
Abstract
Purpose
To report the diagnosis, treatment and follow-up of a case of bilateral acute iris transillumination (BAIT) developed after COVID-19 pneumonia.
Method
Case report.
Case
A 66-year-old male patient with COVID-19 pneumonia received systemic treatments of favipiravir, prednisolone, moxifloxacin and piperacillin-tazobactam during hospitalization. The patient applied to our clinic with the complaint of blurred vision 20 days after the diagnosis of COVID-19. The best corrected visual acuity (BCVA) was 0.3 in the right eye and 0.5 in the left eye. In the anterior segment examination; ciliary injection, intense pigment dispersion in the anterior chamber, pigment deposits on the lens and iris, 2–3 + cells in the anterior chamber, posterior synechia, and 360 degrees diffuse iris transillumination were observed in both eyes. The pupillary response to light was weak. Bilateral fundus examination were normal. In the anterior chamber sample; HSV, VZV, CMV and Toxoplasma PCR were negative. Bilateral acute iris transillumination (BAIT) diagnosed in the patient and topical 0.1% dexamethasone and topical 1% cyclopentolate were started. In the follow-up, visual acuity increased 1.0 in both eyes, there were no cells in the anterior chamber, and the pigment dispersion was still continuing despite a decrease.
Conclusion
BAIT, which can usually be seen after upper respiratory tract infections, can also be seen after covid 19 pneumonia and be kept in mind as a possible eye involvement in patients with COVID-19 infection.
Introduction
Bilateral acute iris transillumination syndrome (BAIT) is a partially new syndrome characterized by bilateral iris transillumination, iris sphincter paralysis and anterior chamber pigment dispersion. It was first defined by Bringas Calvo et al. in 2004. 1 In 2011, Tugal-Tutkun et al. described the clinical manifestations of the syndrome with a series of 26 cases. 2
The etiopathogenesis of the disease remains unclear. Most patients have recent upper respiratory tract infection (URTI) symptoms or a history of systemic-intracameral antibiotic use (especially moxifloxacin). Therefore, a history of viral URTI and systemic antibiotics are seen as triggering factors in the etiology.2–4
BAIT is usually in middle-aged women; presents with hyperemia, photophobia, pain and blurred vision. On examination; bilateral and often diffuse iris transillumination is seen. Pigment dispersion is observed in the anterior chamber, which may cause high laser flare photometry values. These pigments may accumulate in the lens or corneal endothelium. It is necessary to distinguish them from keratic precipitates and inflammatory cells. The typical feature of the syndrome with iris transillumination is sphincter paralysis; Patients have weak or absent pupillary response to light. Increased intraocular pressure (IOP) is often seen due to pigment deposition in the trabecular meshwork. Posterior segment involvement is not expected.
Herein, we report a case with BAIT occured after severe acute respiratory syndrome - coronavirus-2 (SARS-CoV-2,COVID-19) pneumonia.
Case report
A 66-year-old male patient was hospitalized for COVID-19 pneumonia one month ago. During hospitalization, the patient was consulted to some units because of the lesions around the left eye and accompanying complaints of redness, photophobia and pain in the both eyes. The lesions were diagnosed as shingles by the dermatology unit and oral valacyclovir treatment was started. Although the patient did not have corneal involvement, ganciclovir gel was started because of conjunctival hyperemia. The patient also received systemic treatments of oral favipiravir, intravenous prednisolone, moxifloxacin, and piperacillin-tazobactam during hospitalization.
Blurred vision was added to the patient's complaints at the first examination after discharge. Best-corrected visual acuity (BCVA) was 0.3 on the right and 0.5 on the left. IOP was 12 mmHG on the right and 13 mmHG on the left. In the anterior segment examination; 360 degrees diffuse iris transillumination was observed in both eyes (Figure 1(a) and (b)). Intense pigment dispersion in the anterior chamber, pigment deposits on the lens and iris (Figure 1(c) and (d)) and posterior synechia (Figure 1(E) and (F)) were observed bilaterally. Laser flare photometry could not performed due to intense pigment dispersion. Bilateral pupillary response to light was weak. Posterior segment examination and optical coherence tomography (OCT) were normal.
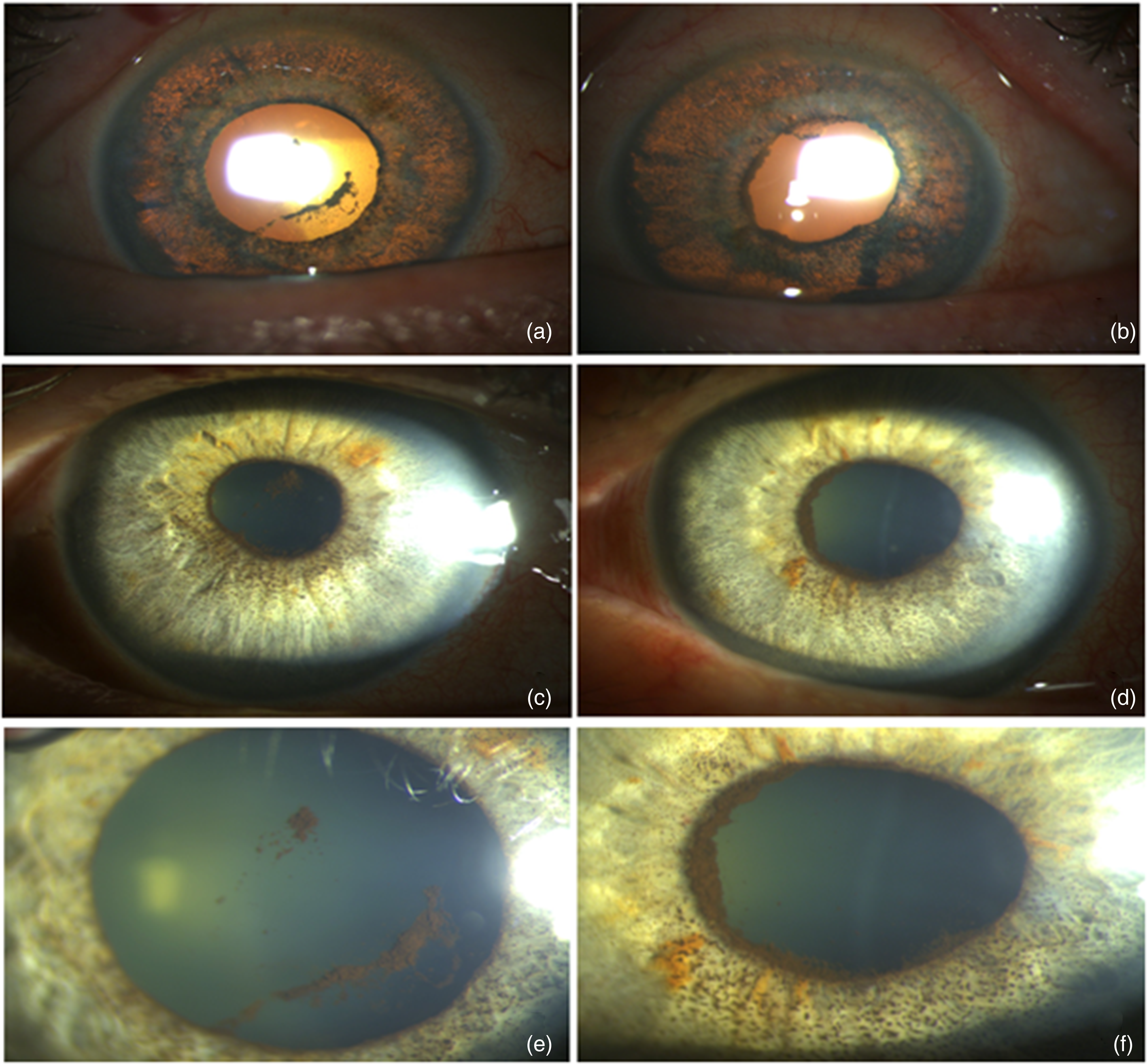
(a) and (b) bilateral diffuse iris transillumination is observed. (c) and (d) Significant pigment deposition on the iris. (e) and (f) Posterior synechiae with broad base and thick iris layer.
To rule out herpetic uveitis, anterior chamber paracentesis was performed to the right eye and HSV, VZV, CMV and Toxoplasma PCR were negative. With the diagnosis of BAIT, the patient was started topical % 0.1 dexamethasone drops every hour daily and tapered weekly and topical % 1 cyclopentolate drops 3 times a day. At the follow-up one week later, IOP increased to 30 mm Hg in both eyes. Topical timolol/dorzolamide fixed combination(twice a day) and topical brimonidine(twice a day) were added to the treatment. At the follow-up 20 days later, BCVA was 1.0 in both eyes. IOP was 14 mmHG on both eyes. Although anterior chamber pigment dispersion was reduced, it still persisted (Figure 2). It was planned to reduce and discontinue topical steroid therapy.
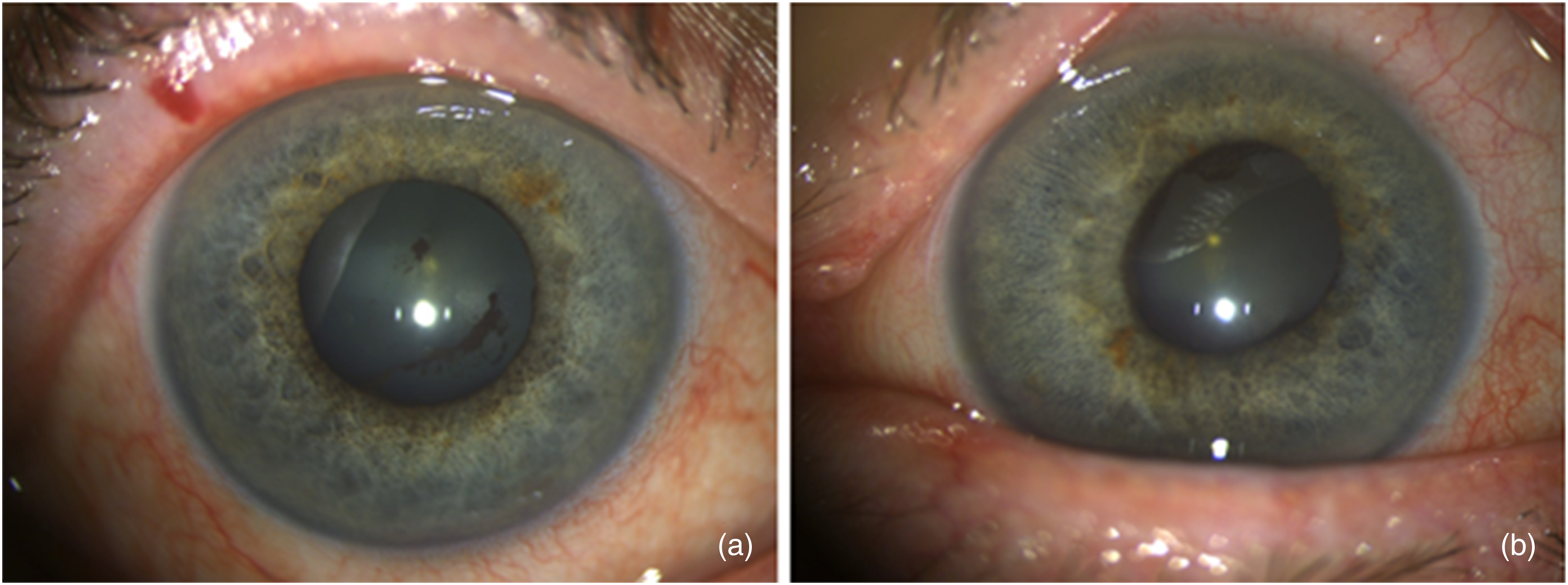
Pigment dispersion in the anterior chamber and on the iris is reduced but still persists.
Discussion
Various ocular manifestations of COVID-19 have been reported including conjunctivitis, anterior uveitis and optic neuritis.5–7 The most common ocular symptoms in COVID-19 patients were dry eye or foreign body sensation, redness, tearing, itching, eye pain, and discharge. 8 Although conjunctivitis is most common ocular disease in COVID-19 patients, anterior uveitis should be kept in mind with these findings. In this case report; we described a patient presented with redness, photophobia and blurry vision after COVID-19 pneumonia and was diagnosed with BAIT. The symptoms regressed with topical steroid treatment and visual acuity was fully recovered. It was observed that the pigment dispersion in the anterior chamber decreased but persisted.
To the best of our knowledge, this case, together with the case reported by Yağcı et al., 9 is one of the first cases of BAIT occurred after COVID-19. In the report of Yağcı et al.; the patient presented with complaints of blurred vision, pain and redness, similar to our case, 2 weeks after discharge. Pigment deposition in the bilateral corneal endothelium, pigment dispersion in the anterior chamber, iris transillumination and a poorly responsive pupil were observed in the patient. The patient's routine blood tests and anterior chamber sample PCR examination were negative. Pigment dispersion regressed with topical steroid but persisted, similar to our case.
The etiopathogenesis of BAIT is not fully known. The preferred idea is that an ocular inflammatory response secondary to viral infections, especially involving the upper respiratory tract.2,3 This case shows that BAIT syndrome observed after viral infections can also be observed after COVID-19 infection.
In the differential diagnosis, bilateral acute iris depigmentation (BADI) syndrome can be considered as the mild manifestation of BAIT. Although there is a common etiology, there are two most important distinguishing features; Firstly, pupillary reactions are not affected in BADI. Secondly, in BADI, granular geographic depigmentation with distinct borders is observed in the iris stroma, but this depigmentation does not cause transillumination in the iris. Increased IOP can occur in either condition. In another disease, pigment dispersion syndrome, the transillumination is radial shape and is located in the midperiphery of the iris. Pupillary reactions are not affected. Pseudo-exfoliation syndrome, Fuchs uveitis, herpetic anterior uveitis should also be considered in the differential diagnosis.
In conclusion, BAIT may occur after COVID-19 infection and should be kept in mind in the examination of patients with redness, photophobia or blurry vision accompanying COVID-19.
Footnotes
Informed consent
Permission was obtained from the patient to publish the case without using his/her name and private information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.