
Abstract
Purpose
Strabismus sursoadductorius is the most common strabismus of the oblique eye muscles. The changes in squint angle, elevation in adduction, abnormal head posture and binocular vision were collected to get an overview of the results at the largest clinic in Austria.
Methods
This study is a retrospective study. The orthoptic and ophthalmologic parameters of 102 patients who were treated in the Department of Ophthalmology and Optometry between January 2017 und September 2020 were collected and statistically analysed.
Results
The mean age was 12.2 ± 14.8 years. The squint angle changed from 18.3 ± 6.3 presurgical to 13.4 ± 9.7 (p = 0.09) with Hirschberg measurement. The squint angle changed from 12.5 ± 7.7 to 6.7 ± 4.9 (p < 0.01) at distance and from 12.5 ± 7.6 to 6.1 ± 4.5 (p < 0.01) at near with the prism covertest. Elevation in adduction showed a highly significant change (p < 0.01) from 15 ± 5.6 to 1.4 ± 2.8 degrees on average postsurgical. In binocular vision at distance there was also a highly significant (p < 0.01) change with 21.6% to postsurgical 37.3% positive tests. At near, the positives also increased significantly (p = 0.01) from 32.4% to 39.2%. There was no significant change in stereo vision (p = 1.0). Presurgical 52.9% of the sample had an abnormal head posture, postsurgical it was 38.2%, this change is also highly significant (p < 0.01).
Conclusion
The change was significant to highly significant for most parameters (i.e., squint angle, elevation in adduction, and abnormal head posture).
Key messages
If the patient with strabismus sursoadductorius suffers from diplopia, or has an abnormal head posture that can cause chronic muscle tension in the neck or cervical spine discomfort, a strabismus surgery is indicated. In order to reduce the psychological burden of strabismus sursoadductorius and to achieve long-lasting surgical results, strabismus surgery is recommended in childhood for this diagnosis. The results showed a statistically significant improvement in squint angle, elevation in adduction, and abnormal head posture. In the subgroup analysis, it is shown that strabismus surgery can lead to an improvement of binocular vision when strabismus sursoadductorius is diagnosed. The squint angle measurement by Hirschberg test is not recommended for a statistical analysis because it is inaccurate.
Introduction
Strabismus sursoadductorius describes an elevation during adduction of the eye, which is caused by an overfunction of the obliquus inferior muscle or an underfunction of the obliquus superior muscle. It is the most common eye muscle disorder of the oblique eye muscles. 1 According to current scientific knowledge, the exact etiology of this strabismus can be attributed to several causes. For example, hypoplasia of the trochlear nerve or its tendon and a resulting weakness of the superior oblique muscle. Another possible cause may be a dysinnervation of the oculomotor nerve, whereby the clinical picture must be attributed to the congenital cranial dysinnervation disorders.2,3
This congenital strabismus affects individuals of all ages. 2 It can happen that strabismus is well compensated and remains undetected until adulthood. 2 Then it may become conspicuous by complaints such as double vision, asthenopia, or an abnormal head posture. 2 It is important to separate differential diagnoses such as acquired trochlear nerve palsy, dissociated vertical divergence, associated vertical strabismus, or muscular head constraint from true strabismus sursoadductorius.4,6 If these differential diagnoses are ruled out, and the patient suffers from diplopia, or has an abnormal head posture that can cause chronic muscle tension in the neck or cervical spine discomfort, strabismus surgery is indicated.2,4
Aoba and Matsuo 7 describe in their article that surgery for strabismus sursoadductorius performed in childhood leads to a more long-lasting postoperative result due to the improved fusion ability.
Strabismus sursoadductorius can often occur in combination with strabismus convergence and less frequently with strabismus divergence. 8 The sample used for this study therefore includes patients with the common overaction of the musculus obliquus inferior present in essential infantile esotropia and weak superior oblique tendon, as well as other concomitant horizontal strabismus combined with strabismus sursoadductorius. This phenomenon is defined as “combined strabismus sursoadductorius” in this article; without horizontal strabismus, the strabismus sursoadductorius is described as “isolated strabismus sursoadductorius”.
Moreover, the psychosocial burden of strabismus affecting appearance must be considered an indication for strabismus surgery.6,9
The described patients, all have excessive elevation in adduction respectively hypertropia of the affected eye in primary position and had a surgery according to that on their ipsilateral oblique inferior muscle.
We describe and evaluate the results from the largest eye clinic in Austria and follow the patients one year after surgery. The results help us to improve our performance.
Subjects and methods
This work is a retrospective ex-post facto study in longitudinal design. A data analysis of medical findings with strabismus sursoadductorius at clinic for strabismus, pediatric ophthalmology and pediatric ophthalmosurgery between January 2017 and September 2020 was performed.
The surgical method was as follows: Exposure of the tendon of the rectus lateralis muscle, insertion of a 4–0 retaining suture or crosshook and rotation of the bulb nasally upward, exposure of the tendon of the obliquus inferior muscle, detachment and preparation of the tendon from the scleral attachment, refixation in terms of a recession between 10 mm to 12 mm. In some cases, an additional Anteorization of 2 mm to 4 mm was performed. Closure of the conjunctiva with 8–0 Vicryl.
Inclusion and exclusion criteria
Subjects of any age and sex with unilateral or bilateral strabismus sursoadductorius with or without abnormal head posture or with congenital trochlear nerve palsy were included.
Exclusion from this study was due to nystagmus, documented inadequate cooperation of the patient during the assessment, inadequate documentation (for example, missing pre- or postsurgical findings), Graves’ disease, repeated surgery on the same muscle.
Parameters and statsitical analysis
Measurements of the angle of squint are assumed to be the main outcome. This parameter was assessed in two ways, depending on the age of the patient, either by prism covertest or by Hirschberg measurement. Elevation in adduction and measurements of head posture and binocular vision represent the secondary target parameters. Age, gender, and surgical method are considered exploratory parameters.
Other parameters used are the diagnoses, the elevation in adduction, the presence of combined or isolated strabismus, the side of the treated eye and the operative method (repositioning/ anteorization/ combined or isolated).
Therefore, for the variable strabismus angle, the difference between the presurgical measurements and the postsurgical measurements was calculated. Mean, standard deviation, median, minimum, and maximum were calculated for the two time points (presurgical and first examination postsurgical) and for the calculated differences. Graphically, these results were presented using bar charts.
The significance level for all statistical tests was assumed to be α = 0.05, and the confidence interval was calculated as 95%.
Statistically, with a sample size of 102, there is a power of 80% with a two-sided significance level of 5% in this work.
The study adhered to the tenets of the Declaration of Helsinki and was approved by the local ethics committee of the Medical University of Vienna, Austria.
Results
A total of 143 patients who underwent surgery on their inferior oblique muscle during the selected period was decimated to 102 after applying the exclusion criteria.
The frequencies of combined and isolated strabismus sursoadductorius were determined based on the diagnoses for this study.
The main diagnoses in our selected sample were strabismus convergens, strabismus divergens, strabismus sursoadductorius, other congenital oblique disorders, infantile esotropia, decompensated convergent or divergent phoria, periodic alternating strabismus convergens, non-accommodative esotropia, accommodative and partially accommodative esotropia.
The first postsurgical orthoptic and ophthalmologic examination of the treated patients took place after a mean of 8.2 days. The calculated standard deviation is 16.9 days, the median 6 days.
Postsurgical squint angle
Statistical analysis of this variable was performed in two ways to obtain better comparison and significance of the data.
Due to the large confidence intervals for statistical analysis using the t-test for connected samples or Wilcoxon-test of some of the patients in the subgroup analysis, the frequencies of the strabismus angle measurements were also calculated (Figure 1).
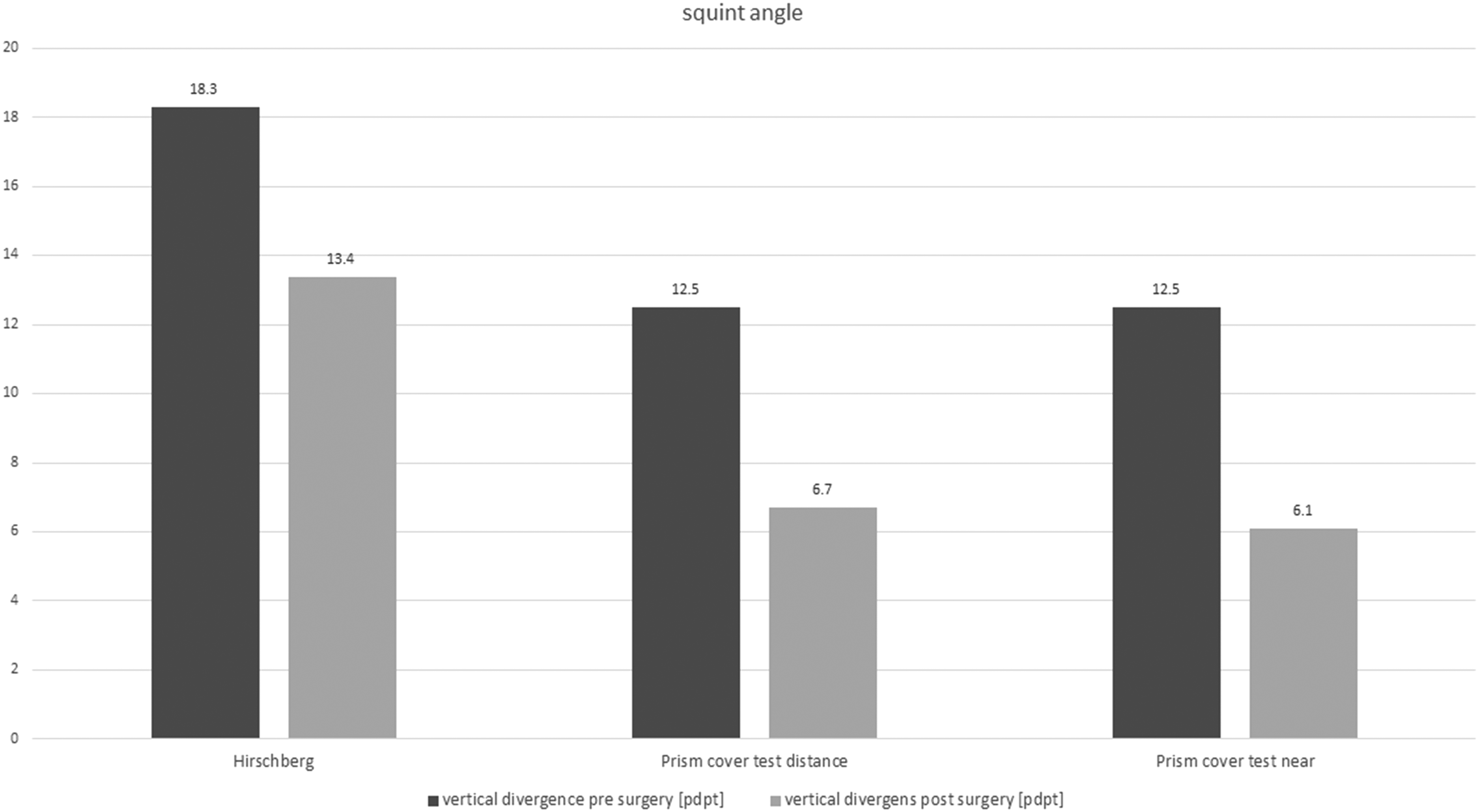
Pre- and postsurgical squint angle.
Postsurgical elevation in adduction
In order to elicit the results and the effect of the surgical method, the data of the postsurgical elevation in adduction are analyzed in this chapter. Again, the absolute change in the hyperfunction of the obliquus inferior muscle is calculated by frequencies on the one hand, and the significance of the change is calculated by McNemar's test on the other hand (Figure 2).
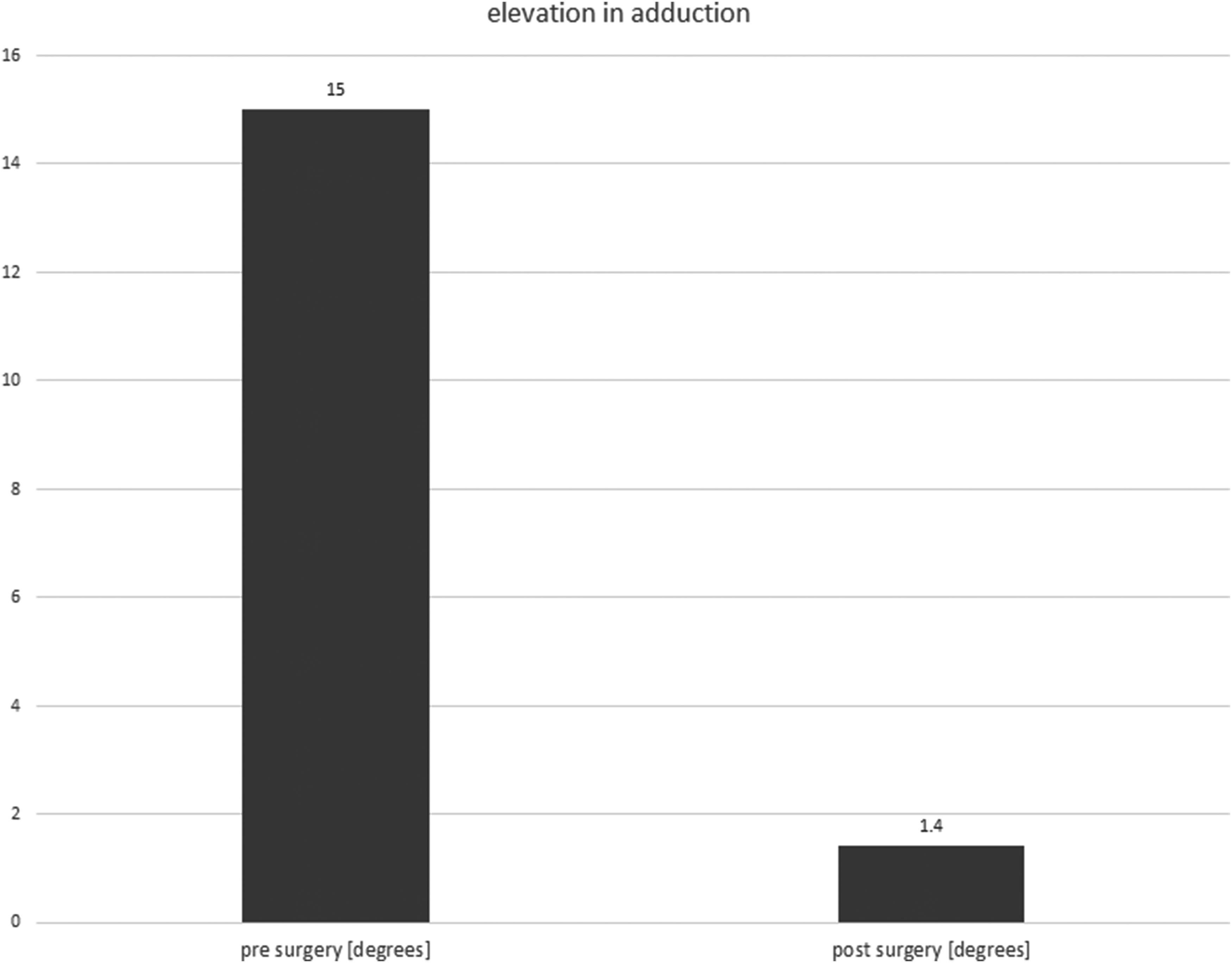
Pre- and postsurgical elevation in adduction.
Postsurgical abnormal head posture
First, the absolute frequencies of the abnormal head posture are calculated and compared with the presurgical values. Then the statistical evaluation of the significances is carried out using the McNemar test (Figure 3).
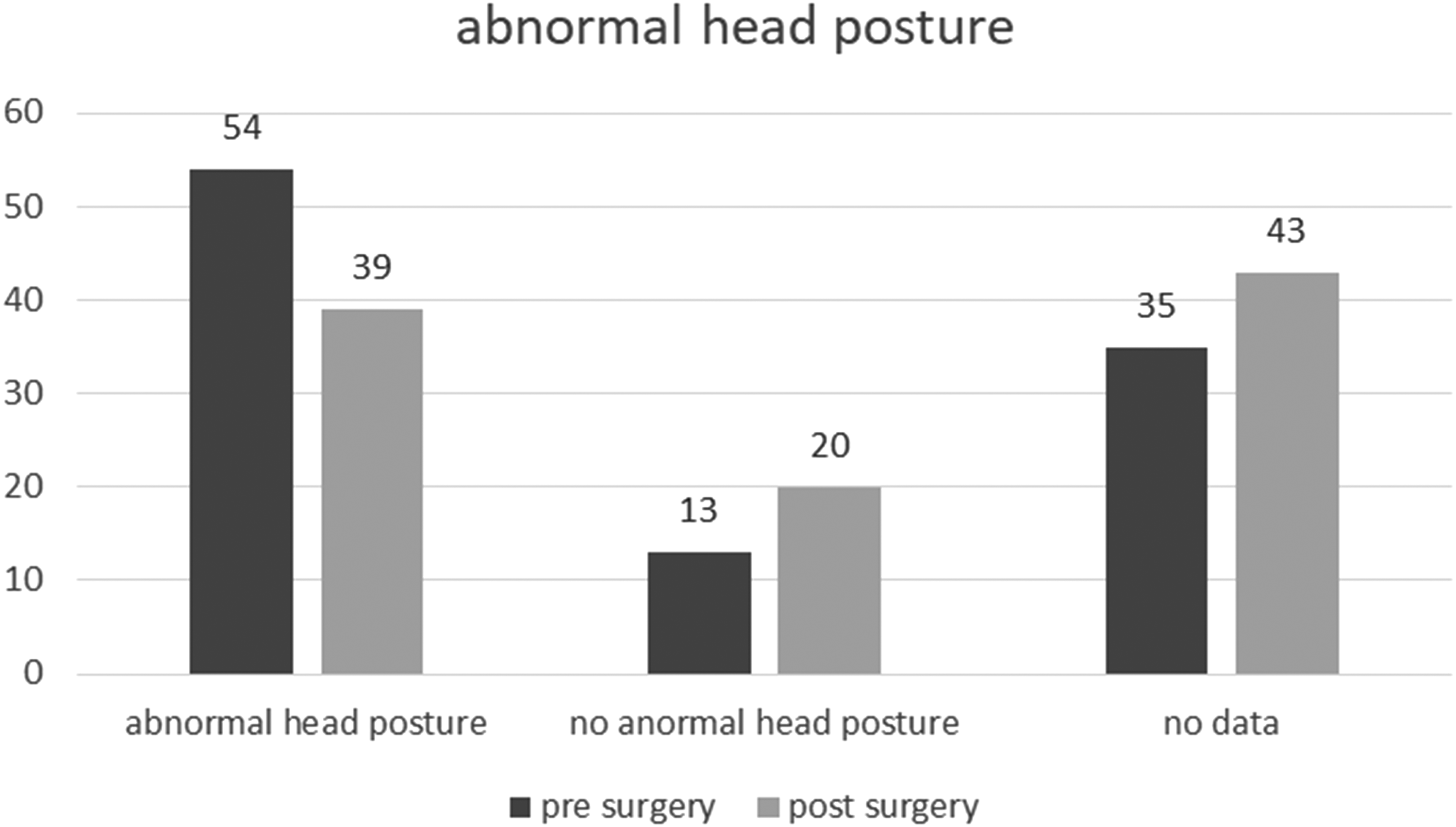
Pre- and postsurgical abnormal head position.
Postsurgical binocular vision
The absolute frequencies of the postsurgical data were analyzed, compared with the presurgical data and presented by bar charts for comparison (Figure 4).
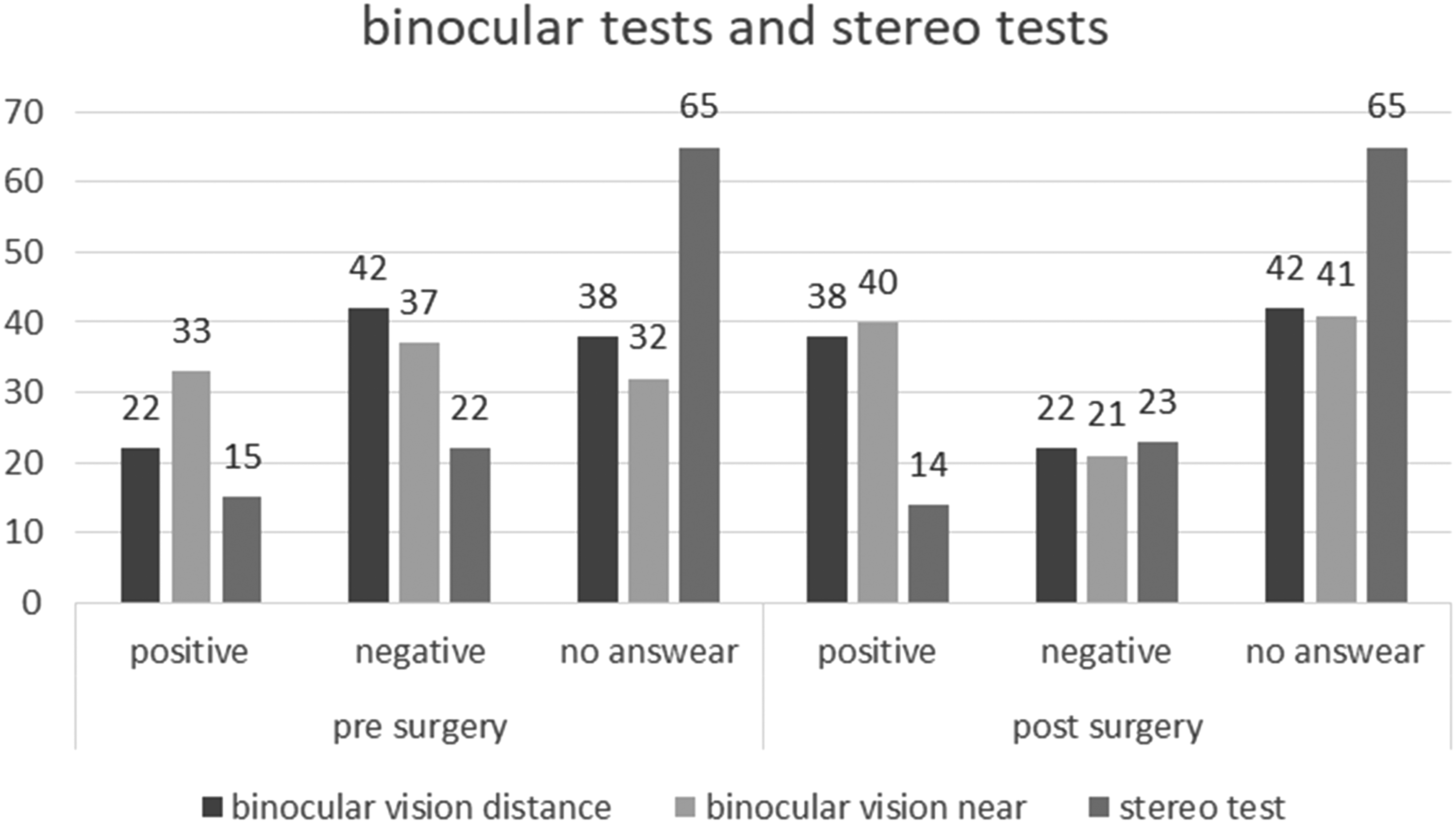
Pre- and postsurgical binocular tests and stereo tests.
In a further subgroup analysis, the data of 36 patients with isolated strabismus sursoadductorius were analyzed. In comparison to the whole sample, it can be seen that 58.3% of the patients reported positive binocular vision at distance and 75% at near. 36.1% also had positive stereo vision. After the surgery these binocular vision values increased to 77.8% and stereo vision to 41.7%. Statistical analysis using McNemar's test showed a significant change in binocular vision at distance with p = 0.016, the changes in binocular vision at near and stereo vision were not significant.
Discussion
The purpose of this paper was to explore the change in orthoptic outcome to be measured after surgery of the inferior oblique muscle using a retrospective data analysis of different parameters.
The age distribution of the sample in this study was a mean of 12.2 years, but the median is five years. This suggests that most patients were younger than the calculated mean. In some cases, values of some parameters are missing and could not be used for the statistical evaluation due to this low median age.
The distribution by gender was balanced with 54 female and 48 male participants.
Presurgical data showed that overactivity of the oblique inferior muscle was less frequent in the right eye (67.6%) than in the left eye (78.4%). The distribution was similar for strabismus surgery. While 27.5% of patients underwent surgery on the right eye, 42.2% underwent surgery on the left eye.
When the frequencies of combined strabismus are compared with the performance of combined surgery in this sample, it is noticeable that a total of 74 patients (72.5%) in the sample had either combined convergence or combined divergence. This is more than twice as many individuals as those with isolated strabismus sursoadductorius (27.5%). However, combined surgery was performed in only 65 participants (63.7%). In 36.3% of the patients the isolated strabismus sursoadductorius was treated.
Change of the squint angle
The change in squint angle is considered to be highly significant in almost all areas for this study. For the Hirschberg measurements at near, there was an insufficient amount of data when evaluating the vertical divergence, so it cannot be considered for the discussion.
Better comparisons were obtained for the measurements using the prism cover test at distance and near, so that a highly significant change in the sense of a reduction in vertical divergence could be shown in all points with p < 0.01 (Figure 1).
In the retrospective study by Nejad and Thacker 10 surgical data of 45 patients with a vertical divergence of more than 20 pdpt in primary position are analyzed and the results of different surgical methods are compared. According to the study authors, the repositioning of the obliquus inferior muscle produced a significant result with p = 0.02, but the evaluation showed undercorrection in 75% of cases with this surgical method. These results suggest that retraction of the obliquus inferior muscle in combination with retraction of the contralateral rectus inferior muscle should be considered for large vertical divergences in primary position.
Enz and Jaggi 11 performed a retrospective cohort study of 45 patients with congenital trochlear nerve palsy. A repositioning and an anteorization of the oblique inferior muscle was performed in all subjects. Both, three months postsurgically and one year postsurgically showed a highly significant change in terms of a reduction in vertical divergence in primary position with p < 0.01. Enz and Jaggi 11 share the opinion that even in cases of severe strabismus sursoadductorius with a vertical divergence of up to 20° or 35 pdpt in primary position, an anteorization as first surgery can be used as the method of choice as we did with our patients.
Change of the elevation in adduction
The change in elevation in adduction was highly significant (p < 0.01) postsurgery compared to presurgery in this sample (Figure 2).
In a randomized prospective study, Mostafa and Kassem 12 compared surgical outcomes for unilateral strabismus sursoadductorius. The sample of 34 patients was divided into two groups; one group received unilateral and the other received bilateral retraction of the obliquus inferior muscle with or without anteorization. They showed a postsurgical success rate of 64.7% in the unilateral group and 76.5% in the bilateral group.
Enz and Jaggi 11 showed a significant change in elevation in adduction postsurgery after repositioning and anteorizationing the affected obliquus inferior muscle.
Change of the abnormal head posture
For the statistical investigation of abnormal head posture, a binary evaluation was chosen for this study. We distinguished between existing and non-existing abnormal head posture. The young age of some patients is the reason for this approach, since at this age an accurate measurement by goniometer was often not possible and could only be estimated in the findings. Nevertheless, a highly significant change in the sense of an improvement of the head constraint posture could also be found here between the pre- and the postsurgical examination with p < 0.01. This can also be seen in Figure 3.
Bahl and Marcotty 13 compared retrospective surgical results of 85 patients who were treated either by myectomy or by repositioning. It was shown that myectomy produced a significantly better result in postsurgical abnormal head posture. Other parameters, such as vertical divergence or diplopia, showed no significant differences between the two surgical methods.
Change of the binocular- and stereovision
Due to the high number of children under four years of age (29.4%), whose information on binocular and stereo vision was mostly not or only partially possible in the findings, the results of these parameters are less clear than for the squint angle measurements. Nevertheless, a statistically significant change can be detected especially in binocular vision postsurgically at distance with p < 0.01 and at near with p = 0.012. In stereo vision, neither a significant change in the paired samples nor a change in the evaluation of the frequencies was shown postsurgically (Figure 4).
Thus, it must be assumed that surgery of the inferior oblique muscle does not lead to a significant improvement in stereo vision. Nevertheless, it should be taken into account that 72.5% of the patients in this sample had a combined convergence or divergence in addition to the strabismus sursoadductorius. In congenital or childhood-acquired strabismus no positive stereo vision is expected after surgery.
Enz and Jaggi 11 assessed stereo vision using the Lang test, as in the study performed here. However, they were also unable to detect any significant change except for a trend toward a slight improvement postsurgically.
Schmidt and Gräf 14 conducted a retrospective study of 36 children whose strabismus surgery had been performed before the age of eleven. Strabismus angle, head constraint posture, and binocular and stereo function were collected and analyzed in several different ways. Again, there was no significant change between the pre- and postsurgical binocular and stereo vision results.
With focus on the subgroup analysis of patients who had isolated strabismus sursoadductorius, it is noticable that a higher percentage of patients had a positive binocular test preoperatively compared to the entire sample. This percentage increased postoperatively in each case. This shows that strabismus surgery can lead to an improvement of binocular vision when isolated strabismus sursoadductorius is diagnosed. Nevertheless, only a significant change in binocular vision at distance could be demonstrated. However, the subgroup is quite small with 36 patients, therefore a further study with a larger sample in a prospective design may determine possible significances for binocular vision at near and stereo vision.
Conclusion
Due to the high number of children in the sample, some data could not be collected, which means that especially in binocular vision no valid effect can be detected. Overall, also considering the literature, it appears that a single strabismus surgery in childhood is beneficial and often sufficient. In contrast, more measurements can be made presurgically for surgery of strabismus sursoadductorius in adulthood, which can lead to a more accurate assessment of the extent of overactivity of the obliquus inferior muscle and assist in the choice of surgical method.
Thus, we agreed to decide individually in each patient.
Another important finding was that although measurement of the strabismus angle using the Hirschberg test is a helpful tool in everyday clinical practice for quick and uncomplicated assessment of the strabismus angle, the data measured with it are not sufficiently usable for statistical analysis.
The studies found in the literature on this topic often differ greatly in the selection of the parameters collected, the surgical method, or the sample. However, some of these studies also show significant results for the same parameters as in this study. Therefore, we conclude that despite the high level of research, there is no consensus on the correct surgical method for strabismus sursoadductorius.
Thus, this suggests that the surgical method must be chosen individually for each patient based on her or his amount of strabismus, abnormal head posture, elevation in adduction, and a combined horizontal strabismus.
Footnotes
Author contribution
ES, SRD, VVS: design of the study; ES, SRD, VVS: data collection and analysis; SRD, ES, VVS: writing of the manuscript; ES, SRD, TN, USE, VVS: critical review of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.