
Abstract
Purpose
To investigate the need of rebubbling for small graft detachments after Descemet Membrane Endothelial Keratoplasty (DMEK).
Methods
In this retrospective study we evaluated 111 eyes from 111 patients that showed graft detachment after DMEK surgery and have achieved graft adherence by injection of air or 20% sulfur hexafluoride (SF6) to the anterior chamber (rebubbling group; n = 57) or by spontaneous adherence without intervention (control group; n = 54) at final examination. Subgroups in terms of the maximum height and in terms of the detachment area in relation to graft area were formed. Outcome measures were the increase in best-corrected visual acuity (BCVA) and the decrease in central corneal thickness (CCT) from the measurement before DMEK to six months after surgery and postoperative endothelial cell density.
Results
BCVA increased in the rebubbling group and the control group, the difference being 0.22 logMAR, p = 0.048. For eyes with a maximum height less than 500 µm, the increase of BCVA was 0.39 ± 0,36 logMAR in the control group and 0.62 ± 0,53 logMAR in the rebubbling group, p = 0.045. There was no difference of statistical significance of BCVA between both groups regarding the detachment area of less than 20% in relation to graft area. The mean decrease in CCT and postoperative endothelial cell density showed no significant difference between the rebubbling group and the control group.
Conclusion
Compared to spontaneous graft adherence, a rebubbling shows no beneficial effect on the clinical outcome for small detached DMEK grafts. Rebubbling does not decrease postoperative endothelial cell density.
Introduction
Since Melles et al. 1 first described Descemet Membrane Endothelial Keratoplasty (DMEK) in 2006, this type of transplantation has become the gold standard surgery for corneal endothelial disorders like Fuchs endothelial corneal dystrophy. Benefits include fast visual rehabilitation as well as few occurring complications.2–4 Still, the most frequent postoperative complication is partial graft detachment. 5 The injection of air or 20% sulfur hexafluoride (SF6) into the anterior chamber, so called rebubbling, is a widespread intervention to reattach the graft to the host posterior stroma. Graft detachments nearly always appear immediately after surgery but then often attach spontaneously.6,7 However, they are clinically relevant when resulting in stromal edema with reduction of visual acuity. Still, it is contentious whether a rebubbling then is necessary. Fluctuating rebubbling rates in various centres5,8,9 indicate that there are no consistent, widely accepted clinical algorithms. Usually, rebubbling is performed when graft detachments involve the optical axis. 8 In cases of smaller dehiscence, it is also possible to wait for spontaneous graft adherence. So far, there are no clear standards for small graft dehiscence.
The aim of our study was to evaluate the need of rebubbling by means of the clinical outcome for DMEK grafts that reattached after initial dehiscence. We especially focused on detachments of small size and a low maximum height of graft detachment.
Methods
In this retrospective monocentric study, we evaluated clinical data of digital patient files and postoperatively taken Optical Coherence Tomography (OCT)- scans of 111 eyes (111 patients) undergoing DMEK surgery and showing graft detachment postoperatively at the Department of Ophthalmology, University of Leipzig Medical Center, between March 2012 and February 2018.
All included eyes achieved complete graft adherence through rebubbling or through spontaneous adhesion until final examination six months after surgery. Eyes were excluded if OCT quality was insufficient to assess or if data was incomplete. In order to avoid selection bias, subsequent eyes of the same patient were not included in the analysis.
Two groups were formed according to the therapy of graft detachment: the rebubbling group comprising eyes with one or more rebubbling procedures and the control group consisting of eyes that had no intervention. The primary outcome measure was the increase in best-corrected visual acuity (BCVA), the secondary outcome measures were the decrease in central corneal thickness (CCT) in the period from preoperative measurement to the final examination and the endothelial cell density (ECD) taken from the follow-up visit 6 months after surgery. ECD was measured using specular microscopy (CEM-530, Nidek® Co., Ltd, Tokyo, Japan) but measurements were not routinely performed in all patients.
Demographic patient data, ophthalmological diseases including reason for surgery, BCVA and type of initial tamponade were evaluated. Clinical examination and measurements were performed preoperatively as well as six months postoperatively.
Graft adherence or graft detachment was identified and measured using Heidelberg Spectralis® OCT (Heidelberg Engineering®, Heidelberg, Germany) and Heidelberg Eye Explorer® Version 1.10.4.0. Preoperative and postoperative CCT, the detachment's maximum height, detachment's width and diameter were quantified. The detachment's localization was classified in thirds of the cornea as described by Siebelmann et al. 10
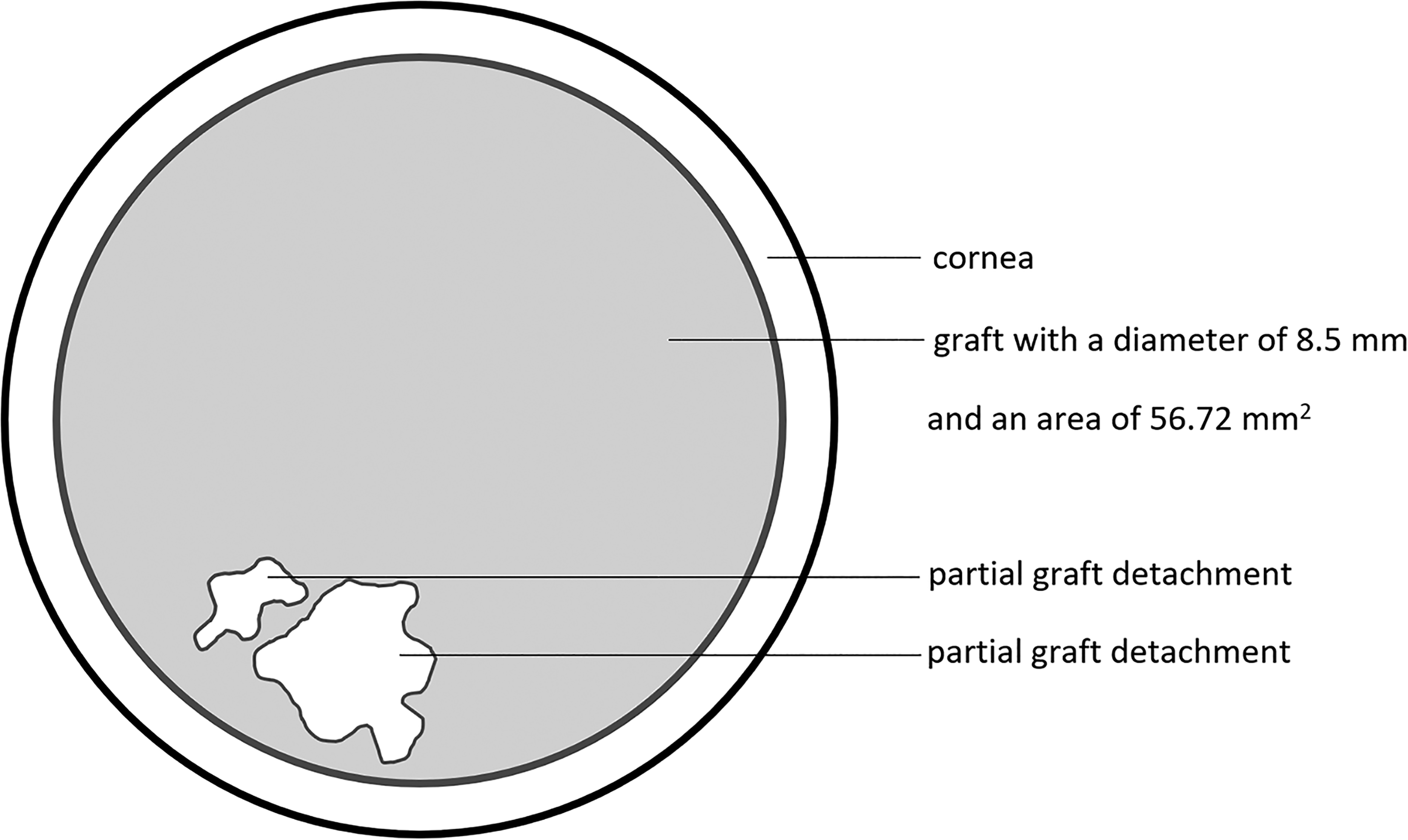
In order to analyze the outcome of rebubbling specifically concerning small detachments, subgroups were formed in terms of the maximum height and in terms of the detachment area in relation to graft area (Figures 1 and 2). The maximum height was divided into the categories „<500 µm“ (small dehiscence) and „>500 µm“ (big dehiscence). The detachment area was divided into the categories “<20% of graft area” (small dehiscence) and “>20% of graft area” (big dehiscence).

Schematic diagram of the cornea.
Schematic diagram of the cornea in cross-section. Detachment area results from the sum of all partial areas of graft detachment.
The study adhered to the principles of the declaration of Helsinki and has been approved by the University Hospital Leipzig's responsible ethics committee (approval number: 193/20-ek).
All surgical procedures were performed by two experienced surgeons (CG, JDU). On-site graft preparation was performed utilizing the “liquid bubble” technique, 11 DMEK was performed according to the technique published by Melles et al. 1 and modified by Kruse et al. 12 All grafts were round and had a diameter of 8.5 mm. In patients with concomitant cataract, phacoemulsification and posterior chamber lens implantation (triple DMEK) were performed within the same session.
Rebubbling was individually indicated for graft detachment diagnosed in OCT scans. After local anesthesia with Conjuncain® EDO® (Oxybuprocaine-hydrochloride, Dr. Gerhard Mann chem.pharm. Fabrik GmbH, Berlin, Germany) and disinfection, aqueous fluid was drained from the anterior chamber via one of the preexisting side port incisions. Then, a subtotal filling with 20% SF6 or air was done. Local therapy using antibiotics, myotics and steroids, present since DMEK surgery, was continued postoperatively and subsequently reduced. Local steroids were recommended to decrease in dose monthly until a maintenance dose once a day was adjusted.
Statistical analyses
Student's t-test was used to compare the control group with the rebubbling group in terms of the outcome measures. First, both groups with the total number of patients and next the subgroups defined by maximum height and area of graft detachment were tested. BCVA was assessed with decimal scale and converted to the logarithm of the minimum angle of resolution (logMAR). Because of skewed distribution data of CCT was logarithmic transformed, results are presented back-transformed.
Linear regression was used to point out the single effects of variables on the increase in BCVA.
SPSS® (IBM® SPSS Statistics, Version 26.0. IBM Corp., Armonk, NY) was used for all statistical analyses. p-values ≤0.05 were considered statistically significant and were adjusted according to Bonferroni regarding multiple testing.
Results
Statistical analyses included 111 eyes of 111 patients in total. Demographic data of the study collective is shown in Table 1, the reasons for surgery were Fuchs endothelial corneal dystrophy (n = 101), pseudophakic bullous keratopathy (n = 4) or other causes (n = 6). Eyes in the rebubbling group (n = 57) underwent one (n = 45), two (n = 10), three (n = 1) or four (n = 1) rebubbling procedures, eyes of the control group (n = 54) had no further intervention.
Demographic data of the study collective.
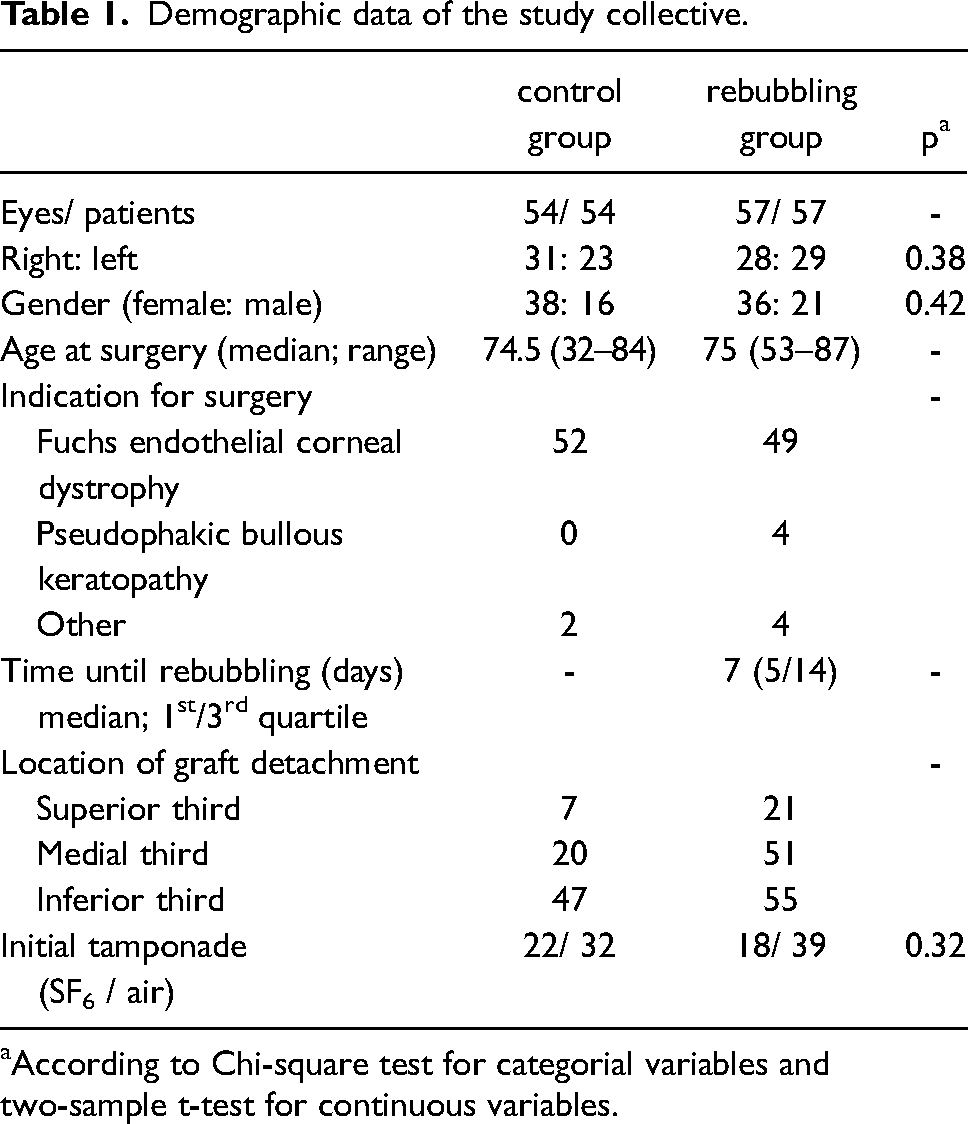
According to Chi-square test for categorial variables and two-sample t-test for continuous variables.
All data of the control group and the rebubbling group did not show differences of statistical significance concerning age, gender, initial tamponade and indication for surgery. The rebubbling group showed a worse BCVA and a higher CCT preoperatively than the control group, as seen in Table 2. Most graft detachments occurred in the inferior third, followed by the medial third of the cornea.
BCVA and CCT when comparing the control group and the rebubbling group (M ± SD).
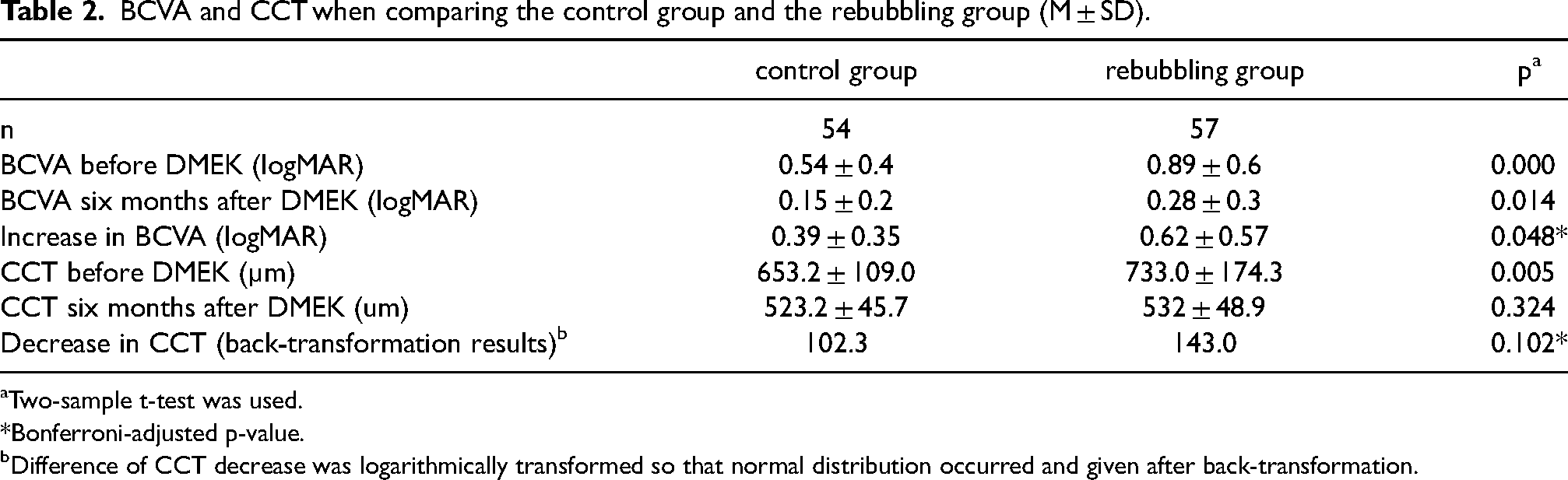
Two-sample t-test was used.
*Bonferroni-adjusted p-value.
Difference of CCT decrease was logarithmically transformed so that normal distribution occurred and given after back-transformation.
Mean increase in BCVA differed between the control group and the rebubbling group by 0.22 logMAR, p = 0.048.
The back-transformed decrease in CCT after logarithmic transformation showed a mean difference of 1.4 (100.1456 = 1.4) between both groups (95% Confidence Interval: 1.31−1.9), p = 0.102. That is, the mean decrease in CCT has a 40% higher value in the rebubbling group than in the control group.
Mean ECD did not differ significantly between the control group (1519 ± 408 cells/mm2, n = 39) and the rebubbling group (1675 ± 434 cells/mm2, n = 28) six months after surgery, p = 0.42.
As shown in Table 3, BCVA for eyes with graft detachments showing a maximum height of < 500 µm rose more in the rebubbling group than in the control group, p = .045. There was no significant difference in the increase of BCVA between the control group and the rebubbling group for eyes with graft detachments having less than 20% of the graft area.
Increase in BCVA (logMAR) in subgroups when comparing the control group and the rebubbling group (M ± SD).
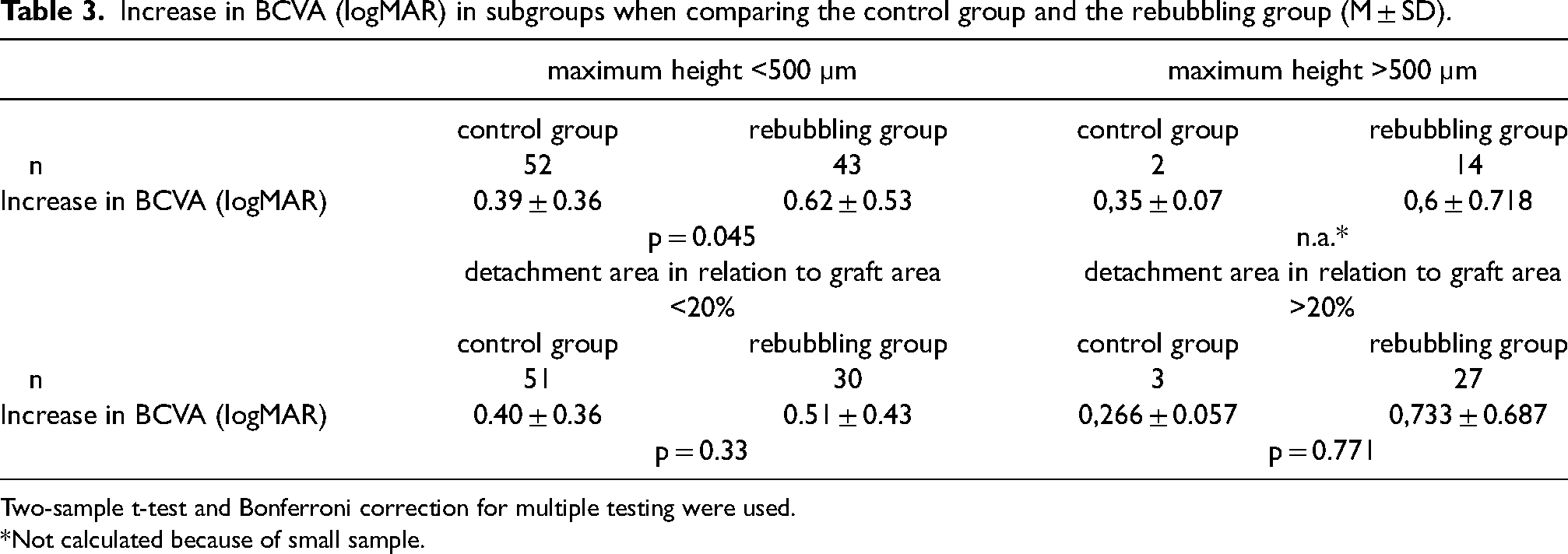
Two-sample t-test and Bonferroni correction for multiple testing were used.
*Not calculated because of small sample.
Linear regression
The linear regression model for the increase in BCVA containing the numeric variables “maximum height of graft detachment” and “detachment area proportional to graft area” and the categorical variable “rebubbling” achieved a power of 0.054 (corrected R2).
The maximum height of the detachment did not effect a change in BCVA, p = 0.08. If there was a rebubbling procedure, BCVA increased by 0.184 logMAR, p = 0.12.
Discussion
Graft detachment is a frequent complication after DMEK. Several biological or immunological causes have been reported, like stromal irregularities and residuals of the host Descemet membrane after incomplete descemetorhexis, 6 a lack of fibronectin and cytokeratin of the host, 13 overlap of the donor and host Descemet membrane14–16 or a low endothelial cell density. 17 Mechanical causes that have been identified as responsible factors are underfilling of gas in the anterior chamber 18 short-term dips of the intraocular pressure 19 and mechanical displacement of the graft.
Dehiscent grafts accompanied by stromal edema are clinically relevant as they might be uncomfortable for the patient and reduce visual acuity.
Our study evaluated the clinical outcome of rebubbling versus spontaneous graft adherence in eyes with detached DMEK grafts. Our results show no beneficial effect of rebubbling on the increase in visual acuity for small detached DMEK grafts, i.e., when graft detachment was less than 20% of the graft area. However, rebubbling does not decrease postoperative endothelial cell density. In our study population, the rebubbling group preoperatively showed a higher CCT. This means initial corneal decompensation due to the underlying disease was more pronounced in these eyes and later led to a necessity of rebubbling. Price et al. 20 reported that corneal decompensation that occurs with graft detachment is even more profound than that seen in primary diseases because of a barrier function of the endothelium and Descemet membrane. When comparing the rebubbling group to the control group in our study, we found a statistically similar decrease in CCT, so initially more edematous corneas cleared in the same way than those with less swelling.
Gundlach et al. 21 recently compared all eyes without rebubbling and eyes with one ore more interventions that underwent DMEK surgery. They found no significant difference in the increase of BCVA. Our results from the examination only of eyes with graft detachment showed a higher increase in BCVA after rebubbling than after spontaneous graft adherence. Statistical significance was narrowly reached. The preoperative BCVA was worse in the rebubbling group, and this group reached the higher increase in BCVA. Apparently, both eyes with advanced and less advanced disease reached a comparable final outcome. The amount of improvement was greater for more advanced disease.
In contrast to Gundlach et al., we excluded subsequent eyes of the same patient to avoid possible intraindividual effects on the clinical outcome. 8 Kim et al. 22 presented a higher probability that graft detachment occurs in the fellow eye if the graft of the first eye detached. If the first eye was rebubbled due to graft detachment, there is a higher rate of rebubbling in the subsequent eye. 8
Eyes that underwent repeated interventions were included in our rebubbling group as final graft adherence was an inclusion criterium. Siebelmann et al. 8 found that there was no influence of the overall number of rebubblings on BCVA. In this context, it is interesting to consider graft plasticity: Siebelmann et al. 7 postulate a dynamic process of detachment and reattachment of the graft instead of a steady state of graft attachment. As the numer of rebubblings increases, they noticed an increasing maximum extent of graft detachments while the number of detachments decreased. 8
Gerber-Hollbach et al. 23 described that right side-up positioned grafts showing areas of corneal clearing as well as areas of deep detachment possibly cannot achieve adherence spontaneously. The present study was to examine small detachments that in daily clinical practice are difficult to assess concerning their need of rebubbling. We therefore chose the limit of 20% of the transplant's area and analyzed dehiscence below this threshold.
Whether there is a negative impact of rebubbling on endothelial cell loss has already been examined by different groups. More endothelial cell loss was found in eyes with one rebubbling compared to eyes with uneventful DMEK surgery. 24 Regarding the influence of the number of rebubblings there are varying study results. On the one hand, no influence of the overall number of rebubblings on ECD or ECD loss was found after one year. 8 On the other hand, Feng et al. 25 found that median endothelial cell loss was higher in eyes that had two or more air reinjections compared to eyes with none or only one reinjection. The authors assumed that grafts with lower ECD at the beginning were more likely to detach due to less innate endothelial function and therefore required more air. Hayashi et al. 26 discussed whether rebubbling procedures itself cause endothelial cell loss or whether endothelial cells with low pump function cause graft detachment necessitating rebubbling. They found a strong relationship between rebubbling and ECD loss. In our study, postoperative ECD did not differ between eyes that underwent rebubbling and eyes that achieved adherence spontaneously. It was, however, not possible to define ECD loss in our study collective.
In other studies, the characteristic of the detachment's size has been described, differently categorized and taken as one criterion for the indication of rebubbling. Its classification varies from just diameter measuring 8 to divisions of clock hours21,27 to more or less than 1/3 of the graft's area. 23 In this study, we formed the rebubbling and the control group regardless of the detachment's size, i.e., indication for rebubbling being not dependent on the area or maximum height of dehiscence. Thus, an advantage of this study is to compare detachments of the same characteristic, like detachment's size, with or without intervention. On the other hand, there might be some selection bias because the surgeon's experience or estimation about how to achieve best visual recovery could have influenced the indication for rebubbling.
We did not find a difference in the initial tamponade used between our groups. As the use of SF6 instead of air is discussed as an associated factor of less graft detachment,18,28,29 we can exclude possible bias due to the initial tamponade.
Study limitations include the retrospective design as it does not allow true randomization of the two groups. Measurement uncertainties or missing identification of graft detachment on OCT scans may have occurred due to the investigator's assessment. Therefore, Heslinga et al. 30 already described the use of automatic location and quantification of graft detachments. First deep learning-based methods on the basis of neuronal networks have also been presented to possibly guide the decision making whether to rebubble or not.31,32 Detection of flat peripheral detachments thereby is still insufficient so manual detection with OCT enabled us to find these while not overlooking detachments compared to clinical slit-lamp examination. 33
To conclude, this study is the first to investigate the impact of rebubbling for small dehiscent grafts after DMEK. We could not show evidence for benefits of a rebubbling procedure.
Though, further examination regarding the detachment's maximum height could be interesting as it is a characteristic easily to identify in daily clinical practice and might help for decision making whether or not to perform a rebubbling.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.