
Abstract
Patients with rheumatic disease (RD) are at high risk for cardiovascular disease (CVD), which is the leading non-communicable chronic disease cause of death worldwide. Inflammatory biomarkers and psychological health status are reliable predictors of CVD in patients with RD. The primary aim of this study was to compare the inflammatory biomarkers and psychological CVD risk factors (CRFs) between a group of community-dwelling adults with RD and CRFs and a group of their peers with CRFs only. The secondary aim of this study was to analyze and compare the collected data by gender in the RD group. Data were collected and analyzed from 355 participants, with the 135 participants with physician-diagnosed RD assigned to the RD group and the remainder (n = 220) assigned to the comparison group. The measures used included a demographic datasheet, medical information, serum homocysteine (Hcy) levels, high sensitive C-reactive protein (hs-CRP) levels, and depression and global sleep-quality scale scores. The RD group had higher ratios of hypertension and depression diagnoses than the comparison group. The gender analysis of the RD group found significantly more-severe sleep disturbances in women than men and a significantly higher mean value of Hcy in men than women. The women in the RD group were significantly older, less educated, and less employed than their male counterparts and thus may be presumed to at higher risk of health illiteracy. Gender-tailored interventions to modify the risk factors of CVD identified in this study for patients with RD are recommended.
Cardiovascular disease (CVD) is the leading non-communicable chronic disease cause of death worldwide (Mendis, 2017; Zhao et al., 2019). Rheumatic disease (RD), a life-threating disease that affects 11.6%–46.4% of the adult population (American College of Rheumatology [ACR], 2023; Zeng et al., 2008) increases the risk of premature atherosclerosis CVD in sufferers and imposes high burdens on individuals, families, and healthcare resources (Chen et al., 2021; Mahtta et al., 2020; Rahman et al., 2013). RD encompasses over 200 distinct rheumatologic conditions characterized by pain and reduced mobility and physical function in one or more areas of the musculoskeletal system. Examples of RD include gout, osteoporosis, osteoarthritis (OA), and systemic autoimmune diseases such as rheumatoid arthritis (RA) and systemic lupus erythematosus (ACR, 2023; Jokar & Jokar, 2018). Although RD affects people of all ages, middle-aged and older adults face the highest risk of contraction and related morbidity (Hung et al., 2019; van der Heijde et al., 2018).
Early identification of CVD risk factors (CRFs) in patients is the most efficient strategy for preventing and treating CVD (Vaduganathan et al., 2022; Zhao et al., 2019). CRFs compromise a cluster of cardiometabolic risk factors that include smoking, being overweight, being physically inactive, and having dyslipidemia, hypertension, and/or diabetes (Jahangiry et al., 2017; van Breukelen-van der Stoep et al., 2016; Yang et al., 2016). The prevalence of CRFs in patients with RD has been investigated in numerous studies. Van Breukelen-van der Stoep et al. (2016) investigated the prevalence of hypertension and hypercholesterolemia in 327 patients with RA with a mean age of 53, with the resultant data used to develop and test a related intervention. They found a high prevalence of hypertension and hypercholesterolemia in these participants and high rates of underdiagnosis for both conditions. In addition, Dalbeni et al. (2020) conducted a longitudinal study in patients with RA, finding higher mean arterial pressure and diabetes to be significantly correlated with the worsening of atherosclerosis. Also, the results of a cohort study by Long et al. (2023) indicate that obesity, diabetes, and CVD are significantly correlated with to knee OA. Furthermore, research has shown an association between the RD-related medicines used by patients (e.g., corticosteroid, nonsteroidal anti-inflammatory, and selective cyclooxygenase-2 inhibitors) and their risk of adverse vascular events (Atiquzzaman et al., 2019; Dong et al., 2018; Nurmohamed et al., 2015).
The inflammatory biomarkers associated with atherogenesis are novel predictors of CVD that may be used in addition to CRFs to assess CVD risk in patients (Blake & Ridker, 2002; Dong et al., 2019). Different RDs exhibit different inflammatory markers that reflect disease severity and risk of developing atherosclerosis, which is an asymptomatic factor in chronic inflammation. C-reactive protein (CRP) plays a universal role in RD. High sensitivity C-reactive protein (hs-CRP) is a powerful biomarker for predicting CVD that is more sensitive than CRP and not affected by diet or variations in the day-night cycle. Thus, several articles in the literature have recommended hs-CRP be included in models used to assess CRFs in patients (Dong et al., 2019; Jin et al., 2015; Ridker, 2016). In addition, serum homocysteine (Hcy) has been identified in several recent studies as a reliable risk factor for CVD (Shin et al., 2021; Vadini et al., 2019) because excess Hcy has a direct and toxic effect on the body in terms of promoting endothelial and adventitial dysfunction, chronic kidney disease, and increased bodyweight and of elevating blood pressure (Balint et al., 2020; Shu et al., 2020). Prior studies have largely assessed patients with RD using traditional CRFs. To the authors’ knowledge, no studies in the literature have assessed whether adult patients with RD diagnosed with at least one traditional CRFs are also affected by higher levels of inflammatory biomarkers. Although Xu et al. (2020) identified gender and age effects on serum Hcy levels in the general population, the related gender effect in adult individuals with RD has yet to be examined. Thus, further study of this issue is required to address this gap in scholarly knowledge.
Furthermore, psychological health has also been identified as a potential CRF. An analysis by Jee et al. (2019) of national health insurance system data (N = 481,355) identified depression as a significant risk factor for CVD in 41% of the men and 48% of the women in that database, with individuals with depression facing a 2.12 to 2.29 times higher risk of CVD than those without. Also, an epidemiological telephone survey found sleep disturbance to be a significant predictor of CVD and thus a significant risk factor for CVD (Grandner et al., 2012).
Although previous researchers have largely focused on specific types of RD such as OA and RA (Long et al., 2023; van Breukelen-van der Stoep et al., 2016), patients with RD generally experience the disease over the course of their lives as a chronic, concomitant illness in various forms. For example, a high percentage of patients with RA experience concomitant osteoporosis (Ketabforoush et al., 2023). In line with the chronic care model, individuals with chronic conditions should be provided adequate information to help them make important health-related decisions and access available community care resources (Boocha & Ploylearmsang, 2023; Kroenke et al., 2023). Thus, community healthcare professionals should provide sufficient RD-related health information to raise public awareness of CRFs, empower community residents affected by RD, and facilitate the early detection and prevention of CRFs in individuals with RD. RD primarily affects women, who on average live longer than men worldwide (Andreoli et al., 2017). Thus, gender may exert an influence on inflammatory biomarkers and psychological CRFs. Further research is required to identify the biomarkers of CRF in women, clarify their clinical significance, and direct the development of effective gender-specific preventive therapies (DuPont et al., 2019; Mason & Bassuk, 2015). Thus, this study was designed to compare the prevalence of specific CRFs, including inflammatory biomarkers (Hcy and hs-CRP) and psychological (depression and global sleep quality) CRFs, among community-dwelling adults with and without RD who exhibit at least one traditional CRF. In addition, differences in prevalence in terms of gender were assessed in the RD group. The findings of this study are hoped to help raise awareness of this issue among community healthcare providers and to accelerate the development of gender-appropriate supportive care models for community residents with RD.
Methods and Materials
Study Design, Participants, and Procedures
A cross-sectional study with comparative design was employed. We enrolled volunteer participants from accessible communities in southern Taiwan. The institutional review board of Pingtung Christian Hospital approved the study protocol (IRB No: IRB554 B) and all of the participants provided written, informed consent after receiving a comprehensive explanation of the study purposes and procedures. Purposive and snowball sampling methods were applied. The inclusion criteria were: 1) community residents aged 40 or over; 2) exhibiting at least one of the following traditional CRFs: cigarette smoking (current smoker or having quit within the past six months), hypertension diagnosis or currently taking antihypertensive medication, dyslipidemia diagnosis or currently taking dyslipidemia medication, physical inactivity (lack of regular exercise [defined as
Otherwise-eligible individuals with any of the following criteria were excluded from participation: 1) currently pregnant, 2) having impaired renal function, congestive heart failure, stroke, myocardial infarction, or a cancer diagnosis, 3) bedridden, 4) having a current cold, any signs of infection (e.g., fever, redness), wound, or surgery during the past month, or 5) having a psychiatric disorder. The effect size was determined based on the methodology described in a prior study (Lakoski et al., 2006) and calculated using the formula of Plichta and Kelvin (2013). G-Power 3.1.2 was used to estimate the minimum sample size with a medium (f = .45) effect size, a significance level of p < .05, and a power of .8. A minimum of 140 participants was determined to be necessary in each group to adequately detect mean intergroup differences. The first author standardized the data collection procedures and trained 3 research assistants to ensure interrater consistency in data collection.
Data Collection
Data were collected between September 2017 and August 2018. During face-to-face interviews, a demographic datasheet was used to collect information on age, gender, educational level, marital status, religious status, employment status, and targeted health behaviors (e.g., cigarette smoking, alcohol consumption). Medical information, including physician-diagnosed disease type, adherence to taking regularly prescribed medications and nutritional supplements during the most-recent 3-month period, and types of nutritional supplements taken were also collected. In addition, psychometric questionnaires, including the 15-item Geriatric Depression Scale [GDS-15] and Pittsburgh Sleep Quality Index [PSQI] were used to collect related data from the participants. Finally, inflammatory biomarkers in blood samples (serum hs-CRP [measured using a Latex enhanced immunoturbidimetric, Siemens Advia 1800 Chemistry Analyzer] and Hcy [measured using a Siemens Advia Centaur Chemiluminescence Immunoassay Analyzer]) were collected and analyzed. All biomarkers were obtained between 08:30–11:00 and all study data were collected at either the participants’ residential community activity/care center or their home. Non-fasting blood samples were taken from the antecubital vein to obtain hs-CRP and Hcy values.
Depression was assessed using the GDS-15, which has previously demonstrated good validity and reliability (Sheikh & Yesavage, 1986) as well as good sensitivity (81.3%) and specificity (78.4%; Mitchell et al., 2010). The GDS-15 consists of 15 yes/no questions relating to how the respondent felt over the past week, with total possible scores ranging from 0 to 15 and scores > 5 indicative of depression. The Cronbach’s α for the GDS-15 was .83 in this study. The Pittsburgh Sleep Quality Index (PSQI), developed by Buysse et al. (1989), is a self-rated questionnaire designed to measure global sleep quality over the past month. The 19 items of this index generate 7 component scores, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The total possible summed score for the 7 components ranges from 0 to 21, with a global PSQI score greater than 5 considered indicative of being a poor sleeper. The PSQI was previously found to have a test-retest reliability of .87, sensitivity of 98.7%, and specificity of 84.4% when used as a marker for sleep disturbance (Backhaus et al., 2002). The Cronbach’s α of the PSQI was .79 in this study. Each participant was apprised of their blood test results and of their identified traditional CRFs.
Statistical analysis
All of the analyses were performed using IBM SPSS Statistics version 22.0 for Windows (SPSS Inc, Chicago, IL, USA). The demographic characteristics of the 2 groups were compared using an independent t test, χ2 test, and Fisher exact test. Age and gender distributions, numbers of traditional CRFs, nutritional supplements used, comorbidities, and regular medication prescriptions differed significantly between the RD and comparison groups. Furthermore, statistically significant differences in age, educational level, employment status, nutritional supplements used, and alcohol consumption were observed between the women and men in the RD group. Analysis of covariance (ANCOVA) was used to examine the intergroup differences in terms of major variables.
Results
Of the 358 individuals invited to participate, 355, with a mean age of 56.2, completed the data collection procedures. The participants had an average of 2.02 (SD = 1.34) traditional CRFs, with the 3 most common being physical inactivity (n = 207, 58.3%), obesity (n = 201, 56.6%; mean of body mass index = 24.62), and hypertension (n = 93, 26.2%). Walking was the most prevalent type of exercise engaged in by participants who exercised “regularly” (n = 77, 69.4%). Over one-third of the participants (n = 120) had one or more chronic diseases, of which hypertension (18.1%) and diabetes (5.7%) were the most commonly cited. Furthermore, the mean levels of serum Hcy and hs-CRP were 13.2 μmol/L and 0.23 mg/dL. The overall sample had a prevalence of hyperhomocysteinemia (HHcy > 15 μmol/L; Xu et al., 2020) of 26.2% and an elevated hs-CRP prevalence (> 0.1 mg/dL indicating moderate [10-year probability of CVD event 6–20%] or high risk [10-year probability of CVD event > 20%] to CVD; Ridker, 2016; Wilson et al., 2008) of 44.6%.
Basic Characteristics by Group (N = 355).
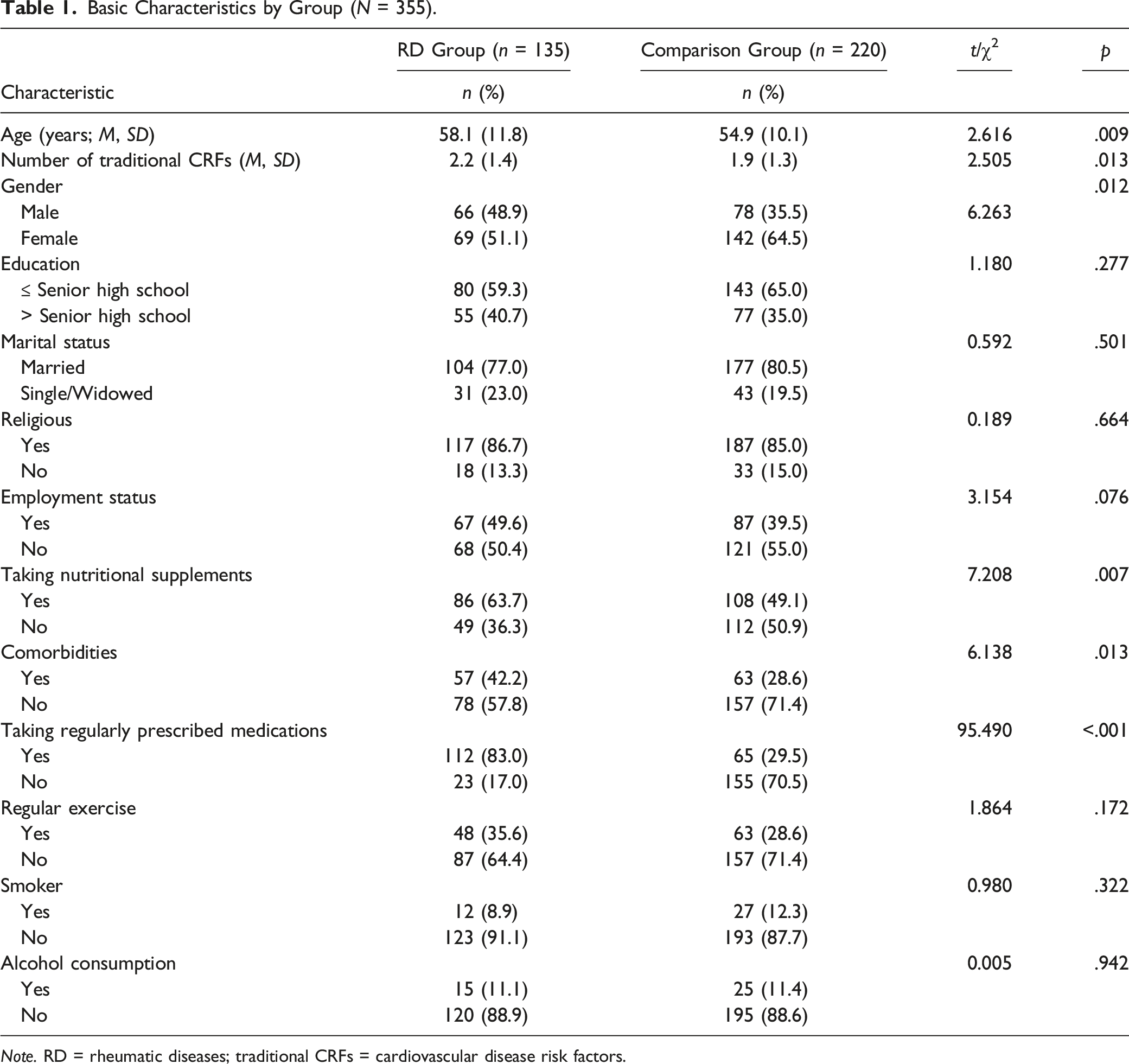
Note. RD = rheumatic diseases; traditional CRFs = cardiovascular disease risk factors.
ANCOVA for Depression, Global Sleep Quality, Homocysteine, and Hs-CRP Between Groups (N = 355).
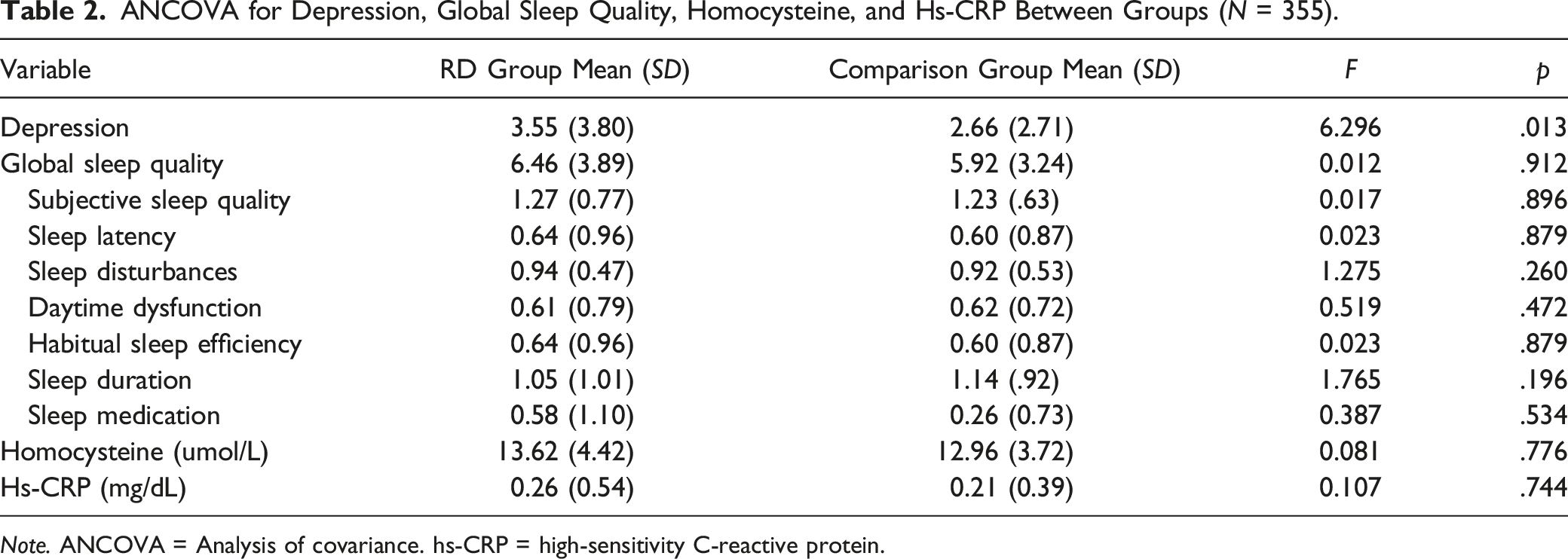
Note. ANCOVA = Analysis of covariance. hs-CRP = high-sensitivity C-reactive protein.
Basic Characteristics by Gender, RD Group (N = 135).
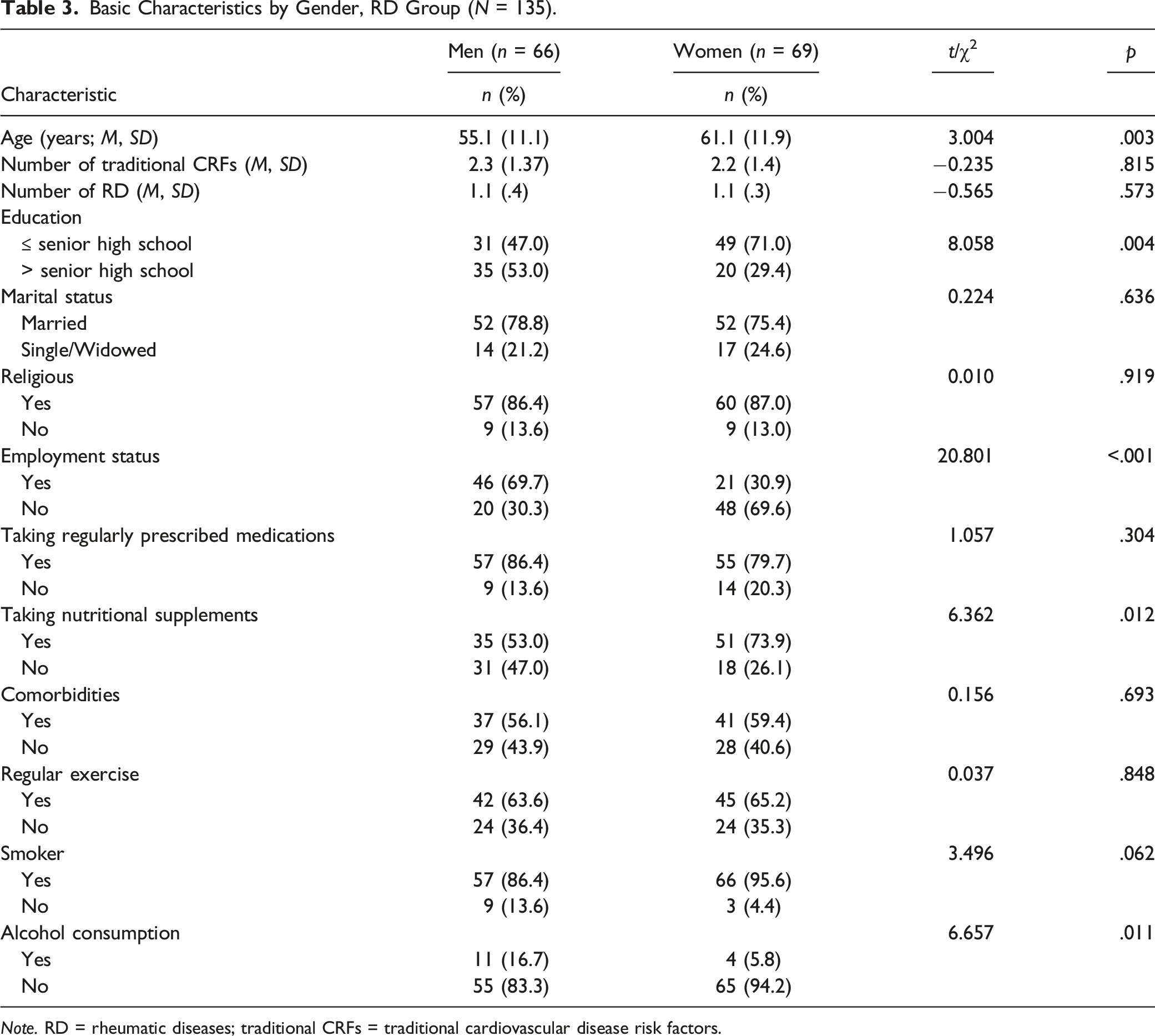
Note. RD = rheumatic diseases; traditional CRFs = traditional cardiovascular disease risk factors.
ANCOVA for Depression, Global Sleep Quality, Homocysteine, and Hs-CRP by Gender, RD Group (N = 135).
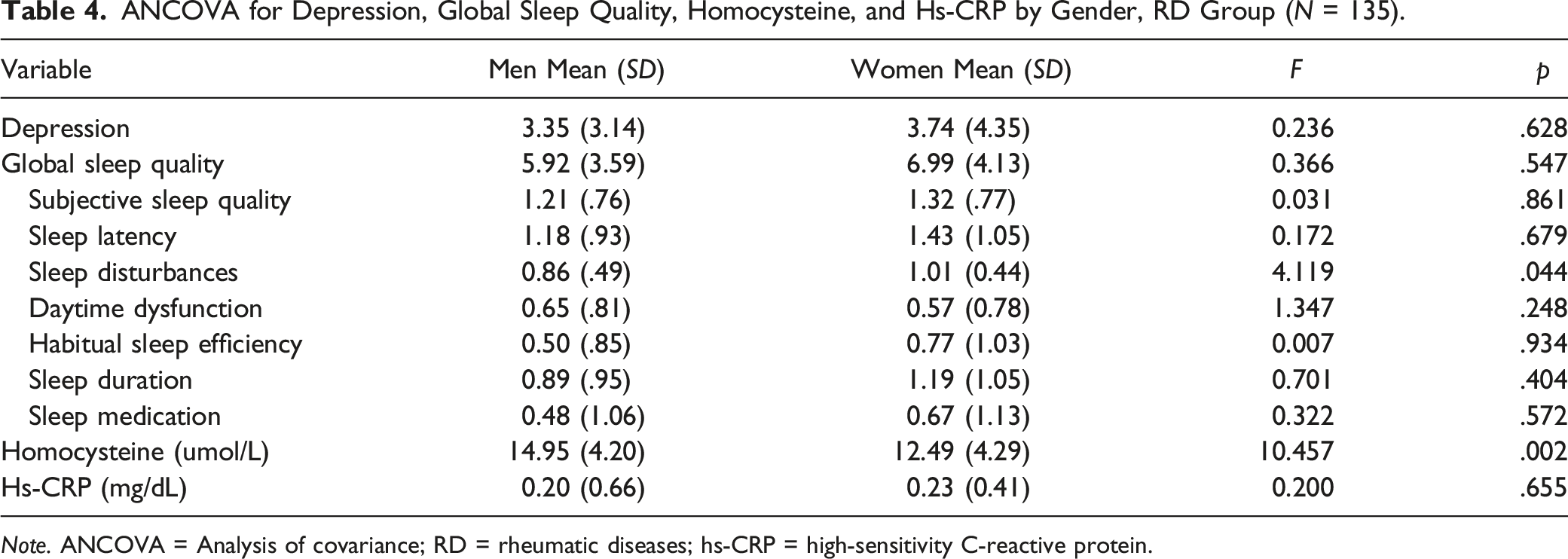
Note. ANCOVA = Analysis of covariance; RD = rheumatic diseases; hs-CRP = high-sensitivity C-reactive protein.
Discussion
The findings of this study support the need to focus more research attention on confirming and validating depression as a significant RD-related CRF and to develop tailored support strategies for middle-aged and older adults with RD. In addition, the results point to sleep disturbance as a significant CRF in women with RD and elevated Hcy, which is amenable to self-management, as a significant inflammatory biomarker of CRFs in men with RD. Several methods were used to enhance the rigor of this study. First, subjective and objective data were collected following a standardized protocol and the same instruments were used to gather the CRF status data for all of the participants in community settings, which may be expected to help improve clinical decision-making. Second, we used 2 sampling methods to increase the number of participants with RD. Third, research assistants were trained uniformly on the data collection procedures to further reduce bias.
The most-prevalent traditional CRFs identified in this study included physical inactivity and obesity. Differences in inclusion criteria and study populations preclude comparing this finding directly with the national surveys conducted by Gu et al. (2005) and Yang et al. (2016) in China. Those 2 studies, which investigated dyslipidemia, hypertension, diabetes, cigarette smoking, and overweight status in nationally representative populations of 35 to 45-year-old adults in China, identified dyslipidemia and hypertension as the 2 most-prevalent traditional CRFs. Notably, in this study, participants were affected by 2 traditional CRFs on average. Following Hendrani et al. (2016), lifestyle modifications such as exercising regularly and consuming diets lower in saturated fats should be promoted as the cornerstone of dyslipidemia, obesity, and hypertension management. Most of the participants in this study who reported exercising regularly cited walking as their primary form of exercise. However, only 42.1% of the participants reported engaging in regular exercise, suggesting that community healthcare professionals should coordinate with sports medicine experts to design moderate-intensity exercise programs that take into consideration the physical-function limitations of older adults living in the community.
Over one-quarter of the participants (26.2%) in this study were diagnosed with hyperhomocysteinemia (HHcy), which is significantly higher than the 3.1% prevalence reported in the retrospective study of Toya et al. (2020), which reviewed the charts of 257 patients available for baseline serum Hcy levels who had undergone a non-invasive peripheral microvascular endothelial dysfunction (PMED) assessment. Also, Toya et al. found a positive and significant association between a mild increase in the concentration of Hcy (>10.0 μmol/L) and PMED, which may partially explain the mechanism behind the positive relationship between CVD levels and HHcy. The average serum Hcy value in this study of 13.2 μmol/L indicates that most of the participants were at increased risk of CVD. A deficiency in B-vitamins or folate potentially increases plasma Hcy (Balint et al., 2020). Thus, the authors advised those participants with modestly elevated Hcy levels to consult their family doctors about this issue. The potential link between B-vitamin and folate supplementation with reduced serum Hcy levels and CVD events will be investigated by the authors in collaboration with nutritional professionals in the future.
The values of Hcy and hs-CRP were slightly but not significantly higher in the RD group than the comparison group. Thus, none of the inflammatory biomarkers differed significantly between the groups, which partially echoes the findings of other related studies. A retrospective cohort study by An et al. (2016) that drew data from a healthcare system database to compare patients with RA and general controls in terms of CRFs found no significant between-group differences in terms of blood pressures and BMI and found that patients with RA used more antihypertensive medication than the controls. Moreover, Han et al. (2006), which compared patients with RD and control subjects using an international disease classification, demonstrated that patients with RD had more comorbidities and used more cardiovascular medications (e.g., vasodilators) than controls.
In this study, although level of depression in the RD group was statistically higher than in the comparison group, global sleep quality was similar in both groups across all seven subscales, partially echoing the findings of previous studies. Fertelli and Tuncay (2019) compared 151 patients with OA of the knee and 147 healthy subjects, finding higher levels of fatigue, sleep disturbance, and depression in the OA patients than in the healthy controls. Individuals diagnosed with RD are particularly susceptible to bodily pain, low vitality, immobility, and disease flare, all of which may adversely affect psychological health (Hung et al., 2019; Kwiatkowska et al., 2019). Moreover, chronic health conditions are often associated with sleep disturbances (de la Vega et al., 2019). In this study, the participants in both groups exhibited poor global sleep quality (PSQI score >5; mean scores of 6.46 and 5.92 for the RD and comparison groups, respectively). However, all of the participants were affected by at least one of the traditional CRFs, including chronic conditions such as hypertension and diabetes, which may negatively impact sleep quality and may explain the similarly poor global sleep quality results for both groups. Therefore, longitudinal studies should be developed to assess the effects of positive coping strategies on CRFs in poor sleepers and depressed individuals.
With regard to gender, in the RD group, the female participants had significantly lower levels of Hcy and experienced worse sleep disturbances than their male counterparts, which partially reflects the findings of Cohen et al. (2019), who conducted a cross-sectional analysis and collected data from medical records between 2000-2014. They found average plasma Hcy to be higher in men (mean age = 48.4 years) than in women (mean age = 47.7 years; 12.6 μmol/L vs. 9.6 μmol/L) and attributed this differences to gender metabolism. Xu et al. (2020) reported a marked increase in Hcy levels in women over 55 years old and the presence of visceral adiposity and lipid metabolic changes in women experiencing menopause, which may warrant special consideration in terms of CVD risk (Mason & Bassuk, 2015). Notably, in the RD group in this study, the average Hcy level was 14.95 μmol/L among the men, which was close to the threshold for HHcy (HHcy > 15 μmol/L; Xu et al., 2020) and significantly higher than the average of 12.49 μmol/L among the women. These findings highlight that, while RD impacts both men and women, the mechanisms underlying the related interactions among gender, Hcy, and traditional CRFs are unclear and require further experimental study. Also in this study, women in the RD group experienced more-severe sleep disturbances than their male peers. Few studies are available in the literature to compare our findings. Sleep disturbances measure the frequency of disturbed sleep incidents (Buysse et al., 1989). Women with higher levels of role load experience adverse mental health effects (Hung et al., 2019), which may indirectly affect the level of sleep disturbances. Also, the investigation of sleep disturbances in mid-aged women conducted by Ornat et al. (2014) found a significant association between disturbed sleep and menopause. The women with RD in this study both had a mean age (61.1 years) that was higher than the average for the overall sample and had a slightly poorer global sleep quality than men (6.99 vs. 5.92).
The women in the RD group in this study were older, less educated, and less employed than their male counterparts, which may limit their health literacy regarding CRF biomarkers. These findings should be considered when developing related educational programs to help women at potentially higher risk of CVD. Furthermore, to improve the reliability and generalizability of our findings, larger sample sizes of men and women should be recruited in future related studies.
The primary limitation of this study is the use of a cross-sectional study design, which provides no evidence or insights regarding the longitudinal relationship between CRFs and CVD in community-dwelling individuals with RD. Because RD is a lifelong chronic illness, we encouraged the participants with CRFs to enhance the self-management support they receive within their community settings. Another limitation of this study is that random sampling was not used due to structural limitations that made it impossible to identify community dwellers with CRFs and RD prior to the assessments. Based on the principle of beneficence in human research (Pieper & Thomson, 2016), the first author (a healthcare provider) defined the target population as middle-aged and older community-dwelling adults. Many of the participants with RD were referred to this study by members of the comparison group, which may also limit the generalizability of the findings. Finally, because participants were recruited from the community, the authors could not review their medical records to verify the effects on biophysical and psychological CRFs using medical or laboratory data.
Conclusions
The findings of this study indicate community residents with CRFs over 40 years old face an elevated risk of exhibiting increased levels of inflammatory biomarkers for CRFs, including modestly elevated serum Hcy and hs-CRP, regardless of RD status. Also, the findings indicate a significant impact of RD on depression status. Moreover, the women participants with RD experienced significantly more-severe sleep disturbances than their male peers. This study adds to the scholarly knowledge regarding the impact of sociocultural factors on human health by providing evidence on the effects of inflammatory biomarkers, psychological CRFs, and gender on the health of patients diagnosed with RD and CRFs.
CVD is a multifactorial disease. The causal exposure model (CEM) is a risk factor model for CVD widely accepted and used by healthcare professionals (Sniderman et al., 2012). Based on the findings of this study, serum Hcy, hs-CRP, and psychological health status should be added to routine tests administered to the general population and community residents with RD and CRFs. Furthermore, appropriate strategies should be developed within the CEM framework through interdisciplinary collaboration to reduce the long-term, negative effects of RD by better controlling the modifiable risk factors of CVD. Gender-tailored interventions to modify these risk factors are also recommended.
Footnotes
Acknowledgments
The authors thank all of the study participants.
Author contributions
Hsuan-Man Hung. contributed to conception and design contributed to acquisition, analysis, and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Ming-Fu Chen. contributed to acquisition and analysis gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Huan-Fang Lee, contributed to analysis gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Hui-Ling Wang. contributed to acquisition gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by grant MOST 106-2314-B-127-002 from the National Science and Technology Council, Taiwan.