
Abstract
Background
Breast cancer is currently the most prevalent malignancy among women. Psychological resilience is an important factor that diminishes the stress-related emotional and psychosocial disturbances triggered when receiving the diagnosis. Furthermore, resilience appears to be associated with cortisol, the hormonal end-product of the hypothalamic-pituitary-adrenal axis; however, further studies are needed due to the mixed results reported. Thus, we aim to examine the predictive role of social support and cortisol in resilience among breast cancer patients.
Methods
A total of 132 women with primary breast cancer completed the Medical Outcomes Study-Social Support Survey (MOS-SSS) and the Resilience Scale (RS-14) and provided four salivary samples for the estimation of participants’ total daily cortisol production, for which the formula of the area under the curve with respect to the ground (AUCg) was applied. Moderation analyses were performed to study the influence of social support and AUCg on psychological resilience levels.
Results
The regression analyses showed a direct significant effect for the emotional support subscale of MOS-SSS on resilience and the interaction between emotional support and AUCg was also found to be statistically significant. Specifically, the conditional effect of emotional support on resilience was found to be significant at middle (M = 3.08; p < .05) and low levels (M = .59; p < .001) of AUCg.
Conclusions
Our results suggest that newly diagnosed breast cancer women with middle and low diurnal cortisol profiles may benefit more from emotional support based-interventions while women with high diurnal cortisol may need more individualized therapies.
Introduction
Breast cancer is currently the world’s most prevalent malignancy among women, with approximately 2.3 million new cases identified in 2020 that are expected to more than double by 2030 (Cerezo et al., 2022; World Health Organization, 2021). The diagnosis of breast cancer is a potentially stressful life event that can significantly deteriorate patients’ health due to its implications and consequences in areas such as physical, psychological, social, economic, and spiritual (Aizpurua-Perez & Perez-Tejada, 2020). Specifically, the scientific literature points to anxiety and depression as highly prevalent emotional problems during the year following diagnosis and throughout the course of the disease (Hernández Blázquez & Cruzado, 2016; Seib et al., 2018) with important repercussions on the patients’ adjustment as they can worsen their disease prognosis and reduce their life satisfaction (Seib et al., 2018). Interestingly, while for some women coping with disease-related demands is a particularly challenging process, many others adapt much more effectively (Macía et al., 2020; Montiel et al., 2016). Psychological resilience has been identified as an important variable in explaining these differences (Mikolajczak et al., 2008).
Resilience is understood as the ability to cope successfully with stressful life events despite the adverse and traumatic nature of the faced circumstances (Bonanno, 2012). In cancer patients, resilience refers to an interactive and dynamic process characterized by effective adaptation to disease-related adversity (Eicher et al., 2015). Thus, highly resilient cancer patients are characterized by individual protective attributes encompassing cognitive flexibility, positive affect, an active coping style, and/or acceptance of adverse events, leading to more adaptive outcomes when facing disease-related challenges (Aizpurua-Perez & Perez-Tejada, 2020; Deshields et al., 2016; Macía et al., 2022). Conversely, less resilient breast cancer patients usually exhibit a more pessimistic outlook on life, decreased physical functioning, and more severe treatment-related side effects (Ristevska-Dimitrоvska et al., 2015).
Among the various protective factors thought to influence resilience, social support stands out as one of the most relevant (Zhang et al., 2017). Social support is defined as the perception of the availability of supportive resources in the environment, such as emotional, affective, or instrumental resources (Sherbourne & Stewart, 1991), which has been found to play a protective role in coping with traumatic or negative life experiences (Migerode et al., 2012; Somasundaram & Devamani, 2016). Moreover, scientific research provides evidence of the positive effects of social support in alleviating the negative effects of stressful circumstances experienced during oncological processes, including breast cancer populations (Kim et al., 2010; Kroenke et al., 2013). Interventions based on increasing awareness of social support in breast cancer patients have demonstrated significant effectiveness in improving their emotional well-being. In fact, perceptions of quality social support have been shown to decrease levels of depression, boost self-esteem, and favor ways of coping with the disease (Fong et al., 2017; Huang & Hsu, 2013; Kim et al., 2010). Breast cancer patients with more perceived social support are more able to cope better with the disease burden and return to their lives faster (Çakir et al., 2021). Nevertheless, the large methodological variability of studies measuring social support and resilience in breast cancer patients makes it difficult to draw firm conclusions about the association between social support and resilience at diagnosis before the initiation of treatment (Aizpurua-Perez & Perez-Tejada, 2020; Huang & Hsu, 2013; Zhang et al., 2017).
In contrast to the large number of studies aimed at examining the psychosocial correlates of resilience, only a few have investigated its biological correlates, and specifically its relationship with cortisol, the hormonal end-product of the hypothalamic-pituitary-adrenal (HPA) axis (Lai et al., 2020). As for the latter, dysregulation of the diurnal cortisol secretion is associated with various pathological disorders such as depression, post-traumatic stress and/or anxiety, cardiovascular diseases, and even breast cancer mortality (Labonté et al., 2014; Speer et al., 2019; Doane et al., 2013; Kumari et al., 2011). In particular, dysregulation of the cortisol-awaking response (CAR) has been found to be related to psychological distress in breast cancer patients (Perez-Tejada et al., 2019). With respect to the relationship between resilience and cortisol, during the last few years some studies have found positive (Lai et al., 2020; Lines et al., 2021), negative (Krisor et al., 2015; Burgin et al., 2020) and null (Ramiro-Cortijo et al., 2021; Sharpley et al., 2018) associations between the two variables in different populations, making it difficult to derive clear conclusions about the nature of their relation from these mixed results. Furthermore, only one of these studies was conducted in cancer patients (Sharpley et al., 2018); after analyzing the basal salivary cortisol response of prostate cancer patients no significant associations between the two variables was found. This coupled with the robust evidence for sex-specific behavioral and physiological responses to stress (Bangasser & Wicks, 2017), as well as studies reporting evidence suggesting that the HPA axis functions in a sex-dependent manner (Barel et al., 2018; Goel et al., 2014; Heck & Handa, 2019), indicate that studies aimed at examining. Bidirectional influences between resilience and cortisol in women with breast cancer are necessary.
Given the large number of studies demonstrating a positive association between resilience and social support (Cai et al., 2017; Çakir et al., 2021), and the close association between diurnal cortisol rhythms and health outcomes (Caulfield & Cavigelli, 2020), it is plausible that resilience is shaped by the same diurnal cortisol rhythm related with better health. The main objective of the present study is to examine the predictive role of social support and cortisol in explaining psychological resilience among newly diagnosed breast cancer patients.
Methods
A descriptive cross-sectional design was used to study the influence of cortisol and social support on resilience among women with breast cancer. Participants were 132 women newly diagnosed with breast cancer recruited from a hospital located in the Basque Country (Spain). The sample focused on those women who received their cancer diagnosis for the first time, due to the possible influence on the psychological state that a previous diagnosis of cancer could have. Therefore, the inclusion criteria for this study were: (1) non-pregnant women aged 18–70 years; (2) cancer diagnosis for the first time within the last 2 months; and (3) no history of a known mental disorder. The exclusion criteria were women with metastases. Women who met the inclusion criteria were informed about the study procedures and those who agreed to participate were given a detailed informed consent with sufficient time for their consideration. All procedures performed in this study were in accordance with the relevant national legislation and were approved by the corresponding Ethics Committee.
Procedure for Salivary Cortisol Collection
After participants signed the informed consent they were provided with four tubes for saliva collection; they were asked to collect saliva at four different times on a single day: upon awakening, 30 minutes after awakening, at 1:00–1:30 pm, and at 8:00–8:30 pm. In order to ensure that saliva sampling was free of contamination from particulate matter or other interfering substances, thus diminishing the possibility of sampling error, participants were instructed to abstain from eating, drinking, or brushing teeth 30 min before sample collection. After the cortisol self-collection, participants were required to store the saliva samples at 4°C in their home freezers and deliver them the next day to the researchers together with the completed questionnaires.
Psychological and Physiological Variables
The psychological measures included the Medical Outcomes Study-Social Support Survey (MOS-SSS) and the Resilience Scale Short version (RS-14). The MOS-SSS (Sherbourne & Stewart, 1991) is a self-administered multidimensional measure of social support that assesses the availability of different types of support through 19 5-point Likert items (ranging from: ‘never’ = 1 to ‘all of the time’ = 5). In the Spanish adaptation of this questionnaire in the oncology population, the factor structure of the MOS-SSS was grouped into 3 factors: (a) emotional/informational support and positive social interaction, (b) affective support, and (c) instrumental support (Costa Requena et al., 2007). To obtain the total scale score, the addition of all the items is necessary (range 19–95). The Cronbach’s Alpha coefficient of total scale in this study was .95.
The RS-14, a short 14-item Spanish version of Wagnild and Young’s (1993) resilience scale was used to identify the level of resilience of the participants (Sánchez-Teruel and Robles-Bello, 2015), understood as the degree of perceived competence and self-acceptance. Each of the 14 items has a 7-point Likert-type response graded from ‘1’ (strongly disagree) to ‘7’ (strongly agree), with a total score range from 14 to 98. In particular, scores under 65 indicate low resilience, those between 65 and 81 reflect moderate resilience, and scores above 81 indicate high levels of resilience (Mirosevic et al., 2019). The reliability coefficient of psychological resilience in the present study was .90.
The saliva was centrifuged at 3000 rpm for 15 min to remove mucins and frozen at −80°C until enough samples were collected to be analyzed in batches. An enzyme immunoassay kit (Salimetrics, Stratech Scientific, UK) was used to determine cortisol levels, and plates were read at 450 nm using a Synergy™ HT plate reader (Bio-Tek Instruments, Inc, Winooski, VT, USA). The assay sensitivity of cortisol was .007 μg/dL, and the average intra and inter-assay variation coefficients were 1.8%, and 1.97%, respectively. Finally, the area under the curve with respect to the ground (AUCg) was calculated for the determination of participants’ total diurnal cortisol production based on the cortisol data time points.
Statistical Aanalysis
To test possible associations between the different variables studied, Spearman correlation coefficient was used. Regression analyses were carried out to study the influence of AUCg, social support subscales, and their interactions on resilience, with the following variables included as controls: type of initial oncologic treatment (chemotherapy or surgery), type of surgery, and use of psychotropic drugs. To assess significant interactions, moderation analyses with the Johnson–Neyman technique were used (Hayes, 2013). All statistical analyses were conducted using the SPSS 26.0 statistical package.
Results
Demographic and Clinical Characteristics of the Sample and Descriptive Data for Psychological and Biological Variables.
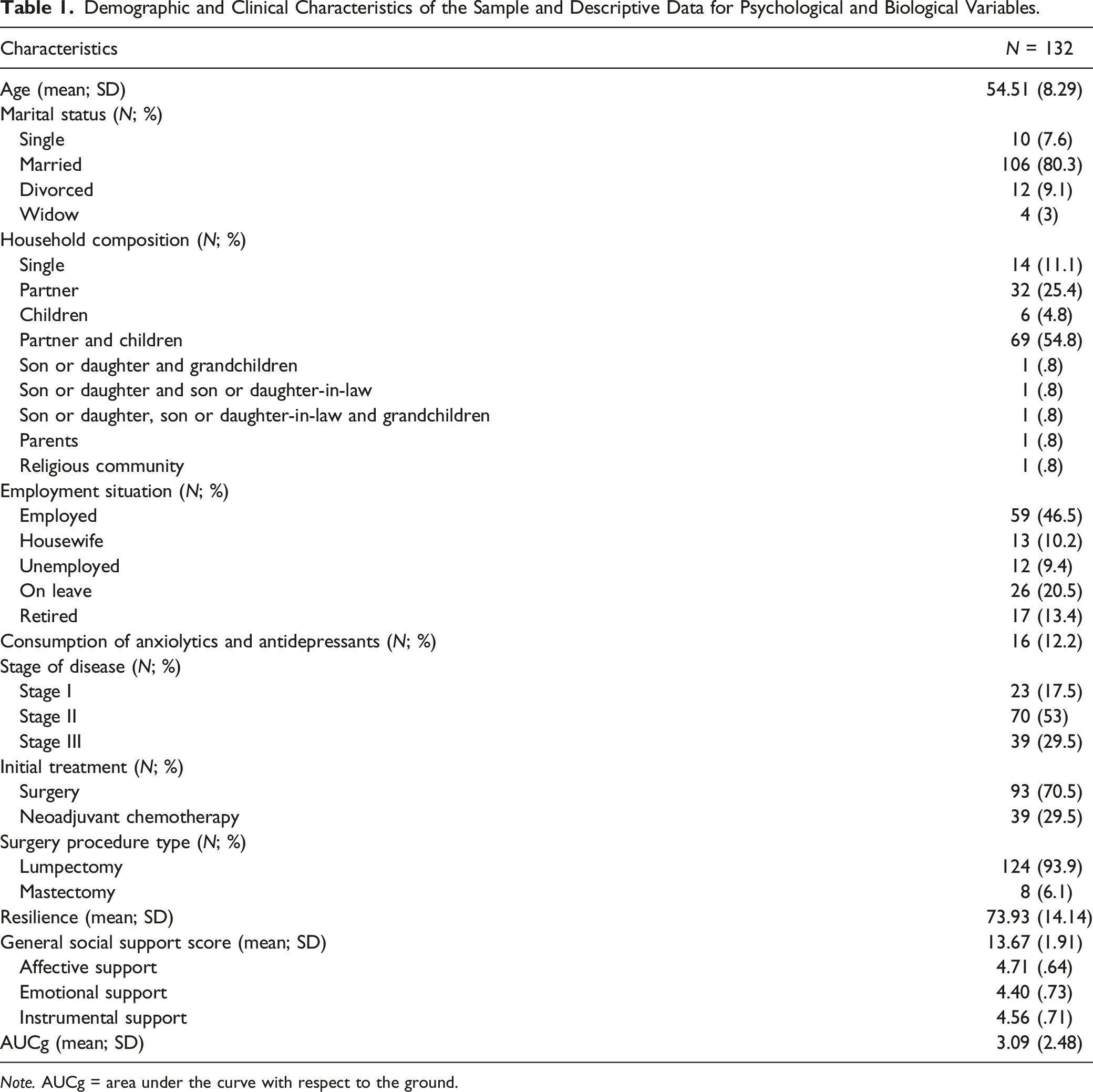
Note. AUCg = area under the curve with respect to the ground.
Correlation Analyses
Spearman Correlations Between Resilience, General Score, and Subscales of Social Support and AUCg.
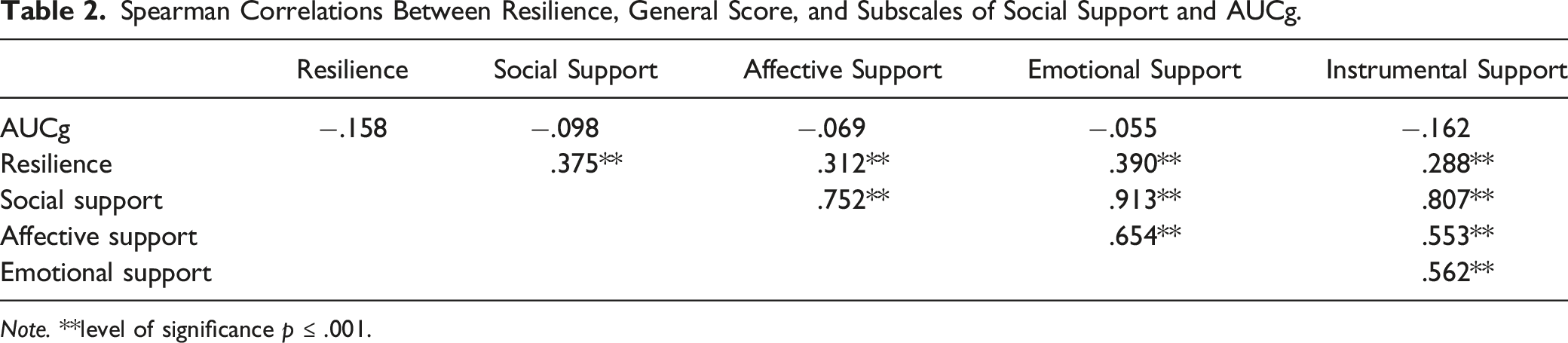
Note. **level of significance p ≤ .001.
Effects of the Interaction Between Psychological Variables and AUCg on Resilience
Regression Analysis for Resilience.
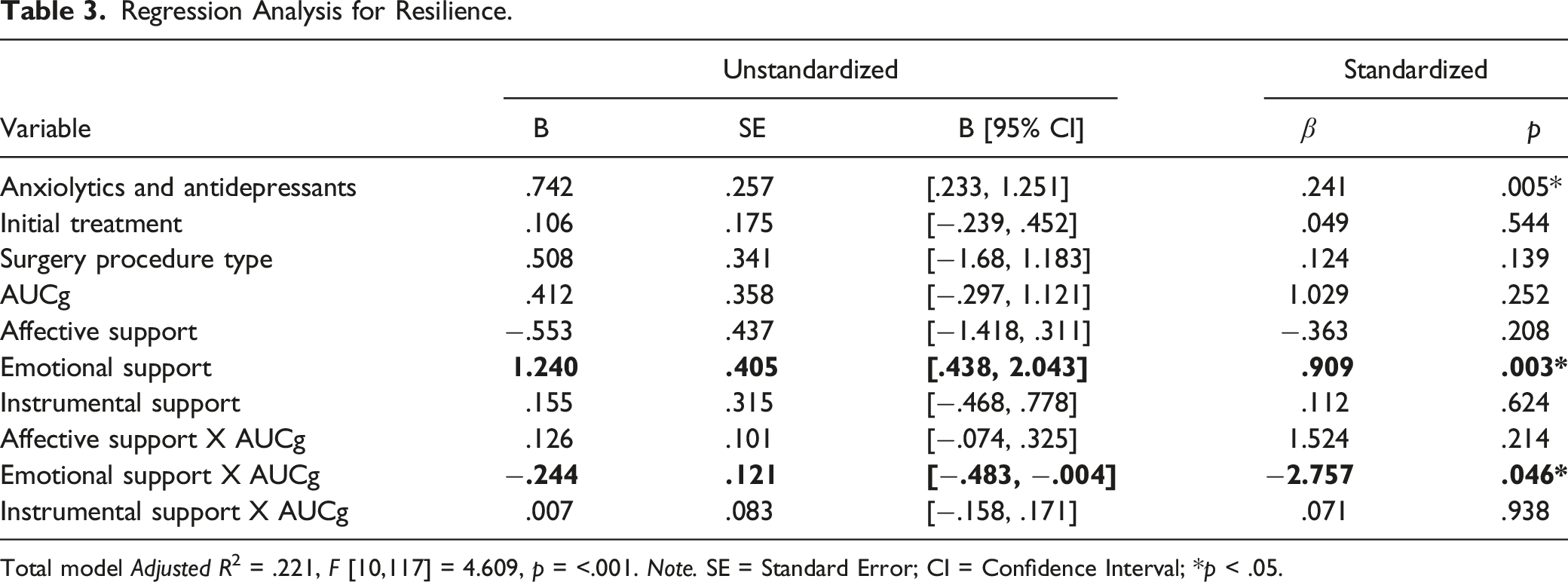
Total model Adjusted R2 = .221, F [10,117] = 4.609, p = <.001. Note. SE = Standard Error; CI = Confidence Interval; *p < .05.
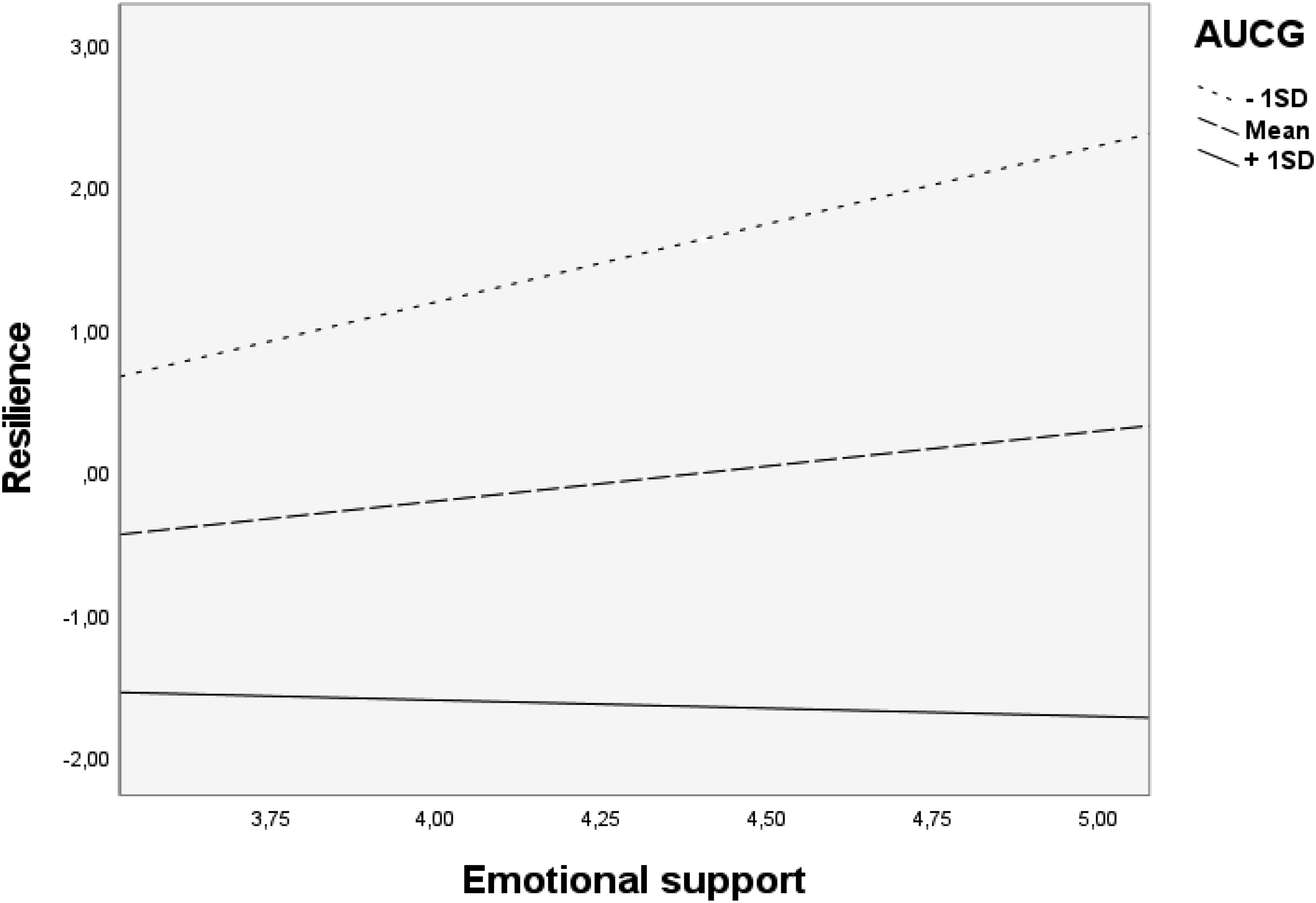
Moderating effect of AUCg on the relationship between emotional support and resilience.
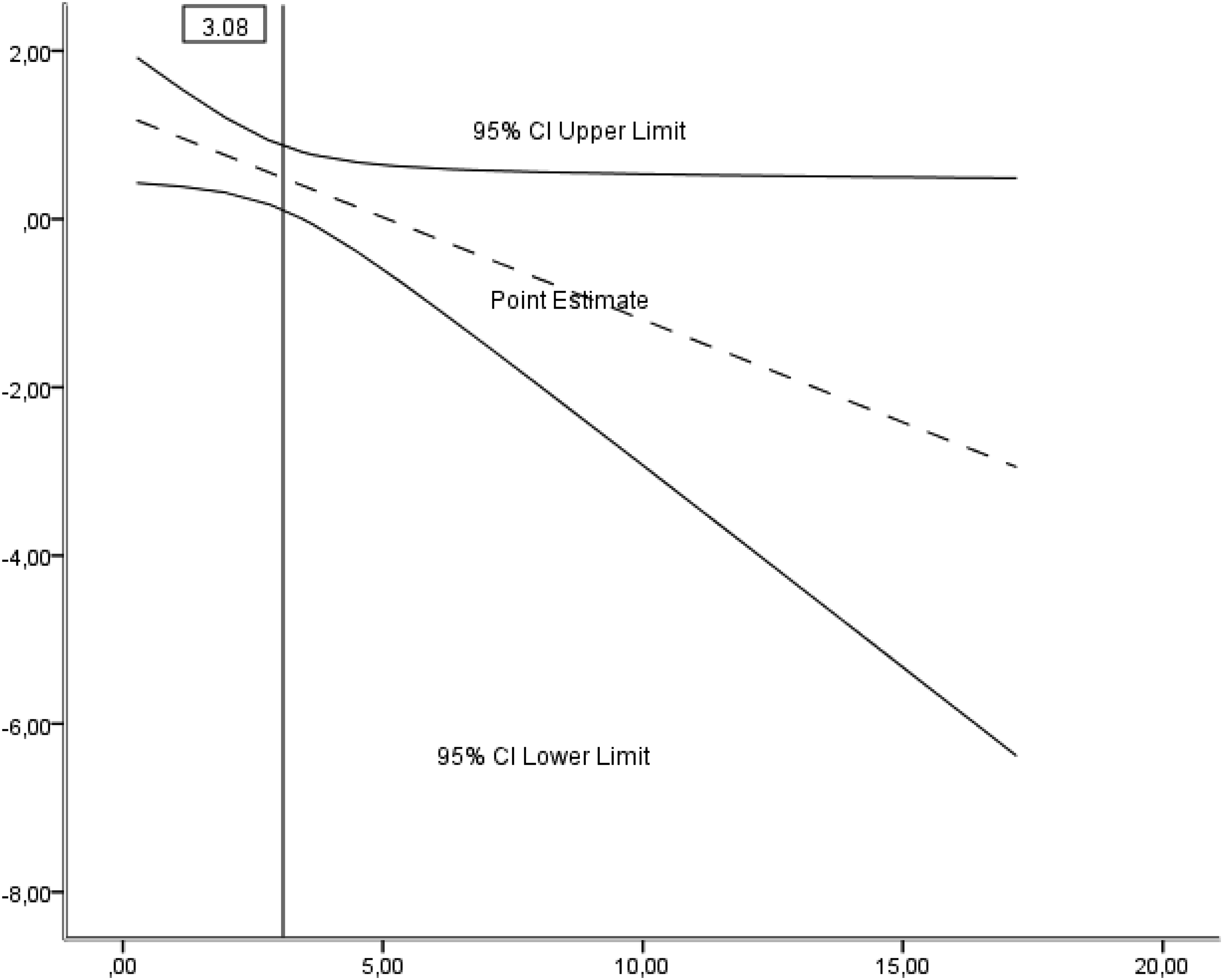
Floodlight analysis graph of the conditional effect of emotional support on resilience as a function of AUCg: the effect of emotional support on resilience is only statistically significant at medium (mean) levels (cutoff point M = 3.08; p < .05; 95%CI) of AUCg, including low (-1SD) levels of AUCg (M = .59; p < .001; 95%CI).
Discussion
Our results indicate that the resilience of newly diagnosed breast cancer patients is partially influenced by social support and diurnal cortisol secretion (AUCg), explaining 28% of the variance. The overall punctuation of the social support scale as well as each of its subscales, namely affective, emotional, and instrumental support, were revealed to positively correlate with resilience. According to a systematic review that supported this finding, patients with breast cancer who perceived higher availability of social support were more likely to display greater levels of resilience (Aizpurua-Perez & Perez-Tejada, 2020), although some other authors reported that social support has a lower impact on resilience when patients are in the moment of the diagnosis (Gálvez-Hernández et al., 2018; Wu et al., 2016). This difference might be the result of important factors that were not previously considered, such as cortisol. In this sense, this is the first study to our knowledge, that measures resilience and cortisol along with social support simultaneously in breast cancer patients, and the results point out the moderating role of AUCg in resilience. Specifically, the correlation analysis showed a negative trend between AUCg and resilience. This finding is in line with studies hypothesizing that resilient individuals may have better regulated cortisol levels than their non-resilient homologs (Nishimi et al., 2022; Petros et al., 2013). Thus, evidence suggests that psychological resilience acts as an attenuator of the deleterious effects of the physiological response to stress by reducing alterations in daily cortisol patterns, serving as a modulator of the link between diurnal cortisol and health and, thereby, improving adaptation (Gaffey et al., 2016). Proof of the latter is the study by Ruiz-Robledillo et al. (2017), which found that higher resilience levels were related to low AUCg in caregivers of children with autism. Moreover, our regression analysis showed a significant interaction between AUCg and emotional support when explaining resilience. Specifically, middle and low levels of AUCg strengthen the positive contribution of emotional support to resilience, while no interaction was found in patients with high levels of AUCg. With regard to the former group, it can be inferred that social support act as a protective factor that promotes adaptation to the shocking diagnosis of breast cancer in low and middle AUCg women and that, in turn, these patients may be especially prone to benefit from interventions of emotional peer support during the cancer process. Hence, AUCg also showed its mediator role in the relationship between emotional intelligence constructs and self-perceived general health in caregivers of people with autism spectrum (Ruiz-Robledillo & Moya-Albiol, 2014), and Sladek et al. (2017) reported that a coping style characterized by greater use of social support predicted flatter average diurnal cortisol slope for young women with attentional avoidance. With regard to the latter group of women, those with high levels of AUCg may need more personalized psychological support to cope with a breast cancer diagnosis, given that it seems that their standard emotional support is not enough to stimulate resilience. This constitutes a challenge in as much as resilience capacity at diagnosis and first stages of the cancer progress can condition posterior health outcomes. According to Tu et al. (2020), trait resilience significantly predicted high levels of perceived growth and health-related quality of life in breast cancer patients. Kourou et al. (2021) also identified low resilience as a heavy predictor of depression in a sample of 609 women recently diagnosed with breast cancer, and Mohlin et al. (2020) showed that higher levels of psychological resilience were significantly related to increased levels of health-related quality of life in women with newly diagnosed breast cancer. These last authors assert that assessment of resilience at the time of breast cancer diagnosis might enable early detection of women in need of more intense psychosocial support.
Similar to the direction of low resilience scores, high AUCg levels have been related to poorer outcomes in different health contexts. For instance, pre-pandemic AUCg was associated with depression, anxiety levels, and total perceived stress levels reported during confinement in young adults (Baliyan et al., 2021) and AUCg also correlated with anxiety scores in patients with coronary heart disease (Merswolken et al., 2013). Fortunately, neither psychological resilience nor AUCg levels are static or non-regulable factors, and emotional support has shown to have predictive value towards resilience in its own right for our regression model. In this regard, Di Giacomo et al. (2018) found a positive impact on psychological resilience and distress following the emotional patient-oriented support psychotherapy intervention in young breast cancer women. Additionally, Aguilar-Raab et al. (2021) reported that a 3-month mindfulness based group-intervention decreased AUCg levels from pre to post-compared to controls in healthy subjects.
The present study has certain limitations that should not be overlooked. The first one concerns possible bias resulting from the inclusion of a representative sample of Caucasian population, which reduces cross-cultural reproducibility. The second limitation refers to the cross-sectional design of the study, which precludes any inference about the causality and/or directionality of the results as well as the evaluation of the evolution of the variables during the cancer continuum. Finally, we consider that our sample size could limit the generalizability of the results. It would therefore be advisable for future research to expand the sample size in order to explore whether the significance and effect of the size of the results increase.
Clinical Implications
Promoting resilience following a diagnosis of breast cancer is necessary for successful adaptation to illness, and the results presented in this paper highlight the need for personalized care delivery programs targeted at women who have different psychobiological profiles. According to our regression analysis and in line with other authors (Zhang et al., 2017), emotional support plays a fostering role in resilience, suggesting that peer support programs aimed at newly diagnosed breast cancer patients can mitigate the detrimental psychological consequences of the cancer process. However, standard social support programs may not be enough to meet the needs of all breast cancer patients because high diary cortisol secretion seems to hinder the beneficial effect of emotional support on resilience. Therefore, assessing resilience and AUCg levels at diagnosis can be crucial in order to identify those women who would be better assisted with individualized psychotherapy interventions. An individualized approach should not only be aimed at preventing the onset of distress and maladaptive situations, but also at reinforcing adjustment for optimal health under the circumstances.
In conclusion, the explanatory role of social support and AUCg in resilience indicates that certain psychobiological profile influences the vulnerability of women when facing their new reality. On the one hand, women with high AUCg levels may be especially vulnerable to the detrimental effect of receiving a breast cancer diagnosis and may be, in turn, more likely to develop stress-related disorders. On the other hand, women with low and middle levels of AUCg may exploit the beneficial effect that provides emotional support sources on them. Overall, these results provide a framework for assessing psychobiological indicators and detecting vulnerable newly diagnosed breast cancer patients before the onset of maladaptive situations or stress-related disorders.
Footnotes
Acknowledgments
The authors would like to thank the women involved in the present study for their participation. This study was supported by the Basque Government predoctoral grant PRE_2019_1_0041.
Author Contributions
Ms has 3 tables and 2 figures Aizpurua-Perez, I. contributed to conception and design contributed to acquisition, analysis, and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Arregi, A. contributed to conception and design contributed to acquisition and interpretation critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Gonzalez, D. contributed to conception and design contributed to acquisition critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Macía, P. contributed to conception and design contributed to interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Ugartemendia, G. contributed to conception and design contributed to acquisition critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Labaka, A. contributed to conception and design contributed to interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Zabalza, N. contributed to acquisition critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Perez-Tejada, J. contributed to conception and design contributed to acquisition, analysis, and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eusko Jaurlaritza (PRE_2019_1_0041 and IT1447-22).