
Abstract
Objective
To retrospectively analyze the effects of different treatments on cognitive functioning, anxiety, and depression in patients with primary central nervous system lymphoma (PCNSL).
Methods
A comprehensive literature search was conducted in multiple databases including the Cochrane Library, CINAHL, PubMed, Web of Science, EMBASE, Sino Med, Wei Pu, Wan Fang, CNKI, and Google Scholar. The search included studies published through June 20, 2023, focusing on cognitive function, anxiety, and depression in adult patients newly diagnosed with PCNSL. Various measurement tools and scales were used to assess the primary outcomes. Descriptive systematic reviews were conducted to integrate the literature and summarize the effects of different treatment modalities on cognitive functioning, anxiety, and depression in PCNSL patients. This review was registered with PROSPERO (CRD42022370250).
Results
A total of 43 studies were included. Induction chemotherapy was associated with improved cognitive function and reduced anxiety and depression in the majority of patients. Whole-brain radiotherapy (WBRT) was found to lead to cognitive impairment, particularly in executive, attention, memory, and motor function. Low-dose WBRT, autologous stem cell transplantation (ASCT), and blood-brain barrier disruption (BBBD) treatments did not result in significant cognitive impairment. Anxiety and depression were observed to decrease over the long term.
Conclusions
Overall, the cognitive functioning, anxiety, and depression of patients with PCNSL can be improved with appropriate treatments. However, patients treated with WBRT are at a higher risk of cognitive decline compared to those receiving other treatment modalities. Therefore, special attention should be given to patients undergoing WBRT, and a comprehensive analysis should be conducted to reduce neurotoxicity and address early cognitive problems in these patients.
Introduction
Primary central nervous system lymphoma (PCNSL) is a rare non-Hodgkin lymphoma, mainly occurring in people over the age of 60, and predominantly located in the brain, spinal cord, or eyes. It accounts for about 3%∼4% of intracranial tumors (Hoffman et al., 2016). The median overall survival of PCNSL is 1∼9 years (Biccler et al., 2019; Löw et al., 2018). In China, which is a population-based country, PCNSL has a higher prevalence than in the United States (Chen et al., 2022). PCNSL is associated with physical function decline, focal neurological deficits, and cognitive or behavioral changes over weeks or months. Neurotoxicity is a common complication in survivors, highlighting the importance of cognitive improvement for their long-term quality of life. Currently, the main treatments for PCNSL include high-dose methotrexate (HD-MTX), whole body radiotherapy (WBRT), autologous stem cell transplantation (ASCT), or blood-brain barrier disruption (BBBD). Conventional chemotherapy with HD-MTX has been shown to reduce neurotoxicity incidence and improve survival compared to WBRT alone (Doolittle, Dósa, et al., 2013; Ferreri et al., 2022; Rubenstein et al., 2013). Cognitive function plays a crucial role in daily living activities and can significantly impact the economic burden on families and society. Additionally, psychological changes in PCNSL should be carefully considered in clinical practice. Studies have shown that experiencing illness in life may lead PCNSL patients to reexamine their priorities and have a more positive view of life (Pertz et al., 2021), and patients who resumed work experienced fewer symptoms impacting their quality of life (Wiemann et al., 2020). Cognitive function and mental health are closely linked (Bai et al., 2023; Gehring et al., 2015), and cognitive training can significantly improve psychological health (Poggi et al., 2009). By considering the relationship between cognitive function and psychology, healthcare professionals can provide targeted care interventions to patients undergoing different treatments, enhancing treatment outcomes.
To address the gaps in the current literature, this systematic review aims to comprehensively explore the impact of various therapies on cognitive functioning, anxiety, and depression in adult patients with newly diagnosed PCNSL. The review includes a comparative analysis of subjective and objective cognitive function, with a focus on treatments and outcomes. By conducting a comprehensive search of English and Chinese language databases, this review provides a theoretical basis for targeted interventions and contribute to the understanding of the effects of different treatments on cognitive function, anxiety, and depression in PCNSL patients.
Methods
Search Strategy
To find literature on cognition, anxiety, and depression in PCNCL, we conducted an extensive search for articles published up until June 20, 2023. We searched five English databases, including Cochrane Library, CINAHL, PubMed, Web of Science, and EMBASE, and 4 Chinese databases, namely Sino Med, Wei Pu, Wan Fang, and China National Knowledge Infrastructure (CNKI). In our search, we used the following Mesh terms and free words: central nervous system/Cerebrospinal Axi*/intraocular/brain*/cerebral*/spine/spinal, Lymphoma/Lymphoma*, cognition/cognit*/learning/memory/language*/reading*/neurocongniti*/cognitive function/cognitive performance/cognitive abilit*/cognitive dysfunction/cognitive impairment*/cognitive disorder*/cognitive complaint*/cognitive failure, anxiety/depression/depressive/psychology/psychosocial/psycholog*/emotion*/mental health/psychological disorders/psychological diseases/depressive disorder/mental disorders/mood disorder/emotional disorder/affective disorder/affective disturbance. displays the search terms using PubMed as an example. A flow chart of search terms.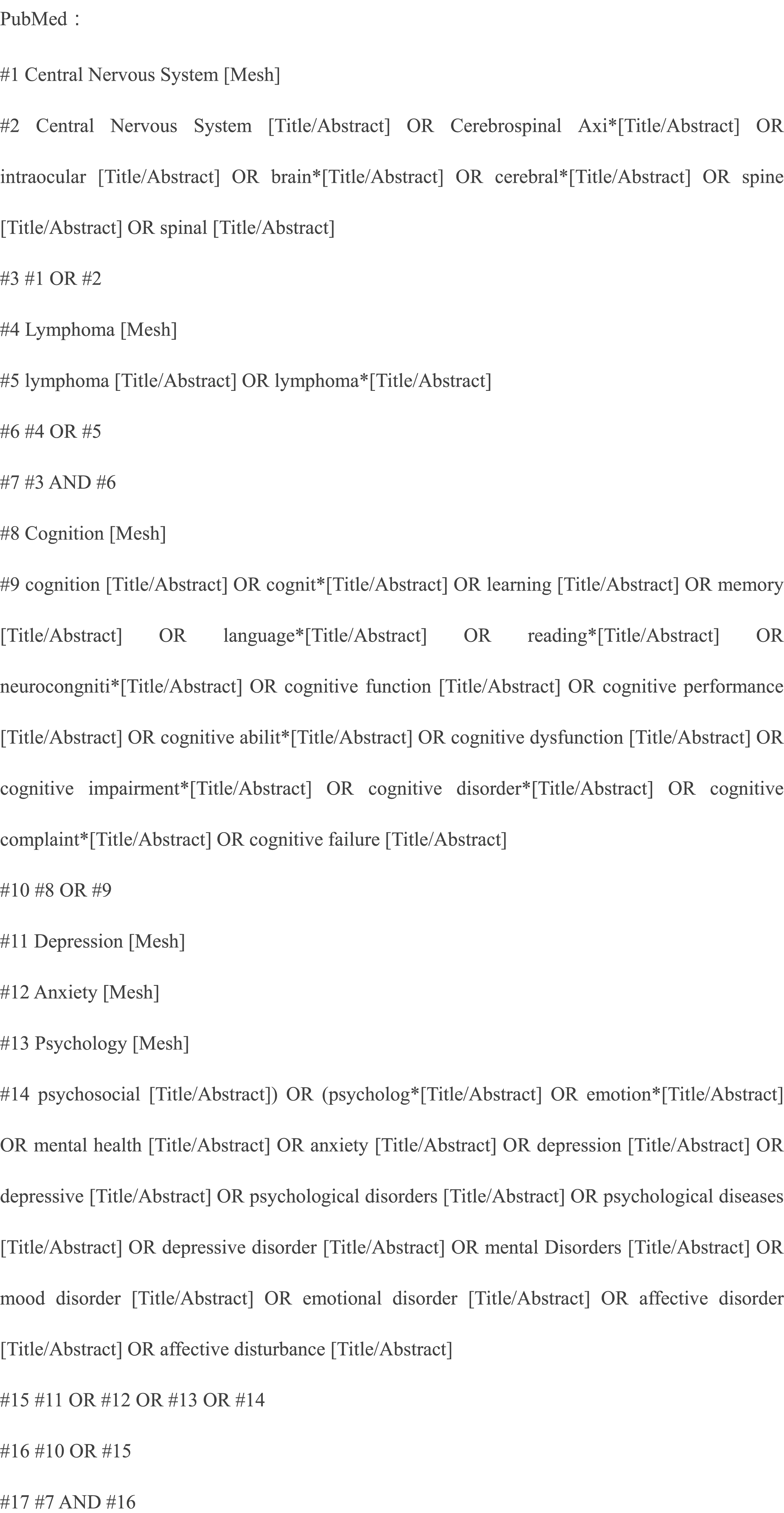
Inclusion Criteria for Study Selection
Studies were reviewed if they met the inclusion criteria: (1) addressed people with newly diagnosed PCNSL, (2) measured cognition functioning, anxiety, and depression through tools with reliable results: objective measures of cognition used neuropsychological tests and appraised cognitive performance; subjective cognitive function was assessed using self-report questionnaires about cognitive function in the real world, such as MMSE (mini-mental state examination), and MoCA (Montreal Cognitive Assessment), the total score is calculated based on the score of each item, appraising the effects of cognitive function on the personal life and functioning in daily life. The higher the score, the better the cognitive functioning. Anxiety and depression were estimated by the Beck Depression Scale (BDI), the Brief mood introspection scale (BMIS), the Hospital Anxiety and Depression Scale (HADS), and the Apathy Rating Scale. Lower scale scores indicate milder anxiety and depression symptoms. Different tools are valid and reliable in PCNSL. There were no restrictions on study design and treatment modes, including chemotherapy, radiotherapy, autologous stem cell transplantation, and blood-brain barrier disruption therapy. Studies were excluded based on the following criteria: (1) participants with a history of secondary tumors or psychiatric disorders, (2) the language of the publication was other than English or Chinese, (3) unable to obtain full text or duplicate publications, systematic reviews and meta-analyses.
Two researchers who had undergone systematic evidence-based nursing studies independently screened and reviewed seven aspects of systematic reviews and meta-analyses, including title, abstract, introduction, methods, results, discussion, and funding. A form was prepared for data collection, and two graduate students independently screened texts and judged whether the studies should be included or excluded. If necessary, consultation with a third senior examiner was done. When the two researchers disagreed, this was resolved through discussion or consulting the definition of the interpretation. All three researchers were fluent in English.
Data Extraction
For each study design, we extracted information including the author, year of publication, sample characteristics, and outcomes. The assessment time, tests, or questionnaires used for measuring cognition, anxiety, and depression were also recorded, along with the extracted results. To indicate the presence and severity of cognitive impairment, outcome measures were extracted from literature data and raw scores or converted into Z-scores of the neuropsychological tests.
Findings
The search yielded 3204 articles. A PRISMA Flow Diagram in Figure 2 was adopted and used as a preferred reporting item for systematic reviews. Of the 78 articles assessed for further eligibility, 43 articles were included. Most articles were excluded due to small sample sizes, cognition not being formally tested or measured, and anxiety or depression not being assessed using questionnaires or tests. The appendix (supplementary material) describes the characteristics of 43 eligible articles in Tables 1–3. Of the 42 included studies on cognitive functioning, 24 measured objective cognitive performance, including digital span, trail-making test, conversion speeds, and complex figure test (Abrey et al., 2003; Correa et al., 2019; Correa et al., 2004; Correa et al., 2009; Correa et al., 2012; Dahlborg et al., 1996; Doolittle, Dósa, et al., 2013; Ferreri et al., 2017; Fliessbach et al., 2005; Fliessbach et al., 2003; Juergens et al., 2010; McAllister et al., 2000; Morris et al., 2013; Neuwelt et al., 1991; Neuwelt et al., 2005; Nilles et al., 2022; Omuro, Chinot, et al., 2015; Omuro, Correa, et al., 2015; Pels et al., 2003; Pertz et al., 2021; Schlegel et al., 2001; Shah et al., 2007; van der Meulen et al., 2021; Wiemann et al., 2020). 14 studies examined only subjective cognitive functioning (Batchelor et al., 2003; Chanswangphuwana et al., 2018; Fisher et al., 2005; Gao et al., 2016; Glass et al., 2016; Herrlinger et al., 2017; Illerhaus et al., 2016; Illerhaus et al., 2008; Kaburaki et al., 2017; Kiefer et al., 2012; Laack, Ballman, Brown, & O'Neill, 2006; Laack et al., 2011; O’Neill et al., 1999; Shan et al., 2014). The effect of treatment on both outcomes was described in 4 articles (Ferreri et al., 2022; Houillier et al., 2019; Ichikawa et al., 2014; Nilles et al., 2022). Objective cognitive functioning primarily includes executive function, attention, memory, language, and visuospatial ability. Subjective cognitive function assessment mainly used MMSE, and MoCA. In addition, several articles used the MDRS (Mattis Dementia Rating Scale), or ADAS (Alzheimer’s disease assessment scale). Studies have shown that dementia scores are effective in predicting cognitive decline (Woolf et al., 2016), and the sensitivity and specificity for identifying cognitive decline are similar to MoCA (Zhuang et al., 2021). Therefore, this study included it as a subjective cognitive measurement. Among them, the higher scores of MMSE, MoCA, and MDRS scales indicate greater cognition, while patients with higher ADAS scores tend to have more severe cognitive impairment. To measure anxiety and depression, authors used the BDI, the BMIS, the HADS, and/or the Apathy Rating Scale. The sample size ranged from 10 to 144 patients, with 34 articles solely describing cognitive functioning, one article solely assessing the effects on anxiety or depression, and eight articles showing the cognitive and emotional results for newly diagnosed PCNSL patients. Seven trials were randomly controlled studies (RCTs), and the remaining were cohort studies. We divided the kinds of literature according to treatment modality: radiotherapy alone (n = 1), chemotherapy or immunochemotherapy only (n = 6), intravenous or intrathecal chemotherapy (n = 5), chemotherapy in combination with WBRT (n = 16), chemotherapy in combination with autologous stem-cell transplantation (n = 4), chemotherapy combined with blood-brain barrier disruption (n = 5), and six direct comparisons of treatment options. PRISMA flow chart.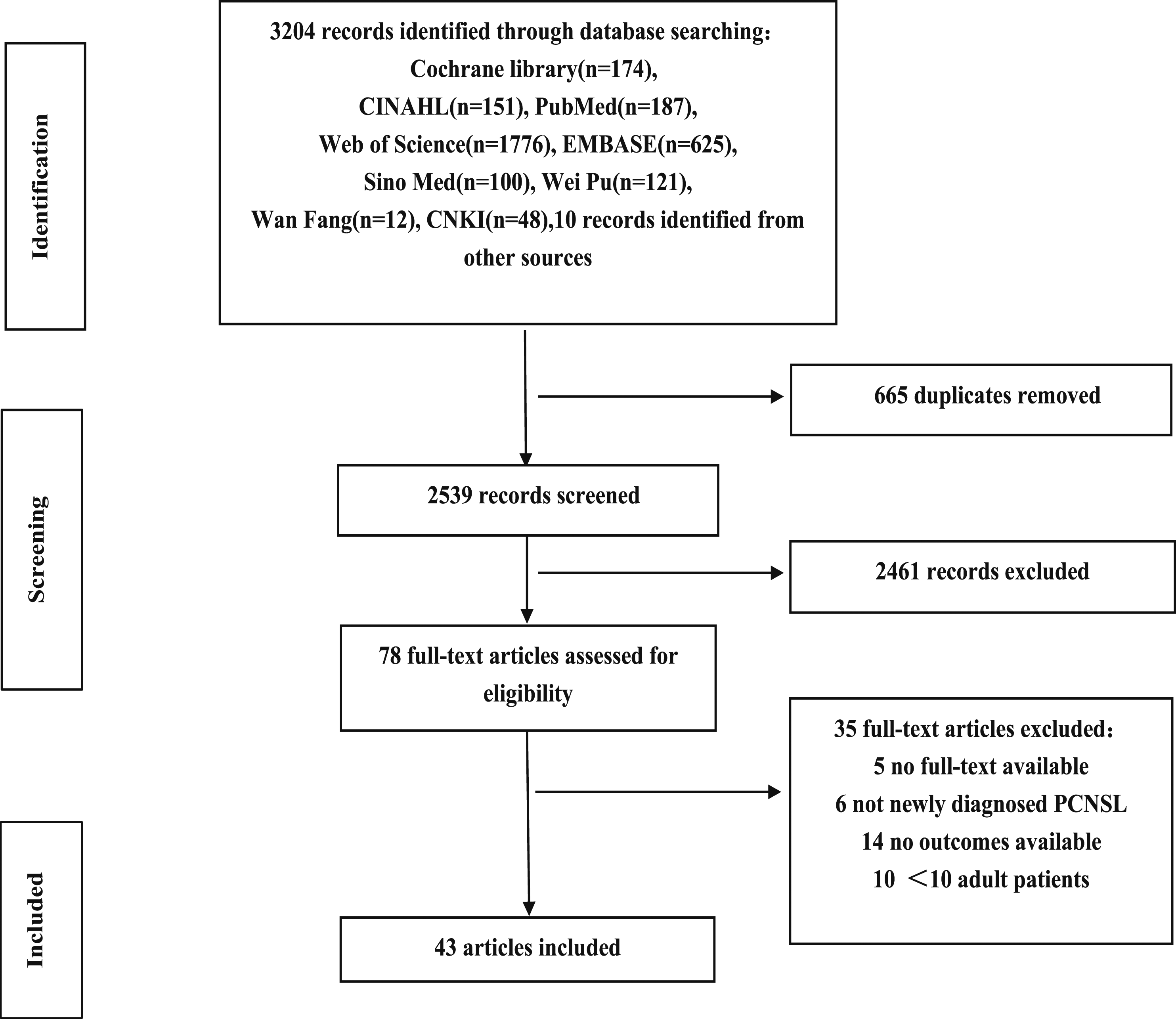
Cognitive Function
Chemotherapy or Immune-Chemotherapy
Six trials examined the impact of chemotherapy or immunochemotherapy on cognitive function. Among these trials, two used the MMSE and ADAS tests and concluded that there was no significant change in cognition, except for a slight decrease in ADAS scores (Batchelor et al., 2003; Nilles et al., 2022). In 5 studies, attention, language, executive, and memory domains were the main focus (Nilles et al., 2022; Omuro, Chinot, et al., 2015; Pertz et al., 2021; van der Meulen et al., 2021; Wiemann et al., 2020). Regarding the assessment of cognitive function through MDRS, one study found that it remained stable during a 16-month follow-up period (Omuro, Chinot, et al., 2015). Similarly, in another study with a median follow-up of 48 months, all cognitive domains showed improvement except for episodic memory. Furthermore, one study showed that chemotherapy did not have an adverse effect on final outcomes (van der Meulen et al., 2021), and there was even an improvement in responsiveness after a 2-year follow-up. A direct comparison between PCNSL patients and healthy controls in terms of cognitive functioning revealed impairment in overall intelligence (Pertz et al., 2021; Wiemann et al., 2020). Z scores were consistently worse (≤−1.5) compared to the general population. In summary, although the cognitive functioning of patients generally declined compared to healthy individuals, most patients either remained stable or experienced improvement after undergoing chemotherapy or immunochemotherapy.
Intravenous or Intrathecal Chemotherapy
In summary, except for those over 60 years old, there was cognitive decline. Five studies reported that all patients were treated with either intravenous or intrathecal chemotherapy. Three other studies found cognitive functioning remained stable on the long-term effects of therapy, ranging from 86 to 109, but scores were lower in people over 60 years. Two articles tested attention and executive, visuospatial, language, and memory functions. One study showed a decline in memory, from 102.3 to 88.5, with remaining functions stable or improving. Intravenous or intrathecal chemotherapy did not affect cognitive function in most patients. (Fliessbach et al., 2003; Juergens et al., 2010; Pels et al., 2003; Schlegel et al., 2001).
Radiotherapy
In one small study conducted by Gao et al. (2016) with a population mainly consisting of elderly individuals and using the MMSE, the effect of low-dose radiotherapy alone on cognitive functioning was investigated. The study included 16 participants. The results demonstrated that cognition remained largely stable compared to the baseline after radiotherapy, and the majority of patients showed stability in their cognitive functioning. Furthermore, a 1-year follow-up indicated no adverse effects of low-dose radiotherapy on cognition. Therefore, it can be concluded that low-dose radiotherapy had no significant impact on cognition.
Chemotherapy Combined With WBRT
Cognitive function after a combination of chemotherapy and radiotherapy was studied in 16 articles, with a specific focus on MMSE and MoCA scores. The short-term impact of WBRT on cognition remained stable, as indicated by studies conducted by Ichikawa et al. (2014), Laack et al. (2011), and O'Neill et al. (1999). However, long-term follow-up trials have reported worse outcomes for patients after WBRT, with MMSE scores decreasing from 28 to 22 (Chanswangphuwana et al., 2018; Fisher et al., 2005; Herrlinger et al., 2017; Laack, Ballman, Brown, & O’Neill, 2006; Nilles et al., 2022). On the contrary, Kaburaki et al. (2017) found that WBRT treatment resulted in higher MMSE scores. Six studies assessed attention, executive function, memory, language, motor skills, and visuoconstruction. Of these, three studies demonstrated short-term improvements with low-dose radiotherapy, which aligns with the subjective cognitive results reported (Correa et al., 2009; Morris et al., 2013; Shah et al., 2007). However, PCNSL patients receiving chemotherapy combined with WBRT showed impairments in attention and verbal memory, as observed in studies by (Correa et al. 2004, 2012). Moreover, after 2 years, areas other than language and visuoconstruction were significantly impaired, with an increased likelihood of neurotoxicity (Ichikawa et al., 2014). In conclusion, the combination of WBRT and chemotherapy has a significant impact on patients’ cognition, particularly in terms of attention, language, and memory impairments, and it also increases the risk of neurotoxicity.
Chemotherapy Combined With ASCT
Four studies were published describing the effects of chemotherapy combined with ASCT (Abrey et al., 2003; Illerhaus et al., 2016; Illerhaus et al., 2008; Omuro, Correa, et al., 2015). Two of these studies evaluated subjective cognition over a long period and reported an improvement in MMSE scores (ranging from 25 to 29; Illerhaus et al., 2016; Illerhaus et al., 2008). The other two articles investigated attention and executive, memory, and language functions. After a median follow-up of 28 months, improvements in all areas were observed as a result of this treatment (Abrey et al., 2003). However, it should be noted that 1-2 years after treatment, the rate of improvement in attention, executive function, and language function subsequently slowed down, and no significant impairment was observed in the remaining areas (Omuro, Correa, et al., 2015). Therefore, based on these findings, it can be concluded that ASCT combined with chemotherapy had no significant effect on cognition.
Chemotherapy Combined With Blood-Brain Barrier Disruption
Five trials (n = 9–24) reported results on objective cognition in patients receiving chemotherapy combined with blood-brain barrier disruption (Doolittle, Dósa, et al., 2013; Ferreri et al., 2017; McAllister et al., 2000; Neuwelt et al., 2005). These studies assessed attention and execution, memory, and language. Among them, two studies reported stable cognitive function, including in elderly patients (over 60 years) (Dahlborg et al., 1996; McAllister et al., 2000). In addition, three studies observed an improvement in cognitive function after treatment. Specifically, one article showed a significant improvement in attention and executive function, but not in memory and language (Ferreri et al., 2017; Neuwelt et al., 2005). Moreover, 4 articles reported no reduction in motor function, as assessed through finger percussion and grip strength testing at the end of the treatment involving high doses of methotrexate in combination with BBBD (Dahlborg et al., 1996; Doolittle, Dósa, et al., 2013; McAllister et al., 2000; Neuwelt et al., 2005). In summary, the findings suggest that BBBD combined with chemotherapy does not have a negative impact on cognitive functioning and remains stable.
Multiple Treatment Modalities in Direct Comparison
In conclusion, six trials directly compared the effects of different therapies on cognition. Three randomized controlled trials (RCTs) found that patients treated with ASCT had higher scores, indicating cognitive improvement. Ferreri et al. (2017) also showed improvements in cognitive function at the last follow-up. Four articles compared the comprehensive situation, attention, memory, language, and motor speed of patients given chemotherapy combined with WBRT or ASCT. These studies found an improvement in most patients after two consolidation therapies, in line with subjective cognition. However, three studies reported impairment in attention, executive function, and memory between these treatment modalities during three or 5 years of follow-up. Furthermore, a study comparing different treatment modalities revealed poorer attention, execution, verbal memory, and motor speed in patients treated with WBRT after achieving CR. Therefore, while patients receiving WBRT therapy experienced cognitive impairment, other patients’ cognition was either unaffected or even improved.
Relationship Between Subjective and Objective Cognition
In an RCT conducted by Houillier et al. (2019), most patients who underwent ASCT treatment had no detrimental effects on subjective and objective cognition. On the other hand, patients who received WBRT experienced worsened cognition, specifically with regard to executive function and comprehensive situation. Similarly, Ferreri et al. (2022) discovered inconsistencies in subjective and objective outcomes. Specifically, patients treated with ASCT had lower MMSE scores compared to the WBRT group. However, the same study also revealed that patients in the ASCT group exhibited remarkable improvements in attention, executive function, and memory function. Furthermore, there were 4 studies that simultaneously assessed subjective cognitive function and objective cognitive performance. Of these studies, two reported that chemotherapy had no negative impact on subjective and objective cognitive functioning. In fact, memory and executive function were found to be improved in these individuals (Ichikawa et al., 2014; Nilles et al., 2022).
Anxiety and Depression
Chemotherapy or Immunochemotherapy
Two studies reported the psychological status of patients receiving chemotherapy or immunochemotherapy (Fliessbach et al., 2003; Pels et al., 2003). Fliessbach et al. (2003) showed that BDI scores were worse in patients with PCNSL (PCNSL 9.8 vs. control 5.3). However, the BDI scores improved after a median follow-up of 35 months. Likewise, using the HADS, Pels et al. (2003) reported lower scores in patients who returned to work (anxiety 6.0 vs. 4.63, depression 5.12 vs. 3.13). These findings suggest that chemotherapy or immunochemotherapy did not affect anxiety, and anxiety decreased at long-term follow-up.
Intravenous or Intrathecal Chemotherapy
In a small study (n = 23) conducted by Juergens et al. (2010), anxiety and depression were examined in individuals who received intravenous or intrathecal chemotherapy. The study found that the majority of patients experienced improved recovery compared to their pre-treatment state. However, after a median follow-up period of 44 months, 4 patients demonstrated signs of depression (as indicated by BDI scores ≥ 13). The study also showed a strong correlation between neuropsychological test results and levels of anxiety and depression (r = .622), with higher cognition scores being associated with lower levels of anxiety.
Chemotherapy Combined With WBRT
Three studies evaluated the anxiety and depression of people treated with chemotherapy combined with WBRT. Two of those studies used the Beck Depression Scale (Correa et al., 2009; Morris et al., 2013), and one study used the Brief Mood Introspection Scale (Adhikari et al., 2018). Correa et al. (2009) reported no significant change in scores over time, with scores ranging from six to 8. In contrast, a longitudinal study by Morris et al. (2013) showed a gradual reduction in depression scores, from eight to 5.1. On the other hand, Adhikari et al. (2018), using the Brief Mood Introspection Scale, reported a fluctuating pattern of mood, with scores initially rising and then decreasing (43.5, 47, 48, 37). In summary, the findings from these studies indicate that WBRT did not have a significant impact on anxiety and depression in patients.
Multiple Treatment Modalities in Direct Comparison
One study found that WBRT treatment did not affect the mood of patients (Correa et al., 2012). Respectively, two studies utilizing the Marlin Apathy Scale and the Beck Depression Scale observed good performances by patients (Correa et al., 2019; Houillier et al., 2019). Furthermore, the patients treated with ASCT demonstrated even better results. In summary, neither ASCT nor WBRT had any detrimental effects on anxiety and depression.
Discussion
Heterogeneity of Studies
Forty-three articles have been included in this review. Methotrexate is the protocol established in the 1980s for patients, blended with additional care that can pass the blood-brain barrier. Moreover, there are differences in the relationship between different drugs and cognitive functioning. The tools reviewed in this article used different rating methods. MMSE or MoCA was the predominant subjective cognitive screening tool. On the other hand, objective cognition was measured by various methods. However, due to differences in measurement tools, rating methods, and insufficient data, these studies would not be suitable for meta-analysis.
Combined Tests Should be Used to Evaluate Objective Cognition in Patients With PCNSL
Cognitive function was assessed in several areas, focusing on attention and execution, memory, language, visuoconstruction, and motor speed. Attention and execution function were evaluated using the Trail Making Test (Abrey et al., 2003; Adhikari et al., 2018; Correa et al., 2019; Correa et al., 2009; Dahlborg et al., 1996; Doolittle, Dósa, et al., 2013; Ferreri et al., 2022; Houillier et al., 2019; McAllister et al., 2000; Neuwelt et al., 1991; Neuwelt et al., 2005; Omuro, Correa, et al., 2015; Shah et al., 2007). This test consists of parts A and B. TMT-A mainly measures psychomotor speed and visual attention, while TMT-B assesses cognitive alternation and set-shifting abilities. Memory function was evaluated using the Hopkins Verbal Learning Test (Abrey et al., 2003; Correa et al., 2019; Correa et al., 2012; Doolittle, Dósa, et al., 2013; Morris et al., 2013; Omuro, Correa, et al., 2015; Poggi et al., 2009; Shah et al., 2007). This test involves the patient reading and then recollecting 12 words after three consecutive studies. It consists of three immediate free recall scores, a delayed free recall score, delayed recognition score, and discrimination scores, and provides a comprehensive analysis of the patient’s memory function. Verbal Fluency was mostly used to assess language function (Abrey et al., 2003; Correa et al., 2012; Ferreri et al., 2017, 2022; Shah et al., 2007), which is defined as “the ability to shape and express words according to the required criteria” and is essential for communication. The assessment of visuoconstruction relies on the Rey-Osterreith complex figure test (Dahlborg et al., 1996; Ferreri et al., 2017, 2022; Ichikawa et al., 2014; McAllister et al., 2000; Neuwelt et al., 1991, 2005), a recognized visuospatial and visual memory test that effectively assesses neuropsychological dysfunction. Motor speed was measured using the Grooved Pegboard Test (Abrey et al., 2003; Correa et al., 2019; Correa et al., 2009; Correa et al., 2012; Doolittle, Korfel, et al., 2013; Ferreri et al., 2017; Morris et al., 2013; Omuro, Correa, et al., 2015; Shah et al., 2007; van der Meulen et al., 2021), which is a manual dexterity test that records the time it takes to complete the test using dominant and non-dominant hands. The combination of these measurement tools allows for a comprehensive assessment of cognitive function, ensuring sensitivity and specificity.
Treatment With WBRT Exhibited the Most Evident Impairment of Cognitive Function
Prior treatment strategies for PCNSL include high-dose chemotherapy with consolidative WBRT. However, this approach is significantly associated with neurological impairment, especially in older adults. MTX is currently one of the standard treatments for PCNSL, supported by studies conducted in the Netherlands and other countries. The Chinese Society of Clinical Oncology guidelines recommend WBRT as the best option for induction therapy when systemic chemotherapy is not suitable (Zhu & Ma, 2021). Another treatment option is BBBD developed by Neuwelt et al. (1991), which has acceptable toxicity. Additionally, ASCT is a new type of consolidation therapy suitable for patients under 70 years old with good physical function (Ferreri & Illerhaus, 2016). HD-MTX has been shown to be an effective therapeutic option for PCNSL, as demonstrated in several studies (Correa et al., 2007; David et al., 2023). Long-term WBRT treatment has been found to adversely affect cognition, and induction chemotherapy, reduced-dose radiotherapy, ASCT, or BBBD can enhance cognition to some extent. Various studies have shown mixed results regarding the cognitive effects of WBRT. Some studies reported a decline in subjective cognition and negative impact on attention and speech memory, while others did not find short-term cognitive impairments. Lowering the radiation dose was not found to have side effects on cognition. It is important to note that the timing and dose of radiotherapy may influence cognitive functioning, and cognitive function may fluctuate in patients treated with WBRT. Furthermore, previous studies have shown that brain volumes and white matter lesions are susceptible to degradation associated with neurological function loss due to radiotherapy (van der Meulen et al., 2021). Therefore, it is crucial to focus on monitoring cognitive changes, early recognition of cognitive impairment, and active intervention in PCNSL patients receiving WBRT.
The Correlation Between Subjective and Objective Cognitive Functioning is Low
The International Working Group on Cognition and Cancer recommends integrating subjective and objective cognitive evaluation tools and using test kits to increase detection rates and enhance scientific rigor. In 2018, the researchers indicated that MMSE or MoCA lack sensitivity to evaluate cognition and may underestimate the incidence of cognition deterioration. Imaging studies have also found that the hippocampus and cortical function in cancer patients are more associated, and the brain may maintain individual performance on cognitive tests through compensatory mechanisms, which explains the difficulty of identifying cognitive changes or deficits in cancer by subjective tests (Apple et al., 2018). Four studies (Ferreri et al., 2022; Houillier et al., 2019; Ichikawa et al., 2014; Nilles et al., 2022) in this review found inconsistent subjective and objective cognitive performance. Neuropsychological tests have benefits in particular cognitive areas. MMSE and MoCA as cognitive screening tools lack the sensitivity to detect cognitive impairment.
Patients With PCNSL Receive Treatment That Improves Their Anxiety and Depression
Analysis of different treatment modalities shows that compared with healthy people, PCNSL patients receiving immunochemotherapy have psychological disorders, delayed return to work, and a subsequent decline. Several studies in this review demonstrated improvement in anxiety and depression (Nilles et al., 2022; Pertz et al., 2021; Wiemann et al., 2020). The psychological state of patients receiving intravenous or intrathecal chemotherapy was enhanced. Likewise, BDI scores were stable in patients treated with WBRT over the long-term follow-up (Correa et al., 2012). Another study reported ASCT treatment as an alternative to WBRT, with both combinations enhancing psychological status (Houillier et al., 2019).
Cross-Sectional Studies Integrated With Longitudinal Studies
One study conducted subjective cognitive tests at the end of ASCT treatment, and results demonstrated 90% of patients had normal cognition functioning (Illerhaus et al., 2008). Comparable to another prospective study (Illerhaus et al., 2016), subjective cognitive scores gradually rise during the treatment. Two cross-sectional studies were evaluated at the end of treatment, results proved that the patients treated with WBRT have better scores in visual construction than the ASCT group (Correa et al., 2004, 2012). However, all other cognitive domains have impairments, and people in the WBRT group had the least efficient and were more prone to neurotoxicity (Correa et al., 2009; Ichikawa et al., 2014; Morris et al., 2013; Shah et al., 2007). Furthermore, there was a cross-sectional study comparing WBRT with ASCT (Kiefer et al., 2012), and results revealed that patients treated with WBRT had lower scores, as with a longitudinal study (Houillier et al., 2019). Contradicting these findings, other research showed that people who had WBRT treatment were shown to enhance their cognitive scores more (Ferreri et al., 2022). In addition to subjective cognitive measures, two studies measured objective cognitive performance in people who had immunochemotherapy at a single point in time (Pertz et al., 2021; Wiemann et al., 2020). When compared to healthy individuals, all cognitive domains showed deterioration. However, in long-term follow-up, except for a minor reduction in DSF (Nilles et al., 2022), the remaining cognitive functions improved (Omuro, Chinot, et al., 2015; van der Meulen et al., 2021). Several cross-sectional studies merely depict outcomes at the end of treatment, and their baseline data are insufficient to infer cognitive changes over time. Therefore, the long-term effects of treatment are difficult to determine. To address this limitation, integrating longitudinal research can help observe trends and identify specific points where medical staff can intervene, thereby facilitating the recovery of patients.
Conclusion
As we evaluated the literature, there were differences in study design, measurement instruments, and outcomes, leading to a significant degree of heterogeneity. Due to this heterogeneity, it was not possible to conduct a quantitative analysis of cognition and psychological states. Additionally, many studies lacked clarity regarding the time of testing, and there was insufficient baseline data to determine if there were any differences in outcomes. Furthermore, the high drop-out rates among patients during long-term follow-ups posed challenges in determining the effects. To improve future research, it is necessary to standardize measurement instruments and outcomes to enhance the study design and research quality. Moreover, further investigation into the effects of different doses of radiotherapy on cognitive functioning and psychology in PSNCL is warranted.
Supplemental Material
Supplemental Material - A Systematic Review of Cognitive Function, Anxiety, and Depression in Patients With Newly Diagnosed Primary Central Nervous System Lymphoma
Supplemental Material for A Systematic Review of Cognitive Function, Anxiety, and Depression in Patients With Newly Diagnosed Primary Central Nervous System Lymphoma by Ziyu Liu, Jingming Zhuang, Li Wei, Aiwen Lu, Jiangang Hou, and Xiaoli Yang in Biological Research for Nursing.
Footnotes
Author Contributions
Liu Ziyu collected all the contributions, interpreted and summarised the literature, and wrote the manuscript. Zhuang Jingming contributed to drafting and designing the manuscript, interpreting the literature, and carrying out a critical revision of the manuscript. Wei Li, and Lu Aiwen helped interpret the literature and revise the manuscript. Contributed to the conception and design of the study, critically revising the manuscript and supervising the study by Yang Xiaoli and Hou Jiangang. This version of the manuscript has been approved by all authors. Liu Ziyu contributed to conception and design contributed to analysis and interpretation drafted manuscript. Select item gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Zhuang Jingming contributed to interpretation drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Wei li contributed to analysis drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Lu Aiwen contributed to analysis drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Yang Xiaoli contributed to conception contributed to acquisition critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Hou Jiangang contributed to conception contributed to acquisition critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the national natural science foundation of China (81771683) and the Fudan University-Fosun Nursing Research Fund Project (FNF202218).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.