
Abstract
Background/Aims
Patients with irritable bowel syndrome (IBS) often report upper gastrointestinal (GI) (e.g., nausea and heartburn), somatic, and emotional symptoms. This study seeks to examine the relationships among younger and older women with IBS and indicators of autonomic nervous system (ANS) function and daily nausea and heartburn symptoms.
Methods
Women were recruited through clinics and the community. Nocturnal heart rate variability (HRV) was obtained using ambulatory electrocardiogram Holter monitors. Individual symptom severity and frequency were collected using 28-day diaries. All variables were stratified by younger (<46 years) and older (≥46 years) age groups.
Results
Eighty-nine women with IBS were included in this descriptive correlation study (n = 57 younger; n = 32 older). Older women had reduced indices of vagal activity when compared to younger women. In older women, there was an inverse correlation between nausea and vagal measures (Ln RMSSD, r = −.41, p = .026; Ln pNN50, r = −.39, p = .034). Heartburn in older women was associated with sleepiness (r = .59, p < .001) and anger (r = .48, p = .006). Nausea was significantly correlated with anger in the younger group (r = .41, p = .001). There were no significant relationships between HRV indicators and nausea and heartburn in younger women.
Conclusions
Age-related differences in ANS function that are associated with nausea may portend unique opportunities to better understand the vagal dysregulation in women with IBS.
Introduction
Irritable bowel syndrome (IBS) is a chronic and common gastrointestinal (GI) disorder of gut-brain interaction (DGBI) with symptoms of abdominal pain and changes in defecation (Camilleri, 2021; Drossman et al., 2018; Lacy et al., 2021). It imposes a significant burden to the affected individuals and the healthcare system. IBS substantially impacts patients’ overall well-being, including their social life, work performance, and quality of life and, as a result, people with IBS often report emotional distress symptoms (Camilleri, 2021; Shiha et al., 2021; Yang et al., 2022). In addition, people with IBS often experience and report somatic symptoms including headache, back pain, and joint pain (Shiha et al., 2021; Jarrett et al., 2014). While abdominal pain and altered bowel habits are the primary IBS symptoms, people with IBS often report increased severity of nausea and upper GI symptoms in both fasting and postprandial conditions compared to healthy controls (Steinsvik et al., 2020). Patients with IBS who have concomitant functional upper GI symptoms (e.g., nausea, heartburn) often have more severe IBS symptoms, higher psychological symptom intensity, and worse quality of life than those without functional upper GI symptoms (Lee & Chang, 2021; Nam et al., 2021). Furthermore, the presence of multiple DGBIs and/or other functional somatic syndromes, i.e., ‘overlapping conditions’ often lead to additional diagnostic tests and interventions (Sperber et al., 2022). Understanding the pathophysiologic basis for overlapping symptoms or conditions across the age spectrum is a growing area of investigation. One of the potential pathophysiologic factors is dysregulation of the autonomic nervous system (ANS).
Surveys of the general population have shown that the presence and severity of IBS as well as other GI symptoms increase and decrease depending on an individual’s age (Houghton et al., 2016). In 2021, a multinational survey study with 73,076 adults from 33 countries found that IBS prevalence decreased with age, though it still remained substantially higher in women (Sperber et al., 2021). Similarly, researchers who conducted a health survey with adults in the general population reported that nausea was independently associated with younger age (Aziz et al., 2019). In contrast, reports of heartburn increase with age (Maret-Ouda et al., 2020). It can be conjectured that younger persons with IBS are more likely to report nausea while older adults are more likely to report heartburn on a daily basis. The pathophysiological and/or psychological basis for these age-related differences in symptoms remains to be resolved.
Autonomic nervous system dysregulation is common among IBS patients (Ruschil et al., 2021). Several investigators have demonstrated reduced heart rate variability (HRV) reflecting decreased parasympathetic input in adults with IBS, particularly those with constipation (Cain et al., 2007; Sadowski et al., 2020). HRV values have been used to quantify ANS regulation and stratify determinants associated with GI disorders (e.g., IBS and DGBIs) and non-GI disorders (e.g., somatic symptoms and emotional distress) (Malik et al., 1996; Ying-Chih et al., 2020). HRV indices are influenced by age, gender, emotional state, and time of day (Natarajan et al., 2020; Schneider & Schwerdtfeger, 2020). The time domain of HRV indicators reduce with age (Natarajan et al., 2020) necessitating the importance of considering age in studies using HRV.
Understanding of the pathophysiology of functional nausea is limited, but is described as multifactorial, involving ANS dysfunction, physical or emotional distress, gastric dysrhythmias, and altered central nervous system processing (Babic & Browning, 2014; Caillet et al., 2022; Cangemi & Kuo, 2019). The ANS, particularly the vagus nerve, modulates essential functions (e.g., motility, secretion) in the upper portions of the GI tract (e.g., esophagus and stomach) (Bonaz et al., 2021). Antiemetic serotonin receptor blockers which reduce nausea in adults also inhibit GI vagal activity, suggesting that vagal activity is linked to nausea (Cangemi & Kuo, 2019; Theriot et al., 2020). Caillet et al. (2022) studied the relationship between HRV indices and nausea severity among individuals between 13 to 31 years of age who experienced functional abdominal pain. They observed that the high-frequency component of HRV decreased in females as nausea severity increased. An opposite pattern was observed in male participants, i.e., as their high-frequency component of HRV increased the nausea severity increased (Caillet et al., 2022). Whether a similar relationship between vagal indicators and nausea exists in older women is not known. It can be hypothesized that age-related decreases in vagal input are linked to possible age-related differences in upper GI symptoms.
This current study focused on comparing daily heartburn and nausea by age (younger vs. older) and examining the relationships between upper GI symptoms (e.g., heartburn and nausea) and the severity of IBS symptoms (i.e., abdominal pain, diarrhea, and constipation) among women with IBS. In addition, we evaluated the associations between upper GI, somatic, and emotional symptoms and ANS indices. We hypothesized that the indicators of ANS, such as reduced parasympathetic indices, would be more strongly associated with upper GI, somatic, and emotional symptoms in older women compared to younger women.
Methods
Design
This correlational descriptive study of upper GI symptoms, somatic symptoms, and emotional distress used baseline HRV indicators collected before starting a nurse-led behavioral intervention (2008–2013) in persons with IBS, which has been described elsewhere (Jarrett et al., 2016).
Setting and Population
Women with IBS were recruited through community advertisements and GI clinics, including pamphlets, air broadcasting, and mailings, in a northwest metropolitan region of the United States. Potential participants were screened with a telephone interview. The qualifications for trial inclusion were evaluated across a 5-week baseline assessment period including an in-person interview, 4-week daily symptom assessment, and night-time HRV measurements. Participants of this study were all adults between 18−70 years of age and were required to meet the following criteria: (1) experienced IBS symptoms for at least 6 months before they were diagnosed; (2) continued to have IBS symptoms for at least 6 months after being diagnosed by a licensed independent practitioner; (3) fulfilled the Rome III IBS criteria; (4) suffered from abdominal pain or discomfort for minimum 2 days in every 7 days for 14 days; (5) did not have an organic disease that caused symptoms at the time of enrollment; (6) adults over 50 years of age had a negative finding of abdominal radiographic and/or sonographic diagnostic tests, colonoscopy, or sigmoidoscopy. Participants were excluded from the study if they: (1) were using pharmaceutical drugs such as antibiotics, beta and calcium-channel blockers, glucocorticoids, acetylcholine blockers, and/or antidepressants; (2) had a history of abdominal surgical procedures (excluding the removal of appendix, gallbladder and uterus, caesarean delivery, female sterilization or ventral hernia reconstruction); (3) had GI pathology (e.g., neoplasm, infectious enteritis, celiac disease, and inflammatory bowel disease) or a cause for moderate or worse pain severity (e.g., spinal degeneration/injury and fibromyalgia); (4) had a metabolic or psychiatric disorder; (5) had a cardiac structural or electrophysiologic disease or immune system disorder or (6) were planning to conceive within 6 months, currently in the period of gestation, or breastfeeding. All participants were recruited after Institutional Review Board approval (IRB No. 32,722) was received and Clinical Trials (NCT00907790) was registered.
Procedures
At the first meeting, informed consent and baseline information (e.g., age, gender, race, highest education levels, medical history, bowel patterns and current home regimen medications) were obtained. Participants were then oriented to the study. Ambulatory electrocardiogram Holter monitors and Burdick 6732 3-channel compact digital Holter recorders (Burdick Inc, Deerfield, WI, USA) was used to collect nocturnal time domain HRV data. Burdick Vision Premier Analysis software was used to compute HRV summary measures from the recordings. All non-sinus beats and artifacts were captured, cleaned, and cross-checked by trained operators prior to analyzing 6-hour (midnight to 6 a.m.) R-R interval data in sequential 5-minute blocks.
Daily Symptom Diary
All participants kept daily symptom diaries for 28 consecutive days, with the first entry starting on the first evening after their initial visit. The daily symptom diary included individual items for GI symptoms (heartburn, nausea, abdominal pain, constipation, diarrhea), somatic symptoms (headache, backache, joint pain, muscle pain, fatigue, sleepiness), as well as emotional distress (anger, panic). Each symptom was rated every evening on a 5-point Likert scaling response, with a range from a minimum of 0 (“not present”) and maximum of 4 (“very severe”). Individual symptoms were then summarized for each patient as the percent of days experiencing “moderate” or worse within 28 days.
Statistical Analysis
We used the IBM SPSS Statistical software for Windows, version 26.0 (IBM Corp, Armonk, NY, USA) to analyze all data. Significance was detected when the p value was <.05. Baseline demographic characteristics, clinical presentations, and HRV measures were summarized and stratified by younger (<46 years) and older (≥46 years) age groups. This cutoff age point was based on a prior study by Natarajan et al. who found that vagal modulation is lower in women than men until age 46 (Natarajan et al., 2020). Chi-square tests, t-tests, the Fisher Exact Test, and analysis of variance were used to assess the baseline and clinical differences across the 2 age groups. Our team applied one-sample Kolmogorov-Smirnov to evaluate normality of the HRV dataset (Ramirez-Villegas et al., 2011). Since HRV measurements generally have a highly skewed distribution, log transformation was used to presume a normal distribution. We then conducted analyses of variance to compare the mean of HRV indices and percent of days experiencing moderate to severe GI, somatic, and emotional distress symptoms between the 2 age groups. Body mass index (BMI) was adjusted for potential confounding effects in analyses (Strüven et al., 2021). The partial correlation analyses controlled with age and BMI were used to assess the relationships between HRV and symptom measures (e.g., GI, somatic, emotional) within each age group.
Results
Comparison of Demographic Characteristics, Gastrointestinal and Psychological Distress Symptoms and Heart Rate Variability Indices in Younger and Older Age Groups of Women with Irritable Bowel Syndrome (IBS).
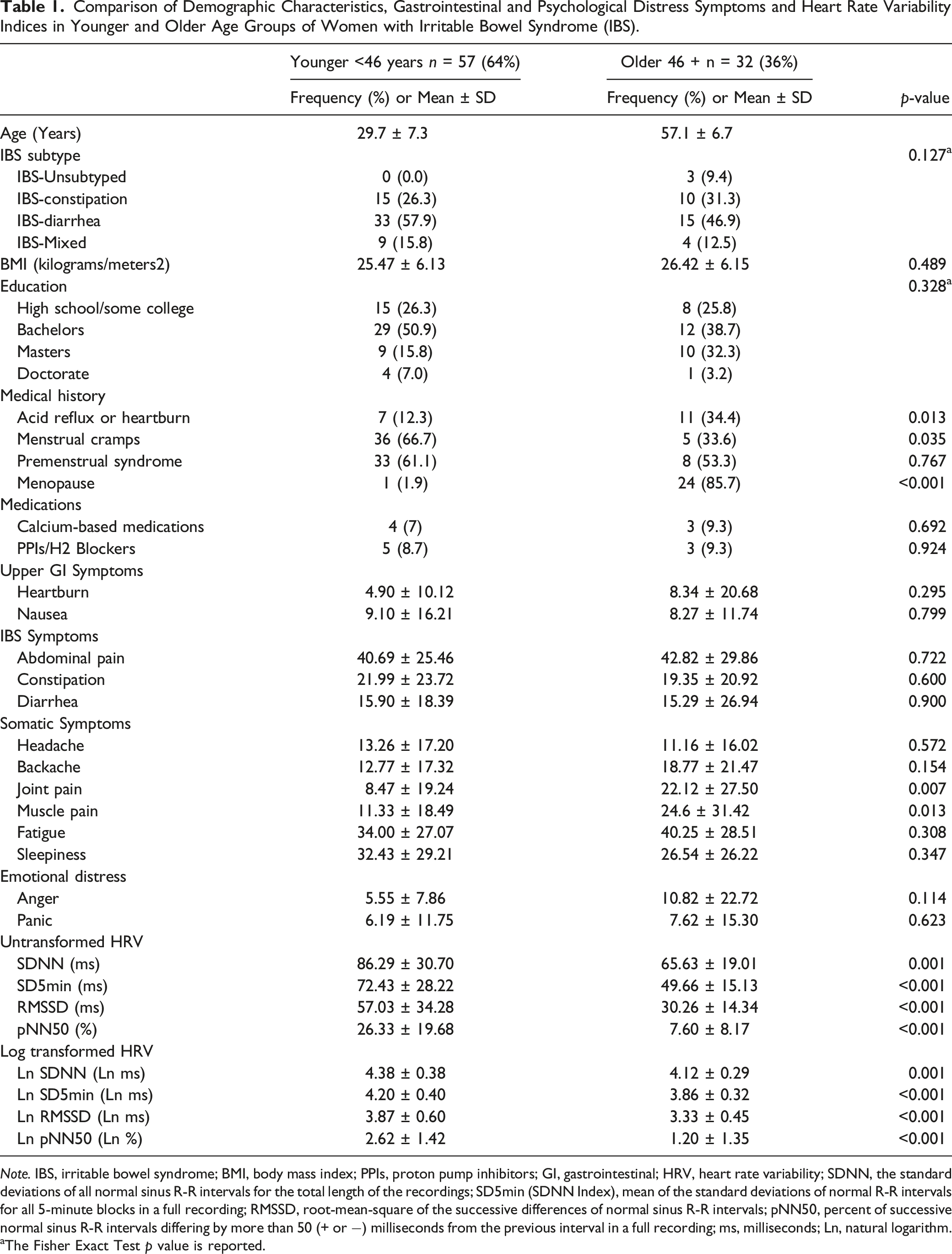
Note. IBS, irritable bowel syndrome; BMI, body mass index; PPIs, proton pump inhibitors; GI, gastrointestinal; HRV, heart rate variability; SDNN, the standard deviations of all normal sinus R-R intervals for the total length of the recordings; SD5min (SDNN Index), mean of the standard deviations of normal R-R intervals for all 5-minute blocks in a full recording; RMSSD, root-mean-square of the successive differences of normal sinus R-R intervals; pNN50, percent of successive normal sinus R-R intervals differing by more than 50 (+ or −) milliseconds from the previous interval in a full recording; ms, milliseconds; Ln, natural logarithm.
aThe Fisher Exact Test p value is reported.
Association of Upper Gastrointestinal Symptoms with Individual Irritable Bowel Syndrome Symptoms
Correlations Between Upper Gastrointestinal Symptoms, Irritable Bowel and Other Symptoms in Different Age Groups.
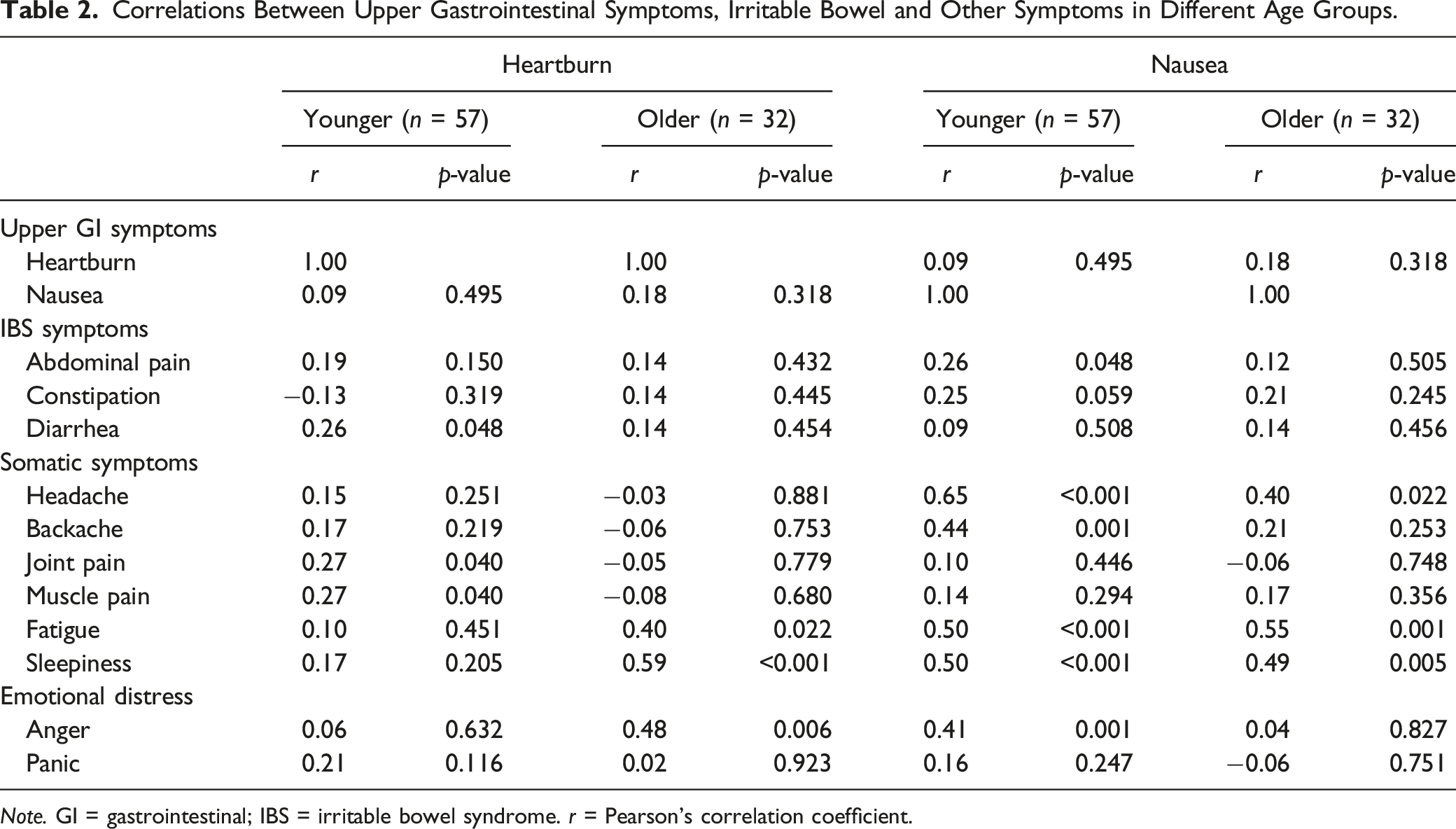
Note. GI = gastrointestinal; IBS = irritable bowel syndrome. r = Pearson’s correlation coefficient.
Association of Upper Gastrointestinal Symptoms with Somatic and Emotional Distress Symptoms
Both joint and muscle pain were significantly associated with heartburn in the younger group (p = .040). Positive associations of heartburn with fatigue (p = .022), sleepiness (p < .001) and anger (p = .006) were significant in older women. Daily nausea was strongly associated with fatigue in both age groups (younger p < .001; older p = .001). In addition, nausea was associated with sleepiness in younger (p < .001) and older (p = .005) women. In the younger group, nausea was significantly associated with headache, back pain, and anger. Of these, only headache was significantly correlated with nausea in the older group.
Heart Rate Variability and Extraintestinal and Emotional Distress Symptoms
Correlations Between Heart Rate Variability Indices and Percentage Days of IBS and Other Symptoms in Younger IBS Women after Controlling Age and BMI.
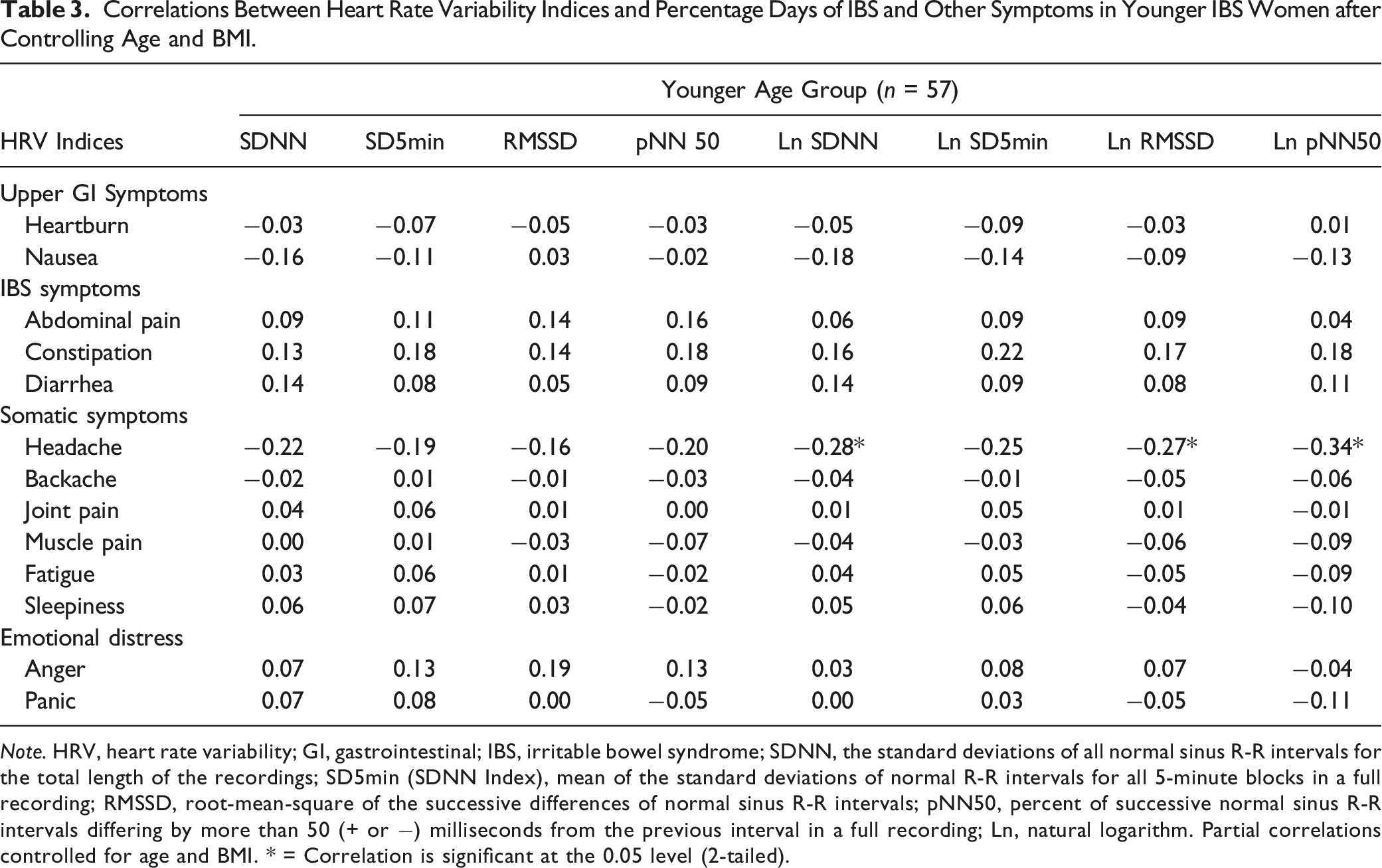
Note. HRV, heart rate variability; GI, gastrointestinal; IBS, irritable bowel syndrome; SDNN, the standard deviations of all normal sinus R-R intervals for the total length of the recordings; SD5min (SDNN Index), mean of the standard deviations of normal R-R intervals for all 5-minute blocks in a full recording; RMSSD, root-mean-square of the successive differences of normal sinus R-R intervals; pNN50, percent of successive normal sinus R-R intervals differing by more than 50 (+ or −) milliseconds from the previous interval in a full recording; Ln, natural logarithm. Partial correlations controlled for age and BMI. * = Correlation is significant at the 0.05 level (2-tailed).
Correlations Between Heart Rate Variability Indices and Percentage Days of IBS and Other Symptoms in Older IBS Women after Controlling Age and BMI.
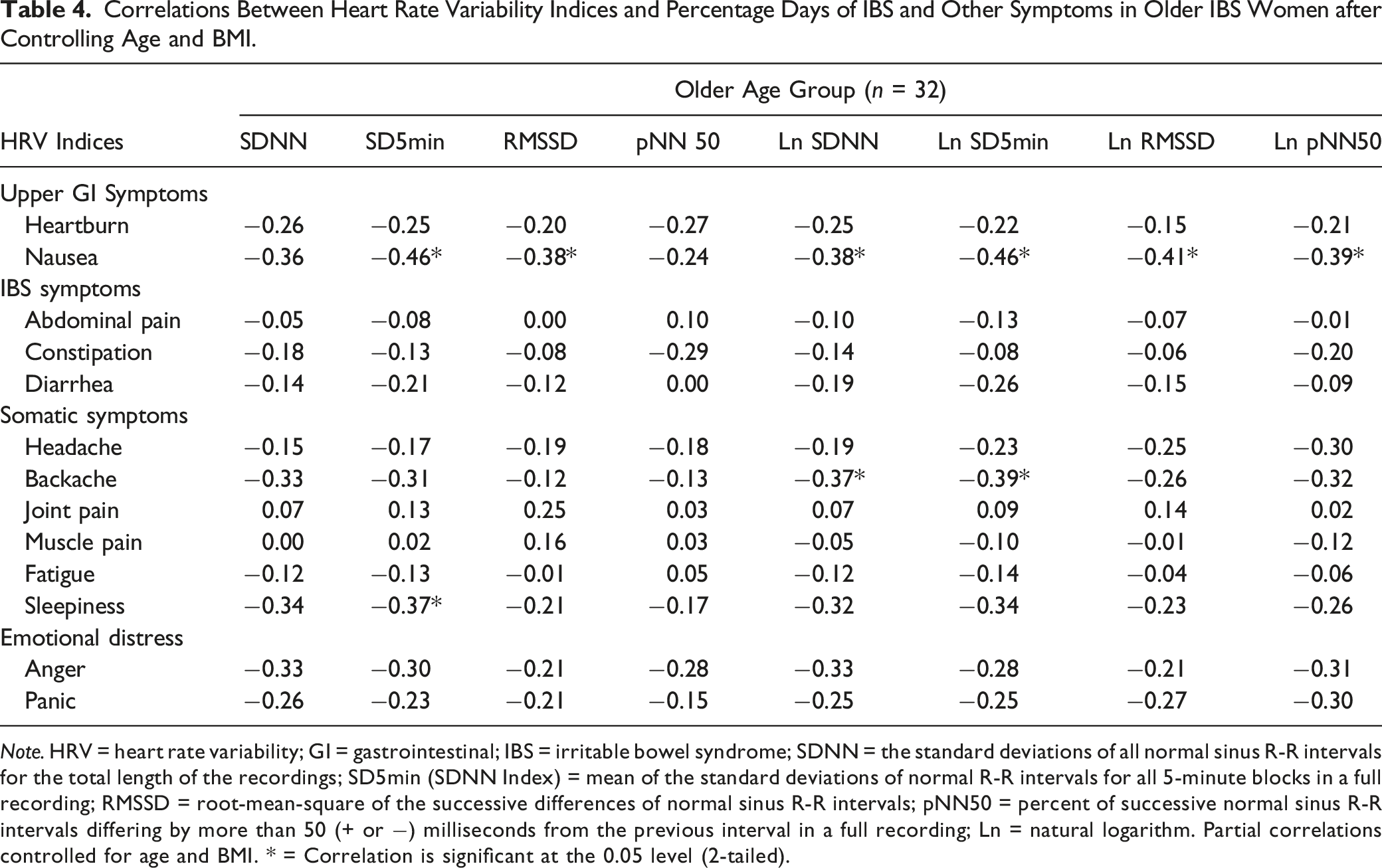
Note. HRV = heart rate variability; GI = gastrointestinal; IBS = irritable bowel syndrome; SDNN = the standard deviations of all normal sinus R-R intervals for the total length of the recordings; SD5min (SDNN Index) = mean of the standard deviations of normal R-R intervals for all 5-minute blocks in a full recording; RMSSD = root-mean-square of the successive differences of normal sinus R-R intervals; pNN50 = percent of successive normal sinus R-R intervals differing by more than 50 (+ or −) milliseconds from the previous interval in a full recording; Ln = natural logarithm. Partial correlations controlled for age and BMI. * = Correlation is significant at the 0.05 level (2-tailed).
Heart Rate Variability and Upper Gastrointestinal Symptoms
In younger women with IBS, we did not detect associations between heartburn, nausea, and indicators of HRV. In older women with IBS, there was no significant relationship between heartburn and HRV measures. However, nausea was inversely associated with mixed PSNS and SNS HRV indices (SD5min, p = .011; Ln SDNN, p = .036; Ln SD5min, p = .011) and PSNS measures (RMSSD, p = .041; Ln RMSSD, p = .026; Ln PNN50, p = .034). Notably, the correlations between nausea and HRV indices of SDNN and pNN50 were not significant. However, the variables became significant when expressed in log transformation (Ln SDNN and Ln pNN50). Partial correlations controlling for age and BMI between HRV measures and symptom severity among older women with IBS are presented in Table 4. Daily reports of anger and panic, 2 components of emotional distress, were significantly correlated with constipation, headache, backache, and fatigue. When women were compared based on menopausal status rather than age group, similar relationships between upper GI, IBS, and extra-intestinal symptoms and HRV measures were found (see Supplemental Table 1).
Discussion
Since the ANS modulates function of the upper GI tract, we sought to compare younger and older women with IBS with respect to upper GI symptoms of heartburn and nausea and HRV indices. In both age groups, the reporting of heartburn and nausea occurred on less than 10% of days over the four-week period. There were significant age group differences in HRV indices with younger women demonstrating higher vagal modulation. In older women, nausea was inversely correlated with HRV indices reflecting lower vagal (PSNS) activity and measures reflecting combined SNS and PSNS modulation. Daily heartburn was not associated with HRV indices in either age group. In older women, heartburn was associated with somatic and emotional distress symptoms including daytime sleepiness and anger. Age-related distinctions in correlations of daily upper GI symptoms and indicators of ANS function were found in this community- and clinic-recruited sample of women with IBS.
To our knowledge, our work is the first to study ANS measures using HRV indicators with respect to upper GI symptoms and age in women with IBS. Age-related differences in autonomic indices as reflected in heart rate and HRV in both healthy adults and those with IBS have been well documented (Thayer et al., 2021; Vreijling et al., 2021). The age-related alterations in ANS modulation are attributed to varied underlying factors, including sex hormones, central nervous system processing, cardiac electrophysiological characteristics, and structural cardiovascular features (Koenig, 2020; Thayer et al., 2021). In addition to significant differences in HRV indicators between younger and older women, we also found an age-related difference in their association with nausea. In older women, nausea was inversely related to indicators of PSNS and measures reflecting mixed SNS and PSNS modulation. These results are similar to a study of ANS function and symptom severity in persons with nausea and vomiting as part of a composite score from a Gastroparesis registry of patients with diabetic and idiopathic gastroparesis. Nguyen et al. showed that PSNS activity was lower in persons with more severe upper GI symptoms than those with mild or moderate symptom severity (Nguyen et al., 2020). Due to the role of the vagus nerve in stimulating gastric motility, it can be conjectured that a reduction in vagal modulation could result in delayed gastric emptying and subsequent feelings of fullness and nausea (Gottfried-Blackmore et al., 2020). Prior HRV studies by our group in separate samples found that IBS women with constipation had decreased vagal modulation compared to IBS women with diarrhea and healthy controls (Cain et al., 2007; Heitkemper et al., 2001). Whether the link of reduced HRV with nausea in older women is due directly to the effects on delayed upper and decreased motility or is a consequence of medications such as intermittent use of laxatives, anti-reflux, or other medications is unknown and warrants further study.
Overall, the lack of differences in IBS symptom intensity among younger and older women, as well as premenopausal and postmenopausal status, is similar to that of Lenhart et al. (Lenhart et al., 2020). However, unlike the Lenhart study, we did not find that older women reported more daily complaints of constipation. This may be related to the fact that the majority of our sample were IBS-diarrhea predominant. Not unexpectedly, age- and menopause-related daily symptom differences were found between joint and muscle pain items which matched previously studied pre and postmenopausal women (Cain et al., 2009).
Heartburn is not part of the diagnostic criteria for IBS but is often included in comprehensive symptom assessments of patients with DGBIs (Sperber et al., 2021). Although commonalities in visceral sensitivity between non-erosive heartburn and IBS have been reported (Rengarajan et al., 2021), we found that younger and older community and clinic-recruited women report moderate to very severe heartburn on less than 10% of days while moderate to very severe abdominal pain was reported on approximately 40% of days. Shah et al. used the GI-PROMIS measure that asked about frequency and severity of symptoms over the past 7 days in a large sample, and reported that heartburn was more severe in persons with IBS-constipation than those with chronic idiopathic or functional constipation (Shah et al., 2018). In our study with both IBS-C and IBS-D, albeit a small sample of IBS-C, we found a significant relationship between daily heartburn and diarrhea symptom severity in younger women using daily symptom records.
Our finding of a positive relationship between indicators of poor sleep (daytime sleepiness and fatigue) with heartburn in older women is consistent with an older study using daily diaries (Naliboff et al., 2004) and a systematic review of sleep quality, fatigue, and nocturnal heartburn among persons with gastroesophageal reflux (Gerson & Fass, 2009). In the current study, participants were asked to complete their diaries at bedtime but to consider symptoms within the 24-hour window. Thus, it cannot be determined whether heartburn was sleep-, stress- and/or meal-related. Understanding the temporal patterns of symptoms would be important for tailoring interventions such as sleep hygiene and meal timing for older women.
Our present study has several cardinal and limited features. The HRV data were recorded in a natural setting with the individual supine over the nighttime hours. However, the measures may not reflect daytime responses when symptoms are most likely to occur. Self-reported symptoms are highly heterogeneous and marked by intra- and inter-individual variability in the severity and frequency that individuals experience. Our current study captured daily ratings of the symptoms within the 24-hour period. Thus, the triggers of symptoms were not identified. Our sample included only women who were enrolled in an intervention trial of cognitive behavioral therapy and consequently may not be representative of all women patients with IBS. Most women had been diagnosed with IBS more than 5 years. This is an exploratory analysis that did not control for multiple comparisons so results should be cautiously interpreted and need to be replicated in independent dataset.
Our study assessed daily heartburn and nausea and HRV indices among women with IBS, stratifying them into 2 age-related groups. Findings revealed age-related differences in ANS factors that are associated with nausea. These differences may be important when considering treatment options such as HRV biofeedback, self-management cognitive behavioral therapy, exercise, acupuncture, and hypnosis for patients with IBS and concurrent upper GI symptoms (Caillet et al., 2022; Chen et al., 2022; Chey et al., 2021; Jarrett et al., 2016). The capture of DGBI overlap could help to tailor the individualized care plan and improve quality of life and health outcomes (Sperber et al., 2022).
Supplemental Material
Supplemental Material - Age Differences in Upper Gastrointestinal Symptoms and Vagal Modulation in Women With Irritable Bowel Syndrome
Supplemental Material for Age Differences in Upper Gastrointestinal Symptoms and Vagal Modulation in Women With Irritable Bowel Syndrome by Li Juen Chen, Robert Burr, Kevin Cain, Kendra Kamp, Margaret Heitkemper in Biological Research For Nursing
Footnotes
Author Contributions
Li Juen Chen, Designed the study, analyzed data, interpreted results, prepared tables, and drafted the manuscript; approved the final draft of the manuscript. Robert L. Burr (bioengineer), Participated in heart rate variability collection with special emphasis on the technical aspects of the analysis, interpreting results, and commenting on the manuscript; approved the final draft of the manuscript. Kevin Cain (biostatistician), Participated in study-design data analysis; approved the final draft of the manuscript. Kendra Kamp, Participated in study interpretation, commented on and edited the manuscript at various stages of its development; approved the final draft of the manuscript. Margaret Heitkemper, Supervised and participated in all aspect of the study, including conception, results interpretation, and manuscript generation; approved the final draft of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute of Nursing Research, National Institutes of Health, USA (Grant No. NR004142). Kendra J. Kamp is supported in part by the National Institutes of Nursing Research (Grant No. K23 NR020044).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.