
Abstract
Background
Glaucoma is a leading cause of blindness worldwide for which trabeculectomy is the most effective surgical intervention for advanced disease. However, trabeculectomy has been associated with alterations to corneal endothelium, including a decrease in corneal endothelial cell density (CECD). The purpose of this study was to investigate changes in CECD after trabeculectomy, and identify factors contributing to cell loss, such as pre-operative biometry and lens status.
Methods
This retrospective study included 72 eyes of 60 patients who underwent trabeculectomy between January 2018 and June 2021 at two private hospitals. Demographic and clinical data were obtained at baseline. Corneal specular microscopy was performed pre-operatively and at 6 months after surgery. CECD was evaluated and compared between groups to quantify changes to corneal endothelium and identify significant factors affecting decreases in cell density.
Results
Mean CECD was 2284.66 ± 375.59 pre-operatively and 2129.52 ± 401.96 after 6 months (p < 0.001). A greater decrease in CECD (p = 0.005) was observed in phakic eyes (235.45 ± 118.32) compared to pseudophakic eyes (137.82 ± 107.30). The amount of cell loss was negatively correlated with pre-operative central corneal thickness (p = 0.009) and anterior chamber (AC) depth (p = 0.033). There were no significant correlations between changes to CECD and patient age, gender, number of pre-operative glaucoma medications and number of post-operative antifibrotic agents.
Conclusions
Significant decreases in CECD occurred after trabeculectomy. Less corneal endothelial cell loss occurred in pseudophakic eyes. Hence, if patients need trabeculectomy and cataract surgery, it may be better to perform cataract surgery first. Longer term studies should derive more information.
Introduction
Glaucoma is a chronic and progressive disease characterised by the loss of retinal ganglion cells, which constitute the fibres of the optic nerve. 1 It is one of the leading causes of blindness worldwide, with the number of people affected projected to increase with population ageing. 2 In its early stages, open angle glaucoma primarily impacts peripheral vision, however advanced disease results in severe visual field loss and a decline in visual acuity. 3
One of the key risk factors for open angle glaucoma is raised intraocular pressure (IOP). 1 Reducing IOP is the only proven treatment shown to slow disease progression and decrease the risk of further visual field loss. 4 While the initial approach to lowering IOP is therapy with topical antiglaucoma drops, adequate reductions in IOP are not always achievable despite maximally tolerable medical therapy. In these circumstances, selective laser trabeculoplasty and various minimally invasive glaucoma surgery (MIGS) procedures can be used. When IOP reductions remain inadequate, glaucoma filtering surgery may be indicated, the most effective procedure for advanced glaucoma being trabeculectomy. 5
Trabeculectomy is the standard operation performed for open angle glaucoma, with evidence to support greater reductions in IOP compared with primary medical therapy. 3 Over the last 50 years, significant advances have been made in the field of glaucoma surgery to optimise safety and visual outcomes, however complications can occur. 6 As with any surgery involving the anterior segment, trabeculectomy has the potential to cause corneal injury and is associated with an accelerated decline in corneal endothelial cell density (CECD).7–9
In current literature, several studies have described significant changes in CECD after trabeculectomy.4,5,9 However, there are limited data on risk factors for corneal endothelial cell loss and the mechanisms responsible for these changes are not well understood.4,10
The purpose of this study was to investigate the changes in the corneal endothelium after trabeculectomy and identify potential factors, such as lens status and pre-operative ocular parameters, that may be associated with decreased CECD.
Methods
Study population
This retrospective study involved 72 eyes of 60 patients who underwent trabeculectomy with a single ophthalmic surgeon (K.O.) at two private hospitals between January 2018 and June 2021. Indications for trabeculectomy were patients with primary open angle glaucoma and uncontrolled IOP despite maximum tolerated topical medical therapy and selective laser trabeculoplasty. Patients were excluded from the study if they underwent trabeculectomy combined with any other procedure.
Informed consent was obtained from all participants. This retrospective study was performed in accordance with the tenets of the Declaration of Helsinki. The study was evaluated by members of the Human Research Ethics Committee of the Northern Sydney Local Health District as a low or negligible risk study.
Data collection
Baseline data including age at surgery, sex, lens status and glaucoma medications were collected. Ocular parameters including anterior chamber depth (ACD), central corneal thickness (CCT) and axial length (AL) were obtained pre-operatively using IOL Master 700 (Carl Zeiss, Germany). CCT was also measured 6 months post-operatively. After trabeculectomy, the number of 5-fluorouracil (5-FU) injections administered during the follow-up period was recorded. IOP was measured by Goldmann applanation tonometry.
Corneal specular microscopy was performed on the central cornea pre-operatively and at 6 months post-operatively. Corneal endothelial cell analysis was conducted using an automated non-contact specular microscope (Tomey EM-3000, Nagoya, Japan). Measurements were obtained by a single examiner, K.O. using the same instrument. CECD was automatically calculated by the device and expressed as the number of cells/mm2. A series of fifteen photographs were taken by the specular microscope, and only the cell density evaluated from the clearest image was recorded.
Statistical analysis
Homogeneity of variance was assessed using Levene's test. The paired t-test was used to compare IOP, CECD and CCT pre-operatively and at 6 months after surgery. Differences in corneal endothelial cell loss between groups were evaluated using the Mann–Whitney U-test, independent t-test or one-way analysis of variance. The Pearson correlation coefficient was used to identify significant correlations between changes in CECD and pre-operative ACD, CCT and AL. A p-value less than 0.05 indicated statistical significance. All statistical analysis was performed using SPSS (version 26.0, IBM Corp., Armonk, NY).
Results
A total of 72 eyes of 60 patients underwent trabeculectomy. Baseline patient characteristics are shown in Table 1.
Baseline patient characteristics.
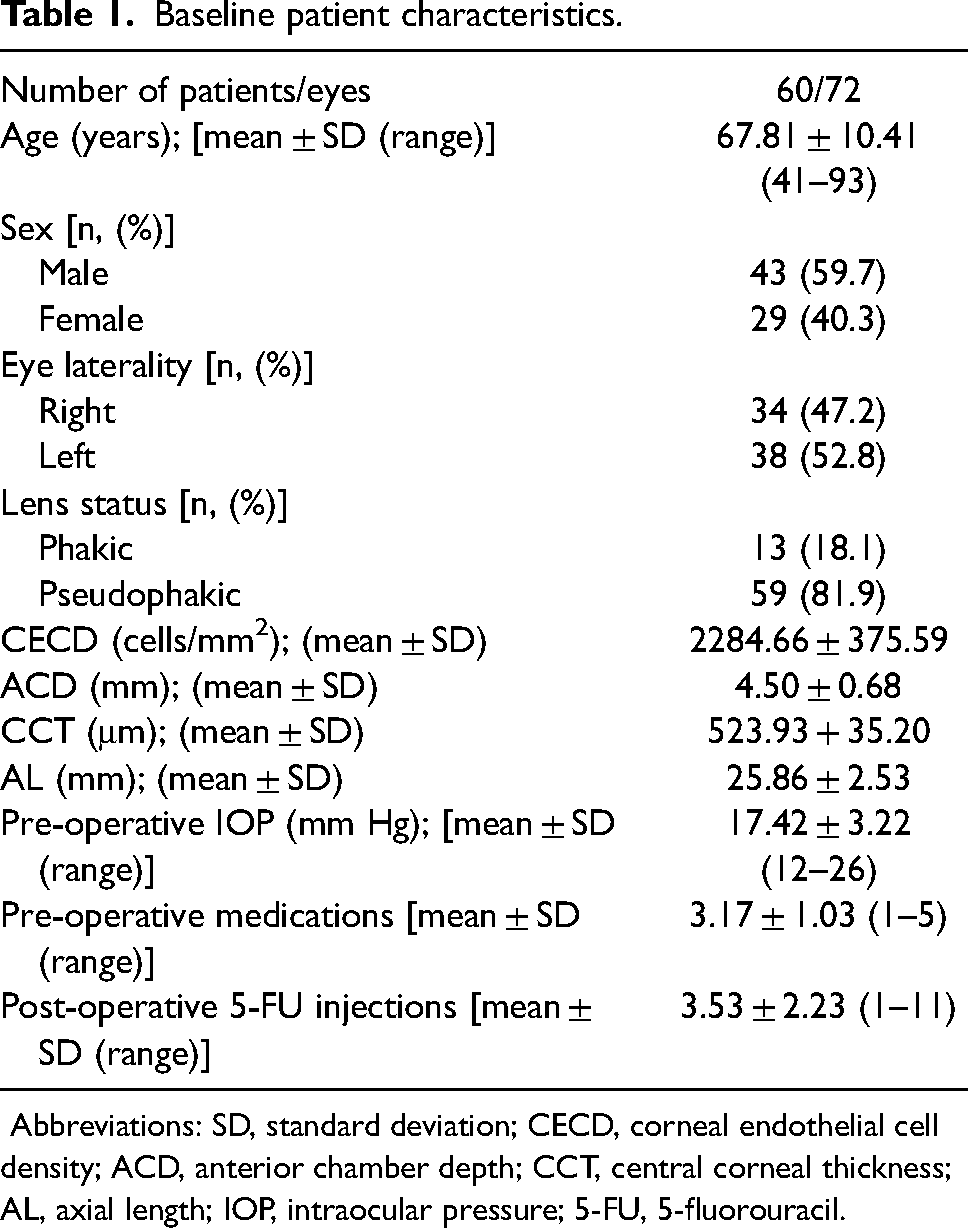
Abbreviations: SD, standard deviation; CECD, corneal endothelial cell density; ACD, anterior chamber depth; CCT, central corneal thickness; AL, axial length; IOP, intraocular pressure; 5-FU, 5-fluorouracil.
Pre-operative ocular parameters and CECD in the phakic and pseudophakic patient groups are presented in Table 2.
Pre-operative characteristics by lens status.
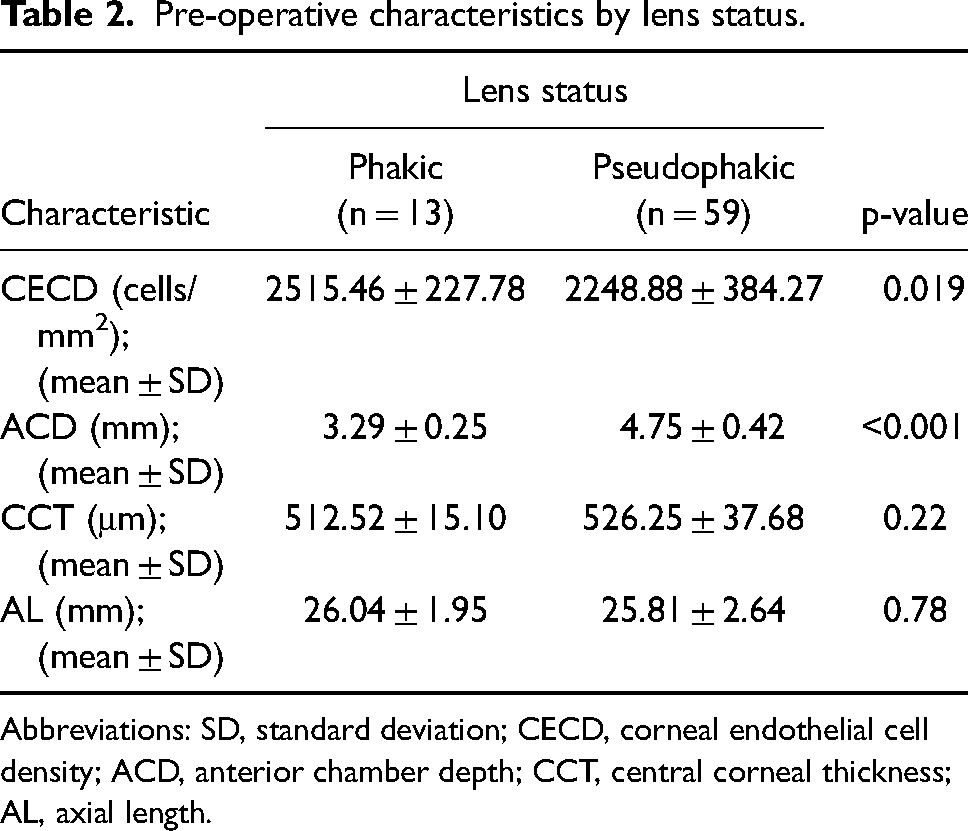
Abbreviations: SD, standard deviation; CECD, corneal endothelial cell density; ACD, anterior chamber depth; CCT, central corneal thickness; AL, axial length.
The changes in IOP, CECD and CCT from a pre-operative baseline are shown in Table 3. After trabeculectomy there was a significant decrease in IOP of 6.77 ± 4.10 mm Hg (p < 0.001). There were significant decreases in CECD (p < 0.001) and CCT (p = 0.008) 6-months post-operatively. The decrease in CECD was 155.15 ± 114.66 cells/mm2, representing a 9.88% mean cell loss.
Changes in IOP, CECD and CCT at 6 months after trabeculectomy.

Abbreviations: IOP, intraocular pressure; CECD, corneal endothelial cell density; CCT, central corneal thickness; SD, standard deviation.
Comparing changes in CECD between groups revealed significantly higher cell loss in phakic eyes compared with pseudophakic eyes (p = 0.005, Mann-Whitney U test). In phakic eyes, CECD decreased by 235.45 ± 118.32 cells/mm2 while in pseudophakic eyes CECD decreased by 137.82 ± 107.30 cells/mm2.
There were no significant differences in CECD loss after trabeculectomy between male and female patients (p = 0.62, independent t-test). In addition, one-way analysis of variance revealed no significant differences in CECD loss with the number of pre-operative glaucoma medications (p = 0.092) and the number of post-operative 5-FU injections (p = 0.17).
We found significant correlations between decreases in CECD and baseline ACD (Figure 1) and CCT (Figure 2). Increased cell loss was observed in patients with shallower anterior chambers (r = −0.27, p = 0.033) and in patients with thinner central corneas (r = −0.33, p = 0.009). No significant associations were found between CECD loss and patient age at surgery (p = 0.78), pre-operative CECD (p = 0.51) and pre-operative AL (p = 0.18).
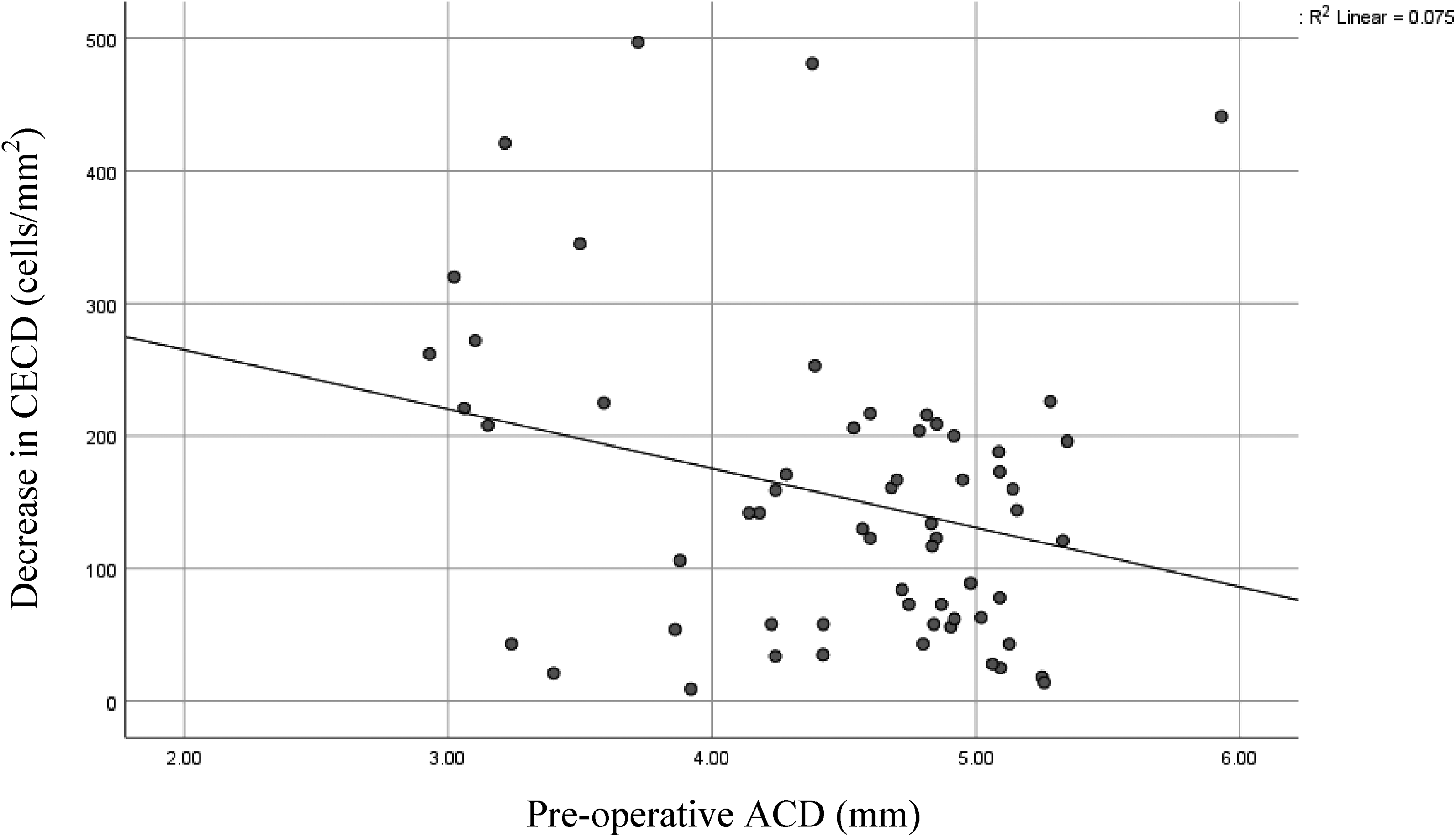
Scatter plot of pre-operative ACD versus CECD loss at 6 months post-operatively.
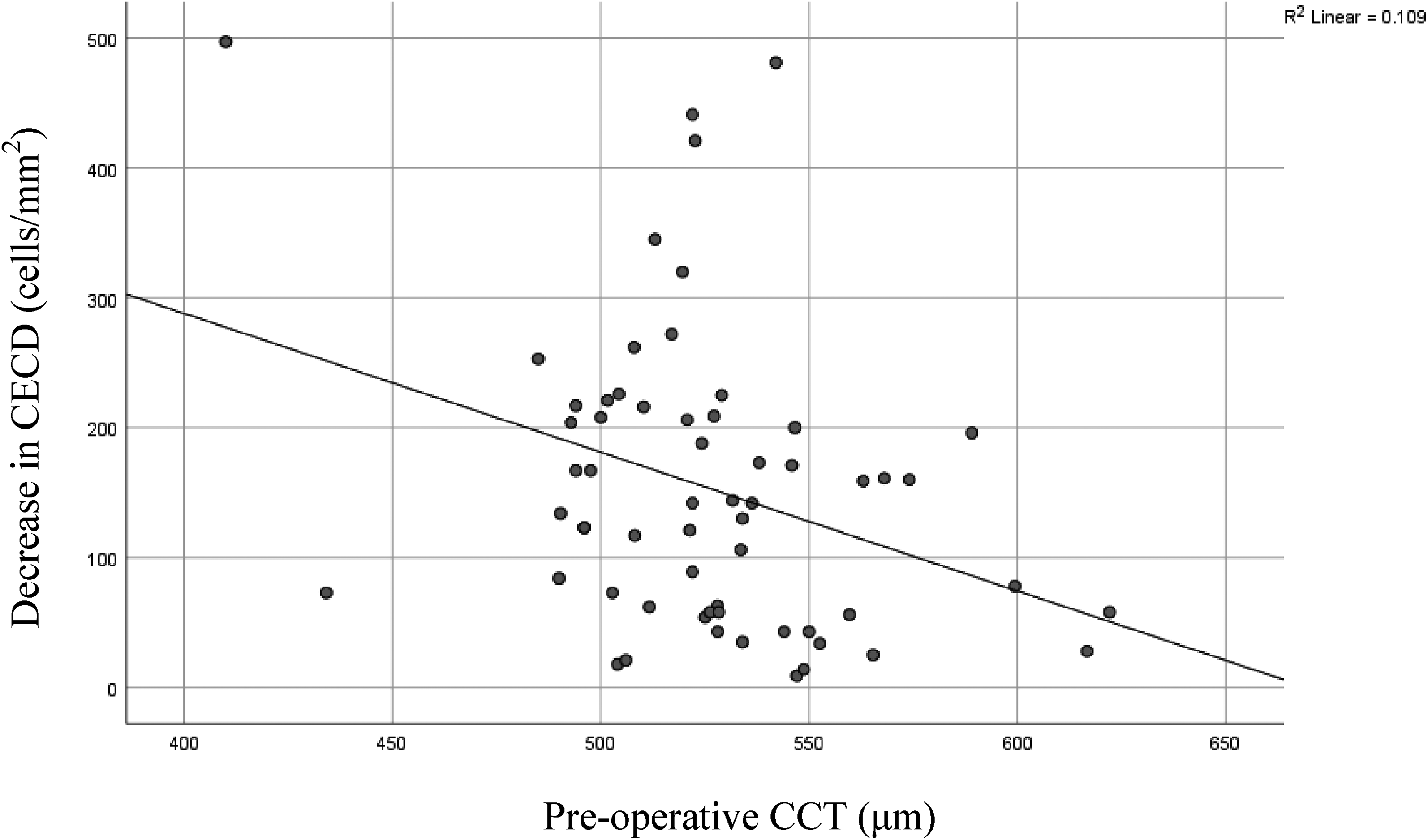
Scatter plot of pre-operative CCT versus CECD loss at 6 months post-operatively.
Discussion
To our knowledge, this study is the first to report significant associations between CECD loss after trabeculectomy and pre-operative ACD, CCT and lens status. The corneal endothelium is responsible for the maintenance of stromal deturgescence, acting as a regulator of fluid and ionic movements between the cornea and aqueous humour. 11 In humans, this monocellular layer has no replicative ability and undergoes cell loss at an estimated rate of 0.6% per year, decreasing from a mean 3500 cells/mm2 at 5 years of age to 2300 cells/mm2 at 85 years. 12
Following corneal trauma, an accelerated decrease in CECD occurs. Previous reports have identified CECD losses ranging from 1.9% at 6 months after trabeculectomy, 13 3.2% at 3 months 14 and 10% after 12 months. 9 The current study revealed a comparable CECD loss of 9.88% at 6 months post-operatively.
The mechanisms underlying the decline in CECD after trabeculectomy are multifactorial and not entirely understood at present.12,15 It is hypothesised that after corneal endothelial injury, remaining viable cells migrate and enlarge to compensate for the area damaged, thereby reducing overall cell density. 4 While the clinical consequences of small decreases in CECD are unclear, when CECD reaches less than 700 cells/mm2 there is a risk of corneal oedema and degeneration of vision. Compared to other anterior chamber procedures such as cataract surgery, filtering glaucoma surgery causes less cell loss, however corneal decompensation is not uncommon.5,14
Several variables have been considered as potential risk factors for increased CECD loss. More established risk factors include the administration of anti-fibrotic agents such as mitomycin C and 5-FU9,11,16 and a shallow post-operative ACD. 17 In recent years, studies have shown significantly greater cell loss associated with older age, type of glaucoma 10 and male gender. 4 Other variables, such as a history of diabetes mellitus, hypertension, previous intraocular surgery and post-operative needle revision have not demonstrated significant associations with post-operative CECD.4,10 Similar to previous studies, we identified no significant differences in CECD loss related to pre-operative CECD4,7 number of antiglaucoma medications and AL.10,13
As the amount of published literature in this area is limited, overall there is much variation regarding factors affecting corneal endothelial cell loss after trabeculectomy. Our study additionally reports significant associations with pre-operative ACD, CCT and lens status, all of which are novel risk factors.
Our findings of decreased cell loss associated with deeper anterior chambers and pseudophakic eyes have implications for clinical practice. Previous studies have analysed the impact of post-operative ACD on CECD changes,4,10,17 however none have investigated the effect of ACD prior to trabeculectomy. A smaller CECD decrease in patients who have undergone cataract surgery and have deeper anterior chambers prior to trabeculectomy may be due to a lower risk of iris-cornea contact. 4 Typical rates of cell loss after cataract surgery have been reported at approximately 10% in the first 12 months post-operatively.18,19 Contrastingly, in a recent prospective study, CECD decreases of 42.6% were observed 12 months after two-step phacotrabeculectomy, where trabeculectomy was followed by phacoemulsification after 3 months. 14 In instances of comorbid glaucoma and cataract both requiring surgical intervention, the results of our study suggest it may be reasonable for cataract surgery to be performed first. This may minimise the potential for further cell loss and corneal decompensation. Irrespective of lens status, CECD should be evaluated in all patients during glaucoma treatment planning, and reassessed during the post-operative period. 20
Our study reports a decrease in CCT 6 months after trabeculectomy compared to a pre-operative baseline (p = 0.008). While CCT has been shown to increase at 1 week-postoperatively, 21 in other studies, CCT has not demonstrated any significant change after surgery.5,14,22 A significant loss of corneal endothelial cells would be expected to affect CCT, particularly in the immediate post-operative period when corneal oedema occurs. 21 However, the overall amount of central corneal thinning in our cohort was small (6.04 ± 16.08 μm) and may not have notable clinical implications.
There are limitations of our study. Measurements of CECD have the potential for variability due to the nature of automated specular microscopy and sampling of images. In addition, assessments were solely made on the central cornea, where decreases in CECD have been described to be less prominent than in areas adjacent to the trabeculectomy filtration bleb. 23 The number of participants included in this study was relatively small and all patients were treated by a single ophthalmic surgeon, which may affect generalisability of findings. As the number of patients in the phakic group was smaller than the pseudophakic group, further studies in larger cohorts may be required to confirm whether other pre-operative variables may have independently affected amounts of cell loss. Finally, results were obtained after 6 months of follow-up, precluding the investigation of longer term changes.
Future studies evaluating the impact of peri-operative complications, such as hypotony and flat anterior chamber, would be beneficial as they may contribute to greater corneal endothelial loss after trabeculectomy. 24 Unfortunately, data on the incidence of such complications were unable to be obtained in the present study. Further, studies identifying the changes in CECD after staged surgeries compared to concurrent phaco-trabeculectomy, would additionally inform management of patients planned for both procedures.
In conclusion, significant CECD loss occurred after trabeculectomy. There was a lower CECD decrease in pseudophakic eyes, which could be as these eyes have a deeper anterior chamber. This suggests that if patients need trabeculectomy and cataract surgery, it may be better to perform cataract surgery first. As this was a 6 month study, a longer term study should derive more information.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.