
Abstract
Purpose
to compare five-year outcomes of two complete intracorneal implants (MyoRing versus annular-shaped intracorneal implant [AICI]) combined with accelerated corneal cross-linking (A-CXL) in progressive KCN.
Methods
In this historical cohort study, preoperative and postoperative visual, refractive, tomographic, biomechanical, and aberrometric parameters of 27 eyes of 27 patients who underwent implantation of two complete rings (13 AICI and 14 MyoRing) combined with A-CXL were recorded.
Results
The mean age of patients in “AICI plus A-CXL” and “MyoRing plus A-CXL” groups were 28.1 ± 4.6 and 26.3 ± 3.8 years, respectively. All pre- and postoperative visual and refractive parameters between the two groups were not significantly different (p > 0.05). Comparing pre- and postoperative tomographic measurements showed that anterior corneal surface (ACS) flat-K and corneal thickness at pachymetric apex significantly improved for MyoRing plus A-CXL group after five years (p < 0.05). On the other hand, ACS K-max and mean-K values were significantly improved for AICI plus A-CXL group after five years (p < 0.05). Both groups revealed significant improvements in ACS steep-K and corneal astigmatism (p < 0.05). Five years after surgery, the high order aberration in the AICI group (2.60 ± 0.83) was significantly better than the MyoRing group (1.70 ± 0.43) (p = 0.007).
Conclusions
Both complete intrastromal rings (MyoRing or AICI) combined with A-CXL significantly Improved visual, refractive, and corneal aberrometric, biomechanical, and tomographic parameters and halt the progression of KCN with comparable long-term outcomes.
Keywords
Introduction
Keratoconus (KCN) is the most common form of corneal ectasia that manifests as a bilateral and asymmetric corneal disease. The severity of KCN determines its visual and structural complications; the more advanced the severity of KCN, the greater its consequences on visual functions and corneal structure. 1 In recent years, several surgical and non-surgical management options have been developed to slow down or halt the progression rate of KCN. However, choosing the best management plan is still a controversial issue. Corneal cross-linking (CXL) is a surgical technique that could control KCN progression. 2 The standard procedure of the original CXL involves ultraviolet-A (UV-A) radiation over the cornea while exposing its surface to vitamin B2 (Riboflavin). 3 This technique reinforces the collagen bindings of the cornea and, accordingly, halts the progression of the disease. 4 The original protocol of CXL is known as the Dresden protocol and requires prolonged irradiation of UV-A over the cornea. 5 With the advent of the accelerated CXL (A-CXL) method, the procedure can be accomplished in a shorter time and with increased intensity of UV-A than conventional CXL protocol. Another treatment modality of KCN are small implantable rings known as the intrastromal corneal ring segment (ICRS). These implants were initially introduced in the form of a complete 360-degree ring to improve mild myopia. Afterward, they were applied for refractive error correction of mild-to-moderate KCN patients. 6 Safety, stability, and reversibility are the main advantages of these corneal implants. 7 Based on the optical design, ICRS implants are classified as complete 360-degree and incomplete or segmental arc-shaped (up to 355 degrees arc length).8,9 The first continuous full-ring ICRS was MyoRing (Dioptex GmbH, Linz, Austria) and introduced in 2007. An advanced type of continuous annular intracorneal implant (labelled as AICI, Ophthalight cor., Tehran, Iran) has also been recently marketed.10,11 This annular-shaped intracorneal implant (AICI) is a one-piece ring with a rectangular cross-section in different thicknesses for vision improvement of KCN in various stages. 12 The designer of this ring (M.J) claimed that this new design has a thinner profile and more desirable curvature than other ICRS, contributing to favorable postsurgical outcomes and fewer complications. 11
Despite the uncertain reports regarding the effectiveness of CXL in improving uncorrected vision in most KCN cases, 3 its combination with other refractive surgery methods could enhance the visual outcomes of the procedure.2,4,13,14 The unique capabilities of ICRS and CXL in vision improvement and slowing down the progression of the KCN resulted in a combined therapeutic approach (CXL plus ICRS) to improve corneal biomechanics and stability. 13 Previous studies reported that the combination of CXL and various types of ICRS implants might be a safe and effective strategy in managing KCN patients.2,15
Numerous published studies compared the clinical outcomes of various types of ICRS (360-degree full rings versus segmental arc-shaped rings) in KCN patients.16–19 However, the ideal design of ICRS for obtaining better outcomes is still a matter of debate. The primary purpose of the current study was to compare the effects of two commercially available complete 360-degree rings combined with A-CXL on visual, refractive, biomechanical, and corneal tomographic and aberrometric aspects in patients treated for their progressive KCN.
Methods
This historical cohort study followed 27 consecutive eyes of 27 KCN patients treated with two different procedures, including a newly launched full-ring implant (AICI) combined with epithelium-on A-CXL and another full-ring implant (MyoRing) plus A-CXL for five years after the operation. All participants were evaluated on a preoperative day and at regular postoperatively years. All surgeries were performed from January 2013 to April 2015 by a single experienced cornea surgeon (M.M) in Farabi Eye Hospital, Tehran, Iran. The patients were followed consecutively for the next five years after the operation. All KCN patients were included in the study provided they had the following characteristics: under 40 years old, KCN stage 2 and 3 (according to Amsler-Krumich staging method), 20 with central and paracentral cone location, progressive KCN during the last two years manifested by the tomographical changes (over 1.00 D increase in steep-K, over 1.00 D increase in cylindrical manifest refraction, and more than 0.50 D change in spherical equivalent manifest refraction), 21 GP lenses intolerance, undesirable best-corrected distance visual acuity (CDVA) using spectacles and GP lenses, average keratometry reading no more than 55 D, thinnest point value over 400 microns, and patients who potentially could carry out the long-term postoperative examinations with annual follow-ups. The patients with a central corneal scar, herpetic keratitis, previous ophthalmic surgery, and any connective tissue disorders were excluded from the study. Patients were scheduled for postoperative evaluations every year up to five years following surgery. Final postoperative findings of different visual, refractive, and corneal tomographic features were compared to their corresponding preoperative values.
The tenets of the declaration of Helsinki were followed during all phases of examinations, and informed consent forms were obtained from all subjects. All examination procedures have been thoroughly explained to the subjects. The ethical board committee of Tehran University of Medical Sciences, Farabi Eye Hospital, Tehran, Iran, has approved the study protocols (IR.TUMS.FARABIH.REC.1397.027).
Annular-shaped intracorneal implant (AICI)
Annular-shaped intracorneal implant (marketed as AICI, Ophthalight cor., Tehran, Iran) is a continuous 360-degree intrastromal ring with a rectangular-shaped cross-section (Figures 1 and 2(a)). 10 This ring is composed of Hexafocon A material, a high oxygen permeable material with an approximate Dk value of 100. The biocompatibility of this material was primarily confirmed in an animal study by Salamatrad et al. 12 After getting approval from the Iran Food and Drug Administration, which is under the supervision of the Iran Ministry of Health and Medical Education, AICI was implanted in human eyes by Jabbarvand et al. 10 Its external diameter, internal diameter, and base curve radius parameters are 6 mm, 4 mm, and 7.4 mm, respectively. AICI is available in four thicknesses, including 140, 160,180, and 200 microns. According to the corneal topography features and refractive status, the manufacturer provides AICI selection criteria (Table 1).
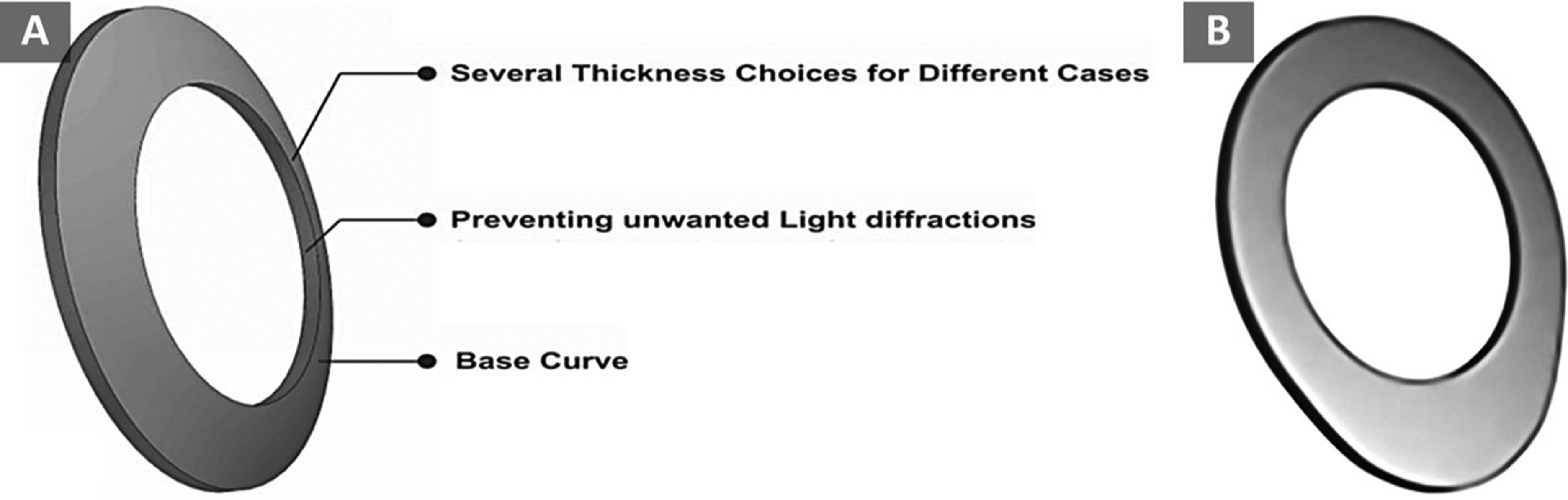
(a) Symmetric Annular Intracorneal Implant (AICI); Schematic view of different specifications. (b) Schematic view of asymmetric AICI.
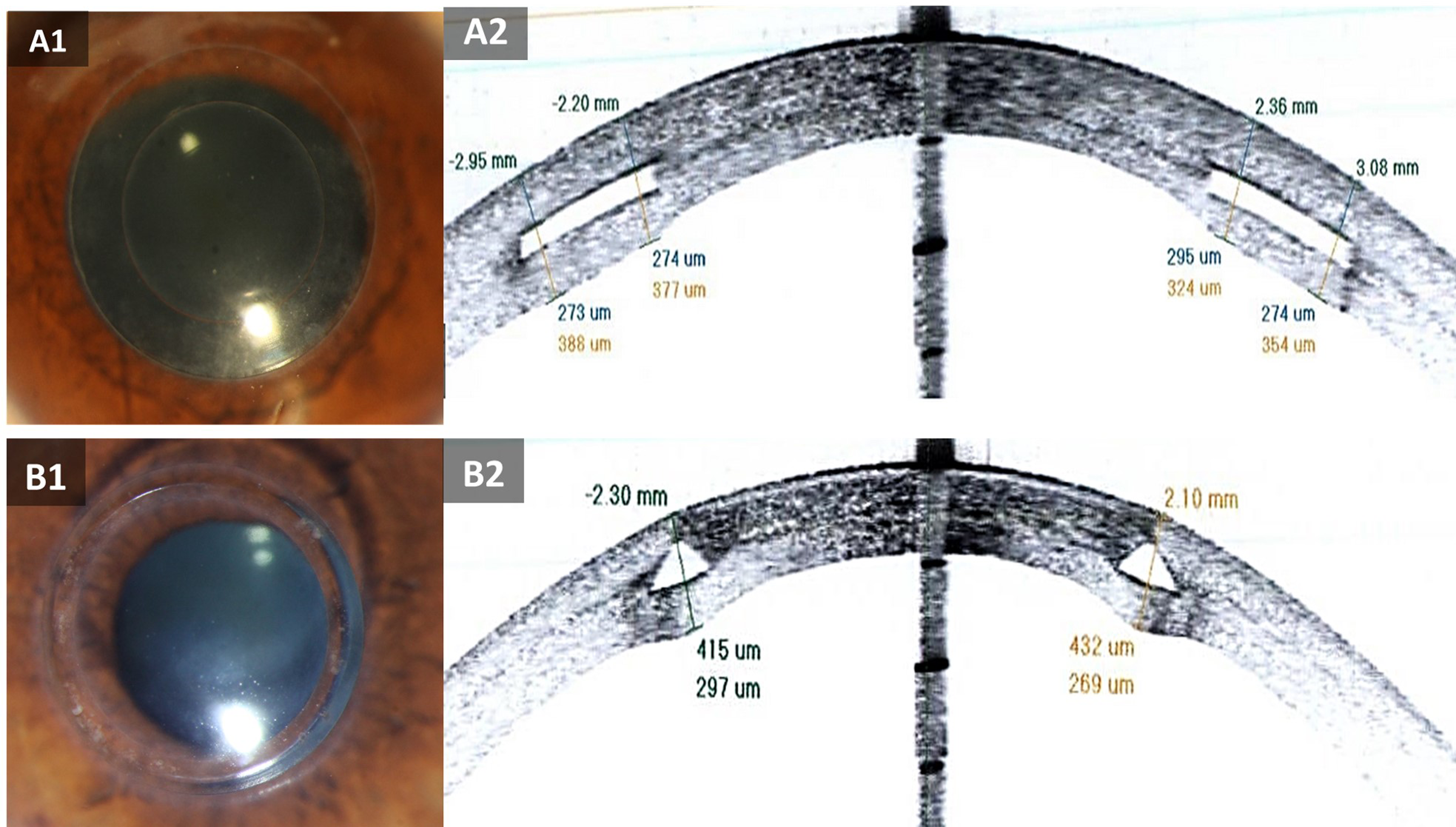
(a) Annular Intracorneal Implant (AICI); (a1) Frontal view of an eye implanted with AICI. (a2) Anterior-segment optical coherence tomography (AS-OCT) view of a cornea implanted with AICI. (b) MyoRing; (b1) Frontal view of an eye implanted with MyoRing. (a2) AS-OCT view of a cornea implanted with MyoRing.
Comparison of visual and refractive parameters of two types of complete intracorneal ring combined with accelerated corneal cross-linking, before and 5 years after surgery.
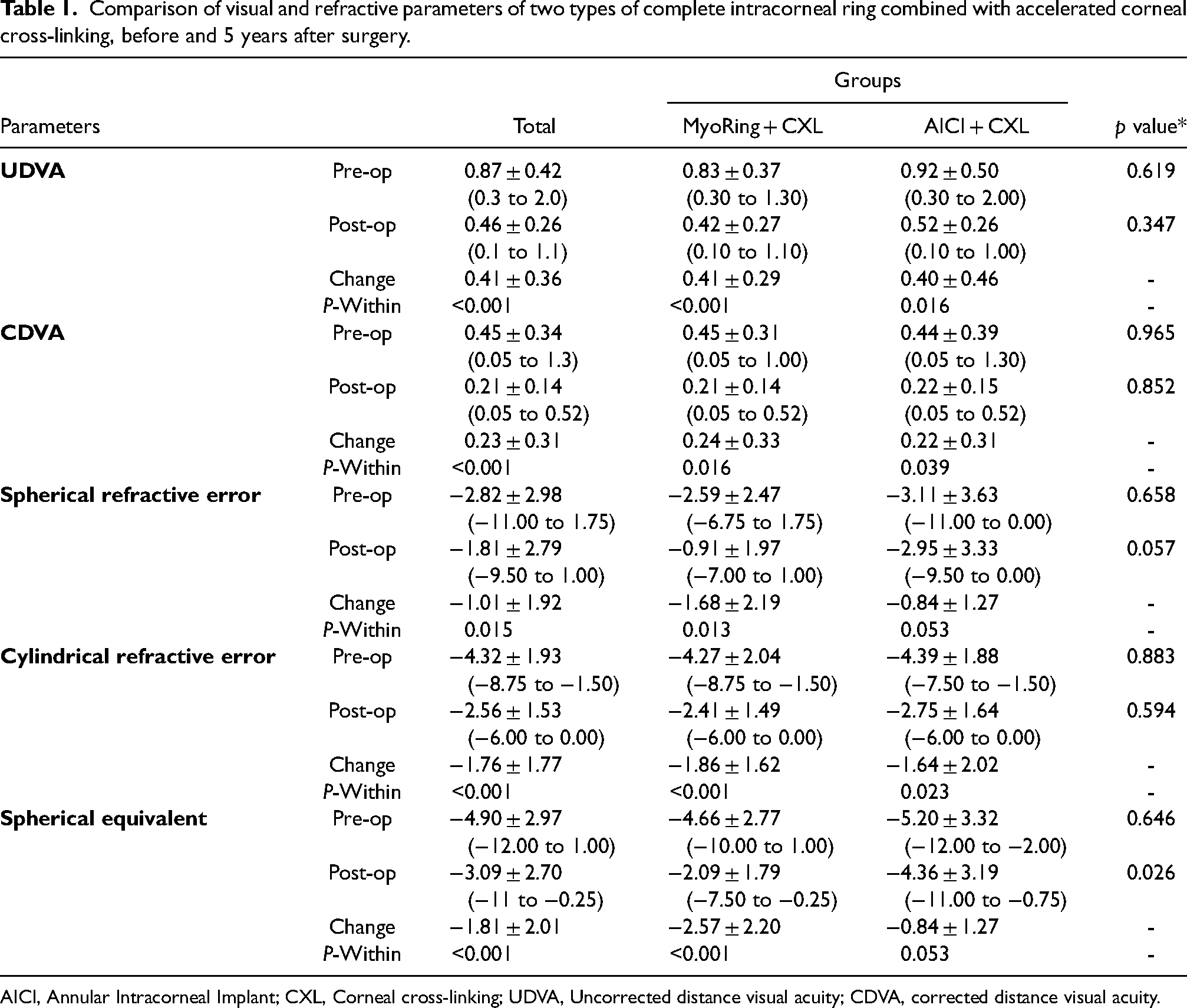
AICI, Annular Intracorneal Implant; CXL, Corneal cross-linking; UDVA, Uncorrected distance visual acuity; CDVA, corrected distance visual acuity.
Myoring
MyoRing is another continuous 360-degree ICRS introduced by Dexar in 2007 (Figure 2(b)
Surgical procedure
Before starting the surgery, the eye was anesthetized with three drops of topical tetracaine 0.5% eye drops. As shown in Supplemental Video 1, the surgery protocol was set based on a novel method introduced by Mohammadpour et al. 23 by which the femtosecond laser-assisted 360-degree ring implantation was combined with epithelium-on A-CXL simultaneously in one session. The first phase of the surgery started by creating a 10 mm intrastromal pocket in the depth of 300 microns around the corneal center that was administered using a 5 mJ powered femtosecond laser machine (Femtec TECHNOLAS Perfect Vision GmbH, Bausch + Lomb, USA). Afterward, dextran-free riboflavin 0.1% was instilled into the stromal pocket. At this level, AICI or MyoRing has been implanted within the stromal pocket. After five minutes, the patient examination has performed by slit lamp to inspect the distribution of the riboflavin into the anterior stroma, posterior stroma, and anterior chamber. Following that, the cornea was exposed to the continuous radiation of 365 nm UVA light (IROC Innocross AG, Bahnhofstrasse, Switzerland) with irradiation of 9 mW/cm2 for 10 min (A-CXL). A bandage contact lens was applied to the corneal surface at the end of the operation. The postoperative therapeutic agent was chloramphenicol 0.5% (Sina Daru, Iran), prescribed every four hours one week after the procedure.
Examination protocol
We recorded the pre- and postoperative data of patients who were followed for five years after AICI plus A-CXL surgery. These data included demographic characteristics, uncorrected and corrected distance visual acuity (UDVA and CDVA) using a standard Snellen chart within a 6-meter distance, spherical and cylindrical subjective refractions, biomechanical parameters using the Corvis ST (Oculus, Inc, Weltzar, corneal aberrometry, and tomography parameters using Pentacam HR (Oculus, Weltzar, Germany). Spherical equivalent (SE) was also calculated as the spherical value plus half of the cylindrical value. All surgeries were performed under anesthesia by an experienced surgeon (M.M) with the same procedure. We instructed all patients not to wear contact lenses before examinations (at least two weeks for softs and four weeks for GPs).
Statistical analysis
Statistical analyses were administered using SPSS 24 (IBM Inc., Chicago, USA). The mean (±SD) and frequency values were reported for every parameter during postoperative follow-up sessions. The normal distribution of all data was first checked by using the Shapiro–Wilk test. In cases of parametric analysis, the paired t-test was administered to compare data of the preoperative and postoperative measurements. An independent sample t-test was used for between-groups comparison. When the parametric analysis was not indicated, the Mann-Whitney U and the Wilcoxon ranked test was executed to compare the values of preoperative and postoperative measurements. p < 0.05 was statistically significant.
Results
This study was performed on 27 eyes of 27 KCN patients. AICI plus A-CXL group included 13 eyes of 13 KCN patients with a mean age of 28.1 ± 4.6 (range 18–37) years, of whom 8 (61.5%) were female, and 5 (38.5%) were male. MyoRing plus A-CXL group included 14 patients [(57.1%) females and 6 males (42.9%)] with the mean age of 26.3 ± 3.8 (range 21–32).
Based on visual, refractive, and tomographic parameters, both groups were matched before surgery (Table 1) (All p > 0.05). The mean amount of UDVA and CDVA, spherical and cylindrical refractive errors, and SE before and five years after surgery in two KCN treated groups are shown in Table 1. As shown, in comparison with baseline preoperative data, all postoperative measurements were significantly improved for both procedures, except for the SE finding of AICI plus A-CXL. Additionally, all postoperative changes between the two methods were not significantly different, except for postoperative SE measurements, in which MyoRing plus A-CXL showed significantly fewer SE measurements (−2.09 ± 1.79) than AICI plus A-CXL (−4.36 ± 3.19). MyoRing plus A-CXL and AICI plus A-CXL caused SE to reduce by −2.57 ± 2.20; p < 0.001, and −0.84 ± 1.27; p = 0.053, respectively.
Comparison of corneal tomographic parameters between two KCN treated groups before and five years after surgery are represented in Table 2. After five years following the procedure, all postoperative measurements were not significantly different between the two studied groups. Comparing pre- and postoperative tomographic measurements showed that anterior segment flat-K and corneal thickness (CT) at the pachymetric apex significantly improved for MyoRing plus A-CXL group after five years (p < 0.05). On the other hand, anterior corneal surface (ACS) K-max and mean-K values were significantly improved for AICI plus A-CXL group after five years (p < 0.05). Both groups revealed significant improvements in ACS steep-K and corneal astigmatism measurements. All posterior corneal topographic measurements showed significant improvements for both methods, except the posterior steep-K value that did not improve significantly for the MyoRing plus A-CXL group. Notably, although the thinnest point (TP) did not improve significantly for both KCN treated groups, mean values of changes in TP values for MyoRing plus A-CXL (8.5 ± 16.1) showed higher improvements than those values for AICI + A-CXL (3.0 ± 14.92). The most noticeable improvements in anterior and posterior corneal parameters for both KCN treated groups occurred in steep-K and flat-K measurements, respectively.
Comparison of topographic parameters of two types of complete intracorneal ring combined with accelerated corneal cross-linking, before and 5 years after surgery.
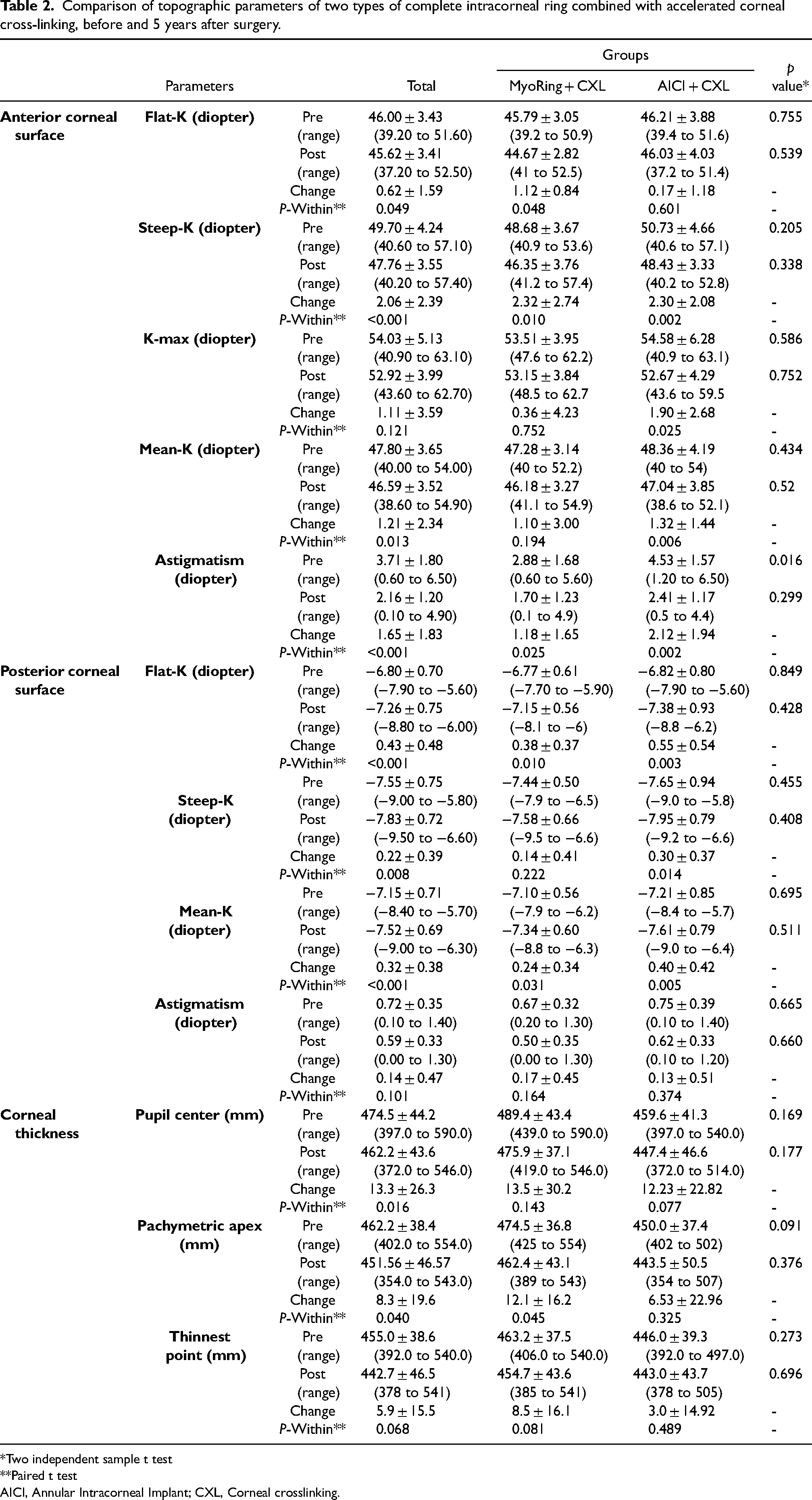
*Two independent sample t test
**Paired t test
AICI, Annular Intracorneal Implant; CXL, Corneal crosslinking.
The postoperative corneal biomechanical and aberrometric indices in both KCN treated groups five years after surgery are reported in Table 3. As shown, there were no significant differences in all obtained corneal biomechanical and aberrometric parameters between two KCN treated groups after five years (p > 0.05).
Comparison of some tomographic, biomechanical and aberrometry index of two types of complete intracorneal ring combined with accelerated corneal cross-linking, 5 years after surgery.
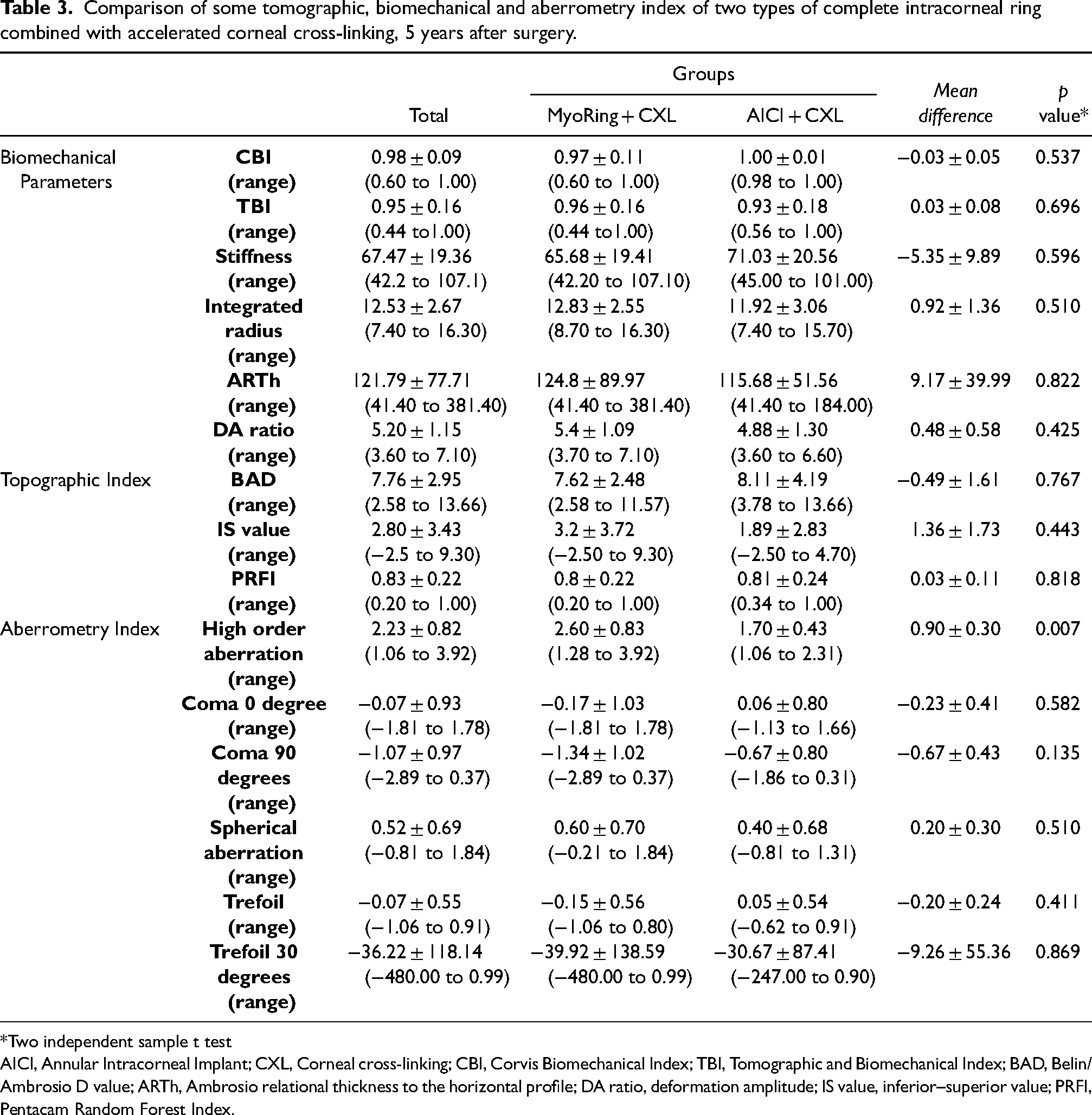
*Two independent sample t test
AICI, Annular Intracorneal Implant; CXL, Corneal cross-linking; CBI, Corvis Biomechanical Index; TBI, Tomographic and Biomechanical Index; BAD, Belin/ Ambrosio D value; ARTh, Ambrosio relational thickness to the horizontal profile; DA ratio, deformation amplitude; IS value, inferior–superior value; PRFI, Pentacam Random Forest Index.
Supplementary Table II represents the visual and tomographic data of a 29-year-old male patient who underwent the AICI plus A-CXL procedure for keratoconus treatment in his right eye. Preoperative (2013) and postoperative (2015 and 2018) findings are compared. As shown in this table, 0.8 logMAR improvement in UDVA of the patient and 3.50 diopter reduction in astigmatism refractive error were observed over the period of five years following surgery.
Figure 3 represents the tomographic maps of a KCN patient before and seven years after MyoRing implantation plus A-CXL. Four refractive maps of a patient with KCN before and eight years after AICI implantation plus A-CXL were also shown in Figure 4. Comparison of preoperative (2013) and postoperative (2015 and 2018) visual, refractive and tomographic findings in a 29-years-old male patient who underwent AICI implantation plus A-CXL for KCN treatment of his right eye was also shown in supplemental table II.
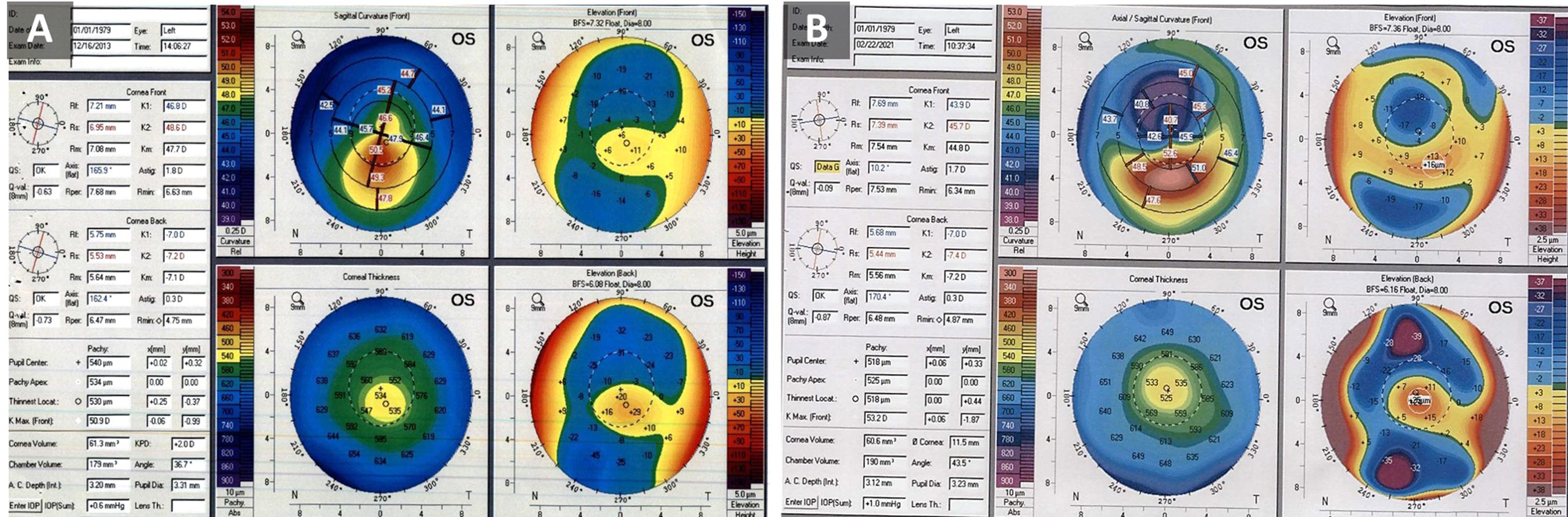
(a) Left eye tomographic maps of a keratoconic patient before MyoRing implantation in 2013 (Pentacam hr, Oculus, Weltzar, Germany). (b) Tomographic finding eight years after MyoRing implantation plus accelerated-corneal cross-linking in 2021.
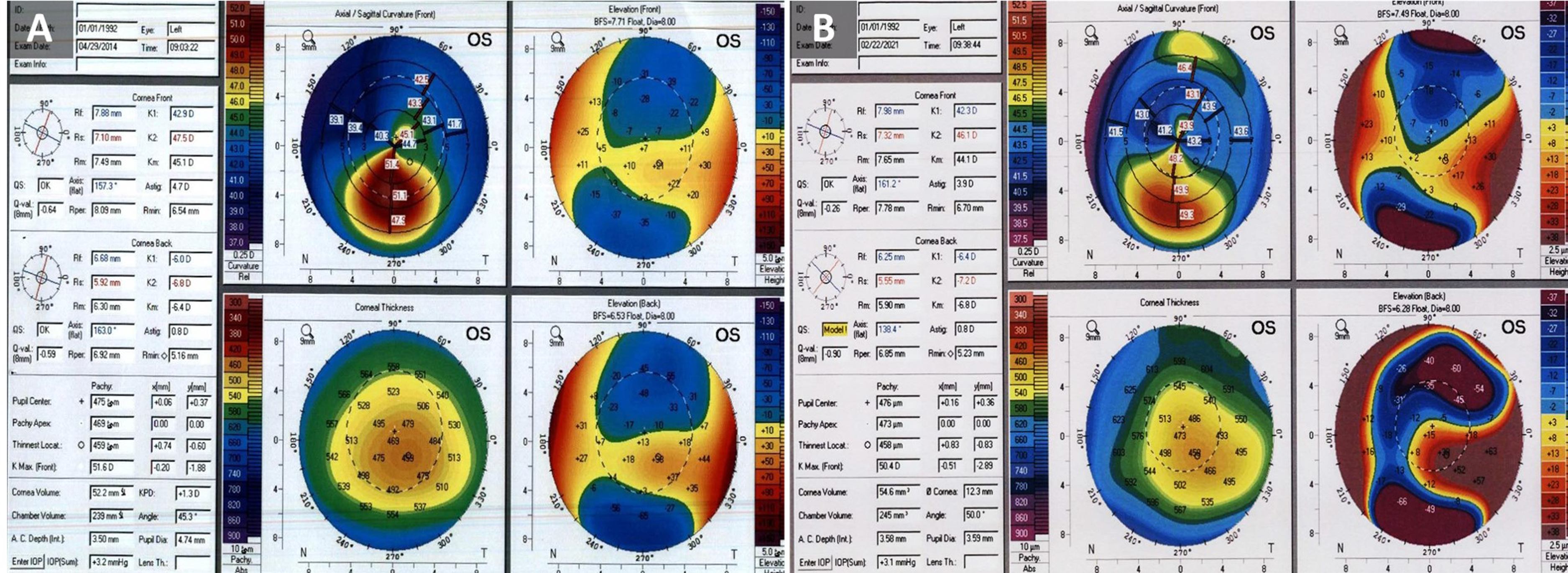
(a) Left eye tomographic maps of a keratoconic patient before Annular Intracorneal Implant (AICI) implantation in 2014 (Pentacam HR, Oculus, Weltzar, Germany). (b) Tomographic finding seven years after AICI implantation plus accelerated-corneal cross-linking in 2021.
Dry eye was the most common postoperative complaint that was managed successfully by lubricants. No clinically remarkable intraoperative and postoperative complication, including epithelial damages, corneal infectious, and ring extrusion was observed in all participants at the end of five-year examinations. All patients had clear cornea with no ICRS extrusion. No case progressed despite treatment in 5 years post-operation.
Discussion
The current study compared five years’ visual, refractive, corneal tomographic, aberrometric, and biomechanical outcomes of two continuous ICRS implants (AICI versus MyoRing) in combination with A-CXL in patients with progressive KCN. To our knowledge, this is the first study that compares long-term postsurgical outcomes of the two commercially available complete rings in combination with A-CXL. We found that the postoperative outcomes of the AICI plus A-CXL and MyoRing plus A-CXL compared to the corresponding preoperative baseline values revealed long-term stability and improvement following both methods in patients with progressive KCN. Despite relatively the same long-term behavior of both methods in KCN patients, outcomes of SE values showed significantly more improvements in patients treated with Myoring plus A-CXL than AICI plus A-CXL. Both methods significantly reduced anterior corneal astigmatism (1.18 D in MyoRing and 2.12 D in AICI group) and steep-K values after five years following the procedure. In addition, the most remarkable change among all corneal tomography data was for the steep-K index. These findings indicate that KCN severity may retard in patients who underwent continuous ring implantation plus A-CXL.
The number of proposed new treatments for KCN is increasing, driven by the demand to avoid keratoplasty. AICI is a novel 360-degree intracorneal implant made of hexafocon A, and with a rectangular profile that could reform the corneal curvature.10,12 In an animal study on rabbits, Salamatrad et al. 12 observed no change in cell density of corneal keratocytes implanted with AICI compared to the control group. In a recently published study, Jabbarvand et al. 1 °conducted the first human study on 34 KCN patients treated with AICI. They investigated visual, refractive, and topographic outcomes one year after ring insertion and concluded that AICI implantation significantly improved visual functions and flattened the anterior surface of the cornea. However, the long-term effects of combined AICI and A-CXL on visual, refractive, and tomographic measurements have not been investigated. In another study, Jabbarvand et al. 11 evaluated the efficacy and safety of AICI implantation by comparing pre- and postsurgical (one year) visual, refractive, aberrometric, and topographic outcomes in 95 KCN patients. They reported improvements in all parameters and the safety and efficacy of 100% (safety index: 1.8) and 45% (efficacy index: 1), respectively. However, the present study compared the long-term outcomes of two continuous ICRS implants with different designs. In agreement with the two studies conducted by Jabbarvand and coworkers, most visual, refractive, and tomographic measurements were improved significantly in KCN patients treated with AICI plus A-CXL.
As per the earlier work of Burris et al., 24 thicker ring implants provide better corneal flattening effect. As Myoring has a thicker profile (200–320 µ) than AICI (140–200 µ), it is expected to perform favorably in KCN patients. However, according to the findings of the present study, both implants combined with A-CXL had almost the same outcomes in regards to visual, refractive, and topographic outcomes. This effect may be due to the differences in other factors such as diameter, profile and cross-section design, and degree of flexibility. 25 From the clinical perspective, these parameters would balance the impact of both implants in the corneal tissue and can induce roughly the same manner in KCN corneas. Considering this compensational effect, as AICI is available in thinner profiles, it may be more suitable in advanced cases of KCN with thin corneas. In addition, comparing aberrometric outcomes of the two ICRS showed that regardless of statistical insignificance, AICI had lower high-order aberration and spherical aberration values than MyoRing, which could be attributed to the difference in cross-section design of the two ICRS (rectangular shape for AICI versus trapezoidal-shape for MyoRing; Figure 2).26,27
The current study showed that combining a complete 360-degree ring and A-CXL is highly effective in flattening the corneal steepness after a long-time period following surgery. In terms of both methods, the most remarkable dioptric change between topographic K values findings of pre- and post-surgery was for the mean value of anterior steep-K, which significantly flattened compared to baseline data (2.32 ± 2.74 for MyoRing plus A-CXL and 2.30 ± 2.08 for AICI plus A-CXL). Anterior astigmatism had also been significantly improved in both KCN treated groups (1.18 ± 1.65 for MyoRing plus A-CXL and 2.12 ± 1.94 for AICI plus A-CXL). Despite the enhancement in every corneal tomography measurement, the pre- and postoperative differences of anterior flat-K and TP for AICI plus A-CXL as well as K-max, anterior Mean-K, and TP for MyoRing plus A-CXL were not statistically significant. However, the stability and improvements in tomographic data clearly showed the practical effectiveness of both procedures in patients who were previously diagnosed as progressive KCN. In line with our results, previous studies found that implantation of other ICRS devices in KCN patients could flatten the cornea in various degrees.8,19,28,29 Vega-Estrada et al. 19 found a significant reduction of mean K-readings six months after ICRS implantation (KeraRing or INTACS). However, five years after the operation, they found a reduction of approximately 1.0 D relative to the average finding of 6-month follow-up, which was not statistically significant. The authors concluded that despite the insignificant regression of 1.0 D, the corneal profile was stable over a period of 5-year follow-up after ICRS surgery. They believed that their data were theoretically sufficient to assume ring implantation as an effective strategy for persistent and long-standing management of KCN patients. Notwithstanding, their methodology was controversial as they used two different segmental ICRS as study groups that were implanted randomly using two different procedures of femtosecond laser-assisted or mechanical technique. The present study used two complete rings in different patients matched by age and severity of KCN before surgery.
Although most previous studies reported short-term effectiveness of segmental ICRS implants on visual and refractive status,14,18,30 some reports found various degrees of visual loss in long-term evaluations of the treated patients with such ring segments. 8 Notably, some studies reported no significant differences in the efficacy of various segmental ICRS implants. 18 In a systematic review and meta-analysis on evaluating the efficacy of a full-ring 360-degree implant (MyoRing) in KCN treatment, Janani et al. 17 found the outperformance of complete ring implantation one year after implantation. In comparing segmented and complete 360-degree ICRS, Saleem studied the efficacy and safety differences between KeraRing and MyoRing combined with CXL. 27 The author found that patients treated with MyoRing plus CXL had less myopia, and patients treated with KeraRing plus CXL had less astigmatic refractions six months after surgery. In accordance with the findings of the current study, improvement of UDVA, CDVA, and refractive errors using a complete 360-degree ICRS has been previously reported.9,31,32 In a short-term study concerning visual acuity, refractive error, and keratometry outcomes of a 360-degree ICRS (MyoRing), Khorrami-Nejad et al. 9 found significant improvement in the outcome measurements six months after the operation. In a retrospective study, Dexar et al. 31 found significant improvements in 5-year outcomes of UDVA, CDVA, K-reading, and refractive components in KCN patients treated with a complete ICRS (MyoRing). They concluded that the treatment could be considered a safe and effective method in treating and stabilizing progressive KCN. In a prospective and interventional study on 25 KCN patients, Hosny et al. 33 compared preoperative values and four weeks postoperative outcomes of a complete with a segmental ICRS (MyoRing versus KeraRing). Similar to the present study, both ICRS implants were inserted using femtosecond laser-assisted procedure. They found that both methods provided the same results for all visual, refractive, and topographic outcomes, except for K-max, which was significantly decreased in the MyoRing group than in the KeraRing group. The authors concluded that both methods could effectively improve visual and corneal parameters of the KCN eyes; however, complete rings may have a higher flattening effect on the anterior corneal curvature. In a recently published cohort study, Mohammadpour et al. 32 found significant changes in long-term postoperative visual, refractive, and corneal topographic data after implanting a 360-degree ICRS (MyoRing). In agreement with the present study, two systematic reviews by Janani et al. 17 and Izquierdo Jr. 16 compared different types of ICRS. They concluded that MyoRing implantation was the most effective method for improving refractive, visual, and corneal curvature. The superior results of complete ICRS implants compared to incomplete ring segments in controlling KCN progression could be explained by two mechanisms: corneal biomechanics and surgeon freedom.22,25,34 The first theory was provided by Daxer et al. 25 in which they assumed that because of the 360-degree design of the complete ring ICRS, it acts as a second limbus. This second artificial limbus supports corneal biomechanical properties and strengthens its circumferences. The second mechanism was also proposed by Dexar et al. 22 They hypothesized that full ring implants provide three degrees of freedom for the surgeon during ICRS implantation. These degrees of freedom included implant thickness, diameter, and position. Segmental ICRS implants provide ring thickness as the sole degree of freedom. 22 Even mild misalignments of a segmented ICRS might dramatically reduce postoperative visual functions. 34 In line with the studies on MyoRing as a complete 360-degree ring, we assumed that the visual and topographical improvement in KCN patients treated with AICI could also be ascribed to the biomechanical balance formation and subsequent relatively equal forces distribution within the cornea. 17
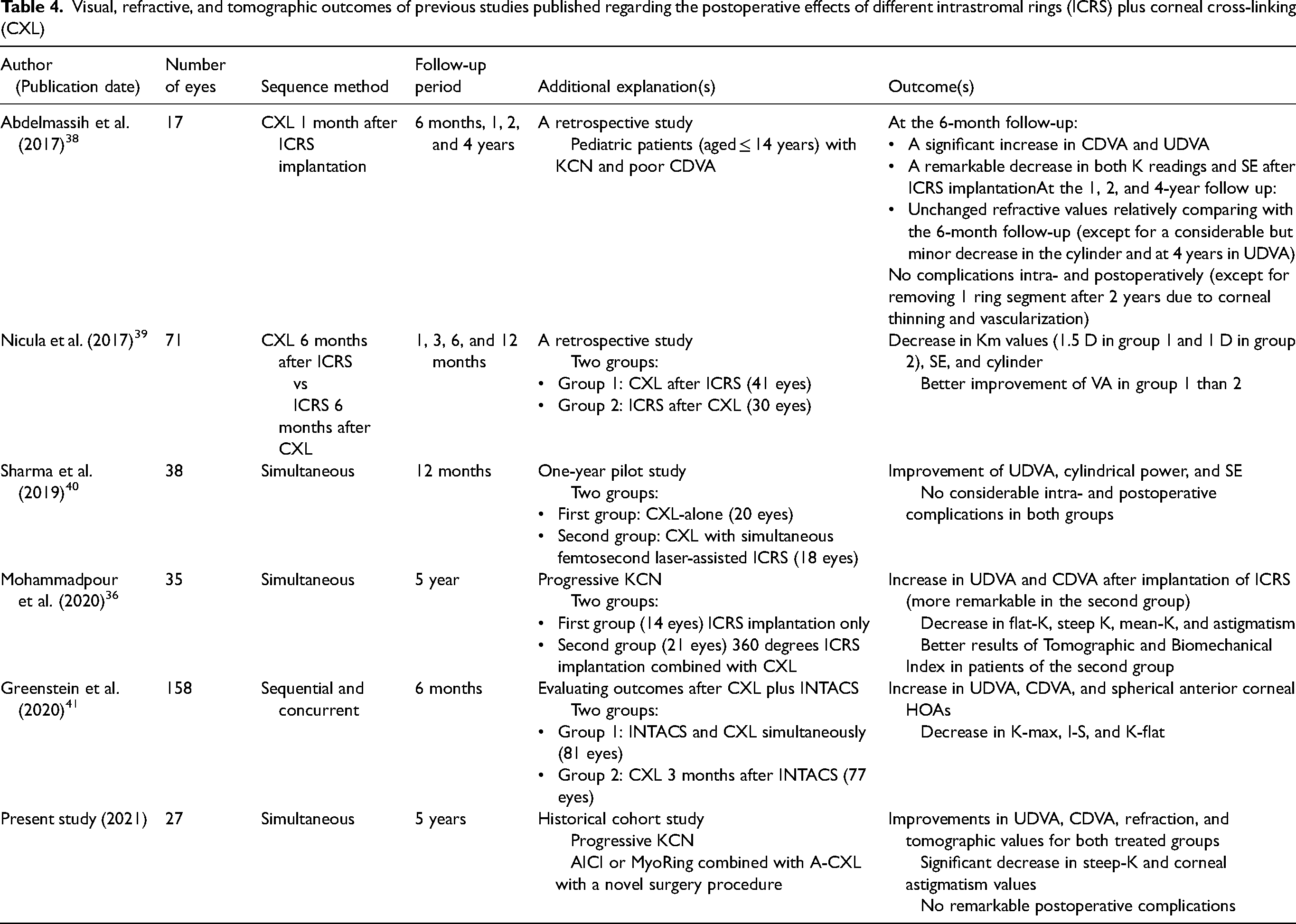
Previous studies showed that CXL combined with ICRS (CXL plus), could be considered more effective compared to each procedure separately.2,4,14,32 Several studies focused on the treatment order to find which of the following management plan sequences could be more effective: ICRS before CXL on different surgery sessions, ICRS after CXL on different surgery sessions, and simultaneous ICRS and CXL in one session.4,15 In a prospective comparative study, Coskunseven et al. 15 found that performing ICRS (KeraRing) before CXL provided superior results comparing CXL before ICRS. Two surgeries were performed with a mean interval of 7 months, and then the patients were followed after an average time of 13 months. They proposed that the patients treated with CXL as their initial procedure may have a stiffer cornea than those treated with CXL as the second intervention. This occurrence could limit the effectiveness of the following ICRS implantation. In contrast, Henriquez et al. 35 found that performing CXL followed by ICRS (Ferrara) could slow down the progression rate of KCN. Legare et al. 2 reported no difference in KCN progression in combined ICRS (INTACS) and CXL versus CXL alone. They hypothesized that the corneal biomechanical aftereffects of the CXL technique could minimize ICRS effectiveness. Simultaneous ICRS plus CXL may lead to more considerable improvements because of the accumulation of vitamin B2 (riboflavin) on the corneal pockets that have been created just before ICRS implantation. 36 This occasion could enhance the flattening effects of CXL over the exposed cornea and therefore provides improvements in postoperative keratometric and refractive findings.4,14 In a systematic review and meta-analysis study on procedure sequence in combined ICRS and CXL, Hashemi et al. 4 reported that although combined ICRS and CXL could result in significant improvements in postoperative visual, refractive, and keratometry outcomes; however, concurrently performed ICRS and CXL had superior results of keratometric findings than staged order. Gouvea et al. 37 reported that despite the more excellent effects of combined ICRS and CXL than sole treatment strategies, both methods of standalone ICRS implantation and combined ICRS and CXL in every form of simultaneous or sequential, are preferably successful in treating KCN patients who could not tolerate contact lenses. Table 4 demonstrates several recently published studies on combined ICRS and CXL. We set the surgery plan as performing concurrent AICI or MyoRing plus A-CXL on the same day.
Visual, refractive, and tomographic outcomes of previous studies published regarding the postoperative effects of different intrastromal rings (ICRS) plus corneal cross-linking (CXL)
We observed no evidence of late sight-threatening complications in our series of both study groups five years following the procedure. This favorable outcome could be assigned to the design and position of 360-degree rings located at the corneal pocket instead of closed channels. This placement method is sutureless and could produce a balanced pressure over the corneal tissue.11,42
Intraoperative stromal pockets could be created using a mechanical or femtosecond laser-assisted procedure. Most studies published before 2010 utilized the mechanical approach as a pocket creation procedure. 43 These studies reported that pocket creation using manual technique might have intra- and postoperative complications such as corneal epithelial damage, corneal perforation, and ICRS dislocations. 43 In an early study conducted by Carrasquillo et al., 44 the authors compared the effectiveness of femtosecond laser-assisted and mechanical procedures on postoperative outcomes 10.3 months after ICRS (INTACS) implantation. They reported that both methods were safe and had similar effects on postoperative outcomes. The following year, Coskunseven et al. 28 and Ertan et al. 29 reported the same conclusions regarding the safety and effectiveness of femtosecond laser-assisted pocket creation in KCN patients. Studies conducted in subsequent years also proved the femtosecond laser as a safe procedure that could improve the postsurgical outcomes due to its high precision in creating stromal channels. 45 In the current study, we utilized a femtosecond laser-assisted procedure to create the stromal pocket for AICI or MyoRing placement. Although minor complications of femtosecond laser-assisted ICRS have been previously reported, the incidence rate of sigh-threatening complications is relatively insignificant. 45
Despite the encouraging results, the main limitations of the present study were the small sample size in either study group and the lack of follow-up between preop and last visit. Accordingly, we could not categorize patients based on their KCN stage. However, improved outcomes values were statistically significant in most statistical analyses. Another limitation was that we did not include other study groups comprised of KCN patients implanted with incomplete ring segments combined with CXL or patients who were operated with only the CXL procedure. To overcome these limitations, further clinical trials with larger sample sizes and more study groups are required.
In conclusion, we found that femtosecond laser-assisted implantation of the complete 360-degree intrastromal ring combined with A-CXL is a safe and effective method in treating corneal ectasia and halting the KCN progression for a long-time period. In addition, we found no significant differences in most visual, refractive, and corneal tomographic, aberrometric, and biomechanical outcomes of two study groups treated with two complete rings (MyoRing versus AICI) combined with A-CXL after five years’ follow-up.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231171420 - Supplemental material for Comparison of two different 360-degree intrastromal corneal rings combined with simultaneous accelerated-corneal cross-linking
Supplemental material, sj-docx-1-ejo-10.1177_11206721231171420 for Comparison of two different 360-degree intrastromal corneal rings combined with simultaneous accelerated-corneal cross-linking by Mehrdad Mohammadpour, Mohsen Heirani, Narges Khoshtinat and Masoud Khorrami-Nejad in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721231171420 - Supplemental material for Comparison of two different 360-degree intrastromal corneal rings combined with simultaneous accelerated-corneal cross-linking
Supplemental material, sj-docx-2-ejo-10.1177_11206721231171420 for Comparison of two different 360-degree intrastromal corneal rings combined with simultaneous accelerated-corneal cross-linking by Mehrdad Mohammadpour, Mohsen Heirani, Narges Khoshtinat and Masoud Khorrami-Nejad in European Journal of Ophthalmology
Footnotes
Acknowledgements
The authors would like to express their special thanks to professor Renato Ambrósio for his excellent suggestions and comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.