
Abstract
Purpose
To report a case of type 3 macular neovascularization presenting with an epiretinal neovascularization.
Methods
Case report.
Results
A 65-year-old gentleman presented with complaints of reduced vision in the left eye (LE) having a best corrected visual acuity (BCVA) of 20/200. Based on fundus examination and multimodal imaging findings he was diagnosed with type 3 macular neovascularization (MNV). An additional unusual finding was the presence of an epiretinal membrane (ERM) and epiretinal neovascularization (ERN), with the latter finding being confirmed on optical coherence tomography angiography (OCTA). He underwent three doses of intravitreal ranibizumab injection following which there was reduction in the epiretinal vascularity.
Conclusions
Multimodal imaging of this case highlights the presence of epiretinal neovascularization associated with type 3 MNV, which has not been reported previously.
Keywords
Introduction
Type 3 macular neovascularization (MNV) is a form of neovascular age related macular degeneration (nAMD) and accounts for 12–15% of all new cases of nAMD. 1 Type 3 MNV refers to a down growth of vessels from the retinal circulation towards the outer retina with the vascular proliferation starting from the deep capillary plexus. 2 Intraretinal hemorrhage and cystoid edema can be present before the clinical appearance of neovascularization which has the potential to bleed. Additionally, subretinal fluid with gradual retinal thinning and emergence of pigment epithelial detachments (PED) can be observed. Proliferation to the level of RPE and eventual breakthrough of this layer can lead to sub-RPE neovascularization with potential for retino-choroidal anastomosis (RCA). Indocyanine green angiography (ICGA) is the gold standard in diagnosing this lesion and reveals a small hyperfluorescent lesion (hot spot) which represents the axial view of downward displacement of vessels and RCA in late stages of the disease. 1
Recent advances in spectral domain optical coherence tomography (SD – OCT) as well as OCT angiography (OCTA) has led to a better understanding of the disease and its stages as well as monitoring treatment. 2 Anti-vascular endothelial growth factors (VEGF) still remain the current first line option in its management. 3
Epiretinal neovascularization (ERN) is a relatively new OCTA finding which was initially described in association with macular telangiectasia type 2 (Mac-Tel 2) where these vascular epiretinal membranes (ERM) communicated directly with intraretinal hyperreflective structures of abnormal vascular plexus. 4 Vascularised ERM have also been described in retinal vascular diseases, Macular Telangiectasia Type 2 (Mac-Tel 2), idiopathic, retinitis pigmentosa (RP) and in Tersons syndrome. We report a rare case of type 3 MNV stage 3 which was associated with an ERN on multimodal imaging.
Case report
A 65-year-old gentleman with no history of systemic illness presented to us with diminution of vision in the left eye (LE) for 6 months. Anterior segment examination revealed pseudophakia in both eyes. Fundus examination of the right eye (RE) was unremarkable. The LE showed a yellowish white subretinal lesion at the macula with superficial vascular anastomosis nasally and a right angled vessel traversing through it temporally, along with traction lines and vessel distortion. There was subretinal hemorrhage at the lesion periphery [Figure 1]. SD – OCT of the LE revealed an irregular fibrovascular PED with a sub RPE and subretinal hyperreflective membranes, with an extension to the inner retina and connecting to the retinal surface with a tag-like projection into the vitreous cavity suggestive of ERM. Subretinal hemorrhage was also noted at the edge of the PED. SD – OCT of the RE was within normal limits [Figure 2]. OCTA of the LE revealed a high flow neovascular network at the vitreo-retinal interface, the superficial vasculature showed vessel distortion and disruption of foveal avascular zone with dipping in of superficial vessels. A large neovascular network was seen at the level of avascular outer retina–choriocapillaris slab. Corresponding colour-coded OCT B scans detected flow in the epiretinal network as well as in the abnormal neovascular network at the level of avascular outer retina–choriocapillaris slab [Figure 3].
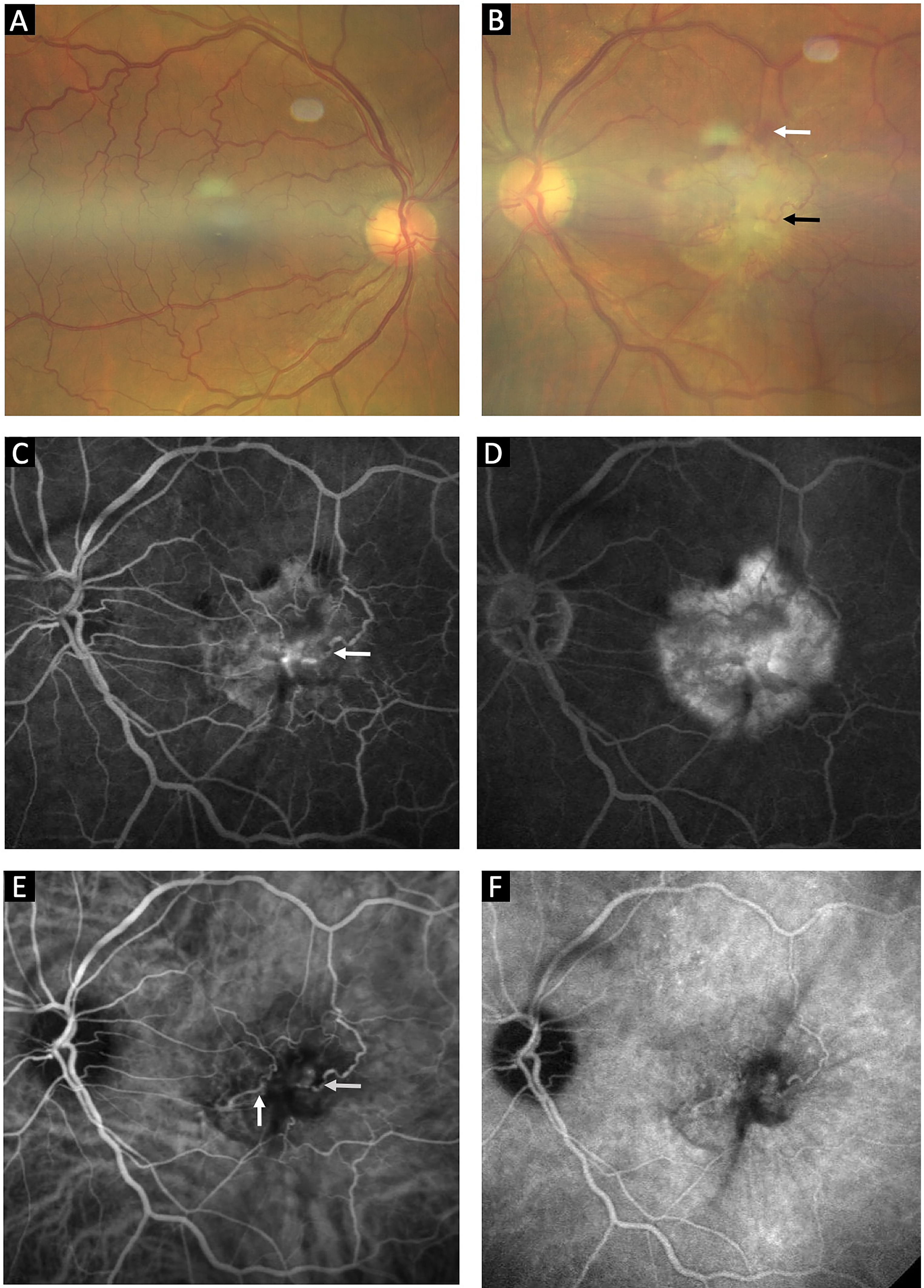
Colour fundus photograph of the right eye of the patient showing a normal fundus (A); Left eye of the patient revealing a yellow-white subretinal lesion with retinal vessels traversing the surface along with a right angled dipping venule at the temporal fovea (black arrow) and subretinal hemorrhage (white arrow) (B); Early phase of FFA revealing retinal vascular filling and leakage starting from the right angled dipping of retinal vessel (white arrow) at the temporal fovea (C); Late phase of FFA revealing hyperfluorescence increasing in size and intensity with surrounding diffuse leakage from subretinal and sub-RPE neovascularisation (D); Early phase of ICGA confirming the presence of retino-retinal anastomosis nasally (vertical white arrow) and retino-choroidal anastomosis at the region of the right angled vessel dipping (horizontal white arrow) (E); Late phase of ICGA showing washout of the dye (F).
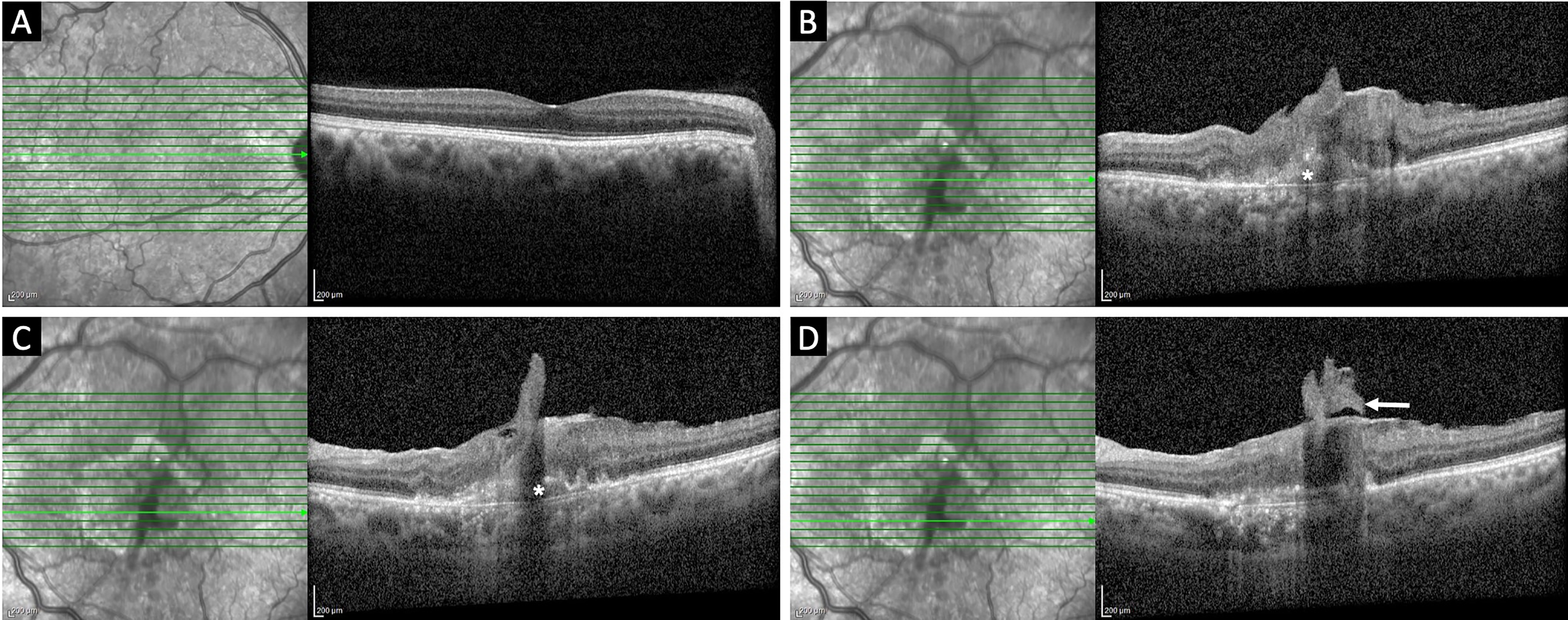
Serial SD-OCT images: Line scan through the fovea in the right eye revealing a normal contour (A); Line scan through the fovea in the left eye showing an epiretinal membrane with retinal layers along with type 1 macular neovascularization (asterix) (B); Line scan below the fovea revealing a tag like projection of retinal tissue into the vitreous cavity along with intra-retinal and sub-RPE neovascularization (C); Line scan below the fovea showing the epiretinal neovascular membrane projecting into posterior vitreous (white arrow) (D).
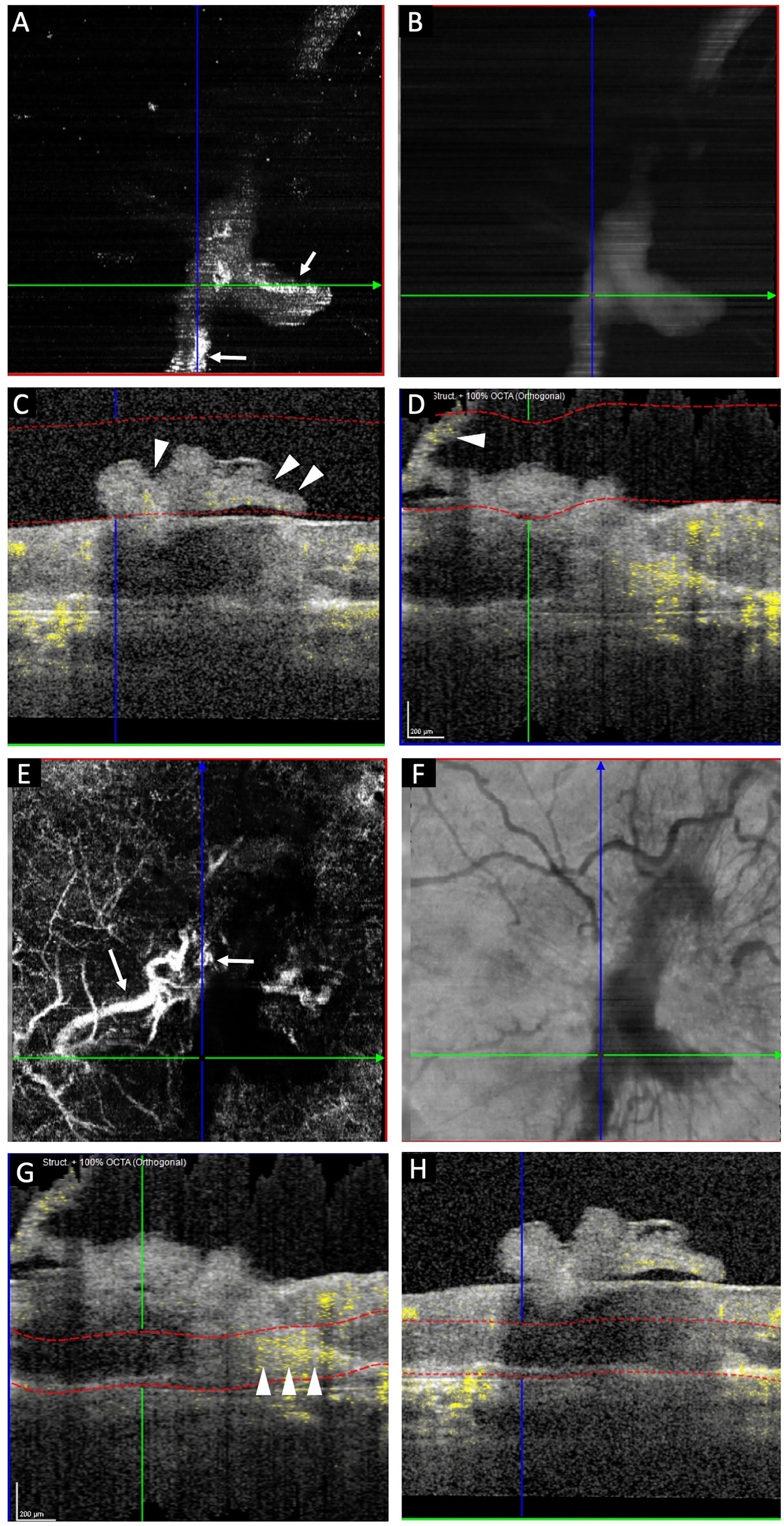
Serial OCTA images of the left eye: Epiretinal high flow neovascular network visualized at the vitreoretinal interface (A); Corresponding enface OCTA image (B); Vertical OCT B scan with the segmentation line at the level of the vitreoretinal interface revealing the presence of high vascular flow which is yellow colour coded (white arrow heads) (C); Horizontal OCT B scan confirming the presence of flow which is yellow colour coded (white arrow head) in the epiretinal neovascular membrane (D); Abnormal high flow large caliber neovascular network seen at the level of outer retina- choriocapillaris (white arrows) (E); Corresponding enface OCTA image (F); Vertical OCT B scan with the segmentation line at the level of outer retina - choriocapillaris revealing the presence of high flow which is yellow colour coded in the type 1 macular neovascularization (arrow heads) (G); Corresponding horizontal OCT B scan with the segmentation line at level of the outer retina-choriocapillaris (H).
Fundus fluorescein angiogram (FFA) in the early phase revealed retinal vascular filling associated with temporal right angle venular dipping and hyperfluorescence, with late diffuse leakage of active sub-RPE neovascularization suggestive of retino-choroidal anastamosis. ICGA in the early phase confirmed the presence of a retino-retinal anastomosis nasally and retino-choroidal anastomosis (white arrows) filling from the retinal side at the temporal foveal right angled dipping vessels into the neovascular network, with late phase dye washout [Figure 1].
Patient underwent three doses of LE intravitreal ranibizumab injections monthly apart and on his final review, BCVA in the LE improved to 20/125. SD – OCT showed reduction in size of the irregular PED with resolution of the subretinal hemorrhage. Additionally, OCTA revealed a reduction in the vascularity of the ERN and a reduction in the size of the neovascular network at the level of the avascular outer retina-choriocapillaris slab [Figure 4].
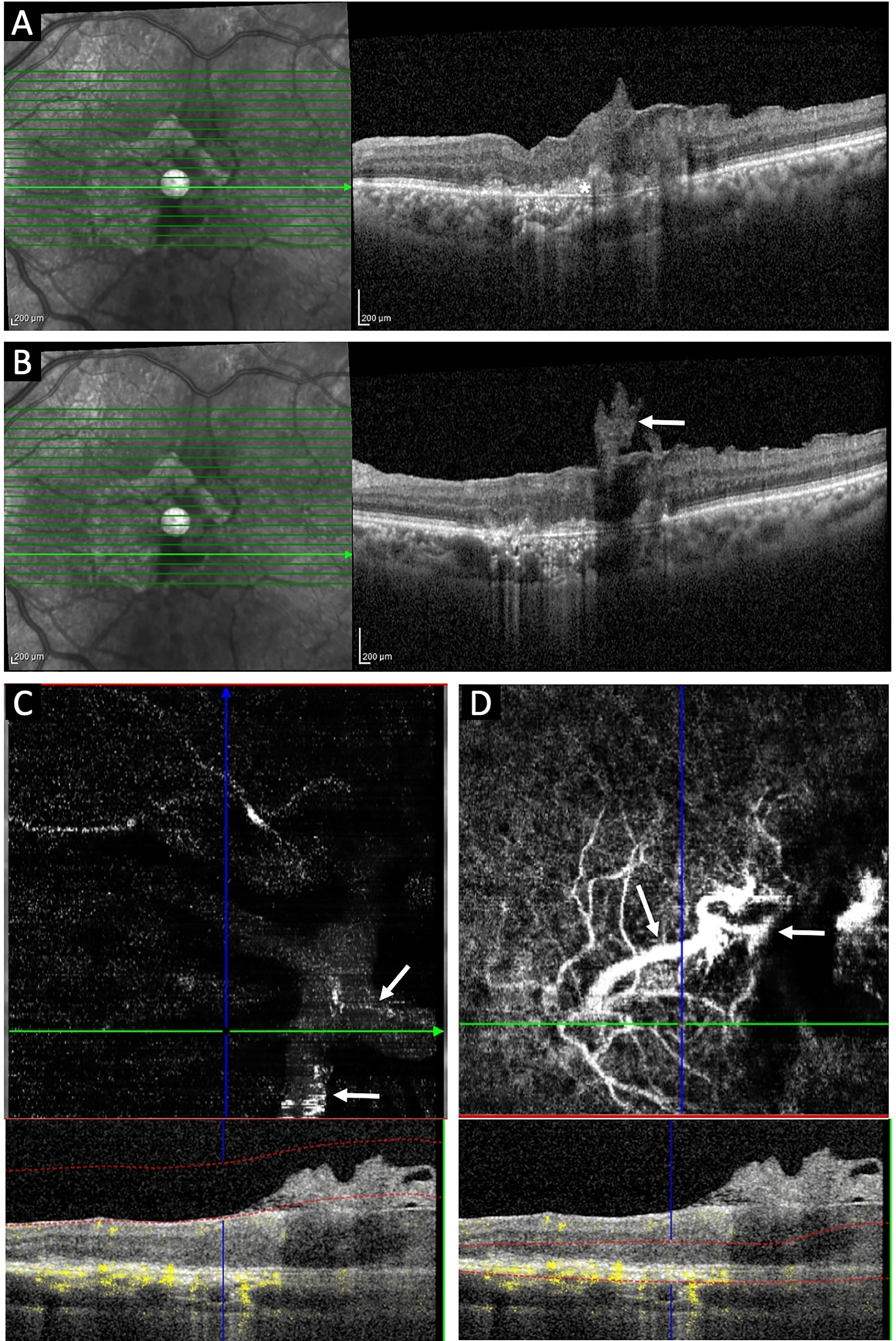
Serial SD-OCT & OCTA of the left eye after 3 doses of ranibizumab: Line scan through the fovea showing reduction in size of the type 1 macular neovascularization (asterix) (A); Minor reduction in size of the epiretinal membrane is seen (white arrow) (B); Reduction in the vascular flow of the epiretinal neovascular network seen with corresponding OCT B scan at the level of vitreoretinal interface (C); Mild reduction in size of abnormal vascular network with a persisting prominent feeder vessel suggestive of retino-choroidal anastamosis (arrows) seen with the corresponding OCT B scan at the level of the outer retina choriocapillaris (D).
An informed consent has been obtained from the patient for publication of images and data.
Discussion
We describe the multimodal imaging features of a unique case of type 3 MNV stage 3 associated with an ERN identified on OCT angiography. OCT angiography is an extremely useful tool to demonstrate the neovascular nature of the ERM at the vitreoretinal interface associated with MNV. ERMs have been categorized as idiopathic, secondary to other ocular disorders such as retinal vascular diseases, posterior uveitis, blunt trauma, retinal detachment and as well as post retinal laser photocoagulation or cataract surgery. ERMs have also been reported to be present in 26% of cases with nAMD, with more number of intravitreal anti-VEGF injections being required to achieve visual improvement in such eyes. 5 In retinal vascular diseases such as diabetic retinopathy and retinal vein occlusions fibrovascular ERMs have been described to form at the vitreoretinal interface due to retinal ischemia which is the root cause of angiogenesis.
Apart from retinal vascular disorders, vascularized ERM was initially described by Toffoli et al in a hypertensive patient with a history of cocaine use presenting with Terson's syndrome. They postulated that retinal vasospasm and hypertensive changes associated with decreased retinal perfusion lead to an ischemic environment which caused the ERM to vascularize. 6 Additionally, idiopathic vascular ERM was also described in a report by Gueunoun et al in a 70-year old woman and highlighted the importance of OCTA in picking up these ERMs. 7 Poornachandra et al described an idiopathic vascularized thick ERM extended from the disc to the fovea with no identifiable cause in a 53-year-old hypertensive woman and reported good visual recovery following pars plana vitrectomy. 8 Giachos et al reported a case of a 71-year-old male who presented with an ERM, a subhylaoid and intraretinal hemorrhage which was confirmed using multimodal imaging and described its treatment response with intravitreal Ranibizumab. 9 Lee et al in their report have described an ERN in a patient with RP and have shown reduction in vascularity post treatment with intravitreal bevazizumab. 10
Ayachit et al described ERN in seven eyes of four patients with Mac Tel 2 and with six of the seven eyes showing a communication with the intraretinal vascular network and with none of the eyes showing MNV. 4 Their series highlighted ERN as a new finding in Mac Tel 2 and emphasized the importance of OCT and OCTA in its diagnosis and evaluation. They postulated that retinal thinning and pigment abutting the ILM causing an ILM breach, may be responsible for the ERN formation which may be a distinct endpoint in Mac-Tel 2 much like MNV formation. 4 Similar to the above report, our patient had neither systemic diseases nor any retinal vascular diseases. However, he revealed presence of ERN associated with type 3 MNV on multimodal imaging. Type3 MNV has similarities with Mac Tel 2, with the presence of primary intra-retinal abnormal vascular plexus and proliferation and presence of right angled dipping of foveal vessels, being common to both these conditions. Vitreoretinal interface abnormalities including ERMs have been described in patients with nAMD, however there are no reports describing the presence of a vascularized ERM or ERN in association with type 3 MNV. ERN was diagnosed on the basis of the presence of a vascular membrane at the vitreoretinal interface that was distinct from the superficial retinal vasculature on OCTA.
Type 3 MNV usually presents with intraretinal hemorrhages, edema, hard exudates and PED. SD – OCT features include the presence of focal hyperreflective intraretinal lesion, intraretinal fluid with or without subretinal fluid, a vascularized PED with or without drusen. FFA usually reveals an occult leak and ICG reveals the characteristic hot spot at the PED centre. 2 Multimodal imaging features of our patient was consistent with stage 3 type 3 MNV with retino-choroidal anastomosis(RCA). Additionally, SD – OCT in our patient also revealed the sub RPE hyperreflective membrane extending into the subretinal space, inner retina and extending into the epiretinal plane, thereby simulating an ERN in the setting of RCA. OCTA confirms the vascularity of the ERN with corresponding deeper slabs revealing the ERN to be linked to an abnormal large caliber vascular network seen in the RPE- RPE fit slab again suggesting RCA. Pathogenesis of type 3 MNV involves the proliferation of the deep capillary plexus within the inner retina leading to intraretinal neovascularization and subsequently deeper extension into the subretinal space leading to subretinal neovascularization and finally sub-RPE and into the choroid causing choroidal neovascularization. 2 Dipping retinal venules have been described and visualized on OCTA that communicate from the epiretinal surface to the deep capillary plexus. 4 However, in our case since there is a well-defined neovascular network on the vitreo-retinal interface with an associated dipping venule, the associated ILM defect might have incited the extension intraretinal neovascularization to the epimacular surface, in addition to the VEGF mediated capillary proliferation. Following intravitreal ranibizumab injection there was mild reduction in vascularity of the ERN in our patient which was seen on OCTA.
To conclude, we describe the multimodal imaging features of a hitherto undescribed finding of ERN in a patient with type 3 MNV in stage 3.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.