
Abstract
Keywords
Introduction
Psychosocial stressors may activate physiological stress responses and lead to health-related issues, (Epel & Lithgow, 2014). The importance of social relationships is well-documented, with strong social connections reducing morbidity and mortality risk by 50%, demonstrating protective effects comparable to smoking cessation (Holt-Lunstad et al., 2010). Nonetheless, the quality of social relationships may undermine their health benefits as chronic stress from negative and conflictual social interactions is associated with poor self-rated health, stress-related diseases, as well as accelerated cellular aging indicated by shortened telomere length (TL) (Uchino et al., 2012a; Umberson & Karas Montez, 2010).
The biological mechanism by which psychosocial stressors affect bodily systems and cellular attrition involves ongoing activation of the initial stress hormone cascade: epinephrine, norepinephrine and cortisol via the activation of the sympathetic adrenal medullary (SAM) axis and the hypothalamic pituitary adrenal (HPA) axis (Epel & Lithgow, 2014). Overtime, recurrent activation of these systems, may lead to impairment of the metabolic, cardiovascular, immune and neuroendocrine systems (Juster et al., 2010; McEwen, 2008; Tomiyama et al., 2012), as well as initiate cellular damage (Epel & Lithgow, 2014). Studies demonstrate that a repeated high level of cortisol secreted in response to psychosocial stress may lead to shortened telomeres, implying a link between glucocorticoid stress response and telomere shortening (Gotlib et al., 2015; Tomiyama et al., 2012).
The postpartum year is a vulnerable period when mothers face increased risk for physical and emotional health problems (Hsu & Wickrama, 2018). Among postpartum women, research demonstrates that higher stress levels increase risk of depressive and anxiety symptoms, while stronger perceived emotional and social support reduce this risk (Schwab-Reese et al., 2017). However, the quality and source of social support matter considerably for maternal health outcomes. While inadequate support increases risk for postpartum depression and anxiety (Hetherington et al., 2018), marital satisfaction serves as a protective factor, with higher marital satisfaction associated with significantly lower postpartum stress levels (Wang et al., 2023). A comprehensive meta-analysis of cohort studies further confirmed that marital quality is consistently associated with lower rates of postpartum major depressive disorder (Wei et al., 2025). Conversely, social negativity, defined as the actual presence of unpleasant behaviors rather than the absence of social support (Brooks & Schetter, 2011a) has particularly detrimental effects. Postpartum women experiencing negative social interactions show slower recovery, increased physical pain, and elevated depression risk (Ali Saleh, 2017; Saurel-Cubizolles, Romito, Lelong, & Ancel, 2000), while those with sustained stress during the first six months postpartum demonstrate increased vulnerability to subsequent health problems (Hsu & Wickrama, 2018). Social negativity is mostly assessed as conflict, criticism, insensitivity, and interference (Brooks & Schetter, 2011a) and may have stronger effects on health than social support, with women being more sensitive to relational distresses than men, as evidenced by inflammatory marker responses to spousal support or strain (Brooks & Schetter, 2011a; Kiecolt-Glaser et al., 2010). Recent research confirms this negativity effect, showing that negative ties are more cognitively salient and physiologically impactful than positive relationships (Offer, 2025).
Telomeres, the protective “caps” at the end of chromosomes, serve as biomarkers for cellular aging and prevent chromosomal deterioration (Barrett et al., 2015). Telomere shortening is related to aging, disease and mortality from psychological and physiological disorders (Mathur et al., 2016). Physiologically, shorter telomeres are associated with increased cardiovascular risk (Haycock et al., 2014), type 2 diabetes (Willeit et al., 2014) and some types of cancer (Wentzensen et al., 2011) and psychologically, various psychosocial stressors have been linked to telomere attrition (Oliveira et al., 2016), of these, relationship styles and social interactions, have been an area of growing research (Barger & Cribbet, 2016; Carroll et al., 2013; Lincoln et al., 2017; Mathur et al., 2016; Oliveira et al., 2016; Uchino et al., 2012b, 2015; Willis et al., 2018) demonstrating their ability to affect one’s health and TL both positively and negatively (Newsom et al., 2022; Uchino, 2013; Uchino et al., 2012b).
Greater social support is associated with longer TL among older adults (Carroll et al., 2013), nonetheless, the source and quality of social support received and perceived is important as individuals, who experience higher negative interactions have shorter telomeres and this is primarily evident in women (Uchino et al., 2012b).
Research on social relationships and TL postpartum is sparse, currently, only one study focused on mother’s TL during the perinatal and postnatal period from early pregnancy to 7-11 weeks postpartum (Mitchell et al., 2018). Findings revealed a significant positive association only with mothers’ perceived family support and TL, but not with perceived social support from friends and “significant others” (Mitchell et al., 2018). Adding to that, the COVID-19 pandemic, that emerged during this study disrupted social networks and support particularly affecting postpartum mothers who reported decreased social support and increased distress (Zhou et al., 2021), This context is relevant as social stressors may have pronounced effects on maternal health and cellular aging during postpartum recovery.
The postpartum period is unique with regards to the aging processes as previous studies noted physiological and cellular similarities between pregnancy and aging, as both induce oxidative stress, and inflammation (Giller et al., 2020) that are associated with cellular damage and shortened TL (Epel & Lithgow, 2014). Within the immediate postpartum period, remarkable rejuvenation occurs, and mothers undergo substantial recovery at both physiological and cellular levels (Giller et al., 2020). However, during the postpartum period, women often experience heightened stress due to sleep deprivation, caregiving demands, and role adjustments, which may contribute to accelerated biological aging especially when support networks are insufficient (Allen & Finkelstein, 2014).
The aim of this study is to examine the effect of positive and negative social interactions on TL among women in Israel, measured one month postpartum and one year thereafter. We hypothesized that: (1) mothers experiencing more negative social interactions, less marital satisfaction and less positive social interactions would demonstrate more telomere attrition over the one-year follow up; (2) perceived stress would mediate the relationship between social interactions (negative interactions, spouse support, and positive social support) and telomere length changes; and (3) social support would moderate the association between stress and telomere dynamics.
Material and Methods
This study recruited 128 first-time postpartum mothers from Mother and Child Health Centers and Bnei Zion Hospital, Haifa, Israel. This study was approved by the Israeli Ministry of Health’s Ethics Committee (MOH-118-2019), Bnei Zion Ethics Committee (0113-20-BNZ) as well as Haifa University’s Ethics Committee (346/19) Data collection occurred from November 2020 to June 2022.
The sample size determination utilized TL data from a previous related study (Steptoe et al., 2016). We determined that a sample size of 25 participants is required to attain a 90% power level at a significance level of 0.05. We increased this figure by 30% to accommodate potential dropout bias and further multiplied it by a factor of two to facilitate subgroup analyses. The planned subgroup analyses included comparisons between ethnic groups (Arab vs Jewish) and socioeconomic status levels (below average, average, and above average income), though the final sample composition did not allow for meaningful comparisons between these groups. Eventually, we settled on a sample size of 120 participants.
Inclusion criteria included healthy postpartum married women with no underlying acute or chronic disease, aged 20-35, gravida 1, para 1, who had uncomplicated pregnancies and labor via spontaneous vaginal delivery of a healthy mature newborn. We objectively assessed participants’ health using medical records and clinical evaluations, with initial interviews conducted by nurses followed by verification by the principal researcher. Exclusion criteria included multifetal gestation and any current use of medication.
Data collection included questionnaires and dried blood spots (DBS) to measure Leukocyte Telomere Length (LTL). DBS were collected via a nurse or independently by mothers, via self-prick, assisted by a video call to ensure testing accuracy, within one day to two weeks after birth and one year (+/− one week) after first collection date. Questionnaires were submitted electronically to all first-time mothers one month postpartum and one-year postpartum. One-month postpartum, mothers self-reported demographic data including age, ethnicity (Arab or Jewish), educational attainment (academic/non-academic), annual household income (below, equal, or above average of net household income of 15,427 New Israeli Shekels), weight, and height. In addition, they responded to questionnaires assessing psychological and physical health related information such as self-reported perceived stress, perceived Covid19 threat, physical activity (Short International Physical Activity Questionnaire- IPAQ), depressive symptoms (Edinburgh Postpartum Depression Scale-EPDS), breastfeeding practices (full or partial breastfeeding), and a questionnaire assessing social interactions including positive and negative social interactions as well as marital satisfaction. During timepoint 1, overall, 128 mothers submitted DBS and the response rate to questionnaires at time 1 was 95%. At timepoint 2 of data collection, mothers were contacted via phone for follow up, a total of 108 mothers agreed to submit DBS for LTL measurement, of these, 103 mothers completed their electronic questionnaires resulting in an 80% response rate. The primary reason for leaving the study was refusal and a secondary reason was change of residence. At timepoint 2, questionnaires repeated questions from timepoint 1 and included reported weight and height, physical activity, perceived stress, perceived Covid19 threat, depressive symptoms, and breastfeeding practices as well as mothers’ pregnancy status. Questions on demographics and social interactions were not repeated. Mothers who either did not provide a DBS sample at timepoint 2 or did not complete an electronic questionnaire at timepoint 1 or 2 were excluded from data analysis. Complete case analysis was performed, including only participants with complete telomere and questionnaire data at both timepoints (n = 103). Non respondents at timepoint 2, did not differ significantly from mothers who agreed to fully participate, in age, education, and income.
Social Interaction Measurements
Social Support: Positive social support was measured using 10 items from Sherbourne and Stewart’s survey, assessing emotional and instrumental support on a 5-point scale (1 = never, 5 = very often), with higher scores indicating more support (Cronbach’s α = 0.884) (Sherbourne & Stewart, 1991).
Negative social interactions: Negative social interactions were measured using a 19-item questionnaire based on Brooks and Dunkel Schetter’s model (Brooks & Schetter, 2011). Adapted from validated questionnaires including Test of negative social exchange (TENSE) (Ruehlman & Karoly, 1991) and Quality of Relationship Inventory (QRI) (Pierce et al., 1991) The scale assesses conflicts, insensitivity, and interference on a 5-point scale (1 = not at all, 5 = extremely), with higher scores indicating more negative interactions (Cronbach’s α = 0.951).
Marital satisfaction Scale: Marital satisfaction was assessed using an 8-item questionnaire adapted from Braiker and Kelley (1979), examining closeness, communication, and conflicts on a 5-point scale (1 = not at all, 5 = very much), with higher scores indicating greater marital satisfaction (Cronbach’s α = 0.827).
Covariates
Perceived Stress Scale: Perceived stress was assessed using the Hebrew version of the 14-item Perceived Stress Scale (PSS) (Cohen et al., 1983), assessing stress frequency in the past month on a 5-point scale (1 = never, 5 = very often), with higher scores indicating greater perceived stress (Cronbach’s α = 0.88).
Perceived Covid19 threat: Perceived COVID-19 threat was assessed using a 9-item of the Health Belief Model scale adapted for COVID-19 (Erkin & Özsoy, 2012) measured on a 5-point scale (1 = strongly disagree, 5 = strongly agree), with higher scores indicating greater perceived threat (Cronbach’s α = 0.74).
Covid diagnosis: Mothers were asked to self-report any positive COVID-19 diagnosis confirmed by testing during the study’s follow-up year.
Postpartum depressive symptoms: Postpartum depressive symptoms were assessed using the Hebrew version of the 10-item Edinburgh Postnatal Depression Scale (EPDS) (Cox et al., 1987). With a 4-point response scale, using a cut-off of ≥10 for postpartum depression risk (Cronbach’s α = 0.88).
Lifestyle health behaviors: Pre-pregnancy and postpartum body mass index BMI (Kg/m2) were assessed by mother’s report of her height and weight and smoking status was assessed via mothers’ self-report, indicating a current smoking or non-smoking status. Exercise was assessed via the short form of the International Physical Activity Questionnaire (IPAQ-SF) which was developed for cross-national monitoring of physical activity. The IPAQ-SF is validated in the general population and in pregnant women (Sanda et al., 2017), and includes measures of the frequency, intensity and time of physical activity. We used the self-administered version, in which women were asked to recall physical activity performed on a usual week during pregnancy during data collection at timepoint 1, and at timepoint 2 during a usual week postpartum.
Telomere Length Measurement
DBS were stored at −80°C within 24 hours of collection and batch-extracted in Oct 2021 (128 samples) and July 2022 (103 samples). Relative TL was measured by quantitative polymerase chain reaction (qPCR) as described previously in the literature (Kang et al., 2021) (detailed in Supplementary material), expressed as the ratio of telomere to single-copy gene abundance (T/S ratio). Twenty-eight samples were re-extracted to adjust for batch differences. The inter-assay coefficient of variation was 2.0 ± 1.4% and the interclass correlation (ICC) was 0.804 (CI 0.624-0.900).
Statistical Analyses
Statistical analyses were conducted with SPSS V25. Descriptive analyses characterized participants’ socio-demographic, health, and social interaction variables. Delta LTL was calculated as the difference between timepoint 2 (M = 1.60, SD = 0.22) and timepoint 1 (M = 1.52, SD = 0.20). A paired t-test demonstrated significant increase in LTL (M = .08, SD = 0.134, t (6.057), p < .001). Delta TL was divided into tertiles: upper (most lengthening), middle (modest lengthening), and lower (no change/shortening). Associations were assessed using independent t-tests, Pearson/Spearman correlations, and Chi-square tests. Mediation and moderation analyses used the PROCESS macro (Hayes & Rockwood, 2017). Multiple linear regression was initially conducted with delta TL as a continuous outcome. Due to non-linear patterns and non-normal distribution of key variables, we proceeded with a hierarchical logistic regression. Hierarchical logistic regression predicted upper tertile delta TL membership using four blocks: (1) demographics (age, baseline TL, income), (2) behavioral factors (BMI, physical activity, COVID-19 diagnosis), (3) psychological variables (depressive symptoms, perceived stress, COVID-19 threat), and (4) social interactions. Due to collinearity, three separate models tested negative interactions, marital satisfaction, and positive interactions. Social variables were dichotomized: upper tertile (33%) vs. lower tertiles (66%) for negative interactions; upper tertiles (66%) vs. lowest tertile (33%) for marital satisfaction and positive interactions. Significance was set at p < .05. The Benjamini-Hochberg procedure controlled for multiple comparisons with false discovery rate of 0.05.
This study was conducted and reported in accordance with STROBE guidelines for cohort studies.
Results
Demographics, Lifestyle, Health, and Telomere Variables, Mean, % and Number (N = 103)
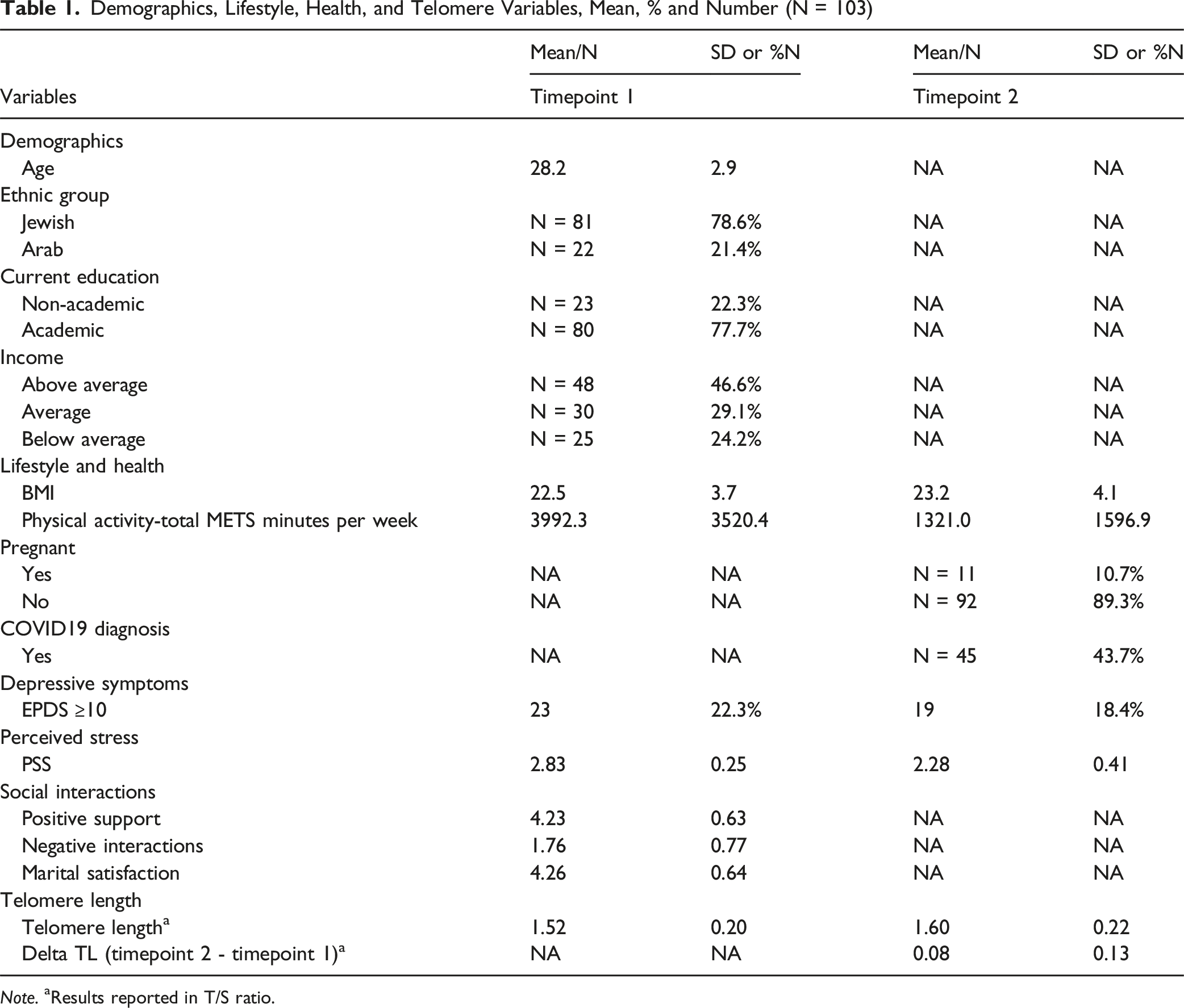
Note. aResults reported in T/S ratio.
Differences Between No Change/Shortened TL and Lengthened Telomere Groups – (Independent Two Tailed Sample T Test)
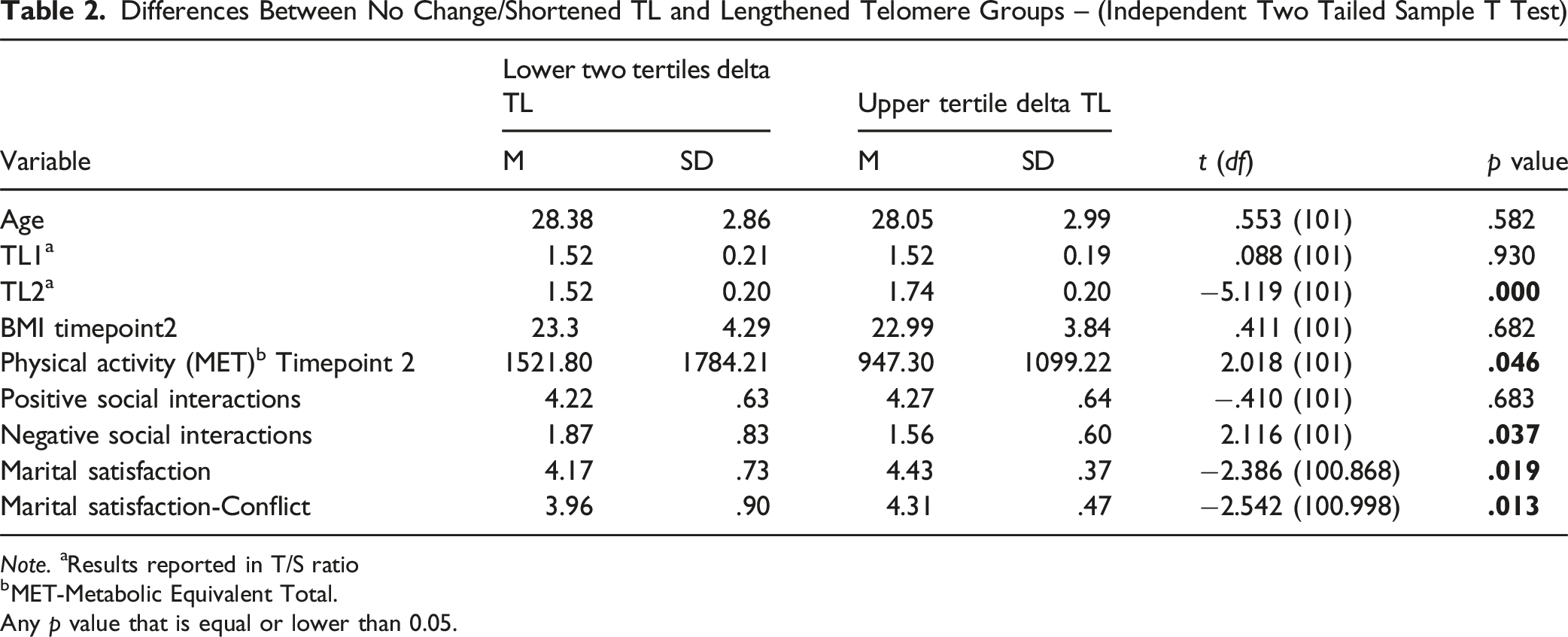
Note. aResults reported in T/S ratio
bMET-Metabolic Equivalent Total.
Any p value that is equal or lower than 0.05.
Linear Regression Analyses
To examine associations between social interactions and Delta LTL we initially examined the relationship between social interactions and delta TL using multiple linear regression. These analyses, with delta TL as a continuous variable, yielded non-significant associations for all of our primary variables of interest: negative social interactions (β = −0.115, SE = 0.019, 95% CI [-0.058, 0.018], p = 0.294), positive social interactions (β = 0.010, SE = 0.022, 95% CI [-0.042, 0.046], p = 0.923), and marital satisfaction (β = 0.085, SE = 0.022, 95% CI [-0.025, 0.061], p = 0.413) after controlling for demographic (Age, TL timepoint1, Income), behavioral (BMI, physical activity, Covid19 diagnosis), and psychological covariates (perceived stress, depressive symptoms, and Covid19 related threat).
Hierarchical Logistic Regression Analyses
Odds Ratios From Hierarchical Logistic Regression Models Predicting Belonging to the Upper Tertile of Delta LTL by Covariates and Social Interactions
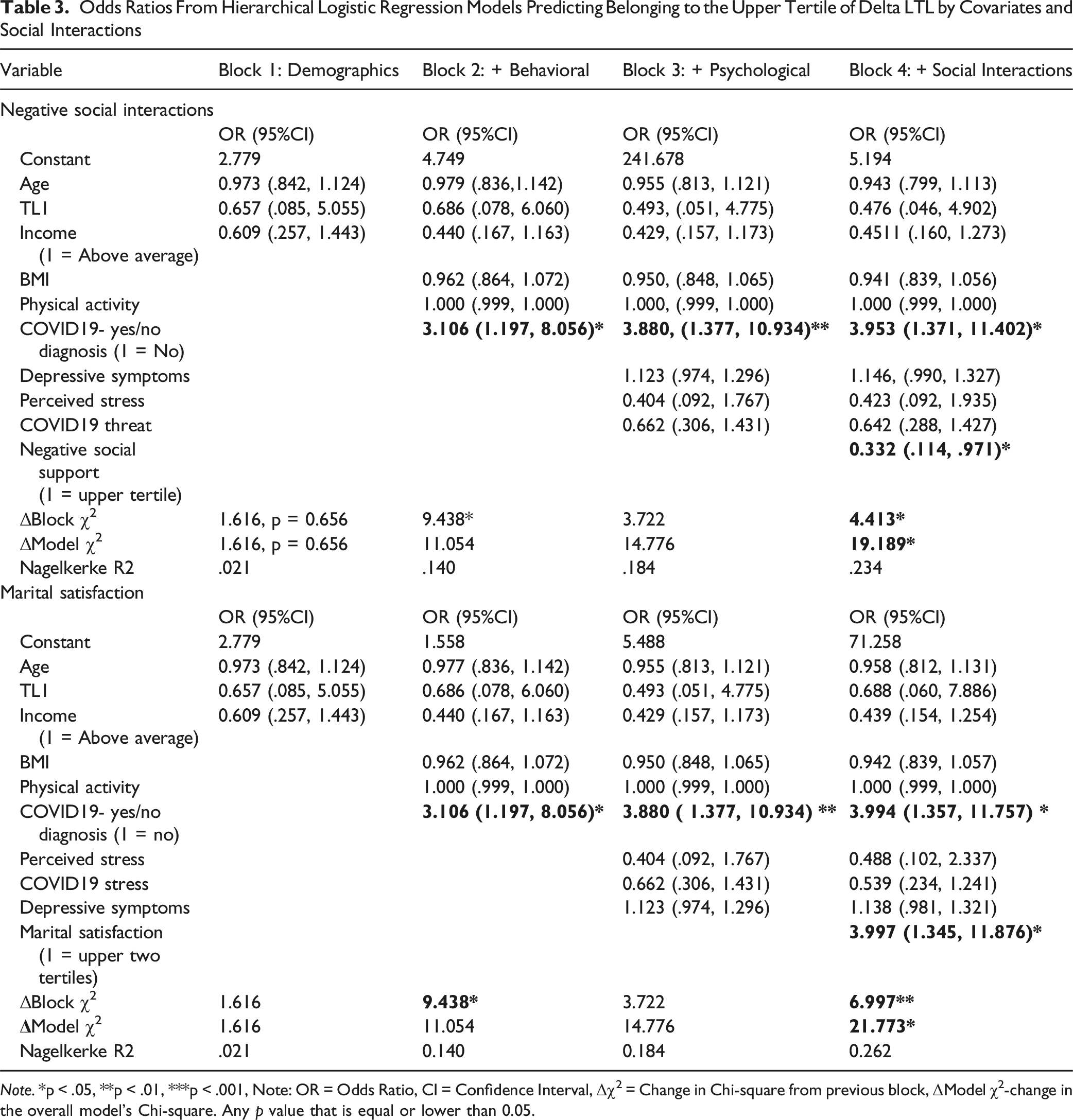
Note. *p < .05, **p < .01, ***p < .001, Note: OR = Odds Ratio, CI = Confidence Interval, Δχ2 = Change in Chi-square from previous block, ΔModel χ2-change in the overall model’s Chi-square. Any p value that is equal or lower than 0.05.
Marital Satisfaction Model
In the hierarchical regression analysis assessing the effect of marital satisfaction on change in TL, the final model explained 26.2% of the variance (Nagelkerke R2 = 0.262, p = .016). Two significant predictors emerged: COVID-19 status (OR = 3.994, 95% CI [1.357, 11.757], p = .012) and marital satisfaction (OR = 3.997, 95% CI [1.345, 11.876], p = .013). Notably, mothers reporting higher marital satisfaction (upper two tertiles) had four times higher odds of showing substantial telomere lengthening (being in the upper tertile delta TL group).
Negative Social Interactions Model
In the hierarchical regression analysis assessing the effect of negative social interactions on change in TL, prior to multiple comparison adjustment, the model showed incremental improvements with each block. The final model, which explained 23.4% of the variance in TL change (Nagelkerke R2 = 0.234, p = .038), revealed two significant predictors: Covid19 status (OR = 3.953, 95% CI [1.377, 10.934], p = .011) and negative social interactions (OR = 0.332, 95% CI [0.114, 0.971], p = .044). Notably, mothers reporting high levels of negative social interactions (upper tertile) had three times lower odds of showing substantial telomere lengthening (being in the upper tertile delta TL group). However, this association became non-significant after Benjamini-Hochberg adjustment for multiple comparisons (BH-adjusted p = .066), as detailed in subsequent analyses.
Positive Social Interactions Model
The hierarchical regression analysis assessing the effect of positive social interactions on change in TL yielded non-significant results. Positive social interactions were not significantly associated with TL change (OR = 1.285, 95% CI [0.607, 2.718], p = 0.512), resulting in a non-significant overall model (p = .125) that explained 18.9% of the variance in TL change.
Exploratory Threshold Analyses
In additional exploratory analyses, we examined the relationship between delta TL and social interactions using different threshold values to dichotomize delta TL. For negative social interactions, the significant association observed in our primary analysis (at the 66th percentile) remained significant when testing values up to the 71st percentile but became non-significant at higher thresholds. This pattern could reflect various underlying phenomena: it might suggest a potential threshold effect, reflect limitations in statistical power due to decreasing sample sizes in the comparison groups, or simply indicate that the relationship does not meaningfully extend to more extreme values. In contrast, the relationship between delta TL and marriage satisfaction demonstrated stability across a wider range of threshold values, maintaining significance even at the 80th percentile (Delta TL = 0.193, OR = 8.309, 95% CI [1.661, 41.554], p = .010) and above. While noteworthy, these exploratory findings should be interpreted with caution, as the selection of threshold values was data-driven rather than theoretically predetermined.
COVID-19 diagnosis remained a significant predictor across all blocks in the multiple hierarchical regression analyses, with individuals who were not diagnosed with COVID-19 being nearly four times more likely to experience telomere lengthening. In contrast, demographic (age, TL at timepoint 1, income), behavioral (BMI, physical activity), and psychological variables (perceived stress, COVID-19 related threat, depressive symptoms) did not significantly predict TL changes in any of the models.
We ran an additional hierarchical logistic regression analyses that excluded all pregnant mothers at timepoint 2, and results remained consistent (OR = 0.292, 95% CI [0.096, 0.887], p = .03, OR = 4.947, 95% CI [1.569, 15.596], p = .006, OR = 3.504, 95% CI [1.206, 10.180], p = .02) for negative interactions, marital satisfaction, and COVID-19, respectively. Except for positive interactions which remained non-significant.
To address concerns about multiple comparisons, we applied the Benjamini-Hochberg (BH) procedure to our primary analyses. After adjustment, marital satisfaction remained significantly associated with the outcome (unadjusted p = .013, BH-adjusted p = .039). The association for negative interactions became non-significant after adjustment (unadjusted p = .044, BH-adjusted p = .066), while positive interactions remained non-significant (unadjusted p = .512, BH-adjusted p = .512).
In sum, after adjusting for multiple comparisons using the Benjamini-Hochberg procedure, marital satisfaction remained significantly associated with upper tertile delta LTL membership, while negative social interactions, which were initially significant, did not reach statistical significance after adjustment. Additionally, a negative Covid19 diagnosis demonstrated a 4-fold increase in the odds of belonging to the upper tertile of delta LTL.
Discussion
The present study examined the effect of positive and negative social interactions and marital satisfaction on LTL in a sample of 103 postpartum healthy and married women. Our results demonstrated an overall significant increase in LTL from timepoint 1 to timepoint 2, with marital satisfaction emerging as the most robust correlate of changes in LTL, maintaining significance after correction for multiple comparisons, while negative social interactions showed only initial associations.
Social Relationships and Telomere Lengthening
Results from the hierarchical regression models reveal that marital satisfaction emerged as the most robust correlate of changes in LTL, maintaining significance even after correction for multiple comparisons and demonstrating a four-fold increase in odds of substantial telomere lengthening for mothers with higher marital satisfaction. In contrast, negative social interactions showed initial associations but did not remain significant after adjustment. While positive social interactions were not significantly correlated with LTL, in either initial or adjusted analyses. These findings highlight the particular importance of intimate relationship quality over general social support or negativity (Newsom et al., 2022; Uchino et al., 2012b).
Our findings align with previous research demonstrating the impact of spousal relationships on physical health (Holt-Lunstad et al., 2010; Kiecolt-Glaser & Wilson, 2017). Barger et al. showed that individuals lacking spousal support had shorter telomeres, emphasizing that spouse support is essential and not interchangeable with other sources (Barger & Cribbet, 2016). While some studies on marital quality failed to find significant associations with TL (de Baca et al., 2017; Yu & Liu, 2021), our study found robust associations between marital satisfaction and telomere dynamics.
While our initial linear regression analyses did not reveal significant associations, the logistic regression approach, comparing substantial telomere lengthening to minimal change or shortening, uncovered these meaningful relationships. Marital satisfaction demonstrated a more robust association across different threshold values than negative interactions and these relationships remained consistent even when excluding participants who were pregnant at follow-up. While pregnancy-related inflammation might theoretically be expected to affect TL, the specific effects of concurrent pregnancy on telomere dynamics are not well-established in the literature. We conducted the sensitivity analysis to ensure our findings were not influenced by the current pregnancy status of these 11 participants at the time of the second telomere measurement.
Our observation of telomere lengthening aligns with previous longitudinal studies that have documented this phenomenon in various contexts (Chen et al., 2011; Leung et al., 2016; Nordfjäll et al., 2009). The postpartum period may represent a unique time of cellular rejuvenation (Giller et al., 2020), though debate exists regarding measurement error versus true biological lengthening (Bateson & Nettle, 2017; Lindrose et al., 2021; Steenstrup et al., 2013).
Of note, our data collection initiated shortly after the first wave of COVID-19, which significantly altered social interactions. Maintaining social interactions during COVID-19 was highly reliant on proximity, online interactions (Long et al., 2022; Stanley & Markman, 2020) and intimate partners (Williamson, 2020). COVID related stress was associated with poorer relationship quality (Balzarini et al., 2020; Pietromonaco & Overall, 2021), nonetheless, couples who were able to avoid conflict and engage in positive coping efforts, experienced an increase in relationship satisfaction (Williamson, 2020). And perceived partner responsiveness-feeling cared and understood, buffered this association (Balzarini et al., 2020). Williamson (2020) found that couples attributed their partners’ negative behaviors to pandemic stress rather than blaming them for it (Williamson, 2020). This could possibly explain the relatively high scores of marital satisfactions and the relatively low scores of negative social interactions depicted in our study.
Many studies have shown that women going through pregnancy and childbirth during the COVID-19 pandemic experienced higher levels of postpartum depression (Mariño-Narvaez et al., 2021; Mollard et al., 2021), as well as higher levels of stress and anxiety (Mollard et al., 2021; Omowale et al., 2021) which are associated with enhanced telomere attrition (Mathur et al., 2016). Indeed, in our sample, postpartum depression prevalence (detected by a cut off EPDS score of ≥10) was 22.3% at timepoint 1 and 18.4% at timepoint 2, higher than the reported levels of 10%–15% PPD pre-pandemic (Anokye et al., 2018). Postpartum depression in our sample was not correlated with LTL, which may reflect the relatively brief exposure period in our one-year follow-up study. However, telomere attrition associated with depression may require longer exposure periods to become detectable, or the transient nature of postpartum depression symptoms during this unique pandemic context may have differed from chronic depression patterns typically associated with telomere shortening in previous research.
Besides the COVID-19 pandemic’s social impact, recent studies have shown that COVID-19 infection is associated with shortened TL. Patients with shorter telomeres had a higher risk of more severe pathologies in COVID-19 (Dos Santos et al., 2021; Froidure et al., 2020; Sanchez-Vazquez et al., 2021) suggesting TL could be considered as a prognostic factor in COVID-19 (Dos Santos et al., 2021). However, other studies suggested that COVID-19 directly contributed to telomere shortening (Mongelli et al., 2021). Huang et al., investigated whether COVID-19 infection was the cause or consequence of TL shortening (Huang et al., 2022) yet did not find evidence to substantiate a causal association between COVID-19 and TL in either direction. Our study provides some interesting insight to this debate as mothers who confirmed a positive COVID-19 diagnosis within the follow up year had 4-fold decreased odds of being in the upper tertile of delta LTL (with the most positive change in LTL within the follow up year) compared to mothers who self-reported a negative COVID-19 test result.
Strengths of Study
This longitudinal design is optimal for studying TL changes over time in postpartum mothers. Our homogenous sample (all married, healthy first-time mothers with normal healthy singleton births who were not taking any regular medications, validated by hospital records) reduced potential confounding factors affecting TL. Additionally, our study differentiated positive and negative social support types and highlighted the particular significance of spousal support on health and TL.
Study Limitations
Our sample size was relatively small, and recent studies have implied that larger sample sizes are required in longitudinal studies using qPCR methods, for adequate statistical power, especially for short follow up periods (Lindrose et al., 2021). This limitation particularly affected our exploratory threshold analyses when examining more extreme values of TL change. Additionally, our threshold values for categorizing TL changes were determined based on data distribution rather than established theoretical cutoffs, which requires cautious interpretation of these findings. We also did not adjust for childhood adversity which has been demonstrated as a strong psychosocial predictor of TL (Ridout et al., 2018; Willis et al., 2018). Moreover, our sample consisted of healthy, married Israeli women with singleton births, which limits the generalizability of findings to more diverse populations. Finally, social interactions (marital satisfaction, negative, positive) were analyzed as dichotomous variables which may not capture the full dimension of these scales. Nonetheless, these variables were not normally distributed, therefore, dichotomizing enabled us to identify differences between the highest and lowest levels of positive and negative attributes of social interactions.
Recent studies have suggested that the qPCR method we utilized for measuring leukocyte TL, might not detect small changes over short periods and that telomere lengthening, as described above, is more likely due to measurement error rather than a biological occurrence and is negatively correlated with the follow up period (Steenstrup et al., 2013). However, the ability to detect true differences in longitudinal studies lies upon assay precision defined by the intra-class correlation (ICC) (Verhulst et al., 2016), which was relatively high in our study {ICC - 0.804, CI = (0.624, 0.9)}.
Moreover, Bateson and Nettle (2017) have demonstrated using qPCR measurements that telomere lengthening mostly occurred (63%) in individuals whose baseline TL was relatively short (below the mean) and telomere shortening mostly occurred (88%) in individuals whose baseline TL was relatively long (above the mean). These predictable patterns have been attributed to the regression to the mean of data sets encompassing measurement error (Bateson & Nettle, 2017; Steenstrup et al., 2013). Nonetheless, in our data set, we did not find similar patterns. Of the 56 women whose baseline LTL was below the mean, only 21 demonstrated telomere lengthening (37.5%) and of the 47 women whose baseline TL was above the mean only three demonstrated telomere shortening (6%). Having that said, although we re-extracted 28 samples from the first batch to adjust the batch effect from the second batch, we cannot completely rule out a potential residual batch effect that might have contributed to the apparent telomere lengthening.
Covarying for baseline TL in longitudinal studies is debated, while it may increase false positives due to regression to the mean, stronger baseline-follow-up correlations weaken this effect (Verhulst et al., 2013; Vickers & Altman, 2001). Our timepoints showed high correlation (r = .812, p < 0.001). We covaried for baseline leukocyte TL, and analyses with and without this covariation yielded similar significant results.
Conclusions
Postpartum is a time of high vulnerability and health changes. Our study found that TL increased on average during the first year after pregnancy, with marital satisfaction showing the strongest association with telomere dynamics and maintaining significance even after correction for multiple comparisons. During this period of high plasticity, marital satisfaction appears particularly important for cellular health.
These findings suggest that intimate relationship quality during the postpartum period has high potential for becoming biologically embedded. Healthcare providers should consider incorporating marital relationship assessment into postpartum care to identify mothers who may benefit from additional support. Future research across larger and more diverse populations could help establish whether these relationships are consistent and generalizable, emphasizing the need for additional longitudinal studies to assess telomere dynamics as a pathway linking relationship quality with health.
Supplemental Material
Supplemental material - Social Interactions and Cell Aging Dynamics in Postpartum Women
Supplemental material for Social Interactions and Cell Aging Dynamics in Postpartum Women by Nourit Houminer-Klepar, PhD, Shiran Bord, PhD, Elissa Epel, PhD, Jue Lin, PhD, Shlomi Sagi, MD, Orna Baron-Epel, PhD in Biological Research For Nursing
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the highly sensitive nature of the health and personal data collected, including genetic information, the datasets from this study are not available for sharing to ensure participant privacy and confidentiality as required by our ethical approval. In exceptional circumstances where data sharing is critical for scientific advancement or public health purposes, requests will be considered on a case-by-case basis subject to institutional ethics committee approval and stringent data protection measures.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.