clinics, rescheduling of appointments in the early post-COVID was a major challenge. The consequences of the lack or delay in follow-ups, particularly during the earlier waves of the pandemic have not been thoroughly investigated. However, negative impacts caused by delayed glaucoma follow ups have been reported before. In 2009, the National Patient Safety Agency reported 44 glaucoma patients with deterioration of vision, including 13 with total vision loss that were attributed to delayed follow-up appointments. 22 Consequently, Davis et al. 23 in the Moorfields Eye Hospital, identified 145,234 patients lost to follow-up (5251 with glaucoma) between the years 2007 and 2012. Of these, 12,316 required clinical review after examination of medical records that identified 16 major incidents of vision loss, 14 in glaucoma patients. Also in the UK, Foot and MacEwen 24 evaluated the effect of delays in ophthalmic care during a 12-month study period and one hundred sixty-nine cases (70 with glaucoma) with sight loss due to unintended delay were identified. In another study of the Moorfields’ in a series of 100 glaucoma patients whose appointment had been rescheduled, 8% of patients were considered to have progressed during visits, progression being potentially attributable to the delay in health care. 25
Evidence undoubtedly proves that delaying glaucoma follow-ups past initial recommended time lapses is responsible for glaucoma progression in some patients. To analyse the change in glaucoma patient experience and attitudes caused by the COVID pandemic, a survey was performed in 126 patients attending a glaucoma clinic at Cambridge in September 2020. 26 At this timepoint, just after the pandemic outbreak, more patients were likely to agree less with the responses related to their understanding of glaucoma treatment and confidence in their treatment team. 26 These findings are of immense clinical relevance given that impaired confidence in the glaucoma team may affect treatment compliance that can contribute to disease progression. In fact, Subathra et al. revealed that 57.3% of 363 patients lost to follow-up reported non-adherence to medication in a tertiary eye care centre in India. 27 Nevertheless, there are no studies regarding the effect of COVID-19 lockdown in documented glaucoma progression.
In this article we have analysed the impact of delayed appointments on glaucoma patients at a tertiary centre, the WEH. At our centre, all face-to-face clinic appointments and elective ophthalmology surgeries were initially cancelled. Patients were phoned and those with higher glaucoma progression risk were recommended to come in for face-to-face clinical examination and assessment. Glaucoma patients were triaged on the basis of their COVID and medium-term glaucoma risks, similarly to those described by the Moorfields team. 28 In our sample, although no significant differences were found in delay between the three glaucoma severity groups, the median follow-up delay was lower in the advanced glaucoma group, followed by the moderate and early glaucoma groups.
Our findings also show that the BCVA significantly worsened in those patients with longer follow-up delay, and we think that this could be cataract-related, given that no difference in subjective clinical concern was detected between the shorter and the longer delay time groups. The number of topical hypotensive drugs increased significantly overall and in the advanced and moderate glaucoma groups, as more treatment was added at the post-COVID visit and in no patient was the number of drugs reduced. There were no significant changes in IOP between the pre- and post-COVID visits, and this could indicate that although different groups had different IOP targets, IOP control was similar in all groups. Although there were no differences in IOP in the different groups, there was cause for clinical concern in 40 eyes. Thus, clinical concern, although subjective, is clinically more relevant and takes better into account possible disease progression than IOP.
Interestingly, in this study, the VF MD worsened significantly between the pre- and post-COVID visits in the overall group but also in the early glaucoma and longer delay groups. This suggests that a proportion of patients with early glaucoma (and longer delay) progressed between appointments, while those with moderate or advanced forms of the disease did not progress. We are tempted to speculate that these did not progress because they had shorter delay due to appropriate triage. However, this significant MD increase in the early glaucoma group could also be due to a higher IOP target, as the IOP was higher in the early glaucoma group at both visits. The MD increased between visits −1.8, −1.1 and −1.9 in the overall, early glaucoma and longer delay groups, respectively. As the mean delay time was 11 months, and glaucoma follow up is usually between 4 and 6 months, these losses indicate MD loss during 16 months. However, these losses are clinically relevant as losses between −1 and −2 dB/year are considered fast rates of progression.29,30 Therefore, our results highlight the importance of efforts to not delay in-person visits in those with advanced glaucoma and, although they can be more spaced, to still recommend visits in patients with milder forms of the disease given that it is difficult to identify which of these patients are starting to progress.
When our variables were stratified into two groups according to delay, shorter or longer than 12 months, we did not find significant differences in IOP or VF MD between these groups. However, we found significant pRNFL thinning in the longer delay group, and we also found significant decrease of the pRNFL thickness between the pre-COVID and post-COVID visit in all the glaucoma severity and delay time groups. Thus, the pRNFL thickness was the most sensitive parameter for progression in our study. We found median decreases of the pRNFL thickness of −1.1 and −2 µm in the shorter and longer delay groups. As we have pointed out before, these losses represent losses not per year but per 15 months but, because the mean rate of change of the pRNFL thickness caused by age is between −0.1 and −0.6 µm/year,31,32 these differences are clinically relevant and possibly responsible at least in part for the clinical concern found in 40 eyes. Despite these losses, there were no differences in clinical outcomes between the glaucoma severity groups, possibly illustrating that a good prioritisation system had been implemented at the WEH.
At the post-COVID visit, 13 eyes were appointed for surgery, but only one of the eyes received a trabeculectomy. Despite the effort to maintain urgent glaucoma ophthalmologic care, glaucoma surgical practices in the UK changed considerably due to COVID-19. In a UK-based survey, 33 61% of ophthalmologists reported having modified their glaucoma surgery practices, 43% having reduced trabeculectomies. The most common reason for shifting away from trabeculectomy was the desire for less overall patient contact, and reducing the risk of COVID-19 transmission avoiding aerosol generating procedures. Diode laser cyclophotocoagulation, deep sclerectomy and Preserflo were frequently reported alternatives. In Italy, traditional filtration surgery reduced from 62.8% the previous year to 25%, with minimally invasive glaucoma surgeries (MIGS) and nonpenetrating surgeries being performed more compared to before the pandemic. 34 This agrees with our sample, where only one patient underwent trabeculectomy after COVID-19. Instead, MIGS and SLT were performed more commonly, illustrating the shift of glaucoma procedures away from trabeculectomy.
In COVID-19 era, the short-term effects of pandemic related unintended treatment lapses have been evaluated with respect to neovascular age related macular degeneration (nAMD) patients. Although most ophthalmological societies supported intravitreal injections during the pandemic, there was a dramatic decrease in patient attendance for injections, and the reported number of injections decreased by 50–90%.35–38 Delays of more than 3 months in these patients were responsible for visual loss, exudation and increased central subfoveal thickness.39–42 Also, a proportion of patients with dry AMD in the fellow eye before COVID-19 pandemic evolved to nAMD. 43
In nAMD, delay has proven to be significantly associated with worse short-term outcomes. The consequences of lack of treatment are evident even before 3 months of treatment delay,44,45 causing a meaningful increase of large submacular hemorrhages. 46 This compares to glaucoma patients, where vision loss due to glaucoma progression is slower and longer periods of uncontrolled IOP are normally needed to sustain damage. In addition, glaucoma drugs may reduce the speed of glaucoma progression even in sub-optimally controlled patients and the effects of ophthalmological care delay might still be clinically undetected, ‘in the shadows.’ Added to this, it is easier to identify nAMD patients who need attention (visual acuity loss, distortion), while glaucoma progression is more often asymptomatic in the earlier stages – this may result in a continued ongoing reduction in patients seeking health care. Hence, the consequences of COVID-19 in glaucoma patients are still unclear and further prospective studies will be needed.
Some limitations of the present study should be acknowledged. Firstly, it represents the findings in a sample of 200 randomly selected patients from the WEH database and might not fully represent the impact of COVID-19 in glaucoma patients in our centre or in other centres. Secondly, only those who had undertaken a face to face visit post-COVID with VF testing after the first lockdown were included. This might have influenced the sample as some patients at that point may have not been tracked. Finally, since the delayed post-COVID visits were triaged according to risk progression factors, and we did not include patients with delay shorter than 3 months, it is reasonable to assume that this sample does not contain some high-risk patients that may have been asked to attend sooner and their delay possibly did not reach 3 months. We believe that the effects of the triage are reflected in our study, because the time between the pre- and post-COVID visits were shorter in the groups with higher MD and longer in the groups with lower MD. Furthermore, although there were no significant differences on the delay between the glaucoma severity groups, it tended to be shorter in the moderate and advanced glaucoma groups. This demonstrates in part a robust triage process by the WEH ophthalmologists. Finally, another caveat of our study is that we do not have a control group to compare our findings.
In conclusion, we document that delayed care impacts negatively on the glaucomatous disease of our patients and causes clinically detectable progression. The most sensitive parameter to detect progression in our sample was the pRNFL thickness. As a result of the advance of the disease, at the post-COVID visit there were there were reasons for clinical concern in a third of eyes that resulted in change of treatment or surgery. However, these clinical consequences were not related to IOP, glaucoma severity or delay time and reflects that the visits of the glaucoma patients were appropriately prioritised according to disease severity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.