
Abstract
Purpose
To evaluate the feasibility and outcomes of phased strabismus surgery under topical anesthesia, with intraoperative comparison of ocular alignment in supine and seated positions.
Methods
This retrospective clinical investigation analyzed the data of patients who underwent phased strabismus surgery with fixed sutures under topical anesthesia. The technique consisted of 2 phases, spaced out with an intraoperative alternate prism cover test (performed in supine and seated positions): (1) surgery on one or two muscles, as defined by a preoperative surgical plan; (2) if judged necessary, a further one-muscle surgery. Surgical success was defined as a residual angle of horizontal and vertical deviation ≤±8Δ and ≤5Δ, respectively, and the presence of single binocular vision in primary position in patients with preoperative diplopia. Follow-up visits were scheduled 1 day, 1 month, and 6 months after surgery.
Results
The review identified 38 patients (age range: 10–80 years). Surgery was well tolerated by all patients. Twelve (32%) required a second phase. No statistically significant differences were found for intraoperative angles of deviation in supine and seated positions. Surgical success was reached, respectively, in 88% and 87% of cases with horizontal and vertical deviation 6 months after surgery. No patients were reoperated during the follow-up period.
Conclusions
Phased strabismus surgery is a feasible technique for various types of strabismus in adults and children. Secondly, intraoperative evaluation of ocular alignment can be performed either with the patient seated or supine, with the same accuracy in terms of surgical success.
Keywords
Introduction
The goal of strabismus surgery is to realign the eyes, thus improving fusion, recovering binocular vision, or enlarging the field of single binocular vision. The surgery is usually performed with fixed sutures under general anesthesia (GA). 1 Several accurate nomograms have been created over time, but the outcomes can be unpredictable in more complicated cases, such as reoperations, restrictive strabismus, moderate or variable angles.2,3
Some authors have supported the use of adjustable sutures (AS) to manage these more challenging situations, arguing that the possibility of refining ocular alignment led to better outcomes 4 ; others have later recommended AS for all types of strabismus surgery when patients are cooperative.5,6
Sutures’ adjustments can be made postoperatively or even intraoperatively if topical anesthesia is used. 7
Despite the initial enthusiasm, AS have not had the expected spread. A lack of standardization of the procedure, additional logistics for adjustments, extra sedation for pediatric patients, and limited substantial benefit in terms of motor success and reoperation rate have contributed to surgeons’ reluctance to adopt the technique. 8
Ideally, topical anesthesia allows to perform an intraoperative alignment check with optional increment of the number of the operated muscles, but without the need of AS. We herein report the outcomes of a phased strabismus surgery with fixed sutures under topical anesthesia, which offered us the possibility to customize the procedure for each patient.
Methods
We reviewed the charts of all patients who underwent surgery according to the technique described below at a single institution (Ophthalmology Unit of St. Anna University Hospital of Ferrara, Italy) from June 2020 until June 2021. The study adhered to the principles outlined in the 2013 Declaration of Helsinki and was approved by the local Ethics Committee.
Complete ophthalmological and orthoptic evaluations were carried out one-week prior surgery, including assessment of the angle of ocular deviation at distance and near vision with Alternate Prism Cover Test (APCT) or Krimsky test, ocular motility in the nine cardinal positions of gaze, and stereopsis measurement with TNO and Frisby stereo tests. A detailed surgical plan was created for each patient, indicating the muscles that would have been operated on in phase 1 and in phase 2 only if deemed necessary after intraoperative APCT. These plans were based on our previous experience. In brief, 1 mm of lateral rectus (LR) recession accounts for 2Δ; 1 mm of medial rectus (MR) recession for 3–4Δ; 1 mm of LR resection for 3Δ; 1 mm of MR resection for 4Δ; 1 mm of LR advancement for 6Δ; 1 mm of MR advancement for 6–7Δ; 1 mm of MR plication for 4–5Δ; 1 mm of superior rectus advancement for 4–5Δ. We graded the overaction of the inferior oblique muscle from 0 (no overaction) to 4+ according to the amount of overelevation in adduction. 9 For overaction up to 2+, we adopted Fink recession, where the muscle is placed at the bisector between the inferior rectus (IR) and the LR and corresponds to an 8 mm-recession; for overaction greater than 2+, we placed the muscle alongside the IR (this corresponds to a 14 mm-recession).
We used a previously described topical anesthesia protocol: 10 sub-lingual or intranasal midazolam 0.25 mg/kg administered from 20 to 30 min before the entrance in the operating room (OR), followed by instillation of topical benoxinate 4 mg/mL eye drops and then lidocaine 4% eye drops in the conjunctival sac every 5 min before the beginning of surgery. Additional lidocaine 4% eye drops were administered after conjunctival incision and if patients complained discomfort. Pain was assessed using the 4-point Verbal Rating Scale (0 = no pain, 1 = mild, 2 = moderate, 3 = severe). In cases of moderate or severe pain, intravenous injection of propofol 0.3 mg/kg was used. Patient’ vital signs (blood pressure, heart rate and oximetry) were continuously monitored, to promptly identify any oculo-cardiac reflex (OCR) during manipulation and isolation of the muscles. The anesthesiologist was always present in the OR if a conversion to GA became necessary.
The surgical technique consisted of 2 phases, using mainly fixed sutures with limbal approach, and reserving AS (standard sliding noose technique) if deemed necessary. Phase 1 consisted in one or two muscles operated on following the preoperative surgical plan. After an accurate clearance of the visual axis, APCT was performed by an orthoptist under the surgeon's supervision. In case of propofol administration, we waited the time necessary for the patient to be able to adequately answer some simple questions, and at least 10 min for muscle relaxation.
Measurements were recorded in the primary position of gaze while the patient was lying and then sitting on the operating table and fixating on a target at near (33 cm) and at distance (a cross on the ceiling and a target 5 meters away, respectively). The final control was always performed with the patient seated. If further surgery was necessary, phase 2 (one-muscle surgery) was carried out after recreating the operatory field and through administration of lidocaine 4% eye drops.
We considered different surgical goals depending on the presence or absence of fusion potential: patients with esotropia were left within +4Δ or undercorrected by +8 to +10Δ; patients with exotropia were left within −8Δ or overcorrected (esotropia) by +2 to +6Δ; patients with vertical deviations were left within 2–3Δ or 5Δ. In case of preoperative diplopia, the target was to reach no diplopia in primary position and down gaze.
Surgical success was defined as a postoperative residual angle of horizontal deviation ≤±8Δ and of vertical deviation ≤5Δ, and presence of single binocular vision in primary position in patients with preoperative diplopia.
Data were collected at the preoperative evaluation, and 1 day, 1 month, and 6 months postoperatively. The primary outcome measure was the surgical success at each follow-up. The secondary outcome measure was the comparison of intraoperative ocular alignment with the patient in seated and supine positions. All data were entered into the institutional database via Microsoft Excel 2013 (Microsoft Corp., Redmond, Washington). Demographic outcomes were presented as percentages and frequencies for categorical outcomes, whilst continuous variables were reported as mean±standard deviation. A p < 0.05 was considered statistically significant. For the frequencies analysis a Chi square test was used. To compare the amount of ocular deviation in seated and supine positions we used Wilcoxon test (paired samples). To compare different groups, we used Mann-Whitney test (independent samples). To analyse the effect of propofol use we used the ANOVA test.
Results
We identified 38 patients operated on by the same expert surgeon (FF). Twenty-five patients (66%) reached 6 months of follow-up; the remaining 13 patients (34%) did not return due to COVID-19 pandemic or travel issues. There were 12 males and 26 females with a mean age of 47.2±23.9 years (range 10 to 80). There were 9 children (≤18 years old). Twenty-six patients (68%) had pure horizontal deviation: esotropia in 8 cases (7 with potential for bifoveal fusion) and exotropia in 18 (10 with potential for bifoveal fusion). One patient (3%) had pure vertical deviation (with potential for bifoveal fusion), and 11 patients (29%) had a combined horizontal and vertical deviation (11 with potential for bifoveal fusion). Overall, 29 patients (76%) complained preoperative binocular diplopia. Seven patients (18%) underwent previous strabismus surgery. Detailed etiologies of strabismus are reported in Table 1.
Type and etiology of strabismus.
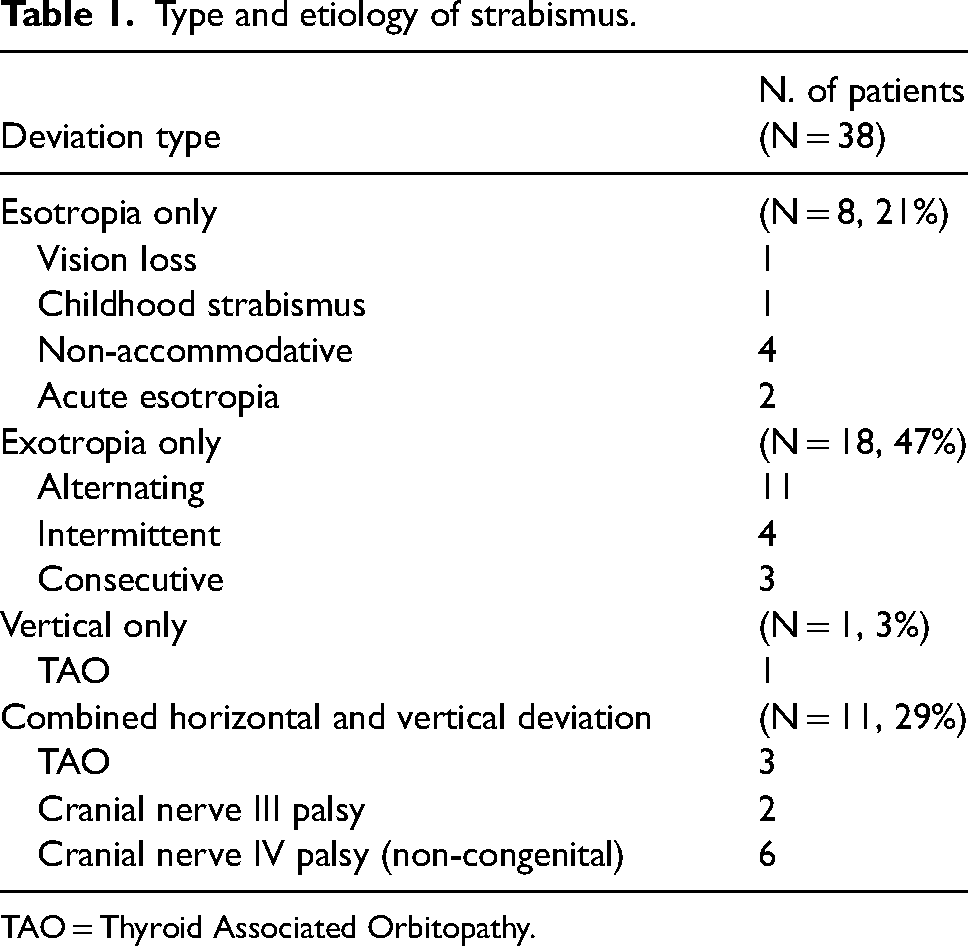
TAO = Thyroid Associated Orbitopathy.
Preoperative angles of deviation for patients with esotropia were 22.1±13.3Δ (0 to 40) and 25.2±11.6Δ (4 to 45) at near and distance, respectively; for patients with exotropia were −28.9±13.1Δ (−4 to −70) and −27.8±11.7Δ (−6 to −65), respectively; for patients with vertical deviation were 17.7±10.8Δ (1 to 40) and 18.1±11.5Δ (1 to 40), respectively.
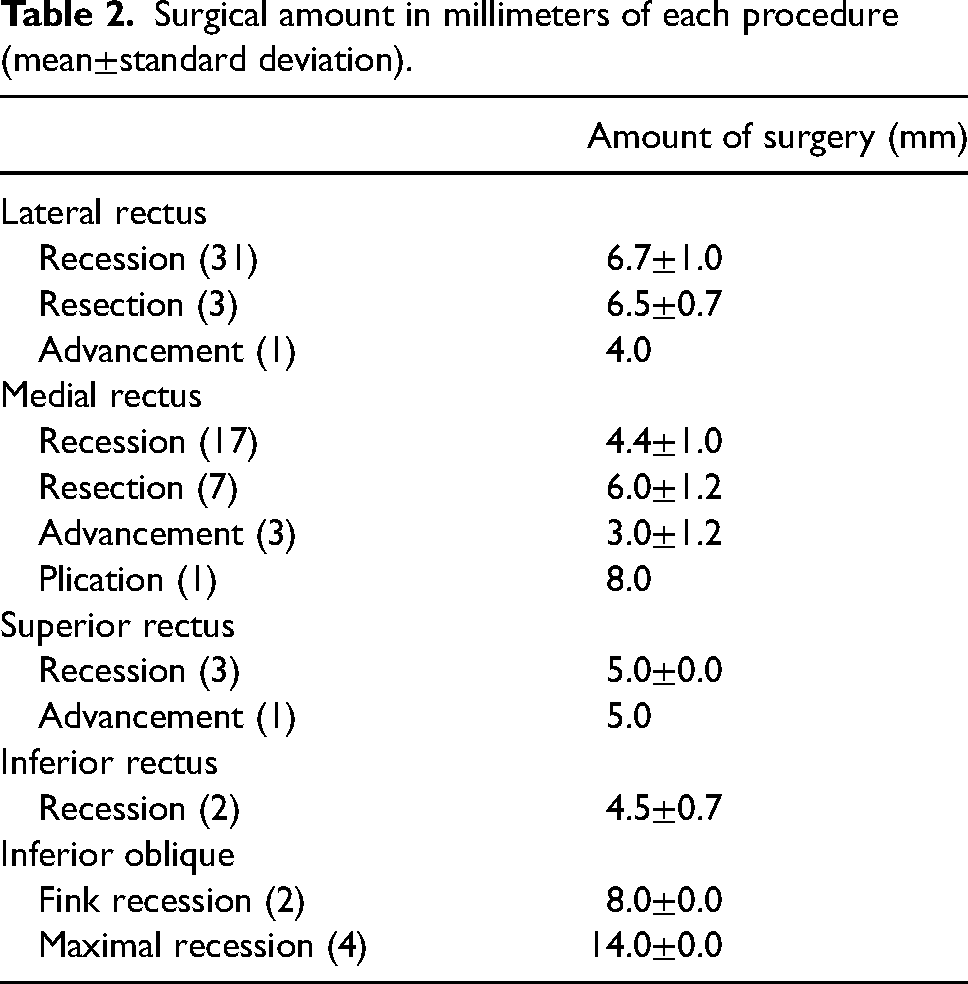
The technique was well tolerated in 31 patients; propofol injection was necessary in 7 patients (18%). Two patients experienced an OCR during muscle manipulation, which required administration of intravenous atropine. In 12 cases (32%) was operated only 1 muscle; in 17 cases (45%) 2 muscles and in 8 cases (21%) 3 muscles. We adopted AS for IR recession in 2 patients with Thyroid Associated Orbitopathy (TAO). Table 2 shows surgical amount of the various procedures carried out.
Surgical amount in millimeters of each procedure (mean±standard deviation).
After intraoperative APCT, 12 patients (32%) required a second phase; 29% of them had pure horizontal deviation, and 38% had combined vertical and horizontal deviations (p = 0.048). Specifically, phase 2 was necessary in 3 cases of non-accomodative esotropia, 1 case of intermittent exotropia, 3 cases of small angle alternating exotropia, 4 cases of reoperation (of which 1 with TAO), and 1 case of IV nerve palsy. Among the patients in whom AS were used, one required intraoperative suture adjustments, while in one the sutures were simply tied off. Mean operating time was 27.9±9.3 min, while mean time necessary for the patients’ recovery and for intraoperative assessment was 23.2±9.9 min.
Intra-operative and post-operative angles of deviation are reported in Tables 3 and 4
Comparison of intraoperative angles of deviation.
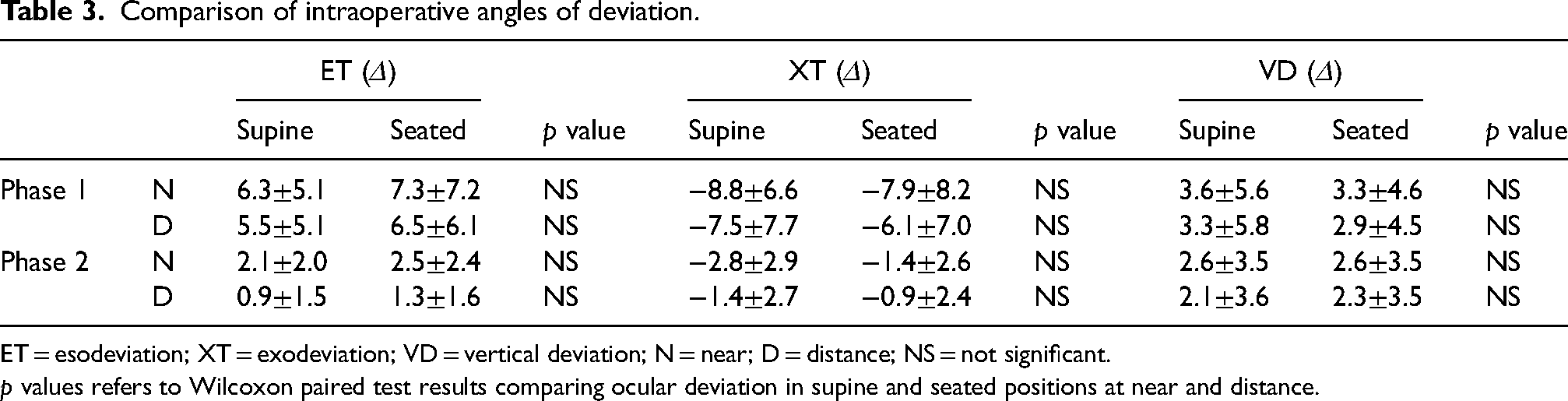
ET = esodeviation; XT = exodeviation; VD = vertical deviation; N = near; D = distance; NS = not significant.
p values refers to Wilcoxon paired test results comparing ocular deviation in supine and seated positions at near and distance.
Comparison between intraoperative and postoperative angles of ocular deviation at distance.
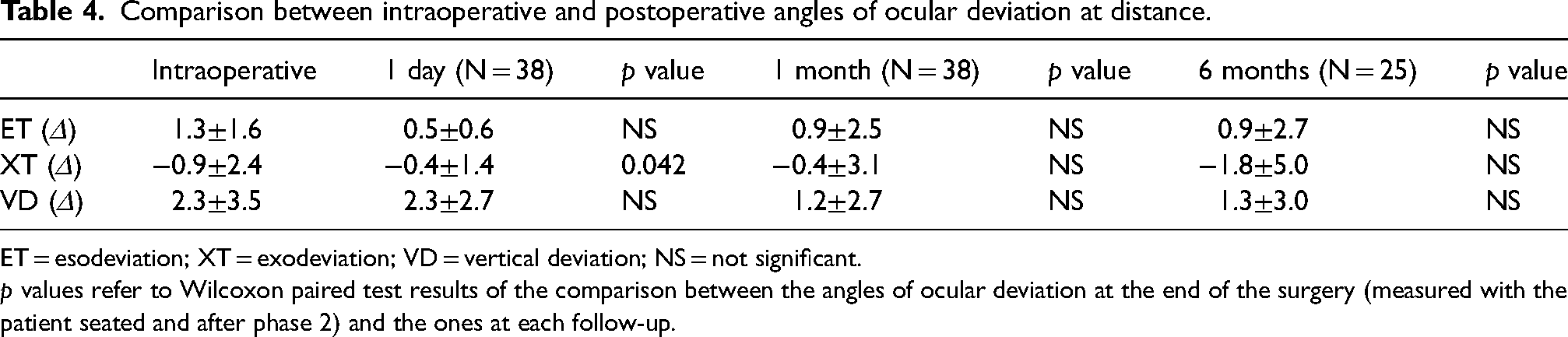
ET = esodeviation; XT = exodeviation; VD = vertical deviation; NS = not significant.
p values refer to Wilcoxon paired test results of the comparison between the angles of ocular deviation at the end of the surgery (measured with the patient seated and after phase 2) and the ones at each follow-up.
Before phase 2, the horizontal deviations in decubitus were −2.4±10.3Δ (near) and −2.1±10.0Δ (distance); with the patient seated were −1.8±11.1Δ (near, p = 0.359) and −1.3±10.2Δ (distance, p = 0.164). The vertical deviations in decubitus before phase 2 were 3.6±5.6Δ (near) and 3.3±5.8Δ (distance); with the patient seated were 3.3±4.6Δ (near, p = 0.243) and 2.9±4.5Δ (distance, p = 0.578). After phase 2, the horizontal deviations in decubitus were −1.2±5.6Δ (near) and −1.2±4.7Δ (distance); with the patient seated were −0.6±6.0Δ (near, p = 0.067) and −0.8±5.2Δ (distance, p = 0.066). The vertical deviations in decubitus were 2.6±3.5Δ (near, p = 0.176) and 2.1±3.6Δ (distance, p = 0.145); with the patient seated were 2.6±3.5Δ (near, =0.069) and 2.3±3.5Δ (distance, p = 0.313). Overall, no statistically significant differences were found between the 2 positions.
When propofol was administered, we did not find significant drift in horizontal deviation one day after surgery (p = 0.188). The mean horizontal drift for all the patients grouped together was −0.4±3.1Δ (range, −12 to 8 Δ) at 1 month, and −1.0±4.0Δ (range, −14 to 8Δ) at 6 months. The mean vertical drift for all patients grouped together −0.3±2.0Δ (range, −6 to 6Δ) at 1 month, and 0.1±3.1Δ (range, −6 to 6Δ) at 6 months. Diplopia resolved in all patients but one with III nerve palsy, who was managed with a small prism and did not require reoperation.
Surgical success rate for horizontal and vertical deviation at distance were, respectively, 100% and 91.7% at 1 day; 93.1% and 94.4% at 1 month; 88.0% and 86.7% at 6 months (Figure 1). No patients were reoperated during the follow-up period.
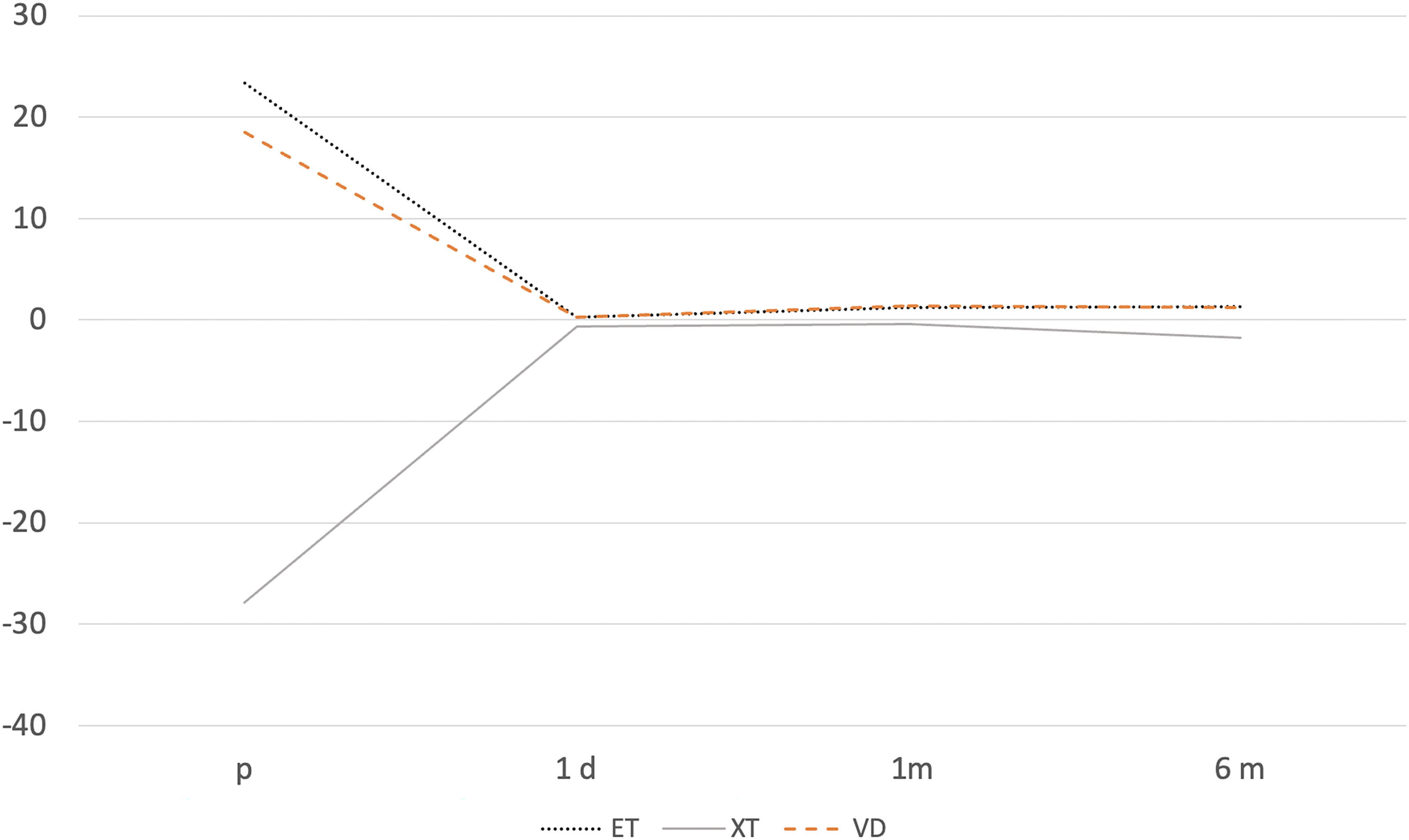
Preoperative and postoperative angles of deviation. ET = esotropia; XT = exotropia; VD = vertical deviation.
Discussion
The same angle of deviation treated with the same amount of surgery may result in different outcomes in different patients. Thus, a mathematical approach to strabismus surgery may be poorly reliable, especially if surgery is performed under GA, which is still the most used for both adults and children. 1
Adjustable sutures have been shown to improve the surgical outcomes, 5 even if only a minority of the studies has provided a statistical support.11–13 The possibility of having a second chance to refine the position of the extraocular muscles is certainly reassuring, but it is not cost effective, as it requires additional time, being overall more expensive. 14 The last report of the American Academy of Ophthalmology highlighted the need for standardization regarding metrics of surgical success, postoperative alignment goals, logistics, timing and number of the adjustments. Finally, in case of intraoperative AS, the position of the patient to perform the APCT is based only on surgeon's preference. 8
With a 6-month success rate near to 90%, the phased approach favorably compared with the results of AS (70–92%) and non-adjustable sutures (27%–82%).2,5,8,15,16 To standardize the technique, we clearly specified the intended alignment goal, in contrast with most AS reports, where the adjustments are made until reaching a satisfactory ocular alignment, or a mild overcorrection to address the risk of long-term ocular drift. 17
The technique enabled to avoid some complications related to AS, like slipped adjustable suture knot, patient's concern and discomfort about the eventual adjustment, and the risk of OCR during adjustment (outside the safety of the OR). Of note, when the adjustment is performed the day after surgery, patient's pain may be more intense due to the accumulation of several inflammatory agents.
We were able to dose the surgery intraoperatively, potentially reducing the number of muscles operated on. As expected, phase 2 was more common in combined vertical and horizontal deviations. The key was the rapid recovery of the patient. Midazolam administered 30 min before the patient's entrance in the OR had the great advantage of being effective at the time of surgery and, with its wash out time of about 1 h, allowed the patient to be fully recovered for the intraoperative evaluation. Moreover, propofol has a synergic effect with midazolam in terms of hypnosis, 18 and did not hinder our intraoperative assessment due to its short half-life and high clearance.
The phased technique was feasible in children, and was effective for cases of reoperation, paralytic strabismus, TAO (we used AS for IR recession in 2 patients with TAO, because of the high rate of overcorrection 19 ), and small to moderate angle of deviation (9 patients in this series had a horizontal deviation ≤20Δ).
When the ocular deviation is small, it may be difficult to decide whether to operate one or more muscles, due to the risk of under or overcorrections, respectively. Two patients of our series were undercorrected 6 months after surgery, despite surgical success was achieved at previous follow-up visits. Recently, Elkamshoushy et al reported a similar technique for deviations ≤25Δ, performing the first step under GA and a 2-muscle-surgery at most. 3 The 6-month success rate was 80%. The authors underlined that their approach was useful for patients with superior oblique palsy, to avoid eventual undercorrection by adding surgery on the contralateral IR. We found that inferior oblique recession procedures were self-grading, being effective to correct vertical deviations from 1 to 40Δ. Of note, superior oblique palsy can be associated with horizontal deviation (5 cases of exotropia and 1 of esotropia in our series), which can improve spontaneously. For this reason, some surgeons suggest postponing horizontal surgery,20,21 but we were able to verify if a concomitant horizontal muscle surgery was necessary, thus avoiding further interventions a few months after the first one.
As secondary outcome, we founded that ocular alignment can be checked intraoperatively both with the patient supine and seated, with the same precision. Most of the studies report an intraoperative APCT with the patient seated, that may appear more feasible, but it requires time to allow the patient to sit safely, especially after an eventual intravenous anesthesia. The supine position may reduce manipulation of the surgical area, with improved sterility, as it is possible to maintain the surgical field intact while performing the APCT. Our results confirmed those obtained by previous authors: 22 Sanz et al performed the APCT using a luminous source for all the measures, except for the supine distance one, for which they asked to look at a cross on the ceiling. As the accommodation influences the deviation (especially in case of exodeviation), we adopted a target for each intraoperative measure, to be consistent.
This study should be considered with its limitations. Topical anesthesia can be related with more patient's discomfort, so it requires a more delicate muscle manipulation compared to general or peribulbar anesthesia. Careful patient selection and proper counseling are important to improve patient's satisfaction. Uncooperative character, mental disorders and retardation, anxious and insecure attitudes in case of pediatric patients may represent exclusion criteria. We did not have a control group, and our follow-up was short, so we were not able to report eventual later drifts. Finally, 13 patients (34%) did not return for the 6-months follow-up visit, introducing potential bias.
Despite these limitations, we suggest that the phased technique is feasible for a wide range of strabismus types, allowing to analyze motor and functional results directly in the OR and offering the option to increase the number of operated muscles in case of undercorrection.
Footnotes
Author contributions
E.F. and F.F. designed the study; F.F. performed the surgery; E.F., S.M. and M.F. collected the data; E.F. generated the figure and the tables; E.F. performed the statistical analysis; E.F., F.F., and E.F. drafted and revised the manuscript; and all approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics
The study was conducted in accordance with the 2013 Declaration of Helsinki and was approved by the local Ethics Committee (CE-AVEC 744/2022/Oss/AOUFe). This study was conduct at the Operational Unit of Ophthalmology, St. Anna University Hospital of Ferrara, Ferrara, Italy.