
Abstract
Purpose
The aim of this study was to investigate the influence of artificial tears containing either cationic nanoemulsion (CCN) or sodium hyaluronate artificial tears (SH) on early postoperative healing after modern surface refractive surgery.
Materials and Methods
In this multicenter, prospective, double-masked, parallel-group (1:1), comparative study, 129 patients (n = 255 eyes) were randomized to receive CCN (n = 128) or SH (n = 127) as an adjuvant treatment after either transepithelial photorefractive keratectomy (transPRK) or Epi-Bowman keratectomy (EBK). The patients’ perspectives were gathered using the Ocular Surface Disease Index (OSDI) questionnaire, and uncorrected (UCVA), and corrected (BCVA) visual acuity were assessed before and one week and one month after the procedure. In addition, corneal epithelization and subjective assessment of visual blur and eye irritation on drop instillation were assessed at one week postoperatively.
Results
No statistically significant differences were found between two groups in age, spherical equivalent refractive error, UCVA, BCVA or OSDI scores before the procedure. There was also no difference between groups in UCVA one week and one month after the procedure. However, statistically significantly lower OSDI scores were found one week and one month after the procedure in the CCN group. Moreover, blurred vision after use of the eye drops was observed less frequently in the CCN group than in the SH group.
Conclusions
The CCN and SH groups had similar postoperative UCVA. However the significantly lower OSDI scores and less frequently blurred vision after application of the eye drops in the CCN group suggest better subjective outcomes in this group.
Keywords
Introduction
Surface keratorefractive surgery with the use of excimer laser was introduced more than 30 years ago, and remains widely used. 1 Studies have demonstrated the efficacy and safety of different kinds of surface refractive surgery including photorefractive keratectomy (PRK), laser-assisted subepithelial keratectomy (LASEK), transepithelial photorefractive keratectomy (transPRK) or EpiBowman blunt keratectomy (EBK).2–5 Modern surface ablation techniques such as transPRK and EBK are associated with rapid healing and visual recovery and are often preferred over LASIK in cases of thin cornea due to their lower risk of corneal ectasia. 6 In the transPRK technique, excimer laser devices are used to ablate the epithelium and then perform refractive ablation of the underlying stroma. 7 During the EBK procedure, mechanical epithelial delamination is performed using an Epi-Clear epikeratome, a single-use blunt device.
Unfortunately, every type of refractive surgery decreases goblet cell populations, damages corneal nerves resulting in loss of corneal sensation, and induces ocular surface inflammation.8,9 This leads to reduced tear secretion, blinking and ocular surface moisture. 10 These changes contribute to the development of dry eye syndrome (DES), the occurrence of which is estimated at approximately 30% among patients after the LASIK procedure and 8.9%–34.8% after PRK.11,12 Moreover, various studies have shown that preexisting DES may lead to severe post-operative DES.13–17
There is no gold standard treatment for this condition. First-line non-invasive treatment usually includes topical application of artificial tears (AT), which hydrate and lubricate the corneal surface. The most common AT contain 0.15% sodium hyaluronate (SH). Numerous studies have demonstrated their efficacy indicating properties of water retention, enhancement of corneal wound healing, and viscoelasticity. 18 In addition to the standard AT, autologous serum eye drops are effective in postoperative DES treatment. 19 A recently developed preservative free AT known as Cationorm® contains cationic nanoemulsion with nonpolar and polar lipids (i.e., a surfactant) has been found to stabilize the impaired lipid layer of the tear film.20,21 Previous studies have shown its safety and efficiency in DES treatment.22,23 Postoperative DES is considered a ubiquitous issue which impedes the healing process and reduces patients’ satisfaction. Due to the lack of clear guidelines for AT selection, it is challenging to find the best option which not only relieves symptoms for patients with postoperative DES but also supports the postoperative healing process.
This study is the first attempt to compare the efficacy of AT containing cationic nanoemulsion (CCN) with those containing SH in the management of DES and in promoting the corneal healing process after modern surface keratorefractive surgery.
Patients and methods
This is a two-center, prospective, randomized, double-masked, parallel-group (1:1), comparative study
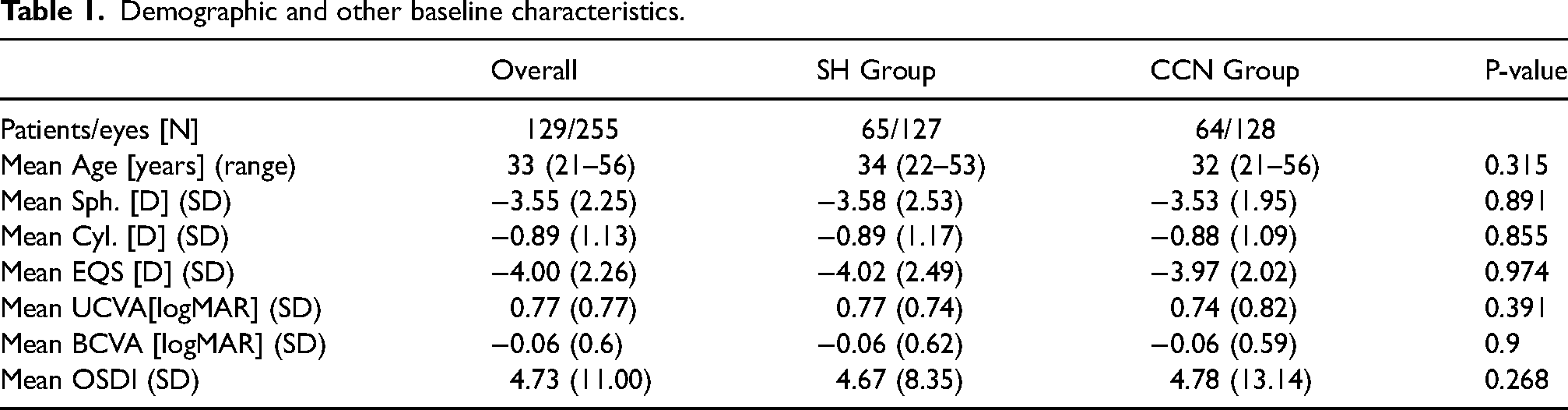
Demographic and other baseline characteristics.
Inclusion criteria were: myopia, myopic astigmatism, age > 21 years, stable refractive error for more than 2 years, and approval to undergo corneal excimer laser refractive surgery. Exclusion criteria were as follows: hyperopia, ocular trauma or previous intraocular surgery, active inflammatory eye disease, monocular best corrected visual acuity (BCVA) poorer than 0.3logMAR before surgery, and significant ophthalmic pathology other than mild DES.
Preoperative examination
Medical history and medication use was obtained from each patient preoperatively. All patients underwent standard ocular examination before the procedure including manifest refraction, uncorrected visual acuity (UCVA) and BCVA, slit-lamp examination, measurement of intraocular pressure (IOP), fundus examination after pupil dilation, and assessment of DES severity using the Ocular Surface Disease Index questionnaire (OSDI). 25 They were then randomly assigned to the CCN or SH group.
Postoperative regimen
All eyes underwent uneventful transepithelial photorefractive keratectomy (transPRK) or Epi-Bowman keratectomy (EBK) with use of the excimer laser Amaris 750 or MEL 80. After sequential binocular surgery, a bandage contact lens was applied (Acuvue Oasis, Johnson &Johnson, USA) for 7 days. The postoperative regimen included 0.3% tobramycin drops twice daily, 0.1%, diclofenac drops and dexamethasone drops once per day for the first week in addition to masked AT every two hours. In the second week dexamethasone drops were applied three times per day, diclofenac drops once per day and masked AT five times per day. During the third and fourth weeks 0.1% fluorometholone and 0.3% tobramycin were applied twice per day and masked AT five times per day.
Postoperative examinations
Postoperative examinations were scheduled at one day, one week and one month after surgery. Every examination included manifest refraction, BCVA, UCVA, slit-lamp examination, measurement of IOP and completion of the OSDI questionnaire. In addition, at the week one examination, the completeness of corneal epithelization was assessed during slit-lamp examination and described as “large”, when it covered >2 mm2, “small” when it covered up to 1 mm2, and “none” in cases with completed epithelization. A subjective questionnaire on blurred vision and eye irritation after eye drop application was also completed during the one week examination. All procedures performed in this study involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. A signed declaration of informed consent to participate in this study was collected from all included patients.
Statistical analysis
The summary statistics are presented as mean ± standard deviation (SD) or as a median and range. The Shapiro‒Wilk test was used to test the normality of data distribution. Differences between continuous variables were analyzed using the Wilcoxon test for demographic data and by the clustered Wilcoxon rank sum test for ocular data. Differences between categorical variables were tested using the chi-square or Fisher exact test for independence. The results were considered statistically significant at p-value < 0.05. The statistical analysis was performed using R-software version 3.6.2.
Results
No statistically significant differences were found between the CCN and SH groups in preoperative UCVA (p = 0.391), BCVA (p = 0.9), OSDI score (p = 0.268), EQS (0.974), or age (p = 0.315) (Table 1).
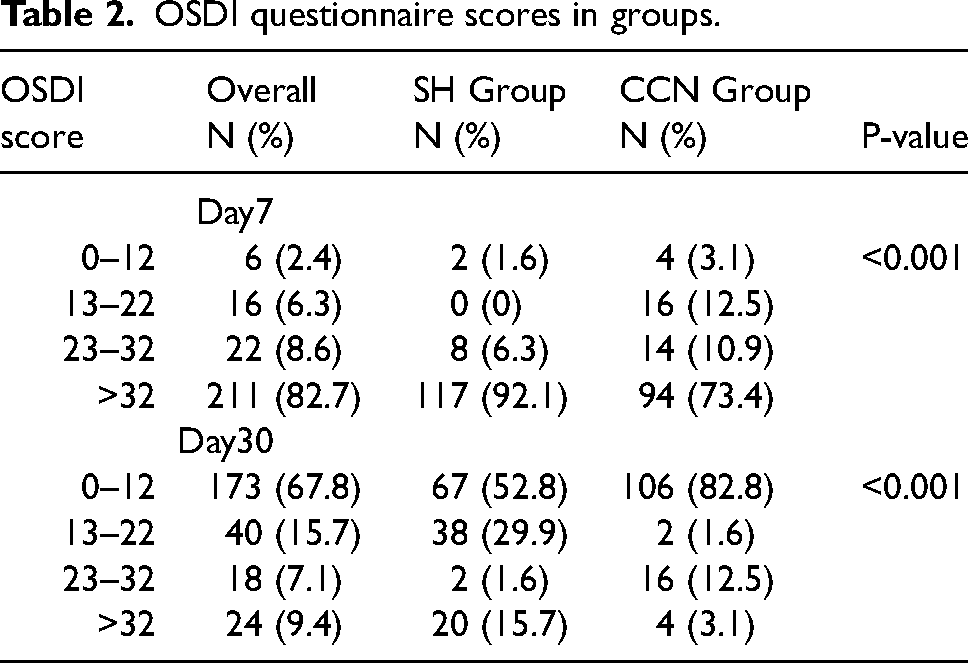
At 7days after the procedure the prevalence of severe DES (OSDI >32) in SH and CCN groups was 92.1% and 73.4%, respectively (p < 0.001). At 30 days after the procedure, the overall prevalence of severe DES was 9.4%, while in SH and CCN groups it was at 15.7% and 3.1%, respectively (p < 0.001; Table 2).
OSDI questionnaire scores in groups.
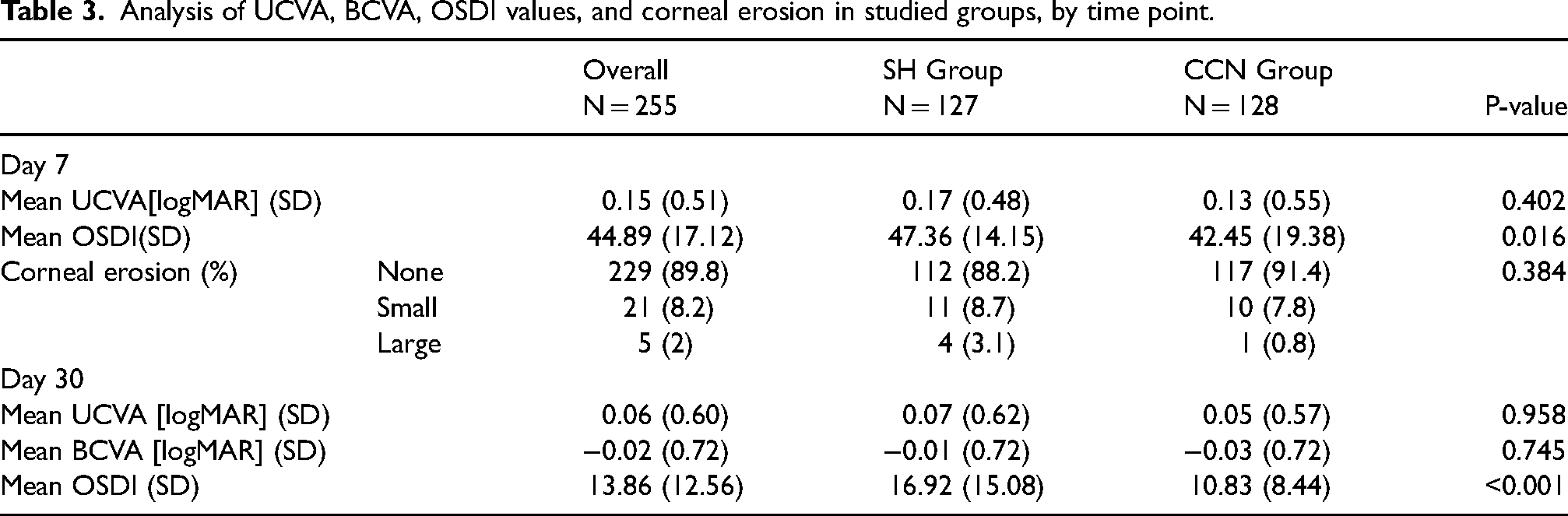
No significant difference between the two groups was found in UCVA, BCVA or completeness of corneal epithelization at 7 and 30 days after surface refractive surgery (Table 3). However, significantly lower OSDI questionnaire scores were found at 7 (p = 0.016) and 30 days (p < 0.001) after the procedure in the CCN group than the SH group (Figure 1, Table 3)
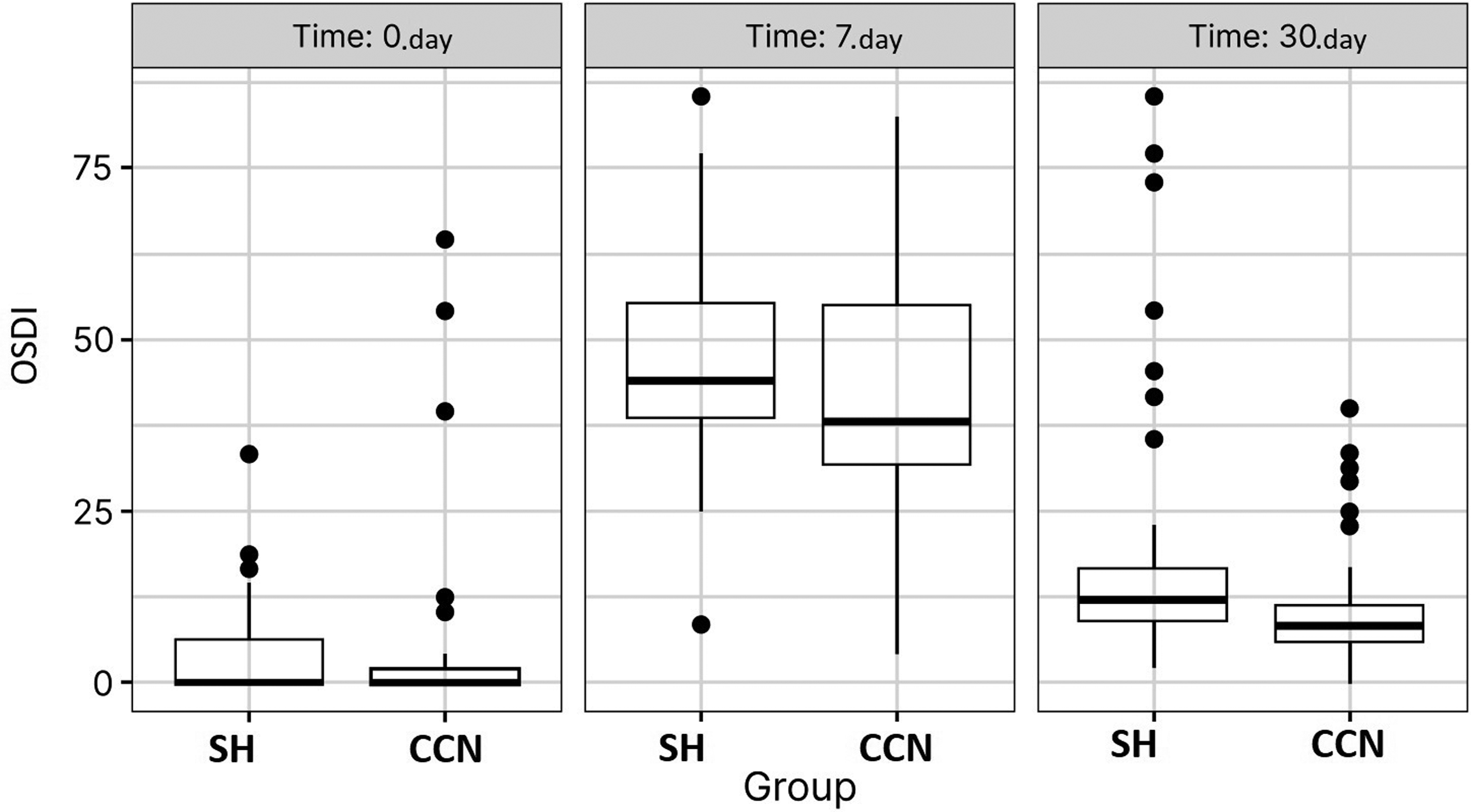
Boxplots showing OSDI scores in both groups before, one week and a month after the procedure (p = 0.016 on the 7th day; p < 0.001 at 30th day by the Wilcoxon test).
Analysis of UCVA, BCVA, OSDI values, and corneal erosion in studied groups, by time point.
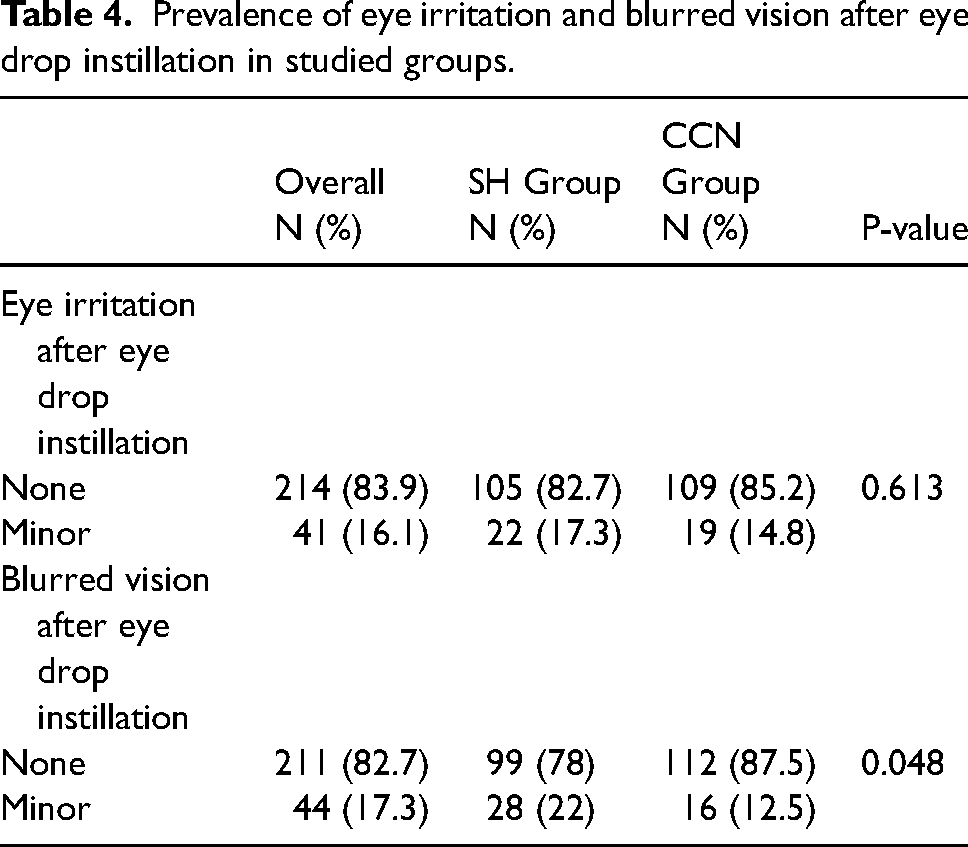
While no significant differences in eye irritation were found between the groups, the occurrence of blurred vision after eye drop instillation was significantly lower in the CCN group than the SH group (p = 0.048) (Table 4).
Prevalence of eye irritation and blurred vision after eye drop instillation in studied groups.
Discussion
Patients may experience DES soon after keratorefractive surgery, and this can persist for some time postoperatively. DES is a complex disease of the ocular surface and tears resulting in discomfort, impaired vision and potential damage to the cornea, accompanied by inflammation. 26 It is characterized by reduced tear production and increased evaporation of the tear film. 27 Efforts to understand the mechanism underlying DES have contributed to development of new AT. Novel types of AT, including CCN are designed to address the above issues and to relieve patients’ symptoms. CCN contains preservative-free cationic nanoemulsion, which is composed of cetalkonium chloride, poloxamer 188, glycerol trishydrochloride, and tyloxapol. It also includes Novasorb, an aqueous emulsion which is produced by cationic nanoemulsion technology and contains positively-charged lipid nanodroplets which cause attraction to the negatively-charged ocular surface20,28 and are responsible for its sustained presence on the ocular surface with prolonged relief of symptoms. The primary aim of the present study was to compare the effect of AT containing cationic nanoemulsion with well-established lubricant 0.15% hyaluronic sodium drops in terms of DES symptoms and ocular surface healing after keratorefractive surgery. Previous studies have shown the negative impact of keratorefractive surgeon neural feedback due to damaged sensory corneal nerves resulting in reduced tear secretion, blinking rate and therefore DES, and impeded healing.29–32 A study by Nejima et al. revealed decreased epithelial barrier function, reduced tear film stability, and lower tear secretion in patients’ eyes after PRK and LASIK. 33 Prevalence of postkeratorefractive surgery DES varies from 8.9% to 34.8%, depending on the surgical approach,11,12 patients’ age, gender, and preoperative contact lens wear. 32 Establishment of an effective treatment for post-keratorefractive surgery DES is crucial, due in part to a high proportion of patients with a history of contact lens wear (44.9% according to a study by Li et al.) who are predisposed to this condition. 34 In addition, the high postoperative DES prevalence, its impact on the healing process, and a lack of accurate predictive tests illustrate the need to develop an effective DES treatment strategy and to find the optimal AT to form an integral part of the postoperative regimen. Previous studies have demonstrated the efficacy of a range of commercially available ATs containing hyaluronic acid, methylcellulose, hydroxyethylcellulose, carboxymethylcellulose, polyethylene glycol, propylene glycol, glycerine or polysorbate.35,36
A recent meta-analysis on AT efficacy found that preserved and preservative-free forms were statistically similar. 37 Preservative-free ATs were used in the present study. Clinical benefits of these include faster DES symptom improvement, while side effects caused by preserved ATs are well documented.38–40 Preservative-free drops are relatively well tolerated in glaucoma treatment 39 while immediate deleterious effects of preserved latanoprost (with 0.02% benzalkonium chloride) on the corneal epithelium have been reported. 41
Another meta-analysis including studies which compared 0.1% to 0.4% preparations of SH-based ATs was not able to distinguish between these due to heterogeneity between studies. 42 In clinical practice higher concentrations of SH are used in more severe DES. In the present comparative study we used 0.15% SH as the comparator due to its demonstrated effectiveness and safety at this concentration.43–45
González-García et al. revealed an increase in pro-inflammatory molecules such as IL-4, IL-5, IL-6, IL-13, IL-17A, and IFN-γ in tears during the weeks following surface corneal refractive surgery.
46
While ATs are effective in the relief of DES symptoms, most of them do not reduce inflammation.
47
Topical corticosteroids may be prescribed post-operatively for rapid anti-inflammatory effects, but their use is not free of adverse effects such as glaucoma or drug-induced cataract.
48
One type of AT, containing cationic emulsion of cetalkonium chloride has been found to have anti-inflammatory effects due to inhibition of IL-6, IL-8 IL-17, TNF
The results of the present and above-mentioned previous studies suggest that CCN maybe beneficial compared with the standard postoperative SH treatment of DES, with improvements in the subjective parameters of DES due to its anti-inflammatory effect. Moreover, previous studies have shown preservative-free CCN to be safe for ocular surface application and efficient in the treatment of DES.22,51–53 In addition, CCN has been described as effective in the treatment of both DES signs and symptoms as well as the new type of delivery vehicle of topically applied lipophilic drugs such as latanoprost.20,54
The advantage of the present study is its two-center, randomized, double-masked design. However, it has some limitations. While the postoperative corneal healing period after surface keratorefractive surgery is up to 12 months, follow up in this study was for one month. We focused on the initial and most important part of the healing process, during which treatment compliance is good and changes in subjectively measured parameters such as symptoms are clear. Other limitations are the lack of objective assessment of DES severity, and the use of two similar but different surgical techniques and only one reference comparator.
Conclusion
In conclusion, the results of this study revealed significant improvement in postoperative visual acuity, and DES symptoms during the first postoperative month in both groups. In the CCN group, we observed relatively rapid improvement in DES symptoms measured subjectively and less blurred vision immediately after AT instillation, while objective results were similar in both groups. Therefore, our findings suggest benefits of CCN over 0.15% SH in the treatment of post-keratorefractive DES and the wound healing process, including an advantage in patient reported symptoms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The professional editing of the paper and open access fee was supported by Santen EMEA Research Grant.